Jeffrey W. Swanson, PhD (Principal Investigator) Thinking ... · denial. Increasing number ......
6
Thinking Carefully about Mental Illness, Gun Violence, and the Law: Balancing Risk and Rights for Effective Policy Jeffrey Swanson, PhD Professor in Psychiatry and Behavioral Sciences Duke University School of Medicine Durham, North Carolina Research Team Duke University School of Medicine Department of Psychiatry and Behavioral Sciences Jeffrey W. Swanson, PhD (Principal Investigator) Allison G. Robertson, PhD, MPH Marvin S. Swartz, MD Michele Easter, PhD Kelly Alanis‐Hirsch, PhD Charles Belden, PhD *** University of Connecticut School of Social Work Hsiuju Lin, PhD (Site Principal Investigator) Linda K. Frisman, PhD (Consultant) *** Yale University School of Medicine Department of Psychiatry Michael A. Norko, MD, MAR (Site Principal Investigator) Madelon Baranoski, PhD, MSN *** Sponsors Fund for a Safer Future Elizabeth K. Dollard Trust National Science Foundation Robert Wood Johnson Foundation Public Health Law Research Program Population attributable risk of minor or serious violent behavior towards others Serious mental illness contributes very little to overall violence towards others Serious mental Illness 4% Other factors that cause violence 96% • Swanson JW. Mental disorder, substance abuse, and community violence: an epidemiological approach. In: Monahan J, Steadman H, editors. Violence and mental disorder. Chicago: University of Chicago Press; 1994. pp. 101‐136. • Swanson JW, McGinty EE, Fazel S, Mays VM (2015). Mental illness and reduction of gun violence and suicide: bringing epidemiologic research to policy. Annals of Epidemiology. S1047‐2797(14)00147‐1. • Young, male • Substance abuse • Impulsive anger • Poverty • Childhood physical abuse • Exposure to violence in the social environment Percent violent within 6 – 12 months People with mental illness are at increased risk of violence when identified in certain settings, in certain periods 2% 8% 23% 36% 37% 0% 10% 20% 30% 40% General population without mental illness Outpatients in treatment Emergency departments Involuntarily committed inpatients First‐episode psychosis patients Sources: Adapted from (1) Choe JY, Teplin LA, Abram KM (2008). Perpetration of violence, violent victimization, and severe mental illness: Balancing public health concerns. Psychiatric Services 59, 153‐164; (2) Large MM, Nielssen O (2011). Violence in first‐episode psychosis: A systematic review and meta‐analysis. Schizophrenia Research 125, 209‐220. Predicted probability of serious violent behavior in persons with serious mental illness by combined risk factors, controlling for significant covariates in logistic regression model (5 site N=802) Source: Swanson JW, Swartz MS, Essock SM, Osher FC, Wagner HR, Goodman LA, Rosenberg SD, Meador KG (2002). The social‐environmental context of violent behavior in persons treated for severe mental illness. American Journal of Public Health, 92(9): 1523‐1531. None (N=54) S (N=14) E (N=27) V (N=132) S+V (N=71) S+E (N=14) V+E (N=225) S+V +E (N=265) Percent violent in past year Additional risk factors N = none V = early victimization S = substance abuse E = exposure to violence in current social environment <.01 .02 - .04 .07 - .10 .31 .10 .20 .40 .30 0
Transcript of Jeffrey W. Swanson, PhD (Principal Investigator) Thinking ... · denial. Increasing number ......
