Lippincott Williams & Wilkins · Web viewCognitive testing showed good working memory but reduced...
10
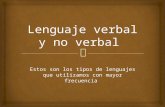
Table e-1. Primers used for Sanger sequencing confirmation. c.DNA change Amino acid change Forward Reverse c.176G>A p.Gly59Asp CGGCAGCAAATGGAAATATC A GGAGTAGACATCGCTGGTGA c.325C>T p.Gln109Ter CGGCAGCAAATGGAAATATC A GGAGTAGACATCGCTGGTGA c.349T>C p.Ser117Pro CATGCAGTTCTCTATCCCGC GGACGCCCAGGTAAAGTAGG c.1383C>G p.Pro420Arg CGATGTCTACTCCTCCGACG AGCGCCATCTCAGTGTAGC c.1401_1402i nsCGCTGGTG p.Trp426Cysf s*11 CGATGTCTACTCCTCCGACG AGCGCCATCTCAGTGTAGC c.1611C>T p.Pro496Leu CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGG c.1598C>T p.Ser533Leu CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGG c.1634G>A p.Gly545Asp CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGG c.1832G>T p.Arg611Leu CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGG c.1967T>C p.Ile656Thr CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGG c.2162G>A p.Gly680Ser CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGG c.2212_2213d el p.Leu696Prof s*10 CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGG Figure e-1. Sanger sequencing confirmation and pedigrees of the families with MYORG mutations reported in this study.
Transcript of Lippincott Williams & Wilkins · Web viewCognitive testing showed good working memory but reduced...

Table e-1. Primers used for Sanger sequencing confirmation.
c.DNA change Amino acid change
Forward Reverse
c.176G>A p.Gly59Asp CGGCAGCAAATGGAAATATCA GGAGTAGACATCGCTGGTGAc.325C>T p.Gln109Ter CGGCAGCAAATGGAAATATCA GGAGTAGACATCGCTGGTGAc.349T>C p.Ser117Pro CATGCAGTTCTCTATCCCGC GGACGCCCAGGTAAAGTAGGc.1383C>G p.Pro420Arg CGATGTCTACTCCTCCGACG AGCGCCATCTCAGTGTAGCc.1401_1402insCGCTGGTG
p.Trp426Cysfs*11 CGATGTCTACTCCTCCGACG AGCGCCATCTCAGTGTAGC
c.1611C>T p.Pro496Leu CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGGc.1598C>T p.Ser533Leu CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGGc.1634G>A p.Gly545Asp CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGGc.1832G>T p.Arg611Leu CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGGc.1967T>C p.Ile656Thr CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGGc.2162G>A p.Gly680Ser CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGGc.2212_2213del p.Leu696Profs*10 CTACTTCAAGTTCGACGCGG GGACGCCCAGGTAAAGTAGG
Figure e-1. Sanger sequencing confirmation and pedigrees of the families with MYORG mutations reported in this study.

Table e-2. Description and classification of all MYORG mutations reported in this study.
Variant description Variant classification Evidence for classificationFrequency Segre
gation
Location and
functional domain
Computational predictions
c.DNA change
Amino acid change
Zygosity in patients
Novelty Mutation type
rsNumber
ACMG criteria
ACMG classification
gnomAD All
Total allele count (het)
In-house controls (4000)
Conservation (GERP ++ score)
CADD score
MutationTaster
c.176G>A p.Gly59Asp Hom Known missense rs778863651
PM1, PM2, PP2, PP4
Likely pathogenic
0.000041 11 0 hom/ 0 het
NA N-terminal cytoplasmic domain
3.3 5 Disease causing
c.325C>T p.Gln109Ter Comp het Known nonsense rs746104060
PVS1, PM1, PM2, PM4, PP3, PP4
Pathogenic 0.000004 1 0 hom / 0 het
yes Helical transmembrane domain
4.87 35 Disease causing
c.349T>C p.Ser117Pro Comp het Novel aa change in known pathogenic position
missense rs755742995
PM1, PM2, PM5, PP4, PP2, PP3
Likely pathogenic
0.000009 9 0 hom/ 0 het
yes Extracellular glycosidase domain
5.82 25 Disease causing
c.1383C>G
p.Pro420Arg Comp het Novel missense NA PM1, PM2, PP2, PP4
Likely pathogenic
absent absent 0 hom/ 0 het
yes Extracellular glycosidase domain
5.08 24.2 Disease causing
c.1401_1402insCGCTGGTG
p.Trp426Cysfs*11 Comp het Known frameshift insertion
rs779658130
PVS1, PM2, PM4, PP3, PP4
Pathogenic 0.00001069
1 0 hom/ 0 het
NA Extracellular glycosidase domain
NA NA Disease causing
c.1611C>T
p.Pro496Leu Hom Novel missense NA PM1, PM2, PP1, PP2, PP4
Likely pathogenic
absent absent 0 hom/ 0 het
yes Extracellular glycosidase domain
5.27 16.4 Disease causing
c.1598C>T
p.Ser533Leu Comp het Known missense rs761392440
PM1, PM2, PP2, PP3, PP3, PP4
Likely pathogenic
0.000025 6 0 hom/ 1 het
yes Extracellular glycosida
5.59 26.2 Disease causing

