Intra-abdominal reactive lymphadenopathy...
5
165 Case Report Kitasato Med J 2012; 42: 165-169 Intra-abdominal reactive lymphadenopathy developing 5 years after endoscopic submucosal dissection for early gastric cancer Kenji Ishido, 1 Satoshi Tanabe, 1 Yuki Shimizu, 1 Akira Naruke, 1 Wasaburo Koizumi, 1 Shinichi Sakuramoto, 2 Tetsuo Mikami 3 1 Department of Gastroenterology, Kitasato University School of Medicine 2 Department of Surgery, Kitasato University School of Medicine 3 Department of Pathology, Kitasato University School of Medicine A 73-year-old man presented with an enlarged intraperitoneal lymph node. In 2003, endoscopic submucosal dissection had been performed for an early gastric cancer that complied with current guidelines for endoscopic treatment. The lesion was completely resected en bloc, curative endoscopic submucosal dissection. The patient was followed up on an outpatient basis, with no evidence of metastasis or recurrence. In November 2008, abdominal ultrasonography during a medical check-up showed an enlarged lymph node, about 20 mm in diameter. Computed tomography and positron emission tomography showed no contrast effects or abnormal accumulations of tracer in the affected region, but malignancy could not be ruled out. In August 2009, laparoscopic intra-abdominal lymphadenectomy was performed. Histopathological examination revealed no atypical cells, and reactive lymphadenopathy was diagnosed. The patient was followed up on an outpatient basis and currently remains well, with no recurrence. Key words: lymphadenopathy, early gastric cancer, laparoscopic lymphadenectomy Introduction ntra-abdominal lymphadenopathy can be caused by various factors, irrespective of malignant or nonmalignant disease. However, it is often difficult to determine whether abdominal lymphadenopathy is associated with benign or malignant disease solely on the basis of imaging studies. Differential diagnosis is particularly challenging in the presence of a solitary enlarged lymph node in patients with no clear-cut evidence of a primary lesion. Endoscopic mucosal resection (EMR) of early gastric cancer (EGC) with no risk of lymph node metastasis has been a standard technique in Japan. 1 Empirical indications for EMR have been: 1. papillary or tubular (differentiated) adenocarcinoma, 2. a lesion less than 2 cm in diameter, 3. no ulceration within the tumor, and 4. no lymphatic or vessel involvement. 2 In 2006, endoscopic submucosal dissection (ESD) was approved by the National Heath Insurance system in Japan for the treatment of early gastric cancer EGC. 3 Recently, attempts have been made to expand the indication range of ESD to include ulcerative or larger lesions, which are difficult to resect by conventional EMR. 2,4 This was a rare case of intra-abdominal reactive lymphadenopathy associated with a lymph node about 20 mm in diameter that developed 5 years after curative ESD for EGC. Case Report The patient was a 73-year-old man who presented with an enlarged intra-abdominal lymph node. In February 2003, a poorly demarcated, superficial and slightly depressed type (0-IIc) lesion was found in the greater curvature of the lower gastric body, and ESD was performed (Figure 1A). Histopathological examination revealed a superficial and slightly depressed type (0-IIc), well-differentiated tubular (tub1), intramucosal carcinoma, measuring 15 × 14 mm, with no ulcer or vascular invasion. The lateral and deep margins were tumor negative (Figure 2A-D). The lesion complied with current guidelines for endoscopic therapy and was completely resected en bloc. 4 Subsequently, the patient I Received 29 June 2012, accepted 3 August 2012 Correspondence to: Kenji Ishido, Department of Gastroenterology, Kitasato University School of Medicine 2-1-1 Asamizodai, Minami-ku, Sagamihara, Kanagawa 252-0380, Japan E-mail: [email protected]
Transcript of Intra-abdominal reactive lymphadenopathy...

