Jb Ja 0820202190
6
Click here to load reader
-
Upload
denuna-enjana -
Category
Documents
-
view
212 -
download
0
Transcript of Jb Ja 0820202190

VOL. 82-A, NO. 2, FEBRUARY 2000 219
A Transverse Acetabular Nonunion Treated withComputer-Assisted Percutaneous Internal Fixation
A CASE REPORT*
BY ROBERT D. ZURA, M.D.†, AND DAVID M. KAHLER, M.D.†, CHARLOTTESVILLE, VIRGINIA
Investigation performed at the Department of Orthopaedics, University of Virginia, Charlottesville
Nonunion of a fracture of the acetabulum is a rareclinical entity. The preferred treatment for this lesion isrigid internal fixation7. We present a case in which apainful nonunited transverse acetabular fracture wastreated with the use of minimally invasive, computer-assisted internal fixation with cannulated screws.
Case ReportA twenty-four-year-old woman was the unrestrained driver of an
automobile involved in a side-impact accident with another motor ve-hicle in August 1996. She had no history of medical problems and didnot smoke. She weighed more than 100 pounds (forty-five kilograms)more than her ideal body weight. Emergency evaluation at another
institution revealed a juxtatectal (directly adjacent to the weight-bearing dome) left transverse acetabular fracture with approximatelyfive millimeters of displacement (Fig. 1). On the basis of the patient’sbody habitus, nonoperative treatment was recommended and the pa-
tient was not placed in skeletal traction. She was rapidly advanced toweight-bearing with a walker as tolerated, and she progressed towalking with a cane in two months. She continued to have pain and towalk with a limp. A computed tomography scan performed in January1997 demonstrated a slightly comminuted juxtatectal transverse ace-tabular fracture with no evidence of healing across the major fractureline. Although her tolerance of weight-bearing improved gradually,the patient required a cane while walking outside of her home, whichshe did three or four days per week. Several physicians had recom-mended total hip arthroplasty on the basis of the persistent symp-toms. She was referred to us by her attorney for another opinionapproximately one year after the injury.
When first seen by us, the patient reported pain, weight gain dueto inactivity, and a persistent limp. She expressed a desire to avoidboth total hip arthroplasty and arthrodesis. The patient received a hip
score of 61 points on the self-administered questionnaire of The Hos-pital for Special Surgery3. On physical examination, she demonstratedpain at the extremes of passive motion without loss of passive motion.She had a left abductor lurch when walking without a cane.
Radiographs confirmed a nonunion of the transverse acetabularfracture with preservation of the joint space and no medial sublux-ation of the femoral head (Fig. 2). Because of the patient’s body habi-tus, it was anticipated that the operative exposures required for openfixation and bone-grafting of both columns of the acetabulum wouldbe associated with a high risk of wound complications. It was recom-mended that computer-assisted percutaneous internal fixation be at-tempted. Informed consent was obtained after a discussion of all
*No benefits in any form have been received or will be receivedfrom a commercial party related directly or indirectly to the subjectof this article. No funds were received in support of this study.
†Department of Orthopaedics, University of Virginia, McKimHall, Box 159, Charlottesville, Virginia 22908. E-mail address forD. M. Kahler: [email protected].
Copyright 2000 by The Journal of Bone and Joint Surgery, Incorporated
FIG. 1
Axial computed tomography image of the pelvis, demonstrating a juxtatectal left transverse acetabular fracture (arrows) with approximatelyfive millimeters of displacement.

THE JOURNAL OF BONE AND JOINT SURGERY
220 R. D. ZURA AND D. M. KAHLER
other options, including internal fixation and bone-grafting throughextensile or dual operative approaches.
In September 1997, the patient was taken to the operating roomfor two procedures. During the first procedure, a two-pin external fix-ator that was fitted with four aluminum spheres (fiducials) was ap-plied to the left ilium (Fig. 3). General anesthesia was used becausethe patient’s body habitus prohibited placement of the frame with lo-cal anesthesia. After the patient had recovered from the initial anes-thesia, she was taken to the computed tomography suite for scans ofthe pelvis with the attached frame (Fig. 4). The patient was then re-turned to the operating room for definitive internal fixation after re-ceiving a second general anesthetic.