se domain
c.1634G>A
p.Gly545Asp Comp het Known missense rs199770930
PM1, PM2, PP2, PP3, PP4
Likely pathogenic
0.00006163
17 0 hom/ 2 het
yes Extracellular glycosidase domain
5.59 27 Disease causing
c.1832G>T
p.Arg611Leu Comp het Known missense rs757944000
PM1, PM2, PP2, PP3, PP4
Likely pathogenic
0.00002069
5 0 hom/ 0 het
yes Extracellular glycosidase domain
5.56 28.5 Disease causing
c.1967T>C
p.Ile656Thr Comp het Known missense rs370944350
PM1, PM2, PP2, PP3, PP4
Likely pathogenic
0.00002500
7 0 hom/ 1 het
NA Extracellular glycosidase domain
5.27 24.9 Disease causing
c.2162G>A
p.Gly680Ser Comp het Known missense COSM4695529
PM1, PM2,PP2, PP3, PP4
Likely pathogenic
absent absent 0 hom/ 0 het
yes Extracellular glycosidase domain
5.54 26.6 Disease causing
c.2211_2212del
p.Leu696Profs*10 Comp het Novel frameshift deletion
NA PVS1, PM2, PM4, PP2, PP3, PP4
Pathogenic absent absent 0 hom/ 0 het
yes Extracellular glycosidase domain
NA NA Disease causing
ENST00000297625, Genbank transcript ID NM_020702. Position on Genome Reference Consortium human genome build 38 (GRCh38). Legend: aa- amino acid, Comp het - compound heterozygous, hom – homozygous, ACMG - American College of Medical Genetics and Genomics, EXAC- Exome Aggregation Consortium, NA- not available, hom-homozygous, het- heterozygous, GERP++ score- Genomic Evolutionary Rate Profiling score, CADD -Combined Annotation Dependent Depletion. In house controls consist of 2800 control cases.

e-3. Phenotype-Genotype correlation for the MYORG mutations identified in this study.
Family 1 is of Pakistani descent. The proband, case 1, was born to consanguineous parents and
presented at 40 years with right arm and leg tremor and rigidity. Her initial clinical examination one
year later showed profound facial hypomimia, hypermetric saccades and reduced upgaze. There was
profound bilateral bradykynesia with increased tone. Her gait showed reduced arm swings and a
combination of ataxia and difficulties turning. Archimedes spiral drawing showed a profound increase
in spiral density and handwriting had a three-sentence micrographia. She had limited response to high
doses of Levodopa. Cognitive testing showed good working memory but reduced verbal fluency, a
concrete verbal reasoning and an impaired Luria 3 test.
WES identified a homozygous variant in MYORG -the c.176G>A, p.Gly59Asp. Located in a conserved
amino acid position, this variant was absent in our in-house control dataset of 2800 individuals and
was absent in homozygous state in Genome Aggregation Database (gnomAD).
Family 2 is of Middle Eastern origin from Israel. We have previously reported the clinical presentation
of the two affected siblings1. The older brother (patient 2) presented at 52 years with walking difficulty,
cramps, dysarthria and memory impairment (MMSE 27/30). The younger brother (patient 3) presented
at 45 years with vertigo, ataxia, memory impairment (MMSE 28/30) and headache. WES in the two
affected siblings identified a shared homozygous c.1611C>T, p.Pro496Leu. This variant was absent in
our in-house and all publically available databases and is located in a conserved amino acid position
affecting the glycosidase functional domain.
Family 3 is Caucasian of British origin. Extensive brain calcifications were identified at the age of 87
years as incidental findings during clinical evaluation for Bell’s palsy (patient 4). Detailed neurological
examination revealed only mild cerebellar and extrapyramidal signs including reduced arm swing,
dysdiadochokinesia and broad based gait. WES revealed a compound heterozygous mutation
c.1598C>T, c.1634G>A (p.Ser533Leu,p.Gly545Asp). Both variants are very rare wih p.Ser533Leu found
with a frequency of 0.000045 and the p.Gly545Asp in 0.0001 in gnomAD and are located in a

