Linc Osami Des
77
LINCOSAMIDES
Transcript of Linc Osami Des
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 1/77
LINCOSAMIDES
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 2/77
Lincomycin (from Streptomyces lincolnensis)
+Clindamycin (semisynthetic derivative of
Lincomycin)
• Clindamycin
• It is similar in mechanism of action (inhibits
protein synthesis by binding to 50 S ribosome)and spectrum of activity to erythromycin.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 3/77
Antibacterial activity: str., staph., pn.,
C. Diphtherine, Nocardia, Actinomycetes,
Toxoplasma+ high activity against anaerobes,specially Bacteroides fragilis.
Aerobic gram negative bacilli are not affected.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 4/77
Pharmacokinetics:
It is administered orally (Oral absorbtion isgood ) but most often is administeredparenterally (i.v.) because pseudomembranouscolitis is less likely to follow parenteraladministration.
It penetrates to most skeletal and soft tissues,but not brain and cerebrospinal fluid;
accumulates in neutrophils and macrophages.It islargely metabolized and metabolites are excretedin urine and bile.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 5/77
Clinical uses:
-skin and soft tissue infections caused by str. and staph.
-anaerobic infections, specially by Bacteroides fragilis(abdominal, pelvic, lung abscesses); it is generallycombined with an aminoglycoside or cephalosporin;
-topical preparations of clindamycin are used to treat infectedacne vulgaris.
-clindamycin, sometimes in combination with anaminoglycoside or cephalosporin is used to treatpenetrating wounds of the abdomen and the gut;
- infections originating in the female genital tract;
-it may be used instead of erythromycin for prophylaxis of
endocarditis in patients with valvular heart diseases whoare undergoing certain dental procedures.
-in AIDS patients (in combination with other drugs) fortoxoplasmosis and Pneumocystis carinii pneumonia.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 6/77
Side effects:
-rashes, urticaria;-abdominal pain;
-the major problem is diarrhoea andpseudomembranous enterocolitis due to
Clostridium difficile superinfection which is
potentially fatal.The drug should be promptly
stopped and metronidazole (alternatively
vancomycin) given to treat it.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 7/77
Dosages:
• Orally, 150-300 mg, every 6 hours: 10-20 mg /
kg / day for children ;
• Intravenously, 600 mg, every 8 hours.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 8/77
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 9/77
POLYPEPTIDE ANTIBIOTICS
POLYMYXIN B and POLYMYXIN
E(COLISTIN )
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 10/77
They are natural compounds obtained
from Bacillus polymyxa (polymyxin B) and
Bacillus colistinus (Colistin ).
Antibacterial activity: gram negative
bacteria only; all except proteus, serattia,
neisseria are inhibited.Both have very similar
range of activity, but colistin is more potent onpseudomonas, salmonella and shigella.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 11/77
• Mechanism of action: They are rapidly acting
bactericidal agents. They act as cationic
detergents.They atach to and disrupt bacterial
cell membrane.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 12/77
• Pharmacokinetics: They are not absorbed
from gastrointestinal tract after oral
administration and they act locally.They are
rarely considered for systemic administration
because of their poor tissue distribution and
their serious adverse effects. They are now
restricted for topical uses.Applied topicallythey are safe, no systemic effect or
sensitization occurs.A rashe is rare.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 13/77
• Clinical uses:
• -orally:
• –gram negative bacillary (E.coli, Salmonella,
Shigella) diarrhoeas, specially in infants and
children;
• -Pseudomonas enteritis;-
• gut sterilization, to supress the aerobic gramnegative members of the intestinal flora in
immunosuppressed patients.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 14/77
• -topically:-usually in combination with other
antimicrobials (neomycin or bacitracin or
glucocorticosteroids) for skin infections, burns,
otitis externa, conjunctivitis, corneal ulcer-caused by gram negative bacteria, including
Pseudomonas. These preparations are available
as ointments, solutions.
• -solutions with polymyxin B can be injected into
joint spaces, pleural cavity(for local action).