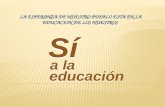
Before the second induction of anesthesia, a three-dimensionalvirtual model of the pelvis was constructed on an integrated image-guided surgical system (Stealth Station; Sofamor-Danek, Memphis,Tennessee) from the data obtained from the computed tomography.This system allows the surgeon to define a precise preoperative planfor insertion of the internal fixation pins using a line defined by identi-fying entry and exit points for each screw on the virtual model. Thesurgeon interactively modifies these planned points until the path ofthe screw traverses a safe anatomical zone across the fracture line. Thepath of intended fixation can be viewed in three dimensions on thecomputer workstation. The virtual path of the planned fixation screwmay then be displayed in two two-dimensional surgical navigationviews orthogonal to the surgical plan. These views are similar to thoseobtained during custom two-dimensional reconstructions of complexfracture patterns, but they are oriented along the intended path ofscrew placement. The length of the screw path is displayed with 0.1-millimeter accuracy (Fig. 5).
Three different surgical plans were developed for the passageof guide-wires for three 7.3-millimeter cannulated screws (SynthesUSA, Paoli, Pennsylvania). A localizing camera interfaced with thecomputer guidance system looked down onto the operating field andprecisely tracked the position of special surgical instruments fittedwith light-emitting diodes. After a second induction of general anes-thesia and sterile preparation and draping of the operative sites, anoptically tracked dynamic reference array was attached to the exter-nal fixator to allow real-time tracking of the pelvis during the opera-tive procedure. The pelvis was registered (localized) with use of anoptically tracked probe that mated with each of the aluminumspheres on the external fixator. The accuracy of registration with thissystem is routinely less than 0.5 millimeter. An optically tracked drill-guide was then used to pass the guide-wires according to the preoper-ative surgical plans. The integrated computer workstation providesvirtual real-time feedback, demonstrating the position of the drill-
guide relative to the previously determined surgical plan. Althoughlimited intraoperative fluoroscopy is used for validation of the regis-tration, the need for intraoperative fluoroscopic guidance is essen-tially eliminated.
The first guide-wire was passed perpendicular to the major frac-ture line in the supra-acetabular region. Slight compression was ap-plied with a 7.3-millimeter titanium cannulated lag screw. A secondguide-wire and lag screw were passed from the posterior aspect of theilium across the fracture into the anterior column and the superiorpubic ramus in an antegrade fashion. Finally, the hip was flexed and apercutaneous retrograde posterior-column screw was passed from theischial tuberosity into the ilium. As the pelvis was continually trackedby the dynamic reference frame, the need for repeat registration waseliminated. The external fixation (fiducial) frame was then removed.The total operative time needed for positioning, preparation, regis-tration, placement of the guide-wires according to the surgical plan,and placement of the lag screws was 105 minutes. The total time forfluoroscopic validation of registration and confirmation of guide-wireposition was thirty-five seconds. Blood loss was negligible, and thefive stab incisions were closed with single sutures. Postoperative ra-diographs confirmed accurate extra-articular placement of the screws
FIG. 2
FIG. 3
Anteroposterior and Judet radiographs of the pelvis, made one year after the injury, demonstrating nonunion (arrows) of the transverse ace-tabular fracture.
Photograph showing the patient in lateral decubitus, with the exter-nal fixator fiducial array in place on the left anterior iliac wing for in-traoperative registration. This position allows for flexion of the hipand access to the ischial tuberosity for the retrograde posterior-column screw.

TRANSVERSE ACETABULAR NONUNION TREATED WITH COMPUTER-ASSISTED INTERNAL FIXATION 221
VOL. 82-A, NO. 2, FEBRUARY 2000
in accordance with the surgical plan (Fig. 6). The patient had no com-plications and was discharged on the second postoperative day. Onlytoe-touch weight-bearing was allowed for the first six weeks, afterwhich weight-bearing was gradually increased as tolerated.
At the time of the three-month follow-up, the patient had pro-gressed to walking without aids, the pain had greatly decreased, andthe limp had resolved. At the time of the seven-month follow-up,union in the periacetabular region was noted on radiographs, al-though a faint lucency remained in the region of the ischial spine(Fig. 7). The passive range of motion of the hip was painless and un-restricted, and walking was unlimited. The maximum level of pain inthe hip in the preceding month was described as mild, and the pa-tient had not needed any over-the-counter or prescription medica-tion for pain. The self-administered questionnaire of The Hospitalfor Special Surgery revealed a hip score of 92 points. The patient wasessentially asymptomatic at the time of a fifteen-month telephonefollow-up.
