LA TIMECTOMIA ROBOTICA - Eurac Research · LA TIMECTOMIA ROBOTICA Prof. Giuseppe Marulli UOC...
47
LA TIMECTOMIA ROBOTICA Prof. Giuseppe Marulli UOC Chirurgia Toracica – Università di Padova
Transcript of LA TIMECTOMIA ROBOTICA - Eurac Research · LA TIMECTOMIA ROBOTICA Prof. Giuseppe Marulli UOC...

LA TIMECTOMIA ROBOTICA
Prof. Giuseppe MarulliUOC Chirurgia Toracica – Università di Padova
…. The thymus presents a challenge to thesurgeon not only as a structure that may beorigin of benign and malignant neoplasms, butalso as a organ that is involved in fundamentalaspects of cellular immunity and neuromuscolarconduction …...
In Shields TW: General Thoracic Surgery, 1994, p.1770

RATIONALE FOR THYMECTOMY IN MG
The thymus may play a role in pathogenesis of myasthenia(possible source of antigen to drive this autoimmune disease)
Most patients with MG and autoantibodies directed against theacetylcholine receptor (AChR) have thymic abnormalities:hyperplasia is found in 60 to 70% and thymoma in 10 to 15%
The disease often improves or disappears after thymectomy(Blalock 1936)
Clagett (1949) …..
Keynes (1955) …..
Viets and Schwab (1960) …...
First thymectomy: Sauerbruch, 1911. Trans-cervical approach in patient with
myasthenia gravis (MG).
Thymectomy for thymoma: Blalock, 1936. Trans-sternal approach in 19 year old woman with
MG and thymoma.
SOME OF THE DIFFICULTIES IN STUDYING MG
MG IS AN UNCOMMON DISEASE THE NATURAL HISTORY IS UNPREDICTABLE THERE ARE SEVERAL VERSIONS OF CLINICAL CLASSIFICATION THE OUTCOMES ARE INFLUENCED BY: AGE, GENDER, TIMING OF
THYMECTOMY, UNDERLYING PATHOLOGY, Ab STATUS…. THERE ARE DIFFERENCES IN THE NEUROLOGIST’S PRACTICE. THERE IS LACK OF UNIFORM STANDARDS IN REPORTING
(THYMOMATOUS AND NON THYMOMATOUS MG). LACK OF RCT

