Juvenile idiopathic arthritis
40
Juvenile Idiopathic Arthritis Prepared By: Mays Husam Nairat Supervised By: Dr. Maysa Alawnih
-
Upload
mays-nairat -
Category
Health & Medicine
-
view
609 -
download
1
Transcript of Juvenile idiopathic arthritis

Juvenile Idiopathic Arthritis
Prepared By: Mays Husam Nairat
Supervised By: Dr. Maysa Alawnih

Objectives
1. Introduction
2. Etiology
3. Epidemiology
4. Clinical Presentation
5. Classification
6. Diagnosis
7. Complications
8. Prognosis
20/12/2015 2 JIA- Mays Nairat

Introduction
• JIA is one of chronic arthritides of childhood
• Juvenile Idiopathic Arthritis = Juvenile Chronic Arthritis = Juvenile Rheumatoid Arthritis
• JIA includes groups of diseases that share specific characteristics
20/12/2015 JIA- Mays Nairat 3
Etiology
• It is an autoimmune disease of unknown etiology
• The common underlying manifestation is the presence of chronic synovitis
20/12/2015 4 JIA- Mays Nairat
Epidemiology
• JIA is the most common chronic rheumatologic disease of childhood
• Prevalence 1:1000
• Two peaks; one at 1-3 yrs & one at 8-12 yrs
• Girls are affected more commonly than boys
20/12/2015 5 JIA- Mays Nairat

Clinical Presentation
•onset of the arthritis is slow •the actual joint swelling is often noticed acutely •confused with trauma
20/12/2015 6 JIA- Mays Nairat

• Pain and stiffness in the joint that limit use, but rarely refuses to use the joint at all
• Morning stiffness and gelling (stiffness after rest)
20/12/2015 7 JIA- Mays Nairat

on physical examination :
• Signs of inflammation; joint tenderness, erythema, and effusion
• Joint range of motion may be limited because of pain, swelling, or contractures from lack of use
• Localized growth disturbances
• Leg length discrepancy if arthritis is asymmetrical
20/12/2015 8 JIA- Mays Nairat
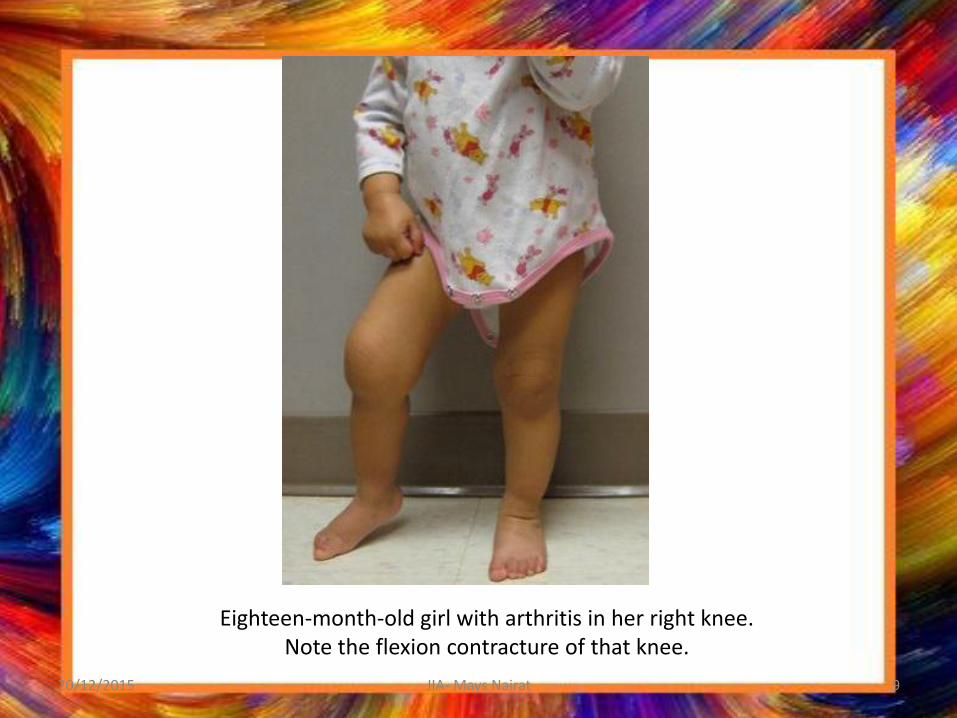
Eighteen-month-old girl with arthritis in her right knee. Note the flexion contracture of that knee.
20/12/2015 9 JIA- Mays Nairat

