K24 Baru Kuliah Malaria Blok Tropmed
17
Malaria
-
Upload
dashari-ermandi-h -
Category
Documents
-
view
46 -
download
0
description
medis
Transcript of K24 Baru Kuliah Malaria Blok Tropmed

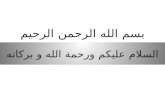
Malaria

Exo-erythrocytic (hepatic) cycle
Sporozoites
Mosquito Salivary Gland
Malaria Life CycleLife Cycle
Gametocytes
Oocyst
ErythrocytiErythrocytic c CycleCycle
Zygote
Schizogony
Sporogony
Hypnozoites(for P. vivax and P. ovale)

Plasmodium spp.1.Plasmodium vivax : Benign
Tertian, Tertian Malaria2.Plasmodium ovale : Ovale tertian Malaria3.Plasmodium malariae : Quartan malaria4.Plasmodium falciparum : Malignant
Tertian malaria.

Affinity of Parasite to ErythrocytesP.vivaxP.malariae Infectes only
young or P.ovale Old
Erythocytes
P.falciparum Infects all age groups

AAlteration of lteration of HHost ost CCells ells A variety of structural changes, which alter
its function, appearance or antigenicity. These alterations are a consequence of
parasite growthAdvantage to the parasite (e.g. increased
membrane permeability, increased selective intake of nutrients, or escape from immunity by sequestration).
The nature of the alterations induced are variable from one species to another.

1. A visible change of shape and reduced deformability
2. The presence of electron-dense protrusions or 'knobs‘
3. The presence of small depressions, or "caveolae", at the surface of the red cell, connected by a network of small vesicles and clefts in P. vivax and P. ovale
The alterations identified The alterations identified include :include :

4.4. TThe cytoadherence to he cytoadherence to endothelial cellsendothelial cells
5.5. TThe adherence to normal he adherence to normal erythrocytes ("rosetting") or to erythrocytes ("rosetting") or to other infectedother infected erythrocyteserythrocytes ("auto-agglutination“("auto-agglutination“ or or clumpingclumping))
6.6. TThe presence of new metabolic he presence of new metabolic channels; evidence of new channels; evidence of new parasite-specific antigens parasite-specific antigens associated with the red cell associated with the red cell membranemembrane
The alterations identified The alterations identified include :include :

PathogenesisRelated to erythrocytic infection by the asexual stages, Gametocytes not involve in pathogenesis
Pathology is associated with: Haemolysis
- Direct invasion & rupture of RBC during erythrocytic cycle- Increased osmotic fragility of RBC
Increased adhesiveness of infected RBC- Increases with the maturity of the parasite (schizont > trophozoite)- Knob theory
Release of pyrogens, toxin and cytokines Immunological responses Capillary permeability Tissue hypoxia

Rosetting
Sludging
Sequestration
PathoPathogenesisgenesis

Pathogenesis
Cytokines can induce (mimic) many of symptoms Cytokines can induce (mimic) many of symptoms and signs of malaria (shivering, headache, chills, and signs of malaria (shivering, headache, chills, spiking fever,sweating, vasodilation, hypoglycemia)spiking fever,sweating, vasodilation, hypoglycemia)
Adherence and inflammation reinforce each other Adherence and inflammation reinforce each other in an unholy circle causing pathologyin an unholy circle causing pathology
Cytoadherence seems to be the mainCytoadherence seems to be the main culprit culprit for for pathogenesispathogenesis Infected RBCs will adhere to the endothelium Infected RBCs will adhere to the endothelium as as well as to each other well as to each other HHigh cytokine levels igh cytokine levels induce induce expression of endothelialexpression of endothelial adhesins -- inflammation adhesins -- inflammation makes the endothelia makes the endothelia ‘‘stickier’ stickier’

ImmunityInfluenced by
GeneticsAgeHealth conditionPregnancy statusIntensity of transmission in regionLength of exposureMaintenance of exposure

ImmunityInnate
Red cell polymorphisms associated with some protectionHemoglobin S sickle cell trait or diseaseHemoglobin C and hemoglobin EThalessemia – α and β Glucose – 6 – phosphate dehydrogenase deficiency
(G6PD)Red cell membrane changes
Absence of certain Duffy coat antigens improves resistance to P.v.

ImmunityAcquired
Transferred from mother to child3-6 months protectionThen children have increased susceptibility
Increased susceptibility during early childhoodHyper- and holoendemic areas
By age 5 attacks usually < frequent and severeCan have > parasite densities with fewer
symptomsMeso- or hypoendemic areas
Less transmission and repeated attacksMay acquire partial immunity and be at higher
risk for symptomatic disease as adults

ImmunityAcquired
No complete immunityCan be parasitemic without clinical disease
Need long period of exposure for inductionMay need continued exposure for maintenance Immunity can be unstable
Can wane as one spends time outside endemic areaCan change with movement to area with different
endemicityDecreases during pregnancy, risk improves with
increasing gravidity

Immune Mechanisms
15
Stage specific : Anti sporozoite antibodies in adults in
endemic areas- blocks liver invasionAnti sporozoite/merozoite antibodies -
block rbc invasionCytokines : TNF blocks merozoite
development; IL1 ; IL10Erythrocyte clearance - liver and spleenBlock cyto-adherenceEnhance clearance through opsonisationADCC likely NK activity


Thank You