L’état des connaisances sur la recherche en transfert des connaissances Jeremy Grimshaw MBChB,...
38
L’état des connaisances sur la recherche en transfert des connaissances Jeremy Grimshaw MBChB, PhD, FRCGP, FCAHS Clinical Epidemiology Program, OHRI Department of Medicine, University of Ottawa Canada Research Chair in Health Knowledge Transfer and Uptake
-
Upload
selina-hovell -
Category
Documents
-
view
212 -
download
0
Transcript of L’état des connaisances sur la recherche en transfert des connaissances Jeremy Grimshaw MBChB,...

L’état des connaisances sur la recherche en transfert des connaissances
Jeremy Grimshaw MBChB, PhD, FRCGP, FCAHSClinical Epidemiology Program, OHRI
Department of Medicine, University of OttawaCanada Research Chair in Health Knowledge Transfer and Uptake

Knowledge translation
CIHR definition• Knowledge translation is a dynamic and iterative process
that includes the synthesis, dissemination, exchange and ethically-sound application of knowledge to improve the health of Canadians, provide more effective health services and products and strengthen the healthcare system.
• This process takes place within a complex system of interactions between researchers and knowledge users which may vary in intensity, complexity and level of engagement depending on the nature of the research results and on the needs of the particular knowledge user.

Knowledge translation
• Knowledge translation is about ensuring that:• stakeholders are aware of and use research
evidence to inform their decision making• research is informed by current available
evidence and the experiences and information needs of stakeholders
• End point of knowledge translation to health care professionals should be evidence based behaviours

Approaches to knowledge translation
Knowledge to action
Graham et al (2006). Lost in Knowledge Translation. Time for a Map? Journal of Continuing Education for Health Professionals

• Structural (e.g. financial disincentives)
• Organisational (e.g. inappropriate skill mix, lack of facilities or equipment)
• Peer group (e.g. local standards of care not in line with desired practice)
• Individual (e.g. knowledge, attitudes, skills)
• Professional - patient interaction (e.g. problems with information processing)
Assessing barriers to KT

Selecting knowledge translation interventions
• Choice of dissemination and implementation should be based upon:• ‘Diagnostic’ assessment of barriers• Understanding of mechanism of action of
interventions• Empirical evidence about effects of interventions• Available resources• Practicalities, logistics etc

Cochrane Effective Practice and Organisation of Care (EPOC) Group
• EPOC aims to undertake systematic reviews of professional, organisation, financial and regulatory interventions to improve health care systems and health care delivery
• Register of 6000+ primary studies• 50 reviews, 41 protocols

http://www.cadth.ca/index.php/en/compus/optimal-ther-resources/interventions

Overview of reviews of professional behaviour change strategies
• Educational materials• Educational meetings• Educational outreach• Local opinion leaders• Audit and feedback• Reminders and prompts• Tailored interventions• Multifaceted interventions

Educational outreach
• Educational outreach - Use of a trained person who met with providers in their practice settings to give information with the intent of changing the provider’s practice. The information given may have included feedback on the performance of the provider(s).

Educational outreach
• Derives from social marketing approach• Use social persuasion methods to target
individual’s knowledge and attitudes• Typically aim to get maximum of 3 messages
across in 10-15 minutes using approach tailored to individual health care provider
• Typically use additional strategies to reinforce approach
• Typically focus on relatively simple behaviours in control of individual physician eg choice of drugs to prescribe

Educational outreach
O’Brien (2007) Cochrane Library• High quality review• 69 studies (RCT, CCT)• Multifaceted educational outreach visits were
generally effective for improving appropriate care• Prescribing behaviours - median effect across 17
comparisons 4.8% absolute improvement, interquartile range 3.0% to 6.5%
• Other behaviours – median effect across 17 comparisons 6.0% absolute improvement, interquartile range 3.6% to 16.0%

Overview of reviews summary
Summary• Variety of interventions to change health
professional behaviour – effects tend to be modest but important from population perspective
• However ‘No Magic Bullets’ – effects of interventions appears to vary across targeted behaviours, professionals and settings
• Feasibility and resources required for interventions also likely to vary

