
Intramedullary cysticercosis
5
Intramedullary cysticercosis N.K. Venkataramana*, V.K. Jain*, B.S. Das*, and T.V. Rao* * Introduction Cysticercosis is infestation of the human body by the larvae of the pork tape worm ‘Taenia Solium’. Though cerebral cysticercosis is very common in endemic areas, spinal cysticercosis is rarely seen. Among the various forms of spinal cysticercosis intramedullary cysts are extremely rare’,*. Patients with spinal cysticercosis usually present with symptoms and signs suggestive of cord compression. It is difficult to diagnose these cysts even with the help of myelography2x3. Results of surgical intervention have not been very encouraging in such patients3. We report two cases of intramedullary cysticercosis in which remarkable neurological recovery was seen after surgery. One of them is probably the first case of spinal cystocercosis reported to show exaggeration of neurological deficits dur- ing consecutive pregnancies. Case reports Case 1 A 22-year-old woman noticed stiffness and lightening pain in her right foot during the fifth month of her pregnancy. These abnormal sensa- tions gradually ascended and involved the entire right lower limb by the time of her confinement. She also developed weakness of her right foot by Summary We are reporting two cases of intramedullary cysticercus cysts. Both patients presented with a clinical picture of progressive cord compres- sion. One of them also had bilateral radicular pain. In the female patient the symptoms be- came exaggerated during her two consecutive pregnancies which is a rare and interesting ob- servation. Excision of cyst resulted in signif- icant improvement in both the patients. Key words: spinal cysticercosis, intramedul- lary cysts. this time. Pain and weakness gradually subsided spontaneously within six months after delivery. However, mild stiffness in the limb persisted for 4 years when she became pregnant again. This time immediately after delivery she developed a lightening pain in both her lower limbs and pro- gressive paraparesis, and in six months time she required support for walking. Further in the following six months, she became bed ridden and developed hesitancy of micturition. At this stage she was admitted to our institute. Examination revealed asymmetric parapare- sis with marked spasticity. Muscle power was grade II proximally and grade 0 distally in the right lower limb. It was grade III proximally and grade II distally in the left lower limb. Spinotha- * Department of Neurosurgery, * ‘Department of Neuropathology, National Institute of Mental Health and Neuro Sciences, Bangalore, India. Address for correspondence and reprint requests: V. K. Jain, Associate Professor, Dep. of Neurosurgery, Sanjay Gandhi Post Graduate Institute of Medical Sciences, P. B. No. 375, Raebareli Road, Lucknow, 226 001, India. Accepted 20.1.89 Clin Neurol Neurosurg 1989. Vol. 91-4 337
Transcript of Intramedullary cysticercosis

Intramedullary cysticercosis
N.K. Venkataramana*, V.K. Jain*, B.S. Das*, and T.V. Rao* *
Introduction
Cysticercosis is infestation of the human body by the larvae of the pork tape worm ‘Taenia Solium’. Though cerebral cysticercosis is very common in endemic areas, spinal cysticercosis is rarely seen. Among the various forms of spinal cysticercosis intramedullary cysts are extremely rare’,*. Patients with spinal cysticercosis usually present with symptoms and signs suggestive of cord compression. It is difficult to diagnose these cysts even with the help of myelography2x3. Results of surgical intervention have not been very encouraging in such patients3. We report two cases of intramedullary cysticercosis in which remarkable neurological recovery was seen after surgery. One of them is probably the first case of spinal cystocercosis reported to show exaggeration of neurological deficits dur- ing consecutive pregnancies.
Case reports
Case 1
A 22-year-old woman noticed stiffness and lightening pain in her right foot during the fifth month of her pregnancy. These abnormal sensa- tions gradually ascended and involved the entire right lower limb by the time of her confinement. She also developed weakness of her right foot by
Summary
We are reporting two cases of intramedullary cysticercus cysts. Both patients presented with a clinical picture of progressive cord compres- sion. One of them also had bilateral radicular pain. In the female patient the symptoms be- came exaggerated during her two consecutive pregnancies which is a rare and interesting ob- servation. Excision of cyst resulted in signif- icant improvement in both the patients.