INDICATIONS FOR THYMECTOMY AND SELECTION OF CANDIDATES
• AGE (15-50 yrs recommended)
• Ab STATUS (AntiAChR+ and antiMUSK - preferred)
• MG CLASS (Generalized MG – Ocular MG???)
• CLINICAL STATUS (Stable disease, no recent crisis)
•ONSET OF DISEASE (Early onset – before 12-24 months -associated withbetter results)
VINCENT A, 2010EFNS GUIDELINES, 2010
EXPECTED BENEFITS OF THYMECTOMY IN MG
- CLINICAL BENEFITS
(REMISSION-IMPROVEMENT OF SYMPTOMS)
- REDUCTION OF MEDICATIONS
(ADVERSE EFFECTS – COSTS)
- MINIMAL INVASIVENESS AND LOW COMPLICATIONS
(RISK-BENEFIT BALANCE)
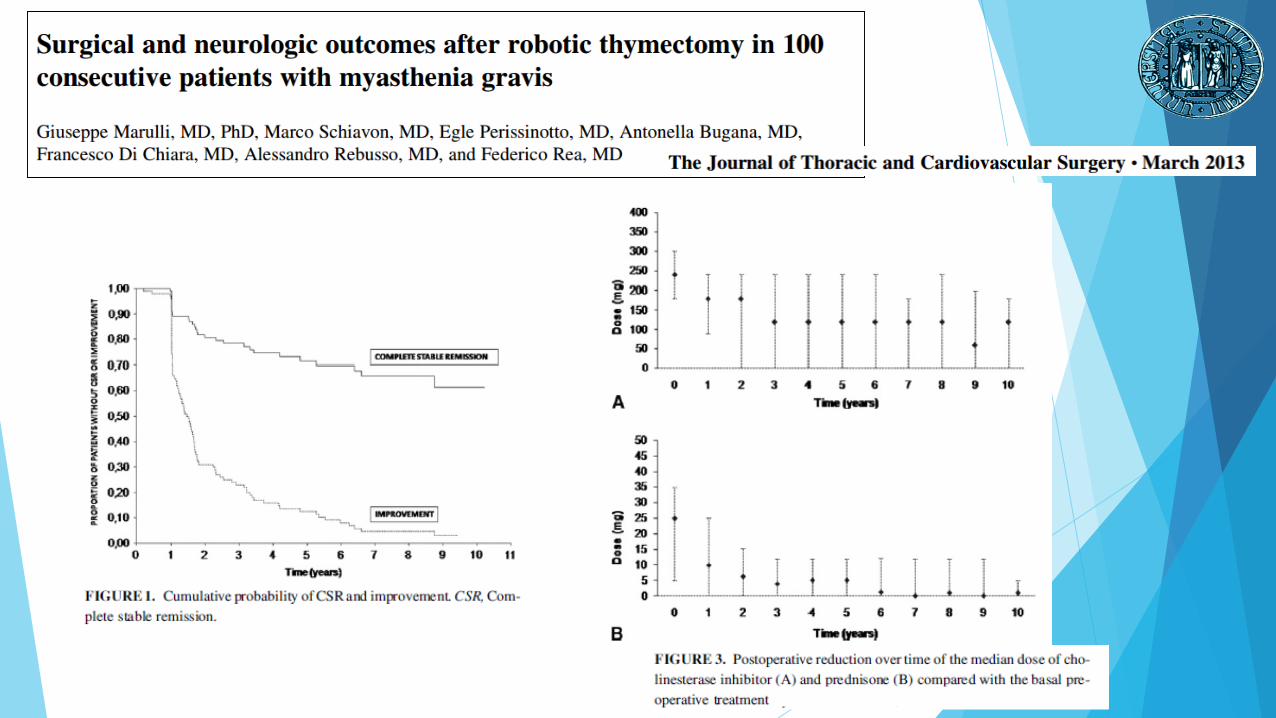
• MG patients undergoing thymectomy were more likely toachieve medication-free remission, become asymptomatic, andimprove than MG patients not undergoing thymectomy.• MG patients undergoing thymectomy were twice as likely to attain medication-free remission, 1.6 times as likely to becomeasymptomatic, and 1.7 times as likely to improve.
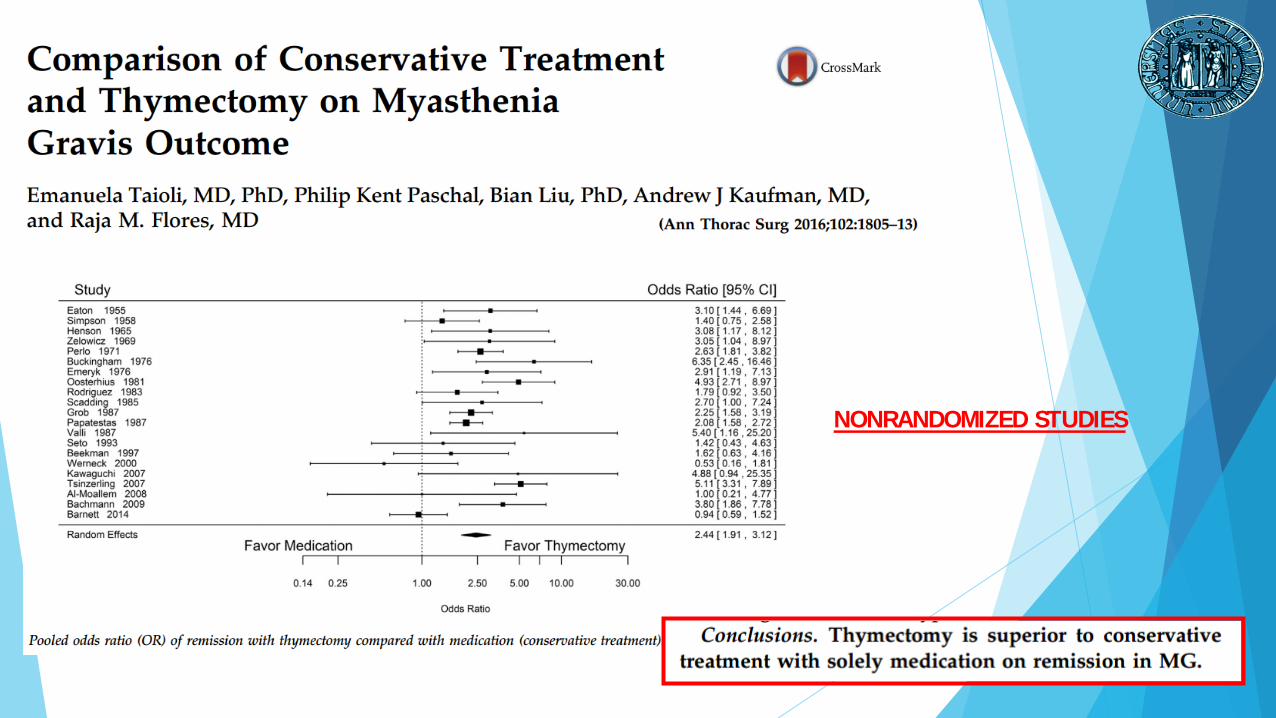
NONRANDOMIZED STUDIES
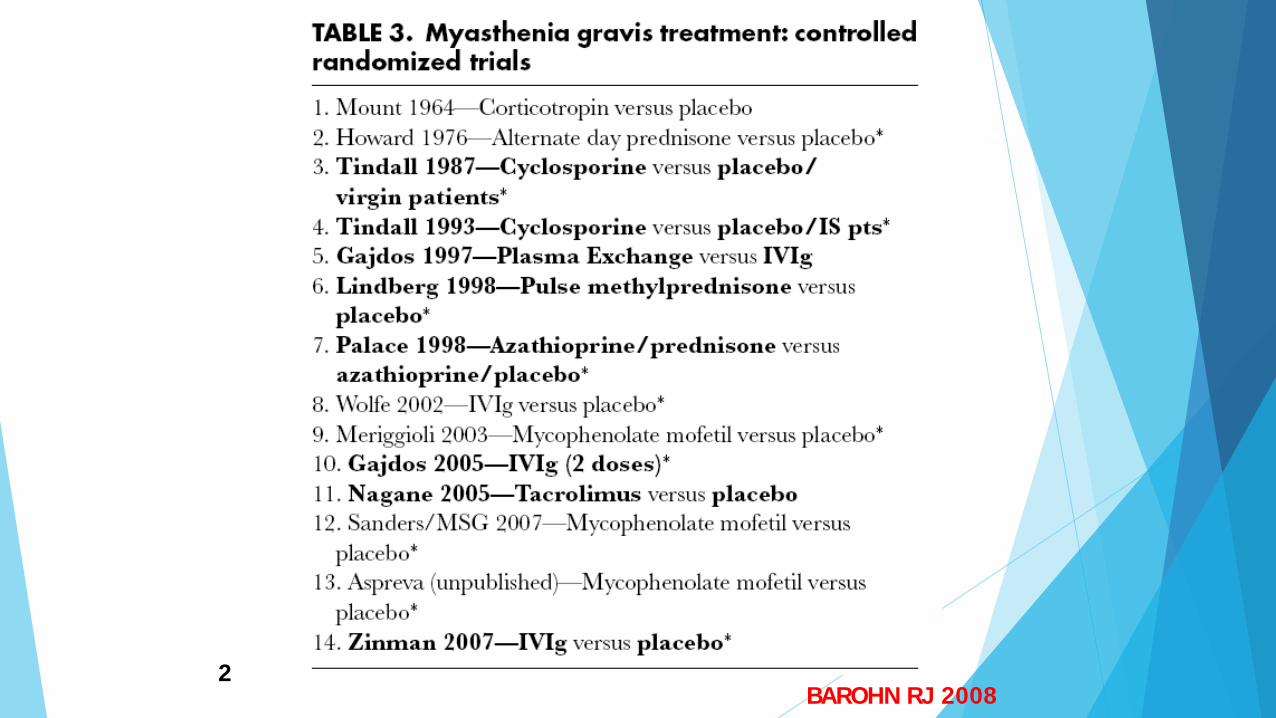
BAROHN RJ 20082