Knowledge translation research
• Knowledge translation is a human enterprise that can be studied to understand and improve knowledge translation approaches
• Knowledge translation research is the scientific study of the determinants, processes and outcomes of knowledge translation.
• Goal is to develop a generalisable empirical and theoretical basis to optimise KT activities

Knowledge translation research
• Knowledge translation research relatively new field in health research
• Inherently interdisciplinary
• Wide range of disciplines need to be engaged
• Clinical
• Health services research
• Educational, behavioural and organisational
• Design and engineering
• Methodologists
• Broad range of forms of enquiry needed

Knowledge translation research
• Knowledge synthesis (to identify the knowledge for KT); • Research into the evolution of and critical discourse around
research evidence; • Research into knowledge retrieval, evaluation and knowledge
management infrastructure;• Identification of knowledge to action gaps;• Development of methods to assess barriers and facilitators to
KT;• Development of the methods for optimizing KT strategies;• Evaluations of the effectiveness and efficiency of KT strategies;• Development of KT theory; and• Development of KT research methods.

Knowledge translation research
• Knowledge synthesis (to identify the knowledge for KT); • Research into the evolution of and critical discourse around
research evidence; • Research into knowledge retrieval, evaluation and knowledge
management infrastructure;• Identification of knowledge to action gaps;• Development of methods to assess barriers and facilitators to
KT;• Development of the methods for optimizing KT strategies;• Evaluations of the effectiveness and efficiency of KT strategies;• Development of KT theory; and• Development of KT research methods.

UK MRC Framework for Evaluating Complex Interventions
Diagnostic Modelling Exploratory trial Definitive RCT Long termimplementation
Pre-clinical
Phase I
Phase II
Phase III
Phase IV
Continuum of increasing evidence

UK MRC Framework for Evaluating Complex Interventions – Diagnostic Phase
• Formal assessment of context, likely barriers to KT
• Consideration of potential theories (behavioural, organisational) that might be helpful
• Mixed methods
• Literature review
• Informal consultation
• Focus groups
• Surveys
• Needs interdisciplinary perspective

UK MRC Framework for Evaluating Complex Interventions – Diagnostic Phase
• Ferlie and Shortell suggest four levels of interventions to improve the quality of health care: • the individual health professional; • health care groups or teams; • organisations providing health care; • the larger health care system or environment in
which individual organizations are embedded. • Different types of theory will be relevant to
interventions at different levels Ferlie, Shortell (2001). Milbank Quarterly

UK MRC Framework for Evaluating Complex Interventions – Diagnostic Phase
• Given that clinical practice is a form of human behaviour, we are currently exploring the applicability of predictive theories of human behaviour from other similar settings.
• Focus has been on theories that:• (Have standard approaches to measurement)• Have been empirically tested.• Explain behavior in terms of factors that are
amenable to change.• Include non volitional factors.

UK MRC Framework for Evaluating Complex Interventions – Diagnostic Phase
Walker (2001) Br J Hlth Psych

UK MRC Framework for Evaluating Complex Interventions – Diagnostic Phase
Available from: http://www.rebeqi.org/

UK MRC Framework for Evaluating Complex Interventions – Diagnostic Phase
More theory, less theories needed• Multiple theories and frameworks of individual and
organizational behavior change.• Most professional behavior change frameworks are
descriptive and normative rather than predictive.• Few have been operationalised in detail• Many have not been prospectively evaluated.• Few head-to-head comparisons of different theories• Need for predictive theories that incrementally improve
likelihood of successful implementation.• Need for rigorous evaluation of candidate theories

UK MRC Framework for Evaluating Complex Interventions – Modelling Phase
Phase 1 – Modelling
• Intervention mapping• Specify intervention objectives• Select methods and strategies• Design program
• Usability testing

UK MRC Framework for Evaluating Complex Interventions – Modelling Phase
Intervention mapping

UK MRC Framework for Evaluating Complex Interventions – Exploratory Phase
Phase 2 – Exploratory studies• Small scale studies to demonstrate that
unit/patient recruitment is likely achievable, intervention is deliverable in study settings, data collection is feasible
• Randomised or non randomised