Key words: spinal cysticercosis, intramedul- lary cysts.
this time. Pain and weakness gradually subsided spontaneously within six months after delivery. However, mild stiffness in the limb persisted for 4 years when she became pregnant again. This time immediately after delivery she developed a lightening pain in both her lower limbs and pro- gressive paraparesis, and in six months time she required support for walking. Further in the following six months, she became bed ridden and developed hesitancy of micturition. At this stage she was admitted to our institute.
Examination revealed asymmetric parapare- sis with marked spasticity. Muscle power was grade II proximally and grade 0 distally in the right lower limb. It was grade III proximally and grade II distally in the left lower limb. Spinotha-
* Department of Neurosurgery, * ‘Department of Neuropathology, National Institute of Mental Health and Neuro Sciences, Bangalore, India.
Address for correspondence and reprint requests: V. K. Jain, Associate Professor, Dep. of Neurosurgery, Sanjay Gandhi Post Graduate Institute of Medical Sciences, P. B. No. 375, Raebareli Road, Lucknow, 226 001, India.
Accepted 20.1.89
Clin Neurol Neurosurg 1989. Vol. 91-4
337
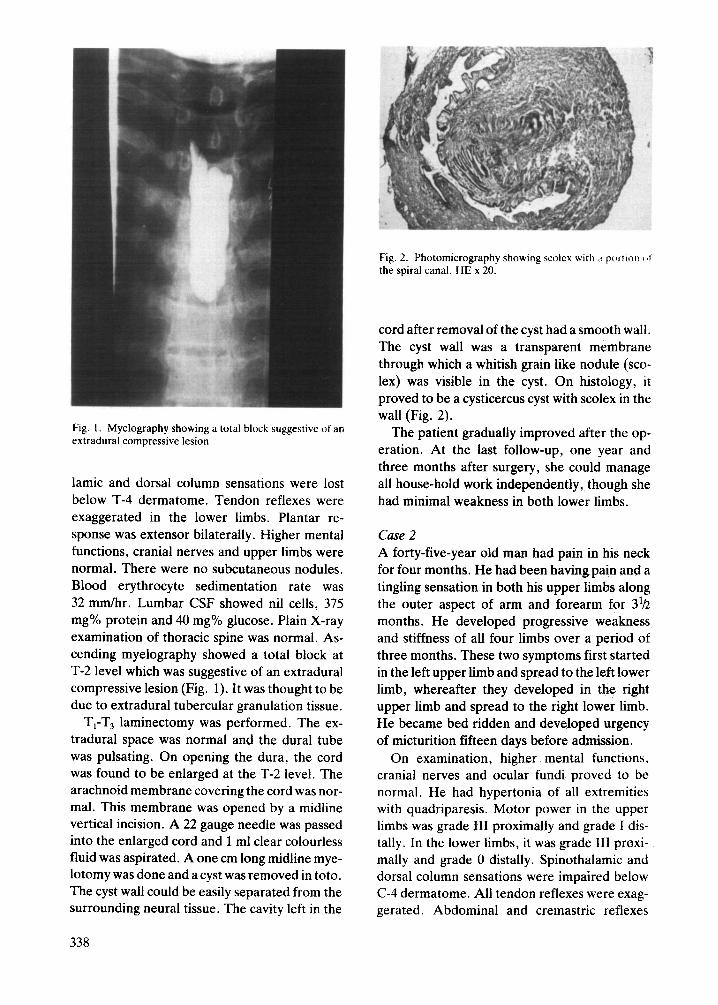
Fig. 2. Photomicrography showing scolex with ti portion $>1 the spiral canal. HE x 20.
Fig. 1. Myelography showing a total block suggestive of an extradural compressive lesion.
lamic and dorsal column sensations were lost below T-4 dermatome. Tendon reflexes were exaggerated in the lower limbs. Plantar re- sponse was extensor bilaterally. Higher mental functions, cranial nerves and upper limbs were normal. There were no subcutaneous nodules. Blood erythrocyte sedimentation rate was 32 mm/hr. Lumbar CSF showed nil cells, 375 mg% protein and 40 mg% glucose. Plain X-ray examination of thoracic spine was normal. As- cending myelography showed a total block at T-2 level which was suggestive of an extradural compressive lesion (Fig. 1). It was thought to be due to extradural tubercular granulation tissue.