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 15/77
• Adverse effects:
• -given orally, side effects are limited to thegastrointestinal tract: occasional nausea,
vomiting, diarrhoea;• -given parenterally they have high toxicity:
marked kidney damage, neurological
disturbances, neuromuscular blockade,flushing and paresthesias due to liberation of histamine from mast cells.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 16/77
STREPTOGRAMINS and
OXAZOLIDINONES
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 17/77
STREPTOGRAMINS
QUINUPRISTIN –DALFOPRISTIN
• It is a combination of two streptogramins;
•
Antibacterial activity: GRAM + COCCI:multidrug resistant strept., penicillin resistant
strept., staph., ec .faecium ( not faecalis);
• It is administered i.v.;
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 18/77
Clinical uses:
• -infections caused by staph. / by Vancomycin
resistant E. faecium;
Side effects:
• -pain at the site of infections;arthralgias.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 19/77
OXAZOLIDINONES
LINEZOLID-synthetic compound;
Antibacterial activity:GRAM + organisms
( staph., strept., ec., gram + rods);• It is bacteriostatic or bactericidal ( on str.);
• Mechanism of action : it inhibits bacterial
protein synthesis;
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 20/77
Clinical uses:
• -vancomycin resistant E. faecium;
• Nosocomial pneumonia;
• Community acquired pneumonia;
•
Skin infections• ! It should be reserved for treatment of
infections caused by multidrug resistant gram
positive bacteria.Toxicity : reversible, generally mild
thrombocytopenia.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 21/77
AMINOGLYCOSIDE ANTIBIOTICS
Natural and semisynthetic
antibiotics originally obtained fromvarious Streptomyces species.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 22/77
Common characteristics:
*they are all structurallyrelated : hexose ring to
which variousaminosugars(two or more)
are attached by glycosidiclinkages.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 23/77
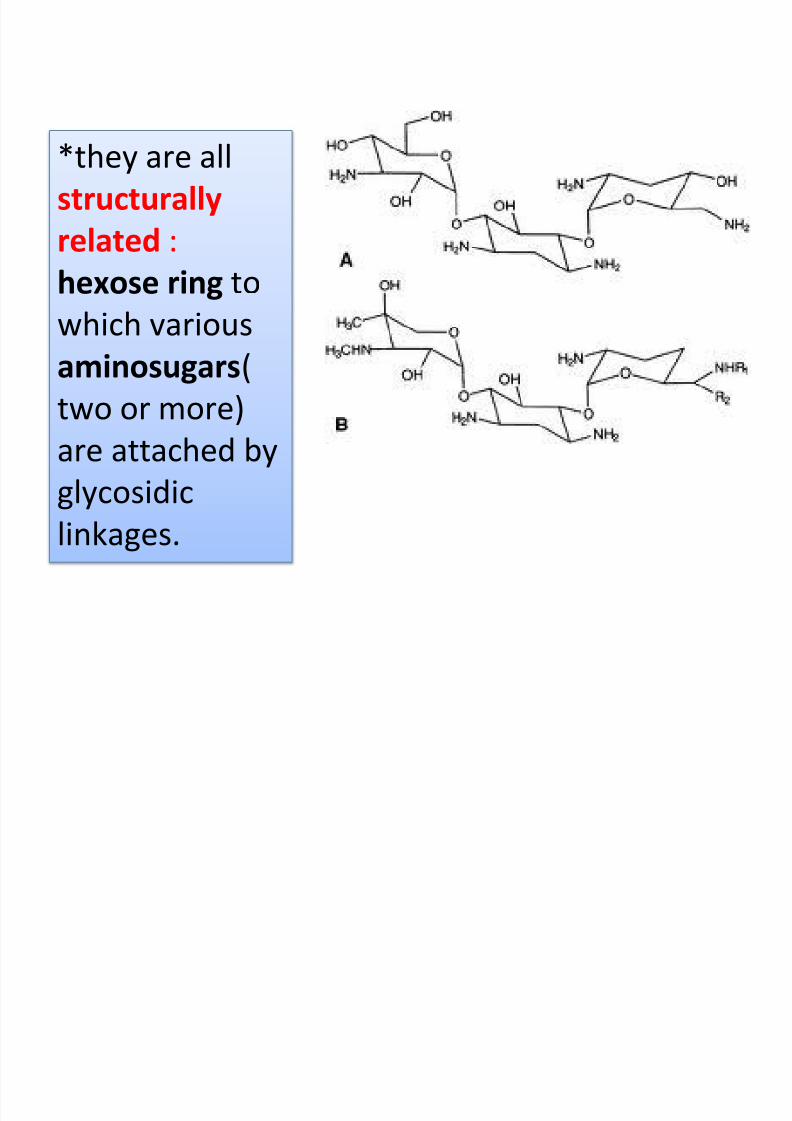
*they are all
structurally
related :
hexose ring towhich various
aminosugars(
two or more)are attached by
glycosidic
linkages.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 24/77
*most of them are given parenterally (i.m. and i.v.);
*they distribute only extracellularly ; do not
penetrate brain or cerebrospinal fluid.*all are used as sulphate salts( highly water
soluble); solutions are stable for months.