Thinking Carefully about Mental Illness, Gun Violence, and the Law: Balancing Risk and Rights for Effective Policy
Jeffrey Swanson, PhD
Professor in Psychiatry and Behavioral Sciences Duke University School of MedicineDurham, North Carolina
Research TeamDuke University School of Medicine
Department of Psychiatry and Behavioral SciencesJeffrey W. Swanson, PhD (Principal Investigator)
Allison G. Robertson, PhD, MPHMarvin S. Swartz, MDMichele Easter, PhD
Kelly Alanis‐Hirsch, PhDCharles Belden, PhD
***
University of Connecticut School of Social WorkHsiuju Lin, PhD (Site Principal Investigator)
Linda K. Frisman, PhD (Consultant)***
Yale University School of Medicine Department of Psychiatry
Michael A. Norko, MD, MAR (Site Principal Investigator)Madelon Baranoski, PhD, MSN
***
SponsorsFund for a Safer Future Elizabeth K. Dollard Trust
National Science FoundationRobert Wood Johnson Foundation Public Health Law Research Program
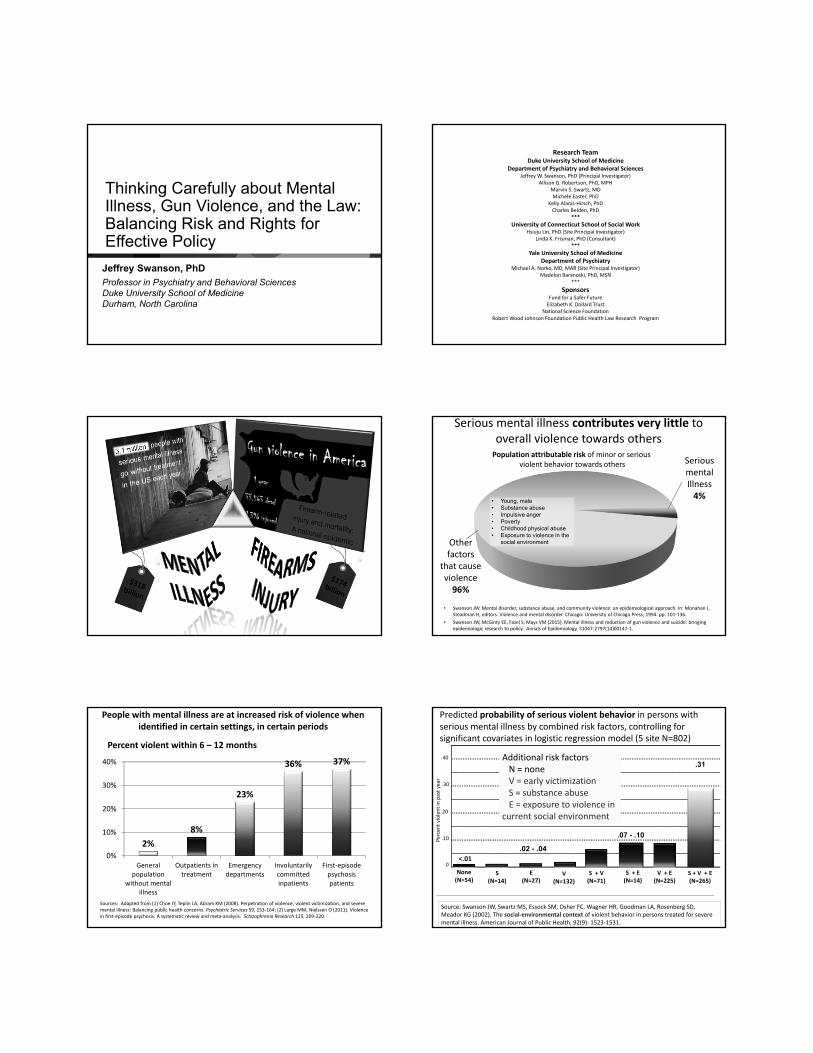
Population attributable risk of minor or serious violent behavior towards others
Serious mental illness contributes very little to overall violence towards others
SeriousmentalIllness4%
Other factors
that cause violence96%
• Swanson JW. Mental disorder, substance abuse, and community violence: an epidemiological approach. In: Monahan J, Steadman H, editors. Violence and mental disorder. Chicago: University of Chicago Press; 1994. pp. 101‐136.