• The time-weighted average Quantitative Myasthenia Gravis score over a three-year period was significantly lower for the thymectomy group compared with the prednisone-alone group (6.15 versus 8.99, estimated difference 2.85, 95% CI 0.47-5.22).
• The average requirement for alternate-day prednisone over three years was significantly lower for the thymectomy group (44 versus 60 mg, estimated difference 16 mg, 95% CI 7-25).
• The proportion of subjects requiring immunosuppression with azathioprine was significantly lower for the thymectomy group (17 versus 48 percent, estimated difference 31 percent, 95% CI 16-47).
• The proportion of subjects hospitalized for MG exacerbations was significantly lower for the thymectomy group (9 versus 37 percent, estimated difference 28 percent, 95% CI 14-42).
• The proportion of subjects who achieved minimal manifestation status was significantly greater in the thymectomy group at 12 months (67 versus 37 percent) and at 36 months (67 versus 47 percent).
EXPECTED BENEFITS OF THYMECTOMY IN MG
- CLINICAL BENEFITS
(REMISSION-IMPROVEMENT OF SYMPTOMS)
- REDUCTION OF MEDICATIONS
(ADVERSE EFFECTS – COSTS)
- MINIMAL INVASIVENESS AND LOW COMPLICATIONS
(RISK-BENEFIT BALANCE)