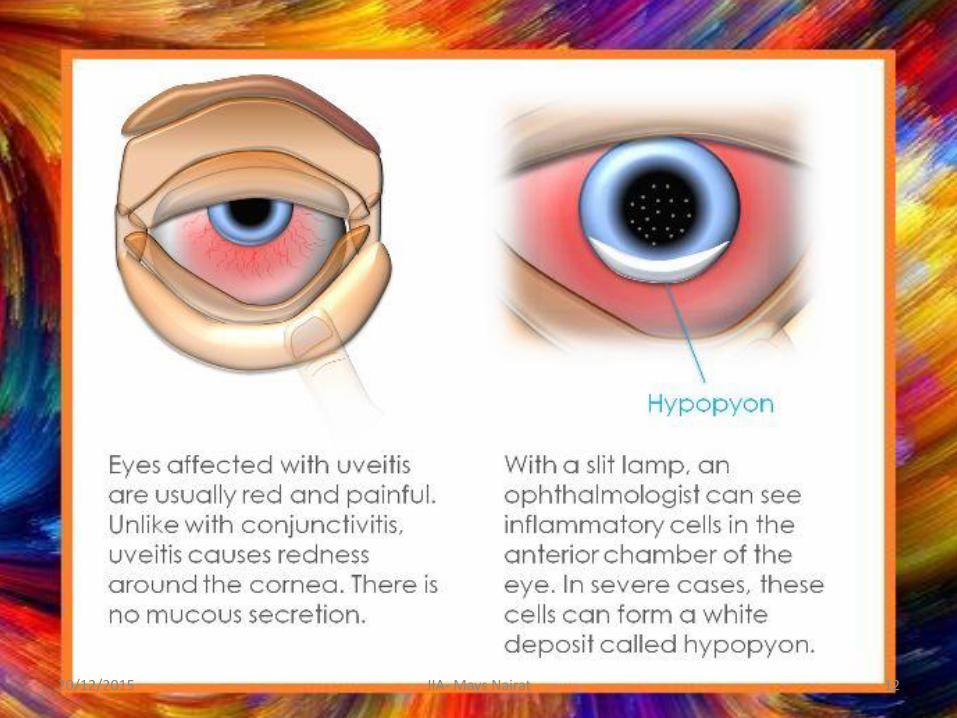
• All children with chronic arthritis are at risk for chronic iridocyclitis or uveitis
• Association between uveitis and HLA-DR5/ DR6/ DR8
• Positive ANA at higher risk for chronic uveitis
20/12/2015 10 JIA- Mays Nairat

Highest risk group:
young girls,
With oligoarticular JIA (less than 5 joints affected),
And Positive ANA
Incidence of uveitis 80%
20/12/2015 11 JIA- Mays Nairat
20/12/2015 12 JIA- Mays Nairat
Classification
1. Oligoarticular JIA
2. Polyarticular JIA
3. Systemic-Onset JIA
4. Spondyloarthropathies
20/12/2015 13 JIA- Mays Nairat
Oligoarticular JIA
• Arthritis in fewer than five joints within 6 months of diagnosis
• The most common form of JIA, 50%
• Two peaks; one at 1-3 yrs & one at 8-12 yrs
• Medium-sized to large joints; knee> ankle > wrist
20/12/2015 14 JIA- Mays Nairat
Oligoarticular JIA
• Children may be otherwise well without any evidence of systemic inflammation (fever, weight loss, or failure to thrive) or any laboratory evidence of systemic inflammation (elevated WBC count or ESR)
Extended Oligoarthritis: Later development of polyarticular disease
20/12/2015 JIA- Mays Nairat 15

20/12/2015 JIA- Mays Nairat 16
Polyarticular JIA
• Children with arthritis in five or more joints within the first 6 months of diagnosis
• 40% of JIA
• Symmetric arthritis, which can affect any joint but typically involves the small joints of the hands, feet, ankles, wrists, and knees
20/12/2015 JIA- Mays Nairat 17
Polyarticular JIA
• The cervical spine can be involved
• Systemic inflammation manifestation; malaise, low-grade fever, growth retardation, anemia of chronic disease
• Elevated markers of inflammation
• Can present at any age; however, there are 2 peaks: in early childhood (RF –ve) and adolescence (RF +ve)
20/12/2015 JIA- Mays Nairat 18

20/12/2015 JIA- Mays Nairat 19
•Patient with active polyarticular arthritis. Note swelling (effusions) of all PIP joints in addition to boney overgrowth. •The patient has interosseus muscle wasting •Subluxation and ulnar deviation of the wrists are present

Systemic-Onset JIA (Still’s disease)
• 10% of JIA
• They does not present with onset of arthritis
• Manifest with a typical recurring, spiking fever, usually once or twice per day, for several weeks to months
• accompanied by a rash, typically morbilliform and salmon- colored - Evanescent, occurs at time of high fever only
20/12/2015 JIA- Mays Nairat 20

20/12/2015 JIA- Mays Nairat 21

Systemic-Onset JIA
• Internal organ involvement also occurs
• Hepatosplenomegaly, 70%
• Serositis, 50%
• Significant constitutional symptoms
• Laboratory findings of inflammation
• The arthritis of JIA follows the systemic inflammation by 6 wks- 6 mo
20/12/2015 JIA- Mays Nairat 22