• Swanson JW, McGinty EE, Fazel S, Mays VM (2015). Mental illness and reduction of gun violence and suicide: bringing epidemiologic research to policy. Annals of Epidemiology. S1047‐2797(14)00147‐1.
• Young, male• Substance abuse• Impulsive anger• Poverty• Childhood physical abuse• Exposure to violence in the
social environment
Percent violent within 6 – 12 months
People with mental illness are at increased risk of violence when identified in certain settings, in certain periods
2%
8%
23%
36% 37%
0%
10%
20%
30%
40%
Generalpopulation
without mentalillness
Outpatients intreatment
Emergencydepartments
Involuntarilycommittedinpatients
First‐episodepsychosispatients
Sources: Adapted from (1) Choe JY, Teplin LA, Abram KM (2008). Perpetration of violence, violent victimization, and severe mental illness: Balancing public health concerns. Psychiatric Services 59, 153‐164; (2) Large MM, Nielssen O (2011). Violence in first‐episode psychosis: A systematic review and meta‐analysis. Schizophrenia Research 125, 209‐220.
Predicted probability of serious violent behavior in persons with serious mental illness by combined risk factors, controlling for significant covariates in logistic regression model (5 site N=802)
Source: Swanson JW, Swartz MS, Essock SM, Osher FC, Wagner HR, Goodman LA, Rosenberg SD, Meador KG (2002). The social‐environmental context of violent behavior in persons treated for severe mental illness. American Journal of Public Health, 92(9): 1523‐1531.
None(N=54)
S(N=14)
E(N=27)
V(N=132)
S + V(N=71)
S + E(N=14)
V + E(N=225)
S + V + E(N=265)
Percent violent in past year
Additional risk factorsN = noneV = early victimizationS = substance abuseE = exposure to violence in
current social environment
<.01
.02 - .04
.07 - .10
.31
.10
.20
.40
.30
0

Not violent689 (72%)
Violent262 (28%)
No gun239 (91%) Gun 23 (9%) Known
14 (61%) Stranger9 (39%)
Gun‐involved violence among discharged psychiatric patients (N=951): New analysis of MacArthur Violence Risk Assessment Study
Any violent behavior in yearfollowing hospital discharge
Any gun involvementin violent acts
Any gun violence against a stranger
Any gun violence in year: 2% of total sample
Steadman HF, Monahan J, Pinals DA, Vesselinov R, Robbins PC (2015). Gun violence and victimization of strangers by persons with a mental illness: Data from the MacArthur Violence Risk Assessment Study. Psychiatric Services 66(11):1238‐41.
Risk‐related characteristics of 23 psychiatric patients who engaged in gun violence (Steadman et al., 2015)
78.3%
52.2%
91.3%
52.2%
91.3%
65.2%60.9%
65.2%
21.7%13.0%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Priorhosp
>3admits
Priorarrest
>3arrest
Abusedas child
Father2+
arrests
Subsabuse
Suicidethreats
Halluc ParanoidSx
33,599 gun deaths in 2014
84,258nonfatalgun
injuries
Suicide63%
Homicide34%
Police 2%Unintentional 1%
Population Attributable Risk (PAR) of suicide associated with diagnosable mental illness:
Current starting point for federal firearms policy
– Constitutional right: • Landmark US Supreme Court decisions striking down across‐the‐board
handgun bans ‐‐ District of Columbia v. Heller, 554 U.S. 570 (2008) and McDonald v. Chicago, 561 U.S. 3025 (2010) ‐‐ affirmed that the Constitution confers an individual right to keep and bear arms
– Right is “not unlimited”• Court emphasized that “nothing in our opinion should be taken to cast
doubt on longstanding prohibitions on the possession of firearms by felons and the mentally ill.”o Mental health prohibitor: Involuntary civil commitment or other mental health
adjudication
– Focus on dangerous people, not so much the guns• Court’s decision seems to imply: In this country, we are prevented
from solving the problem of gun violence by broadly limiting the public’s legal access to firearms. Instead, we must focus more narrowly on how best to identify people at significant risk of harming others or themselves who should not have access to guns.