REDUCTION OF MEDICATIONS
EXPECTED BENEFITS OF THYMECTOMY IN MG
- CLINICAL BENEFITS
(REMISSION-IMPROVEMENT OF SYMPTOMS)
- REDUCTION OF MEDICATIONS
(ADVERSE EFFECTS – COSTS)
- MINIMAL INVASIVENESS AND LOW COMPLICATIONS
(RISK-BENEFIT BALANCE)
MORBIDITY (5-20%)•WOUND HEALING DISORDERS
•STERNUM INSTABILITY
•HAEMORRAGE
•PHRENIC NERVE DAMAGE (2-3%)
•PNEUMONIA (8-10%)
•VENTILATORY SUPPORT (2-5%)
•TRACHEOSTOMY
MORTALITY • 5-15% BEFORE 1970
• < 1% AFTER 1970
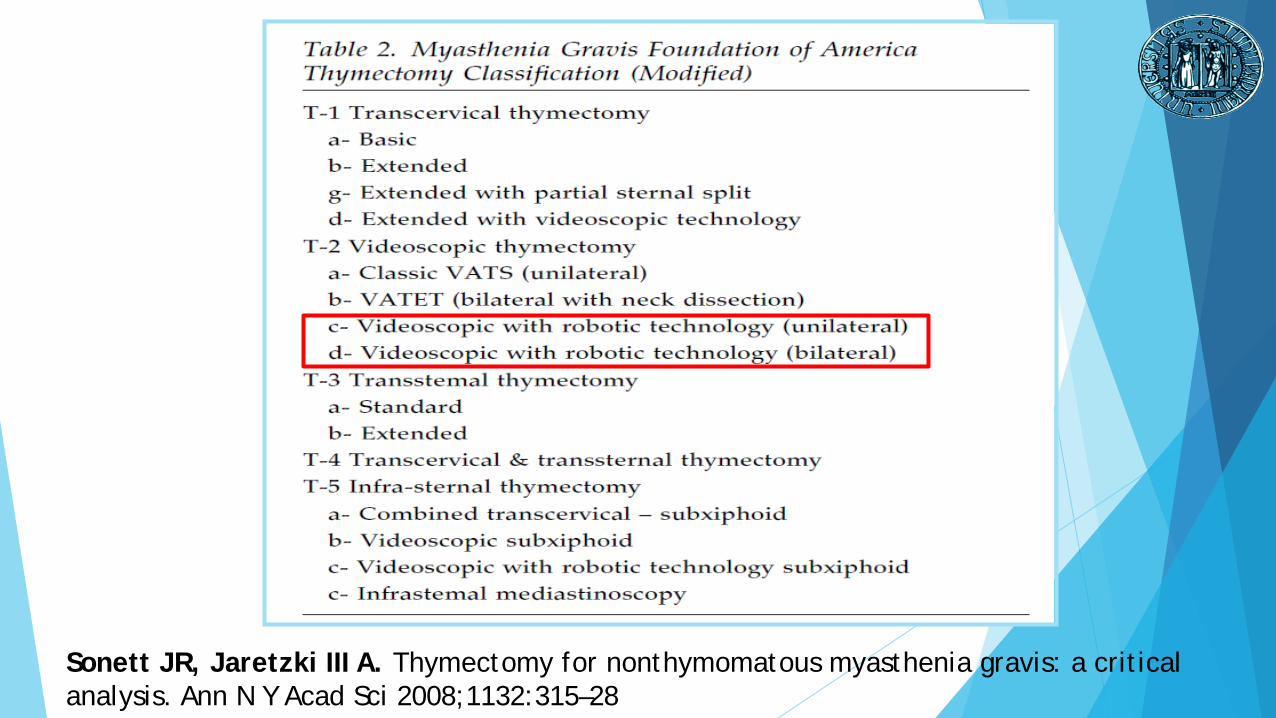
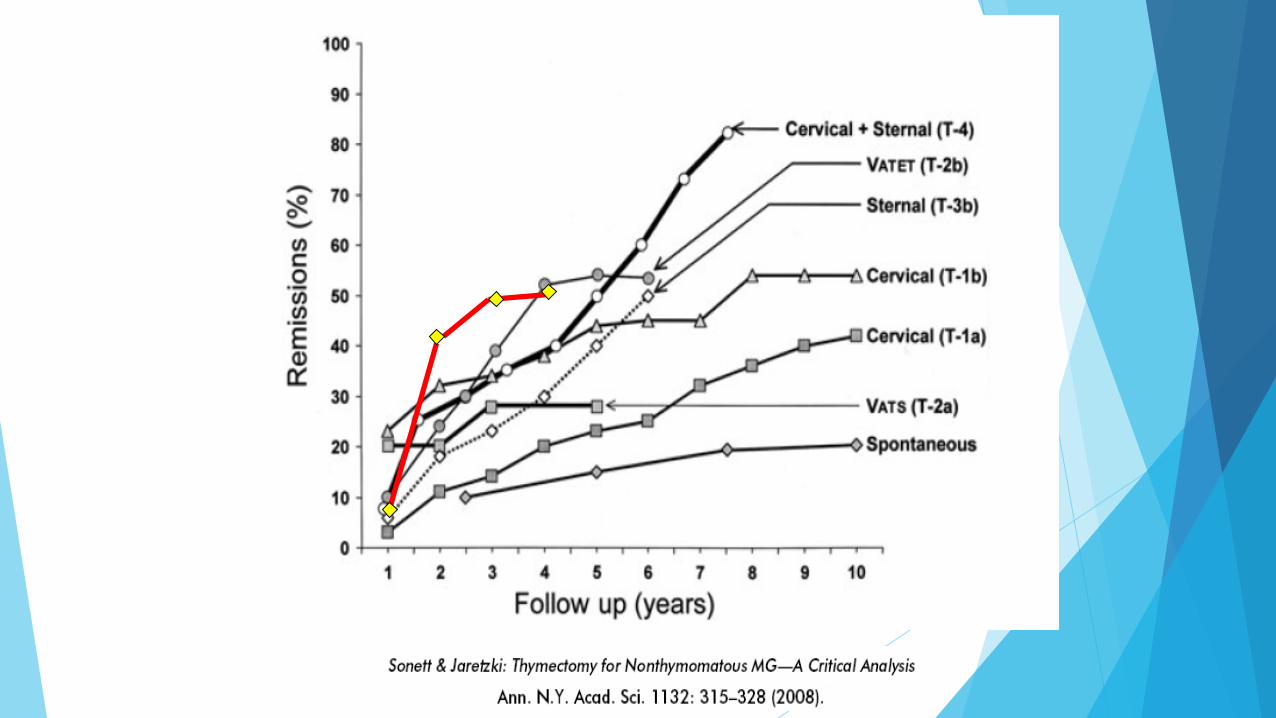
Sonett JR, Jaretzki III A. Thymectomy for nonthymomatous myasthenia gravis: a critical analysis. Ann N Y Acad Sci 2008;1132:315–28

Standard Sternal Extended Sternal Cervical & Sternal
Basic cervical Extended cervical VATS
?
?
?
(40-50%) (75-80%) (80-85%)
(98-100%)(85-95%)(70-80%)
EXTIMATED RESECTIONAL EXTENT OF THYMECTOMY TECHNIQUES

IT IS DIFFICULT TO COMPARE THE OUTCOMES OFTHE DIFFERENT OPERATIVE TECHNIQUES(CONFOUNDING FACTORS INFLUENCED BOTHTHE CONTROLLED AND THE UNCONTROLLEDSTUDIES) BUT OUTCOMES ARE PROBABLYSIMILAR (CLASS III EVIDENCE).
(Meyer et al., 2009)