*they are not metabolized and all are excretedunchanged in urine by glomerular filtration.
*all are active primarily against aerobic gramnegative bacilli (E.coli, proteus, Pseudomonas),
staph., str., but spectrum differs.Anaerobes are resistant because aminoglycosides
transport into cells is oxygen dependent.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 25/77
*They have the same mechanism of action: they are bactericidal agents; they
inhibit bacterial protein synthesis bybinding to 30S ribosomal subunit, or toadditional sites on 50 S subunit as well asto 30S-50 S interface.
Recent experimental studies showthat the initial site of action is the outerbacterial membrane .The cationic
antibiotic molecules create fissures inthe outer cell membrane resulting inleakage of intracelullar contents andenhanced antibiotic uptake.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 26/77
*The aminoglycosides produce toxic effects whichare common to all members, but the relativepropensity differs.All exhibit:
*ototoxicity: cochlear and vestibulardamages of VIIIth cranial nerve, with hearing loss,respectivelly with headache, nausea, vomiting,dizziness, nystagmus, vertigo, ataxia.
* nephrotoxicity: it manifests as tubulardamage.
* neuromuscular blockade.
* Resistance occurs rapidly ( inactivation bytransferase enzymes, impaired entry of aminoglycosides into the cell, alteration of protein receptor on the ribosome)
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 27/77
The most important aminoglycosides:
• AMIKACIN *APRAMYCIN
• ARBEKACIN *RHODOSTREPTOMYCIN
• GENTAMICIN
•
KANAMYCIN SPECTINOMYCIN-chemically related to AMG
• NEOMYCIN
• PAROMOMYCIN
• STREPTOMYCIN
• TOBRAMYCIN
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 28/77
STREPTOMYCIN -obtained from streptomyces
griseus.
-Antimicrobial activity:relatively narrow: only few strainsof E.coli, H. Infl., Klebsiella, Shigella, V. Cholerae,enterococci and some gram positive cocci are nowinhibited that too at higher concentrations.
Sensitive germs are: Brucella, Yersinia pestis,
Mycobacterium tuberculosis, Nocardia, Francisellatularensis.
Resistance: many organisms develop rapid resistance tostreptomycin.Eg: in the intestinal and urinary tractsresistant organisms may emerge within 2 days of therapy. E.coli, H. Infl., Str. Pneumoniae, staph. Aureushave become largely resistant. If it is used alone,Mycobacterium tuberculosis also become resistant.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 29/77
Clinical uses:
-tuberculosis (in combination with other drugs becauseresistance emerges rapidly);
-subacute bacterial endocarditis (caused by streptococciviridans or enterococci) in conjunction with penicillin(today gentamicin is preferred);
-tularemia: it is the drug of choice for this rare disease;
Adverse effects:-vestibulotoxicity(vestibular disturbances);
-it has the lowest nephrotoxicity among aminoglycosides;
-pain at site of injection is common,
Streptomycine is administered i.m.: in acute infections
1 g i.m., twice daily, for 7-10 days.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 30/77
GENTAMICIN -It was obtained from
Micromonospora purpurea .
It is more potent, it has a broader
spectrum of action (comparing with
streptomycin); it is effective against Ps.