165
Case Report Kitasato Med J 2012; 42: 165-169
Intra-abdominal reactive lymphadenopathy developing 5 years afterendoscopic submucosal dissection for early gastric cancer
Kenji Ishido,1 Satoshi Tanabe,1 Yuki Shimizu,1 Akira Naruke,1
Wasaburo Koizumi,1 Shinichi Sakuramoto,2 Tetsuo Mikami3
1 Department of Gastroenterology, Kitasato University School of Medicine2 Department of Surgery, Kitasato University School of Medicine3 Department of Pathology, Kitasato University School of Medicine
A 73-year-old man presented with an enlarged intraperitoneal lymph node. In 2003, endoscopicsubmucosal dissection had been performed for an early gastric cancer that complied with currentguidelines for endoscopic treatment. The lesion was completely resected en bloc, curative endoscopicsubmucosal dissection. The patient was followed up on an outpatient basis, with no evidence ofmetastasis or recurrence. In November 2008, abdominal ultrasonography during a medical check-upshowed an enlarged lymph node, about 20 mm in diameter. Computed tomography and positronemission tomography showed no contrast effects or abnormal accumulations of tracer in the affectedregion, but malignancy could not be ruled out. In August 2009, laparoscopic intra-abdominallymphadenectomy was performed. Histopathological examination revealed no atypical cells, andreactive lymphadenopathy was diagnosed. The patient was followed up on an outpatient basis andcurrently remains well, with no recurrence.
Key words: lymphadenopathy, early gastric cancer, laparoscopic lymphadenectomy
Introduction
ntra-abdominal lymphadenopathy can be caused byvarious factors, irrespective of malignant or
nonmalignant disease. However, it is often difficult todetermine whether abdominal lymphadenopathy isassociated with benign or malignant disease solely onthe basis of imaging studies. Differential diagnosis isparticularly challenging in the presence of a solitaryenlarged lymph node in patients with no clear-cutevidence of a primary lesion.
Endoscopic mucosal resection (EMR) of early gastriccancer (EGC) with no risk of lymph node metastasis hasbeen a standard technique in Japan.1 Empirical indicationsfor EMR have been: 1. papillary or tubular (differentiated)adenocarcinoma, 2. a lesion less than 2 cm in diameter,3. no ulceration within the tumor, and 4. no lymphatic orvessel involvement.2 In 2006, endoscopic submucosaldissection (ESD) was approved by the National HeathInsurance system in Japan for the treatment of early gastriccancer EGC.3 Recently, attempts have been made toexpand the indication range of ESD to include ulcerative
or larger lesions, which are difficult to resect byconventional EMR.2,4
This was a rare case of intra-abdominal reactivelymphadenopathy associated with a lymph node about20 mm in diameter that developed 5 years after curativeESD for EGC.
Case Report
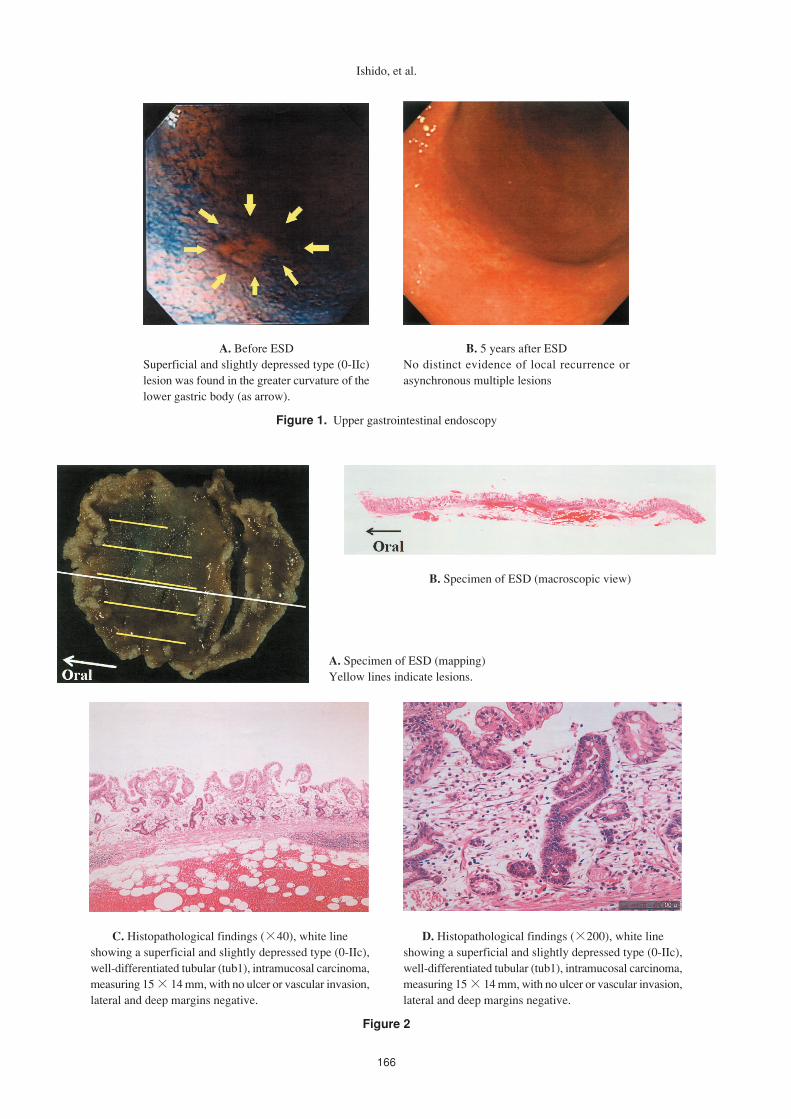