IDEALLY, THE LESS INVASIVE SURGICAL TECHNIQUES ARE DESIRABLE, ASSUMING THE RESULTS ARE EQUIVALENT
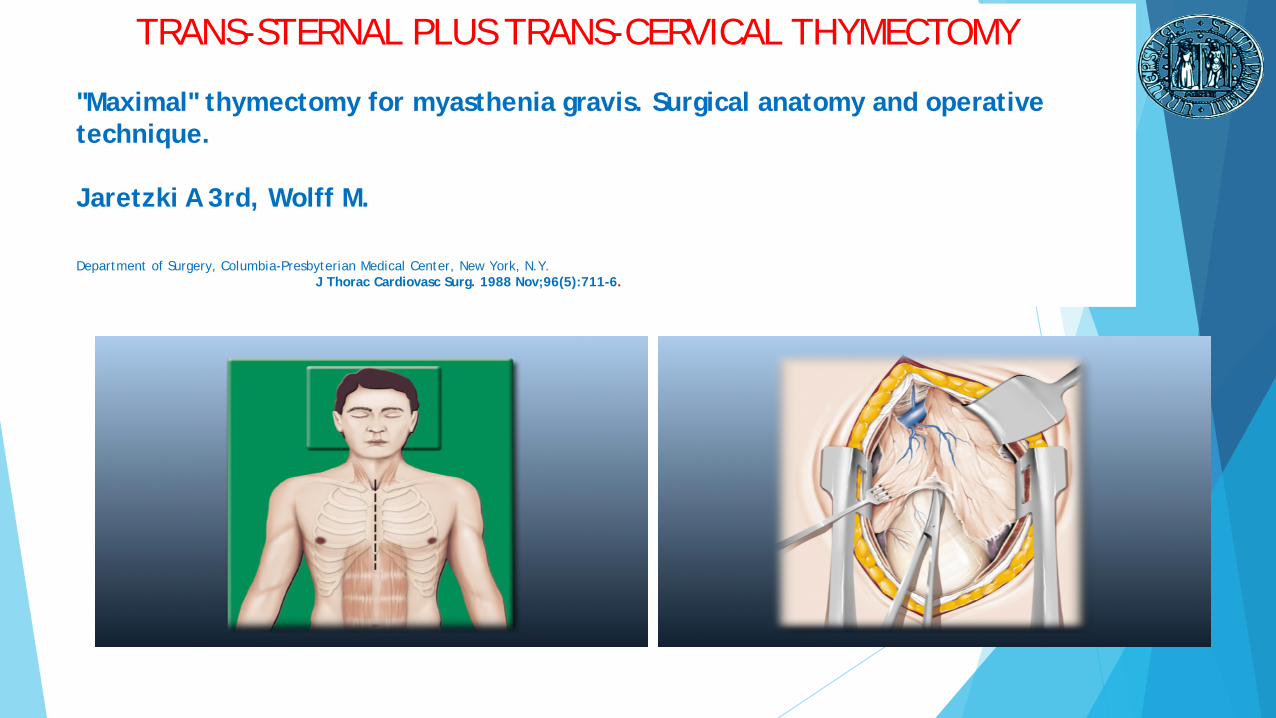
TRANS-STERNAL PLUS TRANS-CERVICAL THYMECTOMY
"Maximal" thymectomy for myasthenia gravis. Surgical anatomy and operative technique.
Jaretzki A 3rd, Wolff M.
Department of Surgery, Columbia-Presbyterian Medical Center, New York, N.Y. J Thorac Cardiovasc Surg. 1988 Nov;96(5):711-6.

ADVANTAGES
DISADVANTAGES
•Optimal exposition of the operative field
•Thymectomy easier and extended to the perithymic tissue
•Low probability of nervous and vascular injuries
•Invasive technique
•Longer hospitalization than minimally invasive techniques
•More complications
•Lesser acceptability by young patients

ADVANTAGES
DISADVANTAGES
•Minimally invasive technique
•Short hospitalization and low costs
•Optimal cosmetic results
•Easily accepted by young patients
•Minimal thoracic trauma and early improved lung function
•2-D view of the operative field
•Arms do not articulate making difficult the dissection of the neck and the access tothe contralateral mediastinum
•Needs in some cases, of a cervical incision
•Impossibility to perform an extended thymectomy (thymus plus perithymic tissues)

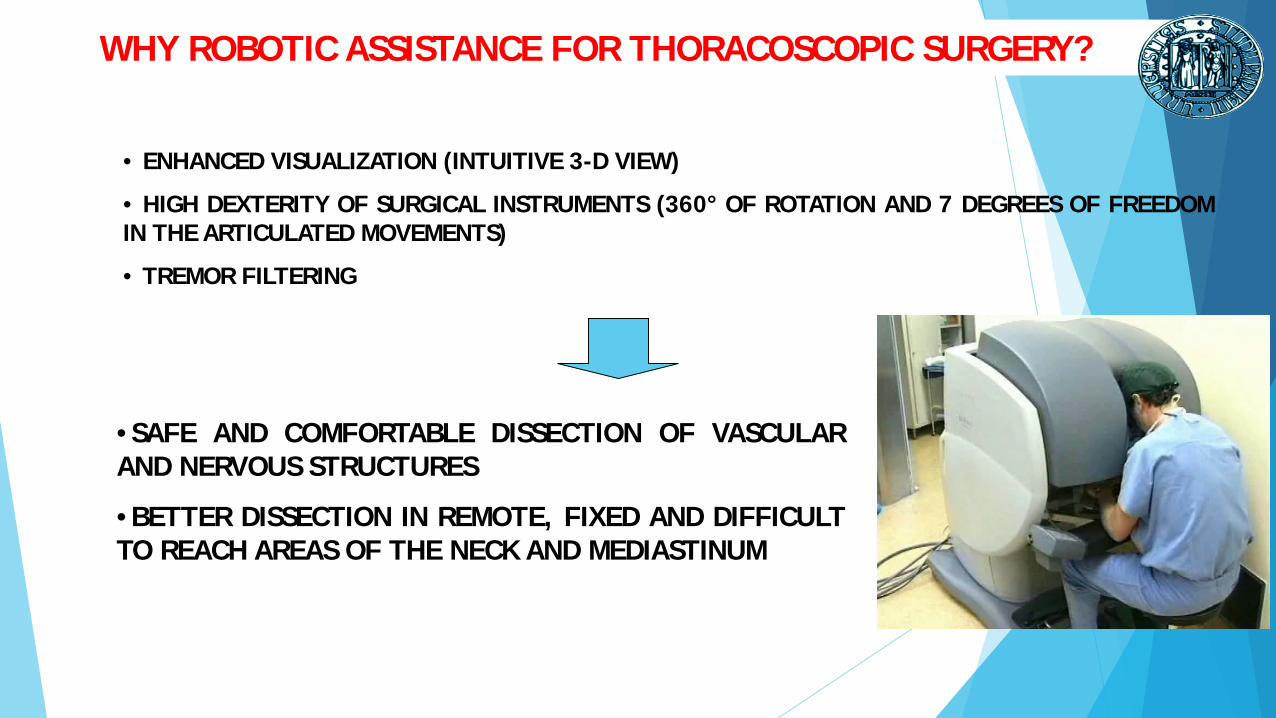
WHY ROBOTIC ASSISTANCE FOR THORACOSCOPIC SURGERY?
• ENHANCED VISUALIZATION (INTUITIVE 3-D VIEW)
• HIGH DEXTERITY OF SURGICAL INSTRUMENTS (360° OF ROTATION AND 7 DEGREES OF FREEDOMIN THE ARTICULATED MOVEMENTS)
• TREMOR FILTERING
•SAFE AND COMFORTABLE DISSECTION OF VASCULARAND NERVOUS STRUCTURES
•BETTER DISSECTION IN REMOTE, FIXED AND DIFFICULTTO REACH AREAS OF THE NECK AND MEDIASTINUM