Federal law categorically excludes some people with mental illness from accessing firearms
• 18 U.S.C. 922(d):
– Prohibited from possessing or purchasing a firearm if (among other things)
• committed to a mental institution
• adjudicated as a mental defective– Legal authority determines: dangerous or incompetent to manage own
affairs due to a mental illness; incompetent to stand trial or acquitted by reason of insanity
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
3,500,000
4,000,000
2007
NICS initiated Virginia Tech shooting
1998
NICS Improvement
Act
2014
300,000
3.7 M
Mental health records accounted for 7% records in NICS index in 2007
Mental health records accounted for 34% of records
in NICS index in 2014
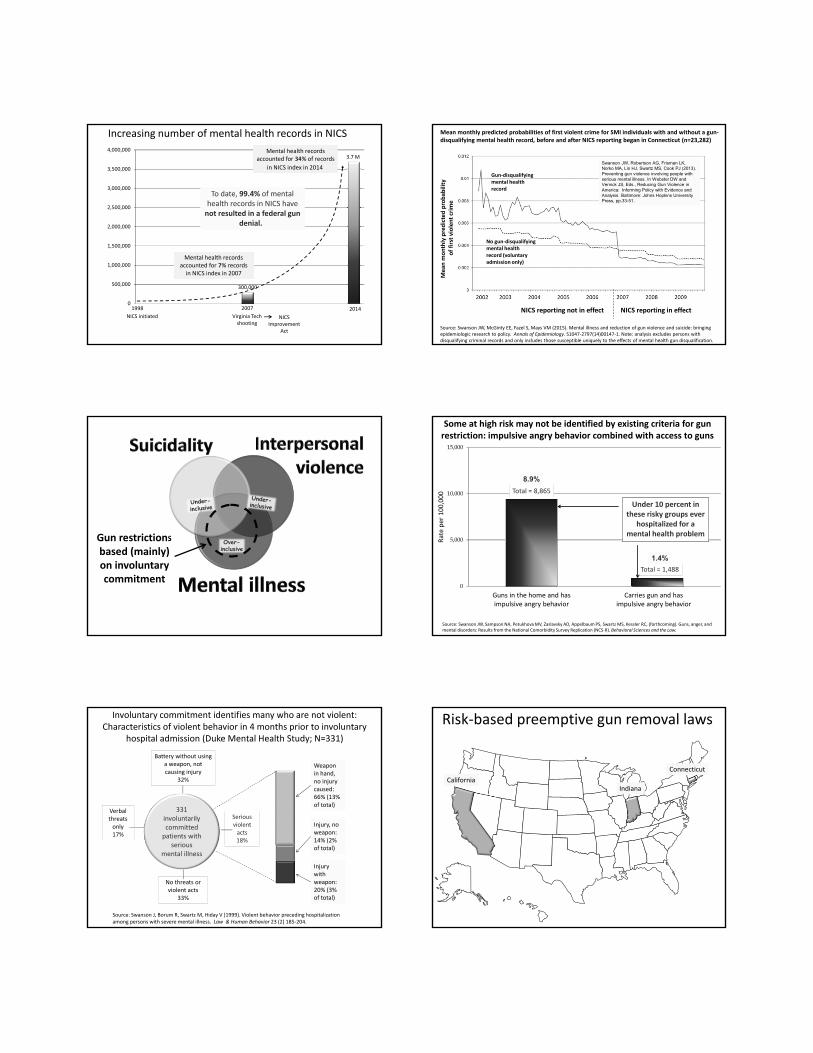
To date, 99.4% of mental health records in NICS have not resulted in a federal gun
denial.
To date, 99.4% of mental health records in NICS have not resulted in a federal gun
denial.