Aeruginosa, and most strains of proteus,E.coli, Klebsiella, Enterobacter, Serratia. It is
also active against staph.
Clinical uses:
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 31/77
Clinical uses:
- preventing and treating respiratory infections in critical ill
patients/ in those with impaired host defence; It is often
combined with a penicillin or a cephalosporin;
-pseudomonas, proteus and klebsiella infections: burns, urinary
tract infections, pneumonia, lung abscesses, osteomyelitis,
septicaemia ;It may be combined with a penicillin
(piperacillin) or a cephalosporin;
-endocarditis due to viridans streptococci or enterococci ;
-meningitis caused by gram negative bacilli;
- middle ear infections, infected burns, wounds, conjunctivitis
with sensitive germs-topically (creams, ointments, solutions);
-gentamicin –PMMA (polymethyl methacrylate) chains is a new
drug delivery system for use in osteomyelitis. Implanted in
the bone cavity after thorough removal of sequestra and left
in place for 10 days, it has achieved high cure rates.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 32/77
Adverse effects: -nephrotoxicity ;-vestibular toxicity.
Dose:The dose of gentamicin must be precisely calculatedaccording to body weight and level of renal function.
The daily dose of gentamicin (and otheraminoglycosides) should be reduced in patients withimpaired renal function according to measuredcreatinine clearance.
For an average adult with normal renal function 3-5 mg/ kg/ day, i.m., either as single dose or divided inthree 8 hourly doses is recommended. Parenteralgentamicin is available as vials: 20, 60, 80, 240 mg per
vial.For topical use: 0,3 % eye / ear drops, 0,1 %skin
cream.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 33/77
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 34/77
KANAMYCINE- It was obtained from
streptomyces kanamycetus.
It is more toxic, both to the cohlea and to
kidney.Hearing loss is more common than
vestibular disturbance. It is ocassionally used
as a second line drug in resistant tuberculosis.
It is administered i.m., usual dose 0,5 g
i.m. Today parenteral use has been largely
replaced. It may be used topically.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 35/77
TOBRAMYCIN- It was obtained from
Streptomyces tenebrarius.
It should be used only as a reserve
alternative to gentamicin.
Serious infections caused by pseudomonas
and proteus are its only current indications.
Ototoxicity and nephrotoxicity - lower than
gentamicin.
It is administered i.m., usual dose 3-5mg/kg in 1-3 doses.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 36/77
AMIKACIN
It has the widest spectrum of activity, includingmany organisms resistant to other aminoglycosides(because it is resistant to bacterial aminoglycosideinactivating enzymes). However, relatively higherdoses are needed for pseudomonas, proteus andstaph. infections.
It is recommneded as a reserve drug for hospitalacquired gram negative bacillary infections wheregentamicin or tobramycin resistance is high.
More hearing loss than vestibular disturbanceoccurs in toxicity.
It is administered parenterally.
NEOMYCIN
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 37/77
NEOMYCIN -obtained from Streptomyces
fradiae.Neomycin is highly toxic to the internal ear(mainly auditory)
and to kidney. It is therefore not used systematically. It is poorlyabsorbed from the gastrointestinal tract.Oral and topicaladministration does not ordinarily cause systemic toxicity.
Clinical uses:
-topically (often in combination with polymyxin, bacitracin,glucocorticosteroids) for infected wounds, ulcers, burn, external earinfections, conjunctivitis ;
-orally for:
-preparation of bowel before surgery: may reducepostoperative infections;
-hepatic coma: neomycin by suppressing intestinal flora
diminishes NH3 production and lowers its blood level; however,because of toxic potential it is infrequently used for this purposeand lactulose is preferred.
-intestinal infections with sensitive germs.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 38/77
Adverse effects:
-applied topically neomycin has low sensitizing potential,however rashes do occur;
-oral neomycin has a damaging effect on intestinal villi –prolonged treatment can induce malabsorbtion
syndrome ; also, due to marked suppression of gutflora, superinfection by candida can occur.
Preparations, doses:• Neomycine sulphate, 350, 500 mg; 0,3 % skin
ointment; 0,5 % skin cream; 0,5% eye ointment.