Initial high costs
Early increased operative time (learning curve)
Absence of tactile feedback
DISADVANTAGES OF ROBOTIC THORACOSCOPIC THYMECTOMY

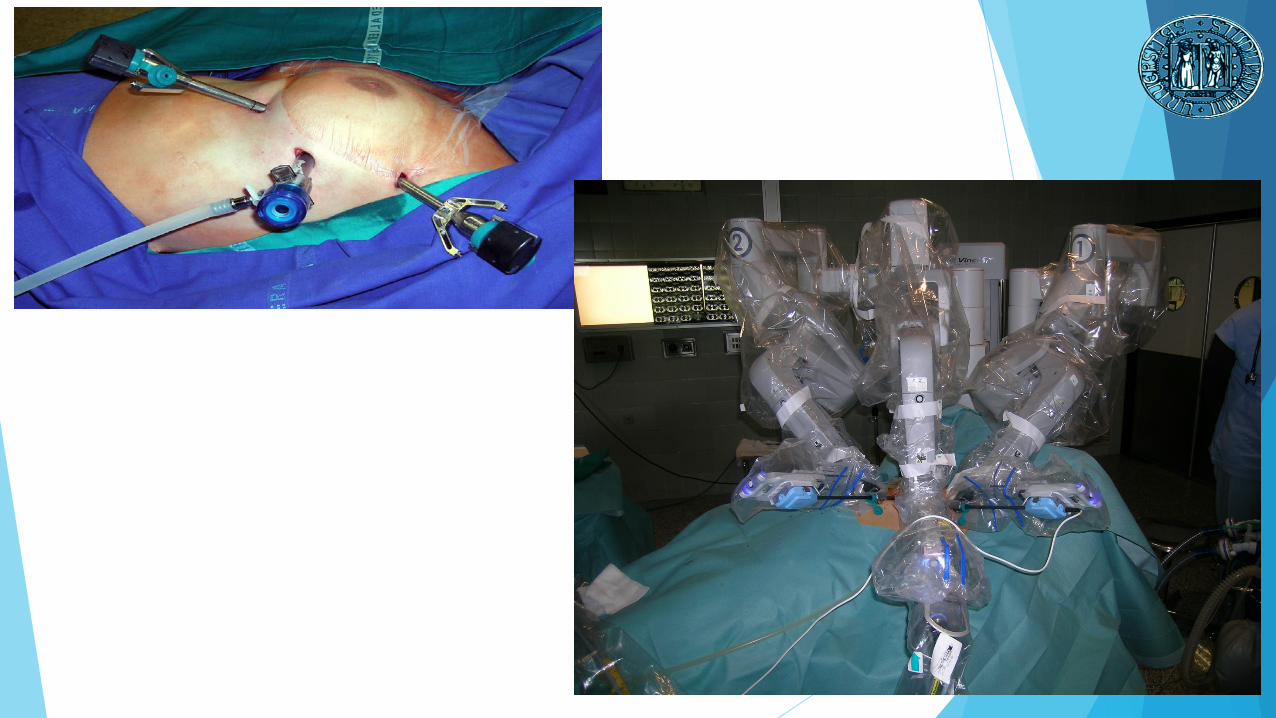
POSITION
Double lumen tubeLeft side approach30 degrees up on bean bagArms at side
PORT PLACEMENT
Left arm- 5th intercostal space - midclavicular line
Camera- 5th intercostal space - anterior portion of
midaxillary regionRight arm
- 3rd intercostal space - anterior portion ofmidaxillary region