Increasing number of mental health records in NICS Mean monthly predicted probabilities of first violent crime for SMI individuals with and without a gun‐disqualifying mental health record, before and after NICS reporting began in Connecticut (n=23,282)
NICS reporting in effectNICS reporting not in effect
Gun‐disqualifying mental health record
No gun‐disqualifying mental health record (voluntary admission only)
Mea
n m
onthly predicted probab
ility
of first violent crim
e
Source: Swanson JW, McGinty EE, Fazel S, Mays VM (2015). Mental illness and reduction of gun violence and suicide: bringing epidemiologic research to policy. Annals of Epidemiology. S1047‐2797(14)00147‐1. Note: analysis excludes persons with disqualifying criminal records and only includes those susceptible uniquely to the effects of mental health gun disqualification.
Swanson JW, Robertson AG, Frisman LK, Norko MA, Lin HJ, Swartz MS, Cook PJ (2013). Preventing gun violence involving people with serious mental illness. In Webster DW and Vernick JS, Eds., Reducing Gun Violence in America: Informing Policy with Evidence and Analysis. Baltimore: Johns Hopkins University Press, pp.33-51.
Gun restrictions based (mainly) on involuntary commitment
Over-inclusive
0
5,000
10,000
15,000
Guns in the home and has impulsive angry behavior
Carries gun and has impulsive angry behavior
Rate per 100,000 Total = 8,865
Total = 1,488
Source: Swanson JW, Sampson NA, Petukhova MV, Zaslavsky AD, Appelbaum PS, Swartz MS, Kessler RC, (forthcoming). Guns, anger, andmental disorders: Results from the National Comorbidity Survey Replication (NCS‐R). Behavioral Sciences and the Law.
Under 10 percent in these risky groups ever
hospitalized for a mental health problem
8.9%8.9%
1.4%1.4%
Some at high risk may not be identified by existing criteria for gun restriction: impulsive angry behavior combined with access to guns
Weapon in hand, no injury caused:66% (13% of total)
Weapon in hand, no injury caused:66% (13% of total)
Injury, no weapon:14% (2% of total)
Injury, no weapon:14% (2% of total)
Injury with weapon:20% (3% of total)
Injury with weapon:20% (3% of total)
No threats or violent acts
33%
Verbal threats only17%
Battery without using a weapon, not causing injury
32%
Serious violent acts18%