20/12/2015 JIA- Mays Nairat 23

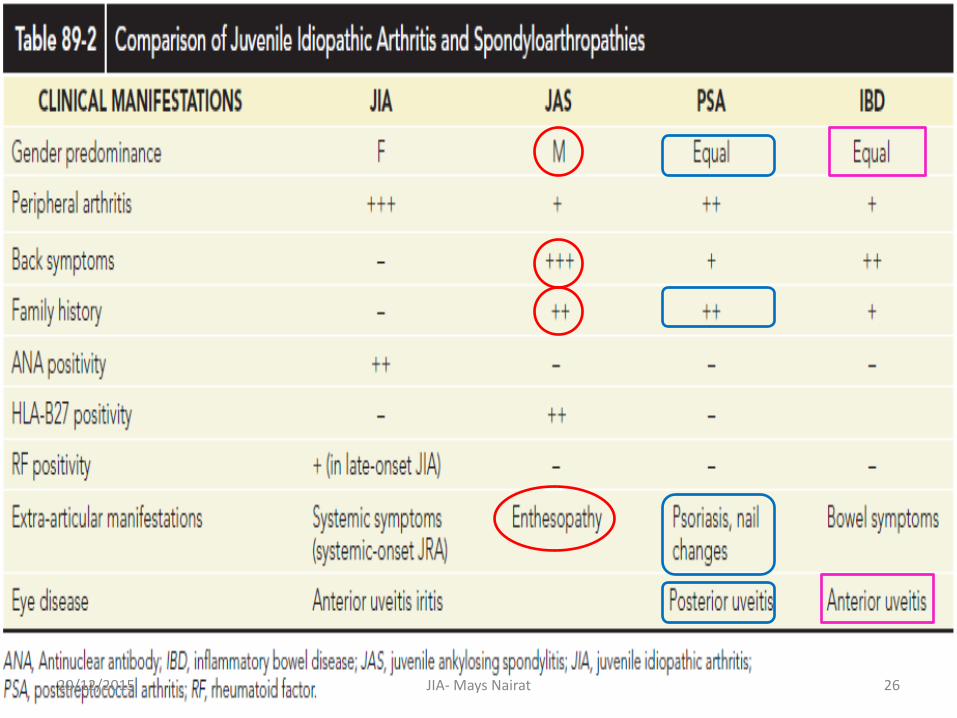
Spondyloarthropathies
• Inflammation of the axial skeleton and sacroiliac joints and enthesitis (inflammation of tendinous insertions)
• These include:
1. Juvenile ankylosing spondylitis
2. Psoriatic arthritis
3. Arthritis of inflammatory bowel disease
20/12/2015 JIA- Mays Nairat 24
Spondyloarthropathies
• Frequent presence of HLA-B27
• Need earlier Tx with TNF blockers
• They can present with peripheral arthritis, so initially classified in other subgroups
• It is only later when the Dx becomes clear
20/12/2015 JIA- Mays Nairat 25
20/12/2015 JIA- Mays Nairat 26
Workup
• CBC
• ESR, CRP
• ANA
• RF
• Diagnostic arthrocentesis: The synovial fluid WBC
count is typically less than 50,000 to 100,000/mm3, predominantly lymphocytes. Gram stain and culture should be negative.
20/12/2015 JIA- Mays Nairat 27

• The most common radiologic finding in the early stages of JIA is ……………………..….
20/12/2015 JIA- Mays Nairat 28
Normal bone x-ray
• Over time, periarticular osteopenia, resulting from decreased mineralization, is most commonly found

20/12/2015 JIA- Mays Nairat 29
•Severe loss of cartilage. •Boney ankylosis involving the lateral 4 carpal bones with sparing of the pisiform. •Erosions are present in the distal radius and ulna. •Narrowing of the carpal/metacarpal joints is present.

20/12/2015 JIA- Mays Nairat 30
Ankylosis in the cervical spine at several levels due to long-standing JIA
Diagnosis
• The diagnosis of JIA is established by the presence of arthritis, the duration of the disease for at least 6 weeks, and exclusion of other possible diagnoses
• Children must be younger than 16 y/o at time of onset of disease
20/12/2015 JIA- Mays Nairat 31
20/12/2015 JIA- Mays Nairat 32
Treatment
1. Suppressing inflammation
2. Preserving and maximizing function
3. Preventing deformity
4. Preventing blindness
20/12/2015 JIA- Mays Nairat 33
20/12/2015 JIA- Mays Nairat 34
Prognosis
• The prognosis of JIA is excellent, with an overall 85% complete remission rate
• Children with oligoarticular JIA tend to do well
• Children with polyarticular disease and systemic-onset disease constitute most children with functional disability
20/12/2015 JIA- Mays Nairat 35

• The importance of physical & occupational therapy cannot be overstated because when the disease remits, the physical limitations remain with the patient into adulthood
20/12/2015 JIA- Mays Nairat 36
20/12/2015 JIA- Mays Nairat 37

20/12/2015 JIA- Mays Nairat 38

20/12/2015 JIA- Mays Nairat 39

20/12/2015 JIA- Mays Nairat 40