T,-T, laminectomy was performed. The ex- tradural space was normal and the dural tube was pulsating. On opening the dura, the cord was found to be enlarged at the T-2 level. The arachnoid membrane covering the cord was nor- mal. This membrane was opened by a midline vertical incision. A 22 gauge needle was passed into the enlarged cord and 1 ml clear colourless fluid was aspirated. A one cm long midline mye- lotomy was done and a cyst was removed in toto. The cyst wall could be easily separated from the surrounding neural tissue. The cavity left in the
cord after removal of the cyst had a smooth wall. The cyst wall was a transparent membrane through which a whitish grain like nodule (sco- lex) was visible in the cyst. On histology, it proved to be a cysticercus cyst with scolex in the wall (Fig. 2).
The patient gradually improved after the op- eration. At the last follow-up, one year and three months after surgery, she could manage all house-hold work independently, though she had minimal weakness in both lower limbs.
Case 2 A forty-five-year old man had pain in his neck for four months. He had been having pain and a tingling sensation in both his upper limbs along the outer aspect of arm and forearm for 3’h months. He developed progressive weakness and stiffness of all four limbs over a period of three months. These two symptoms first started in the left upper limb and spread to the left lower limb, whereafter they developed in the right upper limb and spread to the right lower limb. He became bed ridden and developed urgency of micturition fifteen days before admission.