Involuntary commitment identifies many who are not violent: Characteristics of violent behavior in 4 months prior to involuntary
hospital admission (Duke Mental Health Study; N=331)
Source: Swanson J, Borum R, Swartz M, Hiday V (1999). Violent behavior preceding hospitalization among persons with severe mental illness. Law & Human Behavior 23 (2) 185‐204.
331involuntarilycommittedpatients with
seriousmental illness
CaliforniaIndiana
Connecticut
Risk‐based preemptive gun removal laws
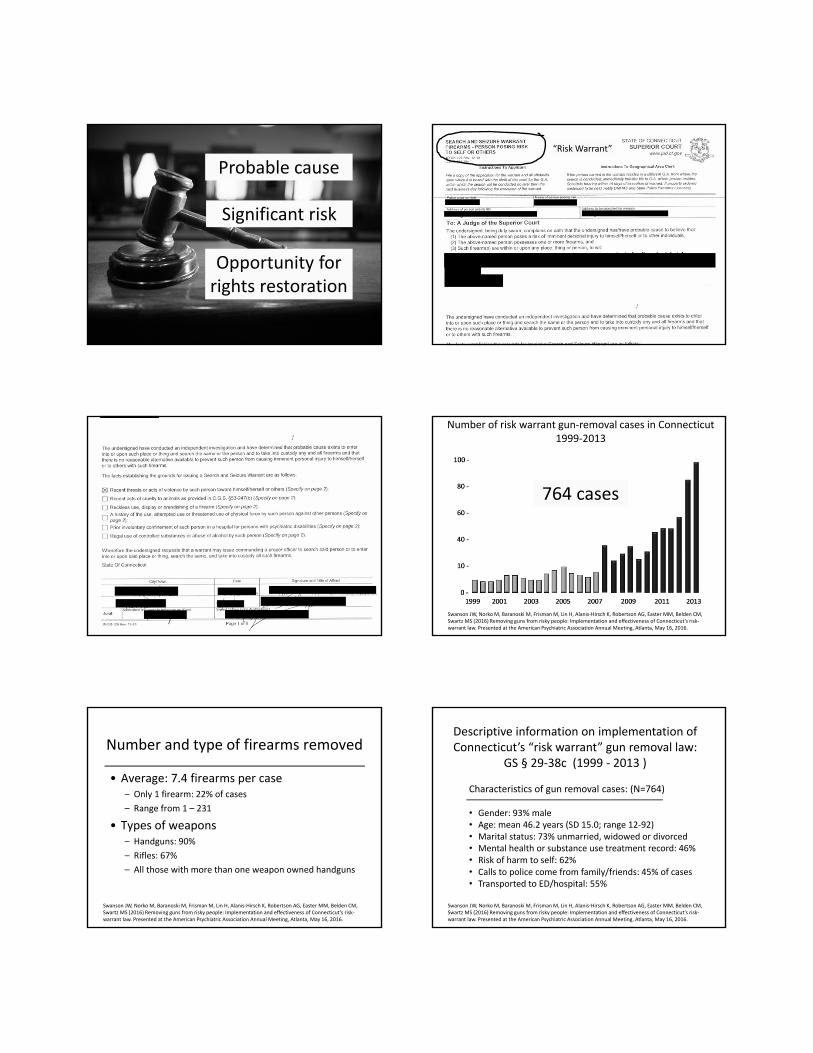
Probable cause
Significant risk
Opportunity for rights restoration
“Risk Warrant”
Number of risk warrant gun‐removal cases in Connecticut1999‐2013
764 cases
Swanson JW, Norko M, Baranoski M, Frisman M, Lin H, Alanis‐Hirsch K, Robertson AG, Easter MM, Belden CM, Swartz MS (2016) Removing guns from risky people: Implementation and effectiveness of Connecticut’s risk‐warrant law. Presented at the American Psychiatric Association Annual Meeting, Atlanta, May 16, 2016.
Number and type of firearms removed
• Average: 7.4 firearms per case– Only 1 firearm: 22% of cases
– Range from 1 – 231
• Types of weapons – Handguns: 90%
– Rifles: 67%
– All those with more than one weapon owned handguns
Swanson JW, Norko M, Baranoski M, Frisman M, Lin H, Alanis‐Hirsch K, Robertson AG, Easter MM, Belden CM, Swartz MS (2016) Removing guns from risky people: Implementation and effectiveness of Connecticut’s risk‐warrant law. Presented at the American Psychiatric Association Annual Meeting, Atlanta, May 16, 2016.
Characteristics of gun removal cases: (N=764)
• Gender: 93% male• Age: mean 46.2 years (SD 15.0; range 12‐92)• Marital status: 73% unmarried, widowed or divorced• Mental health or substance use treatment record: 46%• Risk of harm to self: 62%• Calls to police come from family/friends: 45% of cases• Transported to ED/hospital: 55%
Descriptive information on implementation of Connecticut’s “risk warrant” gun removal law:
GS § 29‐38c (1999 ‐ 2013 )
Swanson JW, Norko M, Baranoski M, Frisman M, Lin H, Alanis‐Hirsch K, Robertson AG, Easter MM, Belden CM, Swartz MS (2016) Removing guns from risky people: Implementation and effectiveness of Connecticut’s risk‐warrant law. Presented at the American Psychiatric Association Annual Meeting, Atlanta, May 16, 2016.