• Neosporin: neomycin 3400 IU+ polymyxin 5000IU+bacitracin 400 IU / g ointment
• Neosporin-H: neomycin 3400 IU+ polymyxin 10.000IU+hydrocortisone 10 mg / ml ear drops.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 39/77
NETILMICIN
It has a broader spectrum of activity thangentamycin. It is relatively resistant toaminoglycoside inactivating enzymes and thuseffective against many gentamicin resistant strains.
It is more active against Klebsiella, Enterobacter,Staphylococci, but less active against pseudomonas.
It is preferred in critically ill and neutropenicpatients, and retain activity in hospitals where
gentamicin resistance has spread.It is ototoxic.
It is administered parenterally.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 40/77
SPECTINOMYCIN
• -aminocyclitol antibiotic that is structurally
related to AMG;
• -it is used almost solely as an alternative
treatment for drug resistant gonorrhoea or
gonorrheae in penicillin allergic patients.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 41/77
ANTITUBERCULAR DRUGS
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 42/77
TBC: a chronic disease caused byMycobacterium tuberculosis.
It’s chronicity is due to:
-the intracellular location of mycobacteria;
-the slow rate of multiplication of thegerm;
-the resistance develops quickly ;
-there are atypical forms of Koch bacillus,which have a low susceptibility to drugs.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 43/77
Classification of antitubercular drugs:
I: MAJOR / FIRST LINE ANTI – TBC DRUGS:
-they are very active;
-they have the greatest efficacy;
-they are frequently used.
Streptomycin (S), Isoniazid (H), Rifampin (R), Ethambutol (E),Pyrazinamide (Z).
II. MINOR / SECOND LINE DRUGS: -they are less efficacious;
-they are less used;
-they are more toxic.
-they are used only when first line antitubercular drugs areineffective (BK is resistant) or are contraindicated.
Ethionamide, Paraaminosalicyloc acid, cycloserine,capreomycine, ciprofloxacin, ofloxacin, kanamycin, amikacin,clarithromycin.
/
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 44/77
I. MAJOR / FIRST LINE ANTI – TBC
DRUGS:
a)Isoniazide(isonicotinic acid hydrazide, H)
It is the hydrazide of isonicotinic acid.
It is a synthetic compound, strucurally
related to vitamine B6 (pyridoxine).
Mechanism of action: inhibition of synthesis
of mycolic acids which is the unique fatty acid
component of mycobacterial cell wall.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 45/77
Pharmacokinetics: It is completely
absorbed orally and penetrates all body
tissues, tubercular cavities, placenta andmeninges. It enters intracellularly. It is
extensively metabolized in the liver by
acetylation and metabolites are excreted inthe urine. The rate of acetylation shows
genetic variation: there are either fast
acetylators and slow acetylators. Importance:some adverse effects are more common in
slow acetylators (e.g. peripheral neuritis).
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 46/77
Clinical uses:
*it is an essential component of all antitubercular
regimens, unless the patient is not able totolerate it or bacilli are resistant.
• It is indicated in all types of TBC (pulmonary andextrapulmonary), only in combination with other
antitubercular drugs.• Exception: when used in prophylaxis of TBC,
when it is used alone.
•
Usual dose: 5 mg/kg/ day (300mg /day, for anadult), once daily or 10 mg/kg/day, 3 days fromone week. It is available as tablets.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 47/77
Adverse effects:
-hepatotoxicity ;
-peripheral neuritis (paresthesias) and a varietyof neurological manifestations (euphoria,mental disturbances, rarely convulsions) – dose-dependent toxic effects.
These are due to interference with utilizationof pyridoxine and its increased excretion inurine. Pyridoxine given prophylactically (10
mg/ day) prevents neurotoxicity.Izoniazideneurotoxicity is treated by pyridoxine 100mg/day.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 48/77
b)Rifampin (Rifampicin, R)
It is a semisynthetic derivative of
rifamycin B obtained from Streptomycesmediterranei.
It is bactericidal to mycobacterium
tuberculosis and many other gram + and
– bacteria like staph. aureus, N.