On examination, higher mental functions, cranial nerves and ocular fundi proved to be normal. He had hypertonia of all extremities with quadriparesis. Motor power in the upper limbs was grade III proximally and grade I dis- tally. In the lower limbs, it was grade III proxi- mally and grade 0 distally. Spinothalamic and dorsal column sensations were impaired below C-4 dermatome. All tendon reflexes were exag- gerated. Abdominal and cremastric reflexes
338
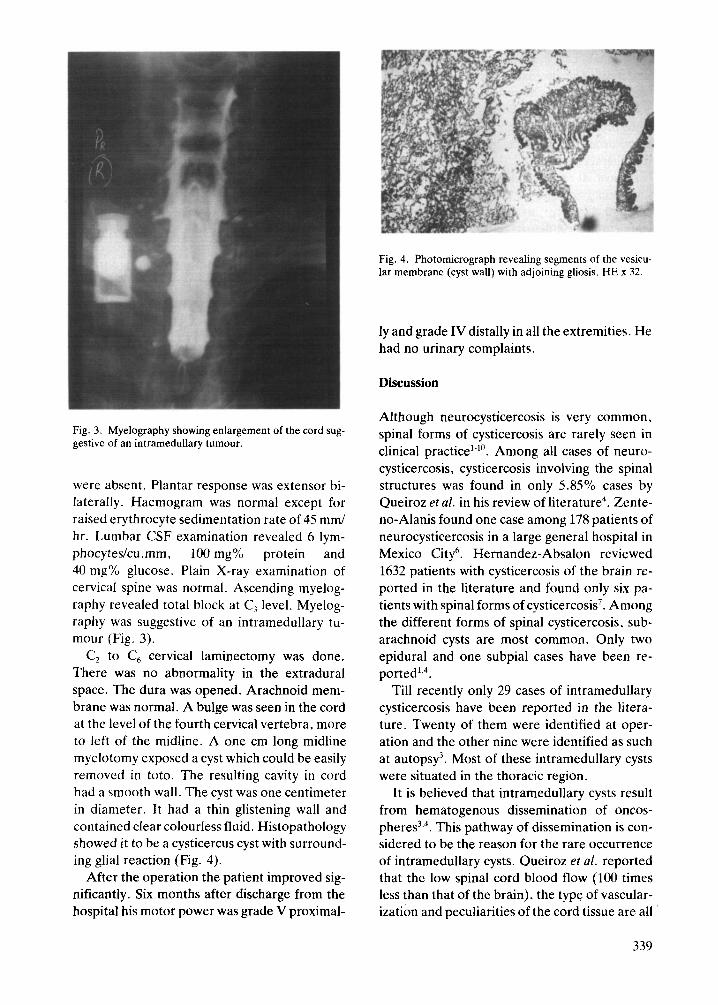
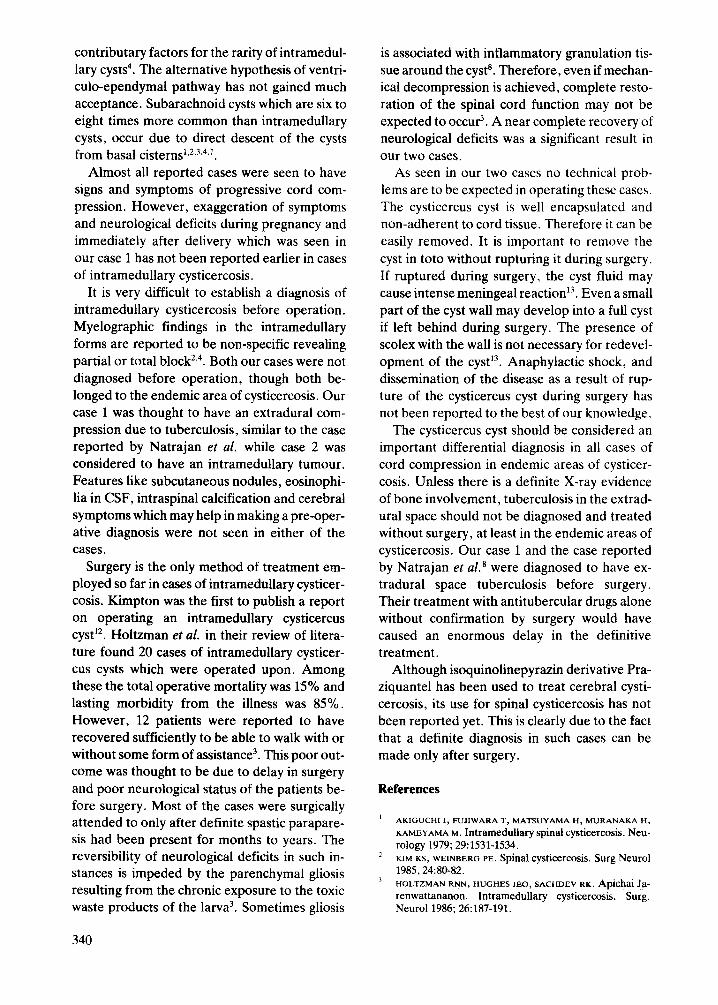
Fig. 3. Myelography showing enlargement of the cord sug- gestive of an intramedullary tumour.
were absent. Plantar response was extensor bi- laterally. Haemogram was normal except for raised erythrocyte sedimentation rate of 45 mm/ hr. Lumbar CSF examination revealed 6 lym- phocytes/cu. mm, 100 mg% protein and 40 mg% glucose. Plain X-ray examination of cervical spine was normal. Ascending myelog- raphy revealed total block at C, level. Myelog- raphy was suggestive of an intramedullary tu- mour (Fig. 3).
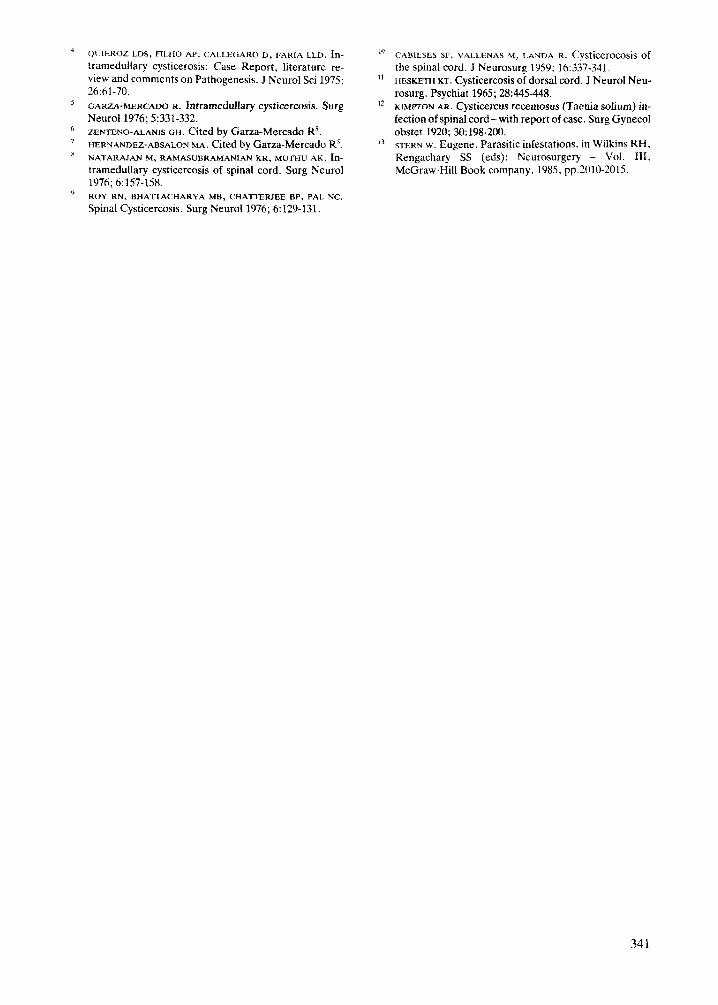
C, to C, cervical laminectomy was done. There was no abnormality in the extradural space. The dura was opened. Arachnoid mem- brane was normal. A bulge was seen in the cord at the level of the fourth cervical vertebra, more to left of the midline. A one cm long midline myelotomy exposed a cyst which could be easily removed in toto. The resulting cavity in cord had a smooth wall. The cyst was one centimeter in diameter. It had a thin glistening wall and contained clear colourless fluid. Histopathology showed it to be a cysticercus cyst with surround- ing glial reaction (Fig. 4).