OPTICS
0 degree scope 30 degree scope6-10 mmHg CO2 insufflation
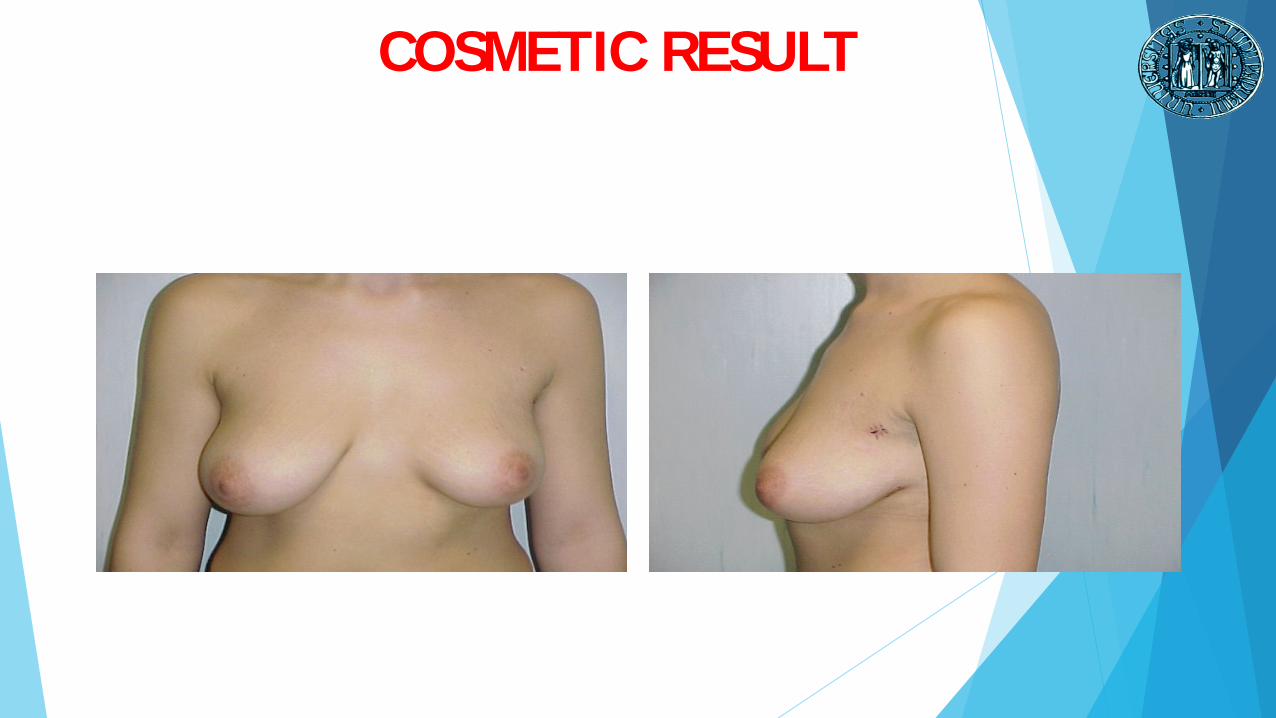
COSMETIC RESULT
APRIL 2002 – APRIL 2017
OUR EXPERIENCE:
186 PATIENTS WITH MG TREATED WITH “DA VINCI” ROBOTIC SYSTEM
THE MAJORITY OF THESE UNDERWENT LEFT-SIDED THORACOSCOPICTHYMECTOMY, SOME PATIENTS WITH RIGHT-SIDED THYMOMA WHEREAPPROACHED FROM THE RIGHT SIDE
133 PATIENTS WERE FEMALE AND THE MEAN AGE WAS 38 YEARS OLD
MOST PATIENTS TAKING COMBINED THERAPY FOR MG IN PARTICULARANTICHOLINESTERASE AND STEROID
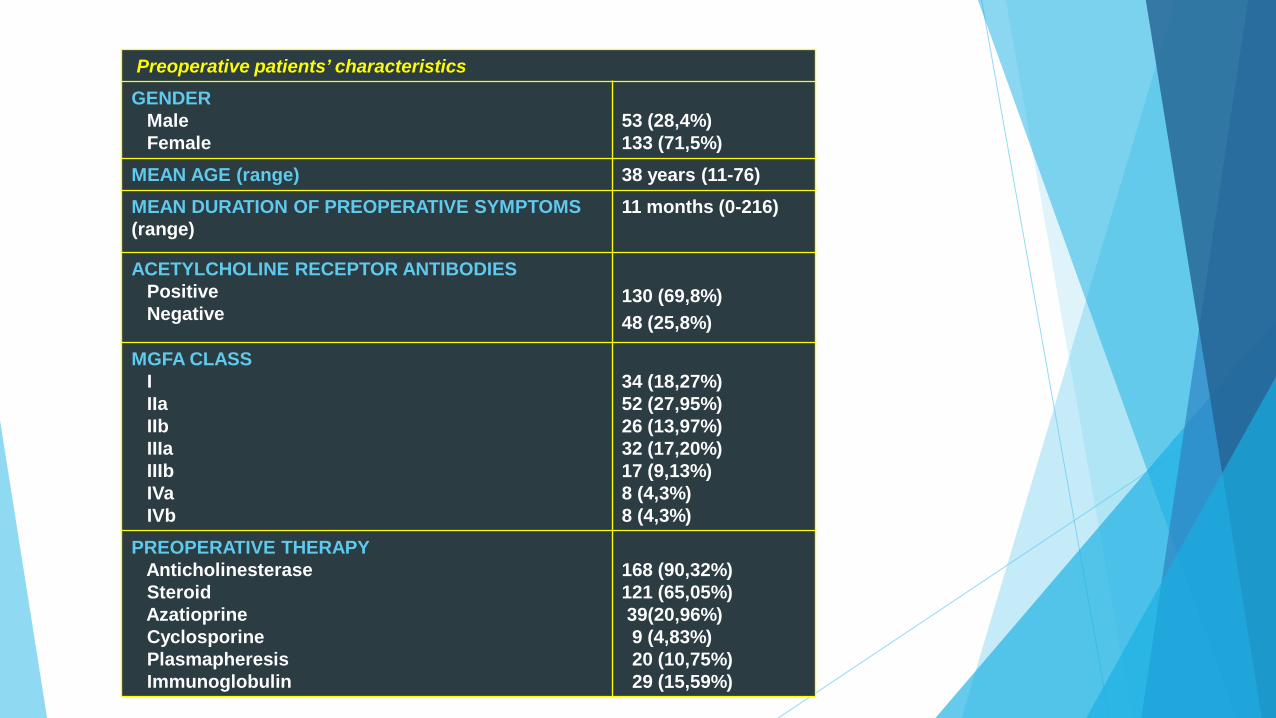
Preoperative patients’ characteristicsGENDER
MaleFemale
53 (28,4%)133 (71,5%)
MEAN AGE (range) 38 years (11-76)MEAN DURATION OF PREOPERATIVE SYMPTOMS(range)
11 months (0-216)
ACETYLCHOLINE RECEPTOR ANTIBODIESPositiveNegative
130 (69,8%)48 (25,8%)
MGFA CLASSIIIaIIbIIIaIIIbIVaIVb
34 (18,27%)52 (27,95%) 26 (13,97%)32 (17,20%)17 (9,13%)8 (4,3%)8 (4,3%)
PREOPERATIVE THERAPYAnticholinesteraseSteroid Azatioprine Cyclosporine PlasmapheresisImmunoglobulin
168 (90,32%)121 (65,05%)39(20,96%)9 (4,83%)20 (10,75%)29 (15,59%)