Meningitidis, H. Infl., E.coli, Klebsiella,
Pseudomonas, Proteus, legionella,
Mycobacterium leprae.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 49/77
Mechanism of action: Rifampin inhibits DNA
dependent RNA synthesis. It enters intracellularly.
Clinical uses:- treatment of tuberculosis only in association with
other drugs; usual dose: 10 mg/kg/day, or 600
mg/day, daily; it is available as capsules, tablets.-other clinical uses: leprosy, prophylaxis of
meningococcal and H. Infl. Meningitis and carrier
state; treatment of serious staphylococcal
infections (osteomyelitis etc.); brucellosis etc.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 50/77
Adverse effects:
-hepatotoxicity(hepatitis) ;
-urine and secretions (tears, sweat, contact lenses) maybecome orange-red;
-„ flu-like syndrome” –with chills, fever, headache,malaise and bone pain;
-it is an enzymatic inducer –enhances its own
metabolism, as well as that of many drugs includingwarfarin, oral contraceptives, corticosteroids etc.
-„ cutaneous syndrome” –flushing, pruritus, rash(specially on face and scalp), redness and watering of eyes.
-"abdominal syndrome” –
nausea, vomiting, abdominalcramps with or without diarrhoea.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 51/77
c) Ethambutol (E) It is a synthetic compound. It is selectively
tuberculostatic.
It is distributed widely but penetrates meningesincompletely and is temporarily stored in red bloodcells.
Clinical uses: TBC in association with other antitubercular
drugs ; usual dose: 15-20 mg/kg/day, daily, or 1000 mg/ day, daily.It is available as tablets.
Adverse effects:
-optic neuritis with loss of visual acuity / colour vision (itis reversible); ophthalmologic control is obligatorybefore, during and after treatment with ethambutol;
-nausea, rashes, fever, are infrequent.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 52/77
d) Streptomycin(S)
It is an aminoglycoside.
It is tuberculocidal but less effective thanisoniazid or rifampin.
It acts only on extracellular bacilli.
It penetrates tubercular cavities, but does
not cross to the CSF and has poor action in acidicmedium. Resistance developed rapidly when Swas used alone in tuberculosis. It is used only incombination with other drugs.
Adverse effects: vestibulotoxic; pain at thesite of i.m. injection. Usual dose: 15 mg/kg/day,daily(1000 mg/day), i.m.
) P i id (Z)
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 53/77
e) Pyrazinamide(Z) It is chemically similar to isoniazid. It is weaklytuberculocidal but more active in acidic medium.
Clinical uses: TBC in association. It is highly effective duringthe first 2 months of therapy when inflammatory changesare present. It is highly lethal to intracellularly locatedbacilli as well as to those at sites showing an inflammatoryresponse (pH is acidic at both of these locations).
Usual dose: 25-30 mg/kg/day, daily (1000 mg/day).It isavailable as tablets.
Adverse effects:
-hepatotoxicity;
-hyperuricemia is due to inhibition of uric acid secretion in
kidney; gout can occur.-rashes, fever, arthralgias etc.
II MINOR / SECOND LINE DRUGS
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 54/77
II. MINOR / SECOND LINE DRUGS
a) Ethioamide(Etm) - moderate efficay;it is seldom used (only in case of
resistance to better tolerated drugs); resistancedevelops rapidly.
-it acts on both intra- and extracellular bacteria.-atypical mycobacteria are sensitive;
Adverse effects:
• -anorexia, nausea, abdominal upset, vomiting;
• -aches, pains, rashes;• -hepatitis;-peripherasl or optic neuritis, mental
disturbances.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 55/77
b) Para-amino salicylic acid(PAS)
-PAS is tuberculostatic and one of the least
active drugs;
-patient acceptability of PAS is poor because of
frequent anorexia, nausea and epigastric pain.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 56/77
c) Cycloserine(Cys) -it is an antibiotic obtained from Streptomyces
orchidaceus; it inhibits bacterial cell wall synthesis;
-it is tuberculostatic and inhibits some other gr+ bacteria,E. Coli, Chlamydia also;
Adverse effects:
-CNS toxicity:sleepiness, headache, tremor and psychosis;
convulsions may be prevented by pyridoxine 100mg/day;
It is rarely used only in resistant cases.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 57/77
d) Amikacin, Kanamycin, Capreomycin -reserve
drugs in rare cases not responding to the
usual therapy, or infection by atypical
mycobacteria.They are toxic antibiotics (oto-and nephrotoxicity).