After the operation the patient improved sig- nificantly. Six months after discharge from the hospital his motor power was grade V proximal-
Fig. 4. Photomicrograph revealing segments of the vesicu- lar membrane (cyst wall) with adjoining gliosis. HE x 32.
ly and grade IV distally in all the extremities. He had no urinary complaints.
Discussion
Although neurocysticercosis is very common, spinal forms of cysticercosis are rarely seen in clinical practice’-“. Among all cases of neuro- cysticercosis, cysticercosis involving the spinal structures was found in only 5.85% cases by Queiroz et al. in his review of literature4. Zente- no-Alanis found one case among 178 patients of neurocysticercosis in a large genera1 hospital in Mexico City6. Hernandez-Absalon reviewed 1632 patients with cysticercosis of the brain re- ported in the literature and found only six pa- tients with spinal forms of cysticercosis’. Among the different forms of spinal cysticercosis, sub- arachnoid cysts are most common. Only two epidural and one subpial cases have been re- ported’.4.
Till recently only 29 cases of intramedullary cysticercosis have been reported in the litera- ture. Twenty of them were identified at oper- ation and the other nine were identified as such at autopsy3. Most of these intramedullary cysts were situated in the thoracic region.
It is believed that intramedullary cysts result from hematogenous dissemination of oncos- pheres . 3-4 This pathway of dissemination is con- sidered to be the reason for the rare occurrence of intramedullary cysts. Queiroz et al. reported that the low spinal cord blood flow (100 times less than that of the brain), the type of vascular- ization and peculiarities of the cord tissue are all
339
contributary factors for the rarity of intramedul- lary cysts4. The alternative hypothesis of ventri- culo-ependymal pathway has not gained much acceptance. Subarachnoid cysts which are six to eight times more common than intramedullary cysts, occur due to direct descent of the cysts from basal cisterns1.2~“*4~7.
Almost all reported cases were seen to have signs and symptoms of progressive cord com- pression. However, exaggeration of symptoms and neurological deficits during pregnancy and immediately after delivery which was seen in our case 1 has not been reported earlier in cases of intramedullary cysticercosis.
It is very difficult to establish a diagnosis of intramedullary cysticercosis before operation. Myelographic findings in the intramedullary forms are reported to be non-specific revealing partial or total block2.4. Both our cases were not diagnosed before operation, though both be- longed to the endemic area of cysticercosis. Our case 1 was thought to have an extradural com- pression due to tuberculosis, similar to the case reported by Natrajan et al. while case 2 was considered to have an intramedullary tumour. Features like subcutaneous nodules, eosinophi- lia in CSF, intraspinal calcification and cerebral symptoms which may help in making a pre-oper- ative diagnosis were not seen in either of the cases.