Proportion in treatment before and after gun removal event
Before
Before
After
After
36%
17%
70%
44%
Mental health andsubstance abuse
diagnosis
Mental health anddiagnosis
Swanson JW, Norko M, Baranoski M, Frisman M, Lin H, Alanis‐Hirsch K, Robertson AG, Easter MM, Belden CM, Swartz MS (2016) Removing guns from risky people: Implementation and effectiveness of Connecticut’s risk‐warrant law. Presented at the American Psychiatric Association Annual Meeting, Atlanta, May 16, 2016.
Suicide deaths
Suicidal thoughts
Suicide attempts 90% survive
Depressive symptoms
Alcoholmisuse
FirearmN= 6 (29%)
Drug ODN= 2 (9%)Gas
N= 2 (9%)
HangingN= 10 (48%)
Stab/cutN= 1 (5%)
Suicide means in gun removal cases
OtherN= 15 (71%)
Swanson JW, Norko M, Baranoski M, Frisman M, Lin H, Alanis‐Hirsch K, Robertson AG, Easter MM, Belden CM, Swartz MS (2016) Removing guns from risky people: Implementation and effectiveness of Connecticut’s risk‐warrant law. Presented at the American Psychiatric Association Annual Meeting, Atlanta, May 16, 2016.
Intentional self‐injuries Attempts
Casefatality rate Not fatal Fatal
Firearm 123 87.0% 16 107
Hanging/strangulation 183 72.7% 50 133
Poisoning ‐ gas 40 37.5% 25 15
Poisoning ‐ drugs 1,857 2.7% 1,807 50
Incision/cut 423 2.4% 413 10
Total 2,626 12.0% 2,311 315
CT adult population suicide data 2012 (Sources: CDC WISQARS and hospital ED reports)
Intentional self‐injuries Attempts
Case fatality rate Not fatal Fatal
Firearm 7 87.0% 1 6
Hanging/strangulation 14 72.7% 4 10
Poisoning ‐ gas 5 37.5% 3 2
Poisoning ‐ drugs 74 2.7% 72 2
Incision/cut 42 2.4% 41 1
Total 142 14.6% 121 21
CT gun seizure cases: suicide outcomes (Sources: Risk‐warrant data and state DPH vital records)
Estimated 1
attemptsEstimated 2
not fatal
1 N total suicide attempts = N completed suicides x (1/CFR)2 N nonfatal attempts = N total suicide attempts – N completed suicides
1 N total suicide attempts = N completed suicides x (1/CFR)2 N nonfatal attempts = N total suicide attempts – N completed suicides
Estimated number of averted suicides: 103
Estimated number of averted suicides: 103
For every 7 risk‐based gun seizures…
1 suicide
prevented
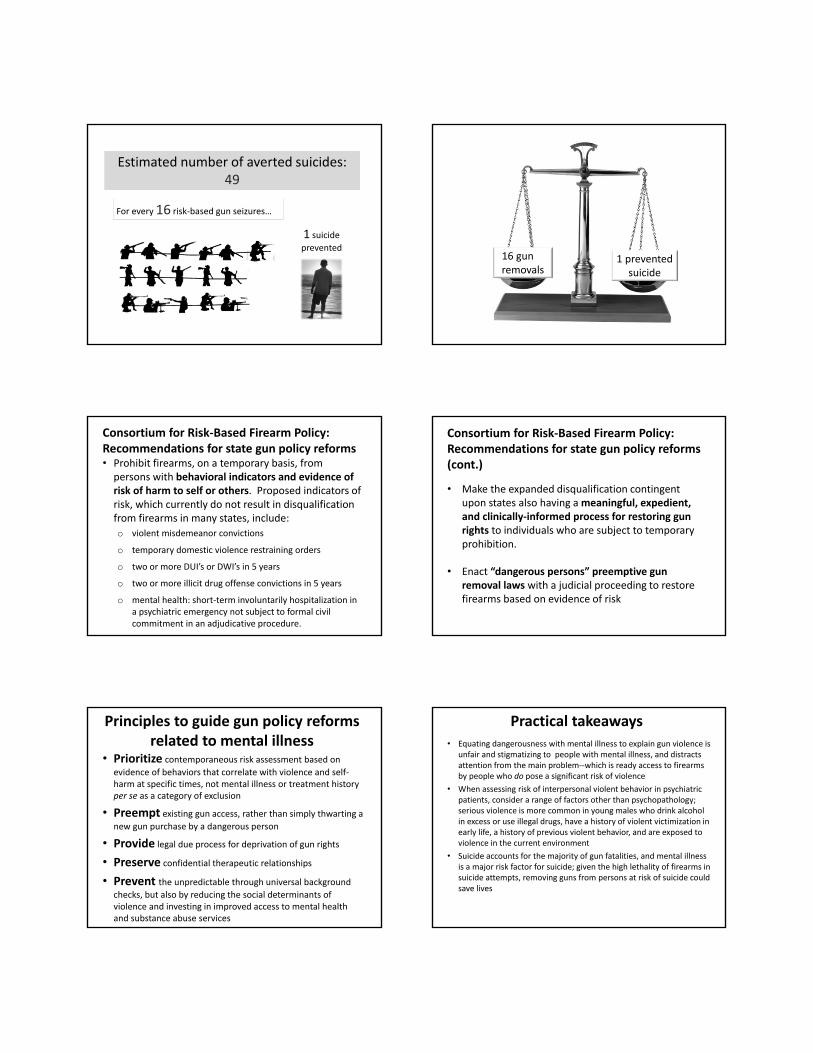
Estimated number of averted suicides: 49
Estimated number of averted suicides: 49
For every 16 risk‐based gun seizures…
1 suicide
prevented16 gun removals
1 prevented suicide