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 58/77
*Newer drugs
e) *Ciprofloxacin, Ofloxacin, Moxifloxacin,Spartfloxacin= fluorchinolones
• They are used in multidrog resistanttuberculosis and mycobacterium aviumcomplex infection in HIV patients.
f)*Clarithromycin, azithromycin –
macrolidesactive against mycobacterium avium complexand other atypical mycobacteria.
TREATMENT OF TUBERCULOSIS
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 59/77
TREATMENT OF TUBERCULOSIS
The treatment is followed under the Revised nationaltuberculosis controll programme.It is a long –term therapy.
General principles:
-drug combinations are used (a combination of two or more
drugs must be used) to reduce the incidence of resistance;-conventional regimens are used: duration of the treatment is 6-
8 months with:
-an initial intensive phase lasting 2-3 months, with dailyadministration of drug combinations (4-5 antitubercular
drugs),- it is followed by a continuation phase lasting 4-6
months, when 2 antitubercular drugs are given, thrice weekly;
-sputum examintion.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 60/77
Chemoprophylaxis:
It is indicated in: -contact with active TBC;
-neonate of tubercular mother;
-patients with old inactive disease who are assessed to have
received inadequate therapy;-children with a TB patient in the family;
-patients of leukemia, diabetes, silicosis, or those who are HIVpositive, or are on corticosteroid therapy.
The drug generally used has been isoniazid 300 mg, daily for
6-12 months. Now because of high incidence of resistance,a combination of isoniazid (5 mg/kg)+rifampin (10 mg/ kg)given for 6 months is preferred.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 61/77
TREATMENT OF LEPROSY
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 62/77
Leprosy is a chronic granulomatous
infection caused by Mycobacterium leprae ;
primarily affecting skin , mucous membranes
and nerves.It is more prevalent among thelowest socio-economic strata.
CLASSIFICATION OF DRUGS USED IN
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 63/77
CLASSIFICATION OF DRUGS USED IN
LEPROSY:
1)Sulfone: DAPSONE
2)Phenazine derivatives: CLOFAZIMINE
3)Antitubercular drugs: RIFAMPIN,
ETHIONAMIDE
4)Other antibiotics: OFLOXACINE,
CLARITHROMYCIN, MINOCYCLINE.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 64/77

7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 65/77
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 66/77
Resistance to dapsone:
*it may be primary –in untreated patients , i.e.
they have acquired infection from a patient
harbouring resistant bacilli or
* secondary which develops during therapy in
an individual patient with a single drug.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 67/77
Pharmacokinetics:
Dapsone is completely absorbed after oraladministration and is widely distributed in the bodythough penetration is CSF is poor. It is 70% plasma
protein bound , but more importantly concentrated inskin ( specialy lepromatous skin) , muscle, liver andkidney.It is metabolized in the liver ; metabolites areexcreted in bile and reabsorbed from intestine and
finally they are excretd in urine.The drug is cumulativedue to retention in tissues and enterohepaticcirculation. Elimination takes 1-2 weeks or longer.
Adverse effects:
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 68/77
Adverse effects:
-well tolerated at doses of 100 mg/day or less;
-gastric intolerance in the beginning ; it decreases
later;-mild haemolytic anemia is comon( dose related
toxicity);patients with glucoso-6-PD deficiencyare more susceptible;
-cutaneous reactions: allergic rashes, drugeruption, phototoxicity etc.
-lepra reaction ( it is a Jarish Herxheimer type of reaction due to release of antigens from the
killed bacilli; it may be mild, severe or lifethreatening –erythema nodosum leprosum).