Surgery is the only method of treatment em- ployed so far in cases of intramedullary cysticer- cosis. Kimpton was the first to publish a report on operating an intramedullary cysticercus cyst . l2 Holtzman ef al. in their review of litera- ture found 20 cases of intramedullary cysticer- cus cysts which were operated upon. Among these the total operative mortality was 15% and lasting morbidity from the illness was 85%. However, 12 patients were reported to have recovered sufficiently to be able to walk with or without some form of assistance3. This poor out- come was thought to be due to delay in surgery and poor neurological status of the patients be- fore surgery. Most of the cases were surgically attended to only after definite spastic parapare- sis had been present for months to years. The reversibility of neurological deficits in such in- stances is impeded by the parenchymal gliosis resulting from the chronic exposure to the toxic waste products of the larva3. Sometimes gliosis
is associated with inflammatory granulation tis- sue around the cyst’. Therefore, even if mechan- ical decompression is achieved, complete resto- ration of the spinal cord function may not be expected to occuti. A near complete recovery of neurological deficits was a significant result in our two cases.
As seen in our two cases no technical prob- lems are to be expected in operating these cases. The cysticercus cyst is well encapsulated and non-adherent to cord tissue. Therefore it can be easily removed. It is important to remove the
cyst in toto without rupturing it during surgery. If ruptured during surgery, the cyst fluid may cause intense meningeal reaction13. Even a small part of the cyst wall may develop into a full cyst if left behind during surgery. The presence of scolex with the wall is not necessary for redevel- opment of the cyst l3 Anaphylactic shock, and .
dissemination of the disease as a result of rup- ture of the cysticercus cyst during surgery has not been reported to the best of our knowledge.
The cysticercus cyst should be considered an important differential diagnosis in all cases of cord compression in endemic areas of cysticer- cosis. Unless there is a definite X-ray evidence of bone involvement, tuberculosis in the extrad- ural space should not be diagnosed and treated without surgery, at least in the endemic areas of cysticercosis. Our case 1 and the case reported by Natrajan et aLs were diagnosed to have ex- tradural space tuberculosis before surgery. Their treatment with antitubercular drugs alone without confirmation by surgery would have caused an enormous delay in the definitive treatment.
Although isoquinolinepyrazin derivative Pra- ziquantel has been used to treat cerebral cysti- cercosis, its use for spinal cysticercosis has not been reported yet. This is clearly due to the fact that a definite diagnosis in such cases can be made only after surgery.
References
AKIGUCHI I, NJIwARA T, MATSUYAMA H, MURANAKA H,
KAMEYAMA M. Intramedullary spinal cysticercosis. Neu- rology 1979; 29:1.531-1534. KIM KS, WEINBERG PE. Spinal CyStiCCrCOSiS. SUrg Neurol 1985,24:80-82. HOLTZMAN RNN, HUGHES JEO, SACHDEV RK. Apichai Ja- renwattananon. Intramedullary cysticercosis. Surg. Neurol 1986; 26:187-191.
340
h
OUIEROZ LDS,FILHO AP,CALLEGARO D,FARIA LLD. fn- tramedullary cysticerosis: Case Report, literature re- view and comments on Pathogenesis. J Nemo1 Sci 1975; 26:61-70. GARZA-MERCADO R. Intramedullary cysticercosis. Surg Neural 1976; 5:331-332. ZEWIENO-ALANIS GH. Cited by Garza-Mercado Rs. HERNANDEZ-ABSALON MA. Cited by Garza-Mercado Rs. NATARAJAN M,RAMA~UBRAMANIANKR, ~uniu AK. In- tramedullary cysticercosis of spinal cord. Surg Neurol 1976; 6:157-158. ROY RN,BUAlTACHARYA MB,CHATTERJEE BP,PALNC.
Spinal Cysticercosis. Surg Nemo1 1976; 6129-131.
'" CABiESES SF, VALLENAS M, LANDA R. CyStiCCrOCOSiS Of
the spinal cord. J Neurosurg 1959; 16:337-341. ‘t HESKETH KT. Cysticercosis of dorsal cord. J Neural Neu-
rosurg. Psychiat 1965; 28445~448. I2 KIMPTON AR. Cysticercus recemosus (Taenia solium) in-
fection of spinal cord-with report of case. Surg Gynecol obstet 1920; 30:198-200.
‘) STERN w. Eugene, Parasitic infestations. in Wiikins RH, Rengachary SS (eds): Neurosurgery - Vol. IfI, McGraw-Hill Book company. 1985. pp.ZOlO-2015.
341


