Discussion
Letournel defined a nonunion of an acetabular frac-ture as a fracture that has remained unhealed for longerthan four months after the injury7. However, nonunion ofan acetabular fracture is rare; it usually occurs when thefracture is unrecognized or untreated or if there is persis-tent dislocation or subluxation of the femoral head1. Non-union occasionally occurs after operative treatment ofacetabular fractures; it occurs less commonly after non-operative treatment. Letournel reported the treatment ofeleven acetabular nonunions; six of the fractures weretransverse, three involved the posterior column, and twowere associated transverse and posterior wall fractures7.In their textbook, Letournel and Judet reported four non-unions (0.7 percent) in a series of 569 acetabular frac-tures; two were both-column fractures and two were
associated transverse and posterior wall fractures8. Mearset al. reported one case of nonunion in their series ofninety-seven patients with 100 acetabular fractures10.
Letournel noted that nonunion of the acetabulum ischaracterized by variable amounts of pain7. Nonunionis generally apparent on radiographs, with irregularityand formation of hypertrophic bone at the site of thenonunion. Fluoroscopic examination can often revealmotion at the fracture site. Spontaneous healing of anestablished acetabular nonunion without operative in-tervention has not been described, to our knowledge. Inan attempt to prevent rapid deterioration of the joint,Letournel recommended operative treatment, includ-ing decortication of hypertrophic bone from the edgesof the site of the nonunion, excision of tissue at the siteof the nonunion, reduction, bone-grafting, and stableinternal fixation.
Computer-assisted surgery is a rapidly expandingfield with tremendous potential in a variety of surgicalsubspecialties. The first neurosurgical procedures usingcomputer-integrated stereotactic imaging were carriedout during the early 1980s6. This technology has foundother applications in the fields of ophthalmology, oto-laryngology, dentistry, radiotherapy, and general sur-gery. In orthopaedic surgery, computer-assisted surgeryhas recently been applied to the placement of pediclescrews in the spine5 and to the insertion of the acetab-ular component in total hip arthroplasty2. Computer-assisted surgery has also been combined with a roboticinterface for preparation of the femoral canal in totalhip arthroplasty11. In general, however, orthopaedic
FIG. 4
Computed tomography image made immediately before the internal fixation, demonstrating persistent nonunion (arrow).

THE JOURNAL OF BONE AND JOINT SURGERY
222 R. D. ZURA AND D. M. KAHLER
surgeons have been relatively slow to embrace thisnew technology.
Several competing integrated image-guided surgerysystems are now available. Most systems employ opticaltracking of surgical instruments with digital camerasthat look down onto the operating field and are inter-faced with the computer workstation. Computed tomog-raphy data that are specific to the patient are loadedonto the workstation with use of a magnetic tape drive.With optical tracking of both the patient and the surgi-cal instruments, the position of the instruments relativeto the patient’s anatomy can be graphically representedon the workstation monitor. A precise preoperative sur-gical plan is stored by identifying the entry and targetpoints for placement of the screw on the virtual model.Two-dimensional reconstructions of the intended pathof the screw can then be generated to ensure safe ana-tomical and extra-articular positioning of the screw andfor precise determination of screw length. The surgeoncan intraoperatively orient a drill-guide or other instru-ment with respect to a previously defined surgical plan.In a cadaver trial, this technique consistently providedsufficient accuracy to allow percutaneous passage of
guide-wires into the anterior column of the acetabulumwithout the use of radiographic guidance4.
In our patient, it was possible to obtain internal fixa-tion and to promote osseous healing with a computer-assisted percutaneous technique. Because of the pa-tient’s large body habitus, we believed that the risks offormal open exposure were so great that an attempt atminimally invasive fixation was justified. The nonunionsite itself was not exposed operatively but was placed un-der compression with a lag-screw technique. A com-puter-guided technique allowed this to be accomplishedwith minimum exposure to radiation; however, two gen-eral anesthetics were required. Radiographs showed evi-dence of osseous healing, and the symptoms rapidlyresolved. Although limited intraoperative fluoroscopywas needed for validation of registration and confir-mation of safe placement of the guide-wires, the use ofcomputer assistance greatly reduced the need for intra-operative radiographic guidance. Computer-guided op-erative procedures may help to decrease the need forformal open operative exposure in the treatment of se-lected acetabular and pelvic fractures. It is hoped thatthis technology will prove useful in open acetabular pro-
FIG. 5
A screen print depicting formulation of the surgical plan for passage of a retrograde posterior-column lag screw. The image at the bottomright depicts the virtual drill-guide entering the ischial tuberosity on the three-dimensional model. The two images at the left show the surgicalplan in two views at 90 degrees to each other. The image at the upper right is perpendicular to the surgical plan at the level of the hip joint,showing safe clearance for a 7.3-millimeter cannulated screw.