SURGICAL RESULTS
- MEAN OPERATIVE TIME: 150 MINUTES (60-300 MINUTES)
- MEAN TIME OF HOSPITAL STAY: 3 DAYS (2-33 DAYS)
- MEDIAN TIME TO CHEST TUBE REMOVAL: 2 DAYS (1-32 DAYS)
- NO DEATHS, NO INTRAOPERATIVE COMPLICATIONS, NORECURRENT LARYNGEAL OR PHRENIC NERVE INJURIES
- POSTOPERATIVE COMPLICATIONS: 2 PT WITH CHYLOTHORAX, 2PTS WITH HAEMOTHORAX
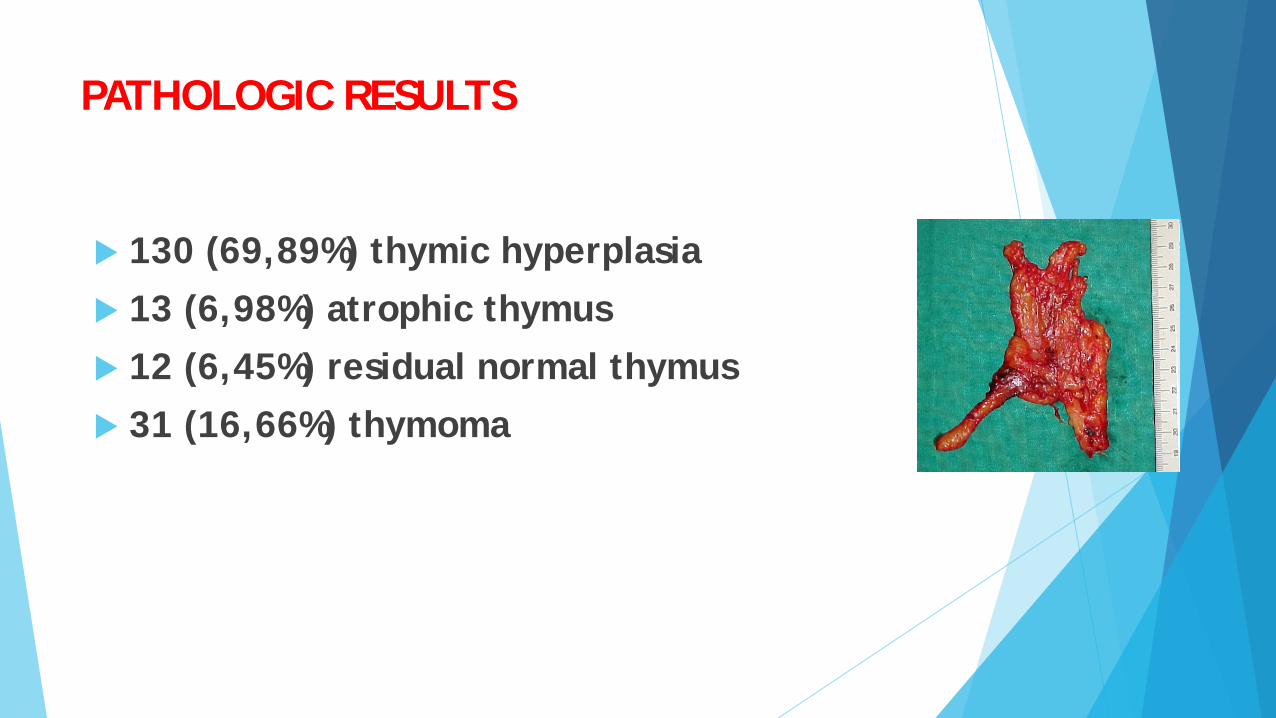
PATHOLOGIC RESULTS
130 (69,89%) thymic hyperplasia 13 (6,98%) atrophic thymus 12 (6,45%) residual normal thymus 31 (16,66%) thymoma

SUMMARY
• Thymectomy has an important role in myastheniagravis patients.
• Lack of randomized trials investigating differentsurgical approaches for thymectomy
• Increasing use of minimally invasive approaches innon-thymomatous MG
• Robotic approach has several advantages: safety, lowcomplications, short hospital stay, optimal cosmeticresults, good neurological results.