evolutionary highly conserved and conserved amino acid position respectively. With CADD scores of 26
and 27, these variants are predicted to affect the extracellular glycosidase functional domain.
Families 4-7 are non-consanguineous, Caucasian, of Italian origin. In family 4 we found two compound
heterozygous variants: c.2211_22126del, c.349T>C (p.Leu696Profs*10, p.Ser117Pro). The
p.Leu696Profs*10 is a frameshift deletion absent in our in-house and all publically available databases
and located in a conserved amino acid position predicted to lead to nonsense-mediated decay (NMD).
The p.Ser117Pro is a novel amino acid change in a known pathogenic position. The two variants
segregated with the disease in the family. The proband (case 5) presented at age 56 with asymmetric
akinetic-rigid parkinsonism and supranuclear gaze palsy with poor response to Levodopa, mimicking a
PSP case. Progressive deterioration of motor function, dysarthria, dysphagia and gait ataxia became
evident over the following years. Depression was reported at age 60 and was treated with sertraline.
In family 5 we found two compound heterozygous missense variants, the c.2162G>A, c.1383C>G
(p.Gly680Ser, p.Pro420Arg). Both variants are absent in publically available databases and are located
in highly conserved and conserved amino acid positions respectively and segregated with the disease
in the family. The proband (patient 6) presented at age 73 with dysarthria and mild ataxic gait. Mild
parkinsonism became evident over the following 4 years and was levodopa-responsive. Dysarthria
showed a progressive course making speech less intelligible. No cognitive or psychiatric disturbances
have emerged 8 years after the onset.
In family 6 we found two compound heterozygous variants, the c.325C>T, c.1832G>T (p.Gln109Ter,
p.Arg611Leu). Both variants are very rare with gnomAD frequencies of 0.000004 and 0.000025
respectively with p.Gln109Ter leading to a premature termination and a highly truncating protein with
a predicted loss of the entire extracellular topological domain. These variants and segregated with the
disease in the family. The proband (patient 7) presented progressive dysarthria and dysphagia since
age 62, and was incidentally diagnosed with PFBC when admitted for a lacunar cerebral stroke.

Cognitive impairment was present by the age of 67 and dysarthria was the most disabling clinical
feature.
In family 7 we found two compound heterozygous variants, the c.1401_14026insCGCTGGTG,
c.1967T>C (p.Trp426Cysfs*11, p.Ile656Thr), both found with very rare frequencies in gnomAD
(0.000045 and 0.00001 respectively). The p.Trp426Cysfs*11 is a frameshift insertion predicted to lead
to severe protein truncation and NMD and the p.Ile656Thr is located in a conserved amino acid
position within the glycosidase functional domain. The proband (case 8) showed a PSP-like phenotype
at the age of 62 years (akinetic-rigid parkinsonism, frequent falls, staring gaze with vertical gaze palsy)
that progressed over 16 years along with gait ataxia, cognitive decline, urinary incontinence and diffuse
pyramidal signs. At the age of 68, the patient was bed-ridden and required assistance for self-care.
Reference:1. Bowirrat, A., Yassin, M., Artoul, F., and Artul, S. (2013). Fahr's disease: bilateral symmetrical
striopallidodentate calcification in two brothers with two distinct presentations. BMJ case reports 2013.