Consortium for Risk‐Based Firearm Policy: Recommendations for state gun policy reforms• Prohibit firearms, on a temporary basis, from persons with behavioral indicators and evidence of risk of harm to self or others. Proposed indicators of risk, which currently do not result in disqualification from firearms in many states, include:
o violent misdemeanor convictions
o temporary domestic violence restraining orders
o two or more DUI’s or DWI’s in 5 years
o two or more illicit drug offense convictions in 5 years
o mental health: short‐term involuntarily hospitalization in a psychiatric emergency not subject to formal civil commitment in an adjudicative procedure.
Consortium for Risk‐Based Firearm Policy: Recommendations for state gun policy reforms (cont.)
• Make the expanded disqualification contingent upon states also having a meaningful, expedient, and clinically‐informed process for restoring gun rights to individuals who are subject to temporary prohibition.
• Enact “dangerous persons” preemptive gun removal laws with a judicial proceeding to restore firearms based on evidence of risk
• Prioritize contemporaneous risk assessment based on
evidence of behaviors that correlate with violence and self‐harm at specific times, not mental illness or treatment history per se as a category of exclusion
• Preempt existing gun access, rather than simply thwarting a
new gun purchase by a dangerous person
• Provide legal due process for deprivation of gun rights
• Preserve confidential therapeutic relationships
• Prevent the unpredictable through universal background checks, but also by reducing the social determinants of violence and investing in improved access to mental health and substance abuse services
Principles to guide gun policy reforms related to mental illness • Equating dangerousness with mental illness to explain gun violence is
unfair and stigmatizing to people with mental illness, and distracts attention from the main problem‐‐which is ready access to firearms by people who do pose a significant risk of violence
• When assessing risk of interpersonal violent behavior in psychiatric patients, consider a range of factors other than psychopathology; serious violence is more common in young males who drink alcohol in excess or use illegal drugs, have a history of violent victimization in early life, a history of previous violent behavior, and are exposed to violence in the current environment
• Suicide accounts for the majority of gun fatalities, and mental illness is a major risk factor for suicide; given the high lethality of firearms in suicide attempts, removing guns from persons at risk of suicide could save lives
Practical takeaways