CLOFAZIMINE
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 69/77
CLOFAZIMINE
-it is a substance with leprostatic and
antiinflammatory properties;
-it acts by interfering with function of DNA;
-when used alone resistance develops in 1-3
years;
-it is administered orally ; it is well distributed in
many tissues but entry in CSF is poor.
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 70/77
Adverse effects: in usual doses it is well tolerated;*skin: reddish –black discolouration of skin,especially on exposed parts;discolouration of hairand body secretions may also occur;
*gastrointestinal symptoms: enteritis withnausea, abdominal pain, anorexia , weight lossparticularly when higher doses are used tocontrol lepra reaction;
*clofazimine should be avoided during earlypregnancy and in patients with liver or kidneydamage.
RIFAMPIN
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 71/77
RIFAMPIN
-bactericidal to M. Leprae;
-upto 99.99% M. Leprae are killed in 3-7 days;
-however, it is not satisfactory if used alone –
resistance develops.
-it has been included in the multidrug therapy
of leprosy and shortens duration of
treatment.
-600 mg once a month.
ETHIONAMIDE
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 72/77
ETHIONAMIDE
-it has significant antileprotic activity but causes
hepatotoxicity;
-it should be used ( 250 mg / day) only when
absolutely necessary.
OTHER ANTIBIOTICS:
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 73/77
OTHER ANTIBIOTICS:OFLOXACIN, PEFLOXACIN, SPARTFLOXACIN
- are highly active against M. Leprae
OFLOXACIN:
-over 99.99% bacilli were found to be killed by22 daily doses of ofloxacin monotherapy;
-however, it is not included in the standardtreatment protocols but can be used inalternative regimens in case rifampin cannotbe used or to shorten the duration of treatment.
-dose: 400 mg/day.
MINOCYCLIN:
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 74/77
MINOCYCLIN:
-its antibacterial activity is much less than that
of rifampin but greater than that of
clarithromycin;
-in doses of 100 mg/day it may be used inalternative multidrug therapy of leprosy.
CLARITHROMYCIN:
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 75/77
CLARITHROMYCIN:
-it is the only macrolide antibiotic with
significant activity against M. Leprae;
-however, it is less bactericidal than rifampin;
-monotherapy with clarithromycin 500 mg daily
causes 99.9% bacterial killing in 8 weeks;
-it is being included in alternative multidrug
therapy of leprosy.
TREATMENT OF LEPROSY
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 76/77
TREATMENT OF LEPROSY
-conventionally , all forms of leprosy had been treatedwith dapsone alone ( monotherapy), 100-200 mg daily, 5 days a week, duration of treatment depending onthe type ( 5-12 years or life long) ; monotherapy is no
longer used because of emergence of resistance;-to deal with dapsone resistant strains of M.leprae and
the problem of microbial persisters ( dormant forms),multidrug therapy with dapsone, rifampin and
clofazimine was introduced in 1981.Multidrug therapyis the regimen of choice for all cases of leprosy.
-alternative regimens incorporating newer antileprotic
7/30/2019 Linc Osami Des
http://slidepdf.com/reader/full/linc-osami-des 77/77
alternative regimens incorporating newer antileproticdrugs are now investigated ; these should be used onlyin cases of rifampin resistance or when it is impossible
to employ the standard multidrug therapy.Somealtrenative regimens are :
* clofazimine 50 mg+ ofloxacine 400 mg/minocycline 100 mg/ clarithromycin 500 mg , daily for
6 months followed by clofazimine 50 mg+ ofloxacine400 mg/ minocycline 100 mg daily for additional 18months.
*in some cases having few bacteria in the body
and only one skin lesion : a single dose of rifampin 600mg +ofloxacin 400 mg+ minocycline 100 mg.
Many other shorter regimens are under evaluation.











![구두파티 - 국민대학교 LINC+사업단linc.kookmin.ac.kr/wp-content/uploads/2018/01/7.issue-6.pdf · 국민대학교 LINC 사업단 뉴스레터 [ Issue 06] 염천교 수제화](https://static.fdocument.pub/doc/165x107/5f0e795f7e708231d43f6bf6/eeoeoe-eeeoee-lincelinc-eeeoee-linc-e.jpg)