TRANSVERSE ACETABULAR NONUNION TREATED WITH COMPUTER-ASSISTED INTERNAL FIXATION 223
VOL. 82-A, NO. 2, FEBRUARY 2000
cedures as well, by allowing accurate blind placement ofscrews for internal fixation without violating the hipjoint.
For percutaneous applications, it is currently neces-sary to place a small external fixator before computedtomography in order to obtain sufficient registration ac-
curacy. It is hoped that this step will be eliminated in thefuture with the development of noninvasive registrationtechniques using ultrasound or fluoroscopy. With fur-ther refinements, this technology may soon be appli-cable to many of the minimally invasive procedurescurrently being performed by orthopaedic surgeons.
References1. Coventry, M. B.: The treatment of fracture-dislocation of the hip by total hip arthroplasty. J. Bone and Joint Surg., 56-A: 1128-1134, Sept. 1974.2. DiGioia, A. M., III; O’Toole, R. V.; Jaramaz, B.; Simon, D.; Blackwell, M.; and Morgan, F.: A computer-assisted planner and intraoperative
guidance system for the accurate placement of acetabular implants. Presented at the Annual Meeting of the American Academy of Ortho-paedic Surgeons, Atlanta, Georgia, Feb. 22-26, 1996.
3. Johanson, N. A.; Charlson, M. E.; Szatrowski, T. P.; and Ranawat, C. S.: A self-administered hip-rating questionnaire for the assessment ofoutcome after total hip replacement. J. Bone and Joint Surg., 74-A: 587-597, April 1992.
4. Kahler, D. M., and Zura, R. D.: Evaluation of a computer integrated surgical technique for percutaneous fixation of transverse acetabularfractures. Lecture Notes Comput. Sci., 1205: 565-572, 1997.
FIG. 7
Radiographs made at the time of the seven-month follow-up, demonstrating healing of the nonunion and early remodeling. The femoralhead remains congruent within the acetabulum, and there is no joint-space narrowing.
FIG. 6
Postoperative iliac oblique, anteroposterior, and lateral radiographs demonstrating operative fixation with three screws. All screws areextra-articular.

THE JOURNAL OF BONE AND JOINT SURGERY
224 R. D. ZURA AND D. M. KAHLER
5. Kalfas, I. H.; Kormos, D. W.; Murphy, M. A.; McKenzie, R. L.; Barnett, G. H.; Bell, G. R.; Steiner, C. P.; Trimble, M. B.; and Weisenberger,J. P.: Application of frameless stereotaxy to pedicle screw fixation of the spine. J. Neurosurg., 83: 641-647, 1995.
6. Kelly, P. J.: Volumetric stereotactic surgical resection of intra-axial brain mass lesions. Mayo Clin. Proc., 63: 1186-1198, 1988.7. Letournel, E.: Diagnosis and treatment of nonunions and malunions of acetabular fractures. Orthop. Clin. North America, 21: 769-
788, 1990.8. Letournel, E., and Judet, R.: Fractures of the Acetabulum, pp. 541-543. New York, Springer, 1993.9. Marsh, J. L.; Buckwalter, J. A.; and Evarts, C. McC.: Delayed union, nonunion, malunion, and avascular necrosis. In Complications in Or-
thopaedic Surgery, edited by C. H. Epps. Ed. 3, pp. 183-211. Philadelphia, J. B. Lippincott, 1994.10. Mears, D. C.; Rubash, H. E.; and Sawaguchi, T.: Fractures of the acetabulum. In The Hip: Proceedings of the Thirteenth Open Scientific
Meeting of The Hip Society, pp. 95-113. St. Louis, C. V. Mosby, 1985.11. Paul, H. A.; Bargar, W. L.; Mittlestadt, B.; Musits, B.; Taylor, R. H.; Kazanzides, P.; Zuhars, J.; Williamson, B.; and Hanson, W.: Develop-
ment of a surgical robot for cementless total hip arthroplasty. Clin. Orthop., 285: 57-66, 1992.