UK MRC Framework for Evaluating Complex Interventions – definitive phase
• Causal description – did our KT strategy lead to improve knowledge use
• Causal explanation – why did our KT strategy work/not work (understanding of mediating pathways)
• Economic evaluation• Understanding of potential effect modifiers (context,
targeted group, targeted behaviour, variations in intervention)
• Many current KT evaluations fail to address some or all of these issues

UK MRC Framework for Evaluating Complex Interventions – definitive phase
• Rigorous evaluations (mainly randomised controlled trials) provide the best evidence of causal description of different interventions because:• Effects of interventions are modest • Limited understanding of likely confounders• Substantial opportunity costs if ineffective or
inefficient dissemination and implementation strategies used

UK MRC Framework for Evaluating Complex Interventions – definitive phase
• Pragmatic largely cluster randomised trials are optimal design for establishing causal description.
• Design aspects can be used to enhance informativeness of RCTs• Multiple arm trials, factorial designs
• Policy friendly designs• Step wedge designs, balanced incomplete block designs
• However for logistical, pragmatic and ethical reasons, quasi experimental designs may be needed.

UK MRC Framework for Evaluating Complex Interventions – definitive phase
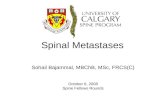
• Evaluated effects of short educational messages on test ordering reports and audit and feedback on subsquent test ordering behaviour
NEXUS
DRAM

Requests per 1000 patients
85.080.0
75.070.0
65.060.0
55.050.0
45.040.0
35.030.0
25.020.0
15.010.0
5.00.0
Requests for knee x-rays
Num
ber
of p
ract
ices
60
50
40
30
20
10
0
Std. Dev = 16.93
Mean = 15.8
N = 247.00
Your practice
Requests per 1000 patients
85.080.0
75.070.0
65.060.0
55.050.0
45.040.0
35.030.0
25.020.0
15.010.0
5.00.0
Num
ber
of p
ract
ices
60
50
40
30
20
10
0
Std. Dev = 16.93
Mean = 15.8
N = 247.00
Your practice
UK MRC Framework for Evaluating Complex Interventions – definitive phase

UK MRC Framework for Evaluating Complex Interventions – definitive phase

UK MRC Framework for Evaluating Complex Interventions – definitive phase
• NEXUS and DRAM short educational messages led to 15-30% reduction in subsequent test ordering
• NEXUS feedback – no effect• DRAM feedback – 10-15% reduction in subsequent test
ordering
• Take home messages• Simple (and cheap) interventions may lead to
improved professional behaviour• Minor changes in audit and feedback design may lead
to different results• Importance of replicating studies

UK MRC Framework for Evaluating Complex Interventions – definitive phase
• Other forms of enquiry needed to determine causal explanation• Process evaluations (qualitative case studies)• Theory based process evaluations (mediating
pathways)• Secondary analyses (moderator analyses)• Temporal analyses
• Embedded economic evaluations

Summary - KT
• Knowledge translation is about ensuring that stakeholders are aware of and use research evidence to inform their decision making
• Knowledge to action loop provides framework for thinking about knowledge translation
• Different approaches likely to be needed depending on innovation, barriers to adoption, targeted stakeholders and health care system
• Evidence base about how to do KT is incomplete especially for policy makers
• Nevertheless opportunities for researchers to be more thoughtful about KT throughout research process

Summary – KT research
• KT is a relatively new field - few health researchers have been engaged in the field for more than 10 years
• Substantive level of research activity• Cochrane Effective Practice and Organisation of Care
(EPOC) group register includes over 6,000 RCTs and quasi experiments of interventions to improve health care delivery and health care services
• Increasing funding and reporting opportunities for knowledge translation research
• Substantial challenges to establishing KT research as a distinct field

Contact details
• Jeremy Grimshaw
[email protected]• EPOC
http://www.epoc.uottawa.ca/index.htm• Implementation Science
http://www.implementationscience.com