The patient was a 73-year-old man who presented withan enlarged intra-abdominal lymph node. In February2003, a poorly demarcated, superficial and slightlydepressed type (0-IIc) lesion was found in the greatercurvature of the lower gastric body, and ESD wasperformed (Figure 1A). Histopathological examinationrevealed a superficial and slightly depressed type (0-IIc),well-differentiated tubular (tub1), intramucosalcarcinoma, measuring 15 × 14 mm, with no ulcer orvascular invasion. The lateral and deep margins weretumor negative (Figure 2A-D). The lesion complied withcurrent guidelines for endoscopic therapy and wascompletely resected en bloc.4 Subsequently, the patient
I
Received 29 June 2012, accepted 3 August 2012Correspondence to: Kenji Ishido, Department of Gastroenterology, Kitasato University School of Medicine2-1-1 Asamizodai, Minami-ku, Sagamihara, Kanagawa 252-0380, JapanE-mail: [email protected]
166
Figure 2
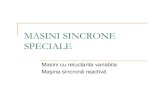
Figure 1. Upper gastrointestinal endoscopy
Ishido, et al.
A. Before ESDSuperficial and slightly depressed type (0-IIc)lesion was found in the greater curvature of thelower gastric body (as arrow).
B. 5 years after ESDNo distinct evidence of local recurrence orasynchronous multiple lesions
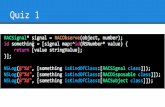
A. Specimen of ESD (mapping)Yellow lines indicate lesions.
B. Specimen of ESD (macroscopic view)
C. Histopathological findings (×40), white lineshowing a superficial and slightly depressed type (0-IIc),well-differentiated tubular (tub1), intramucosal carcinoma,measuring 15 × 14 mm, with no ulcer or vascular invasion,lateral and deep margins negative.
D. Histopathological findings (×200), white lineshowing a superficial and slightly depressed type (0-IIc),well-differentiated tubular (tub1), intramucosal carcinoma,measuring 15 × 14 mm, with no ulcer or vascular invasion,lateral and deep margins negative.
167
Figure 4
Reactive lymphadenopathy after ESD
was followed up on an outpatient basis. To check forlocal recurrence around the scar formed at the site ofendoscopic therapy, upper gastrointestinal endoscopy wasperformed 2, 6, and 12 months after treatment and at 12-month intervals thereafter. To confirm the presence orabsence of distant metastasis, abdominal ultrasonographywas performed at 12-month intervals. There was noevidence of metastasis or recurrence. However, inNovember 2008, abdominal ultrasonography during amedical check-up revealed an enlarged lymph node inthe abdomen, and the patient was referred to ourdepartment. He had a history of hypertension and diabetesmellitus.
Physical examination showed no clinically significantfindings. On laboratory tests, the fasting blood glucosewas 281 mg/dL, the hemoglobin A1c level was 7.6%,and the urine glucose was +4. There were no clinicallysignificant increases in the levels of interleukin-2 receptoror tumor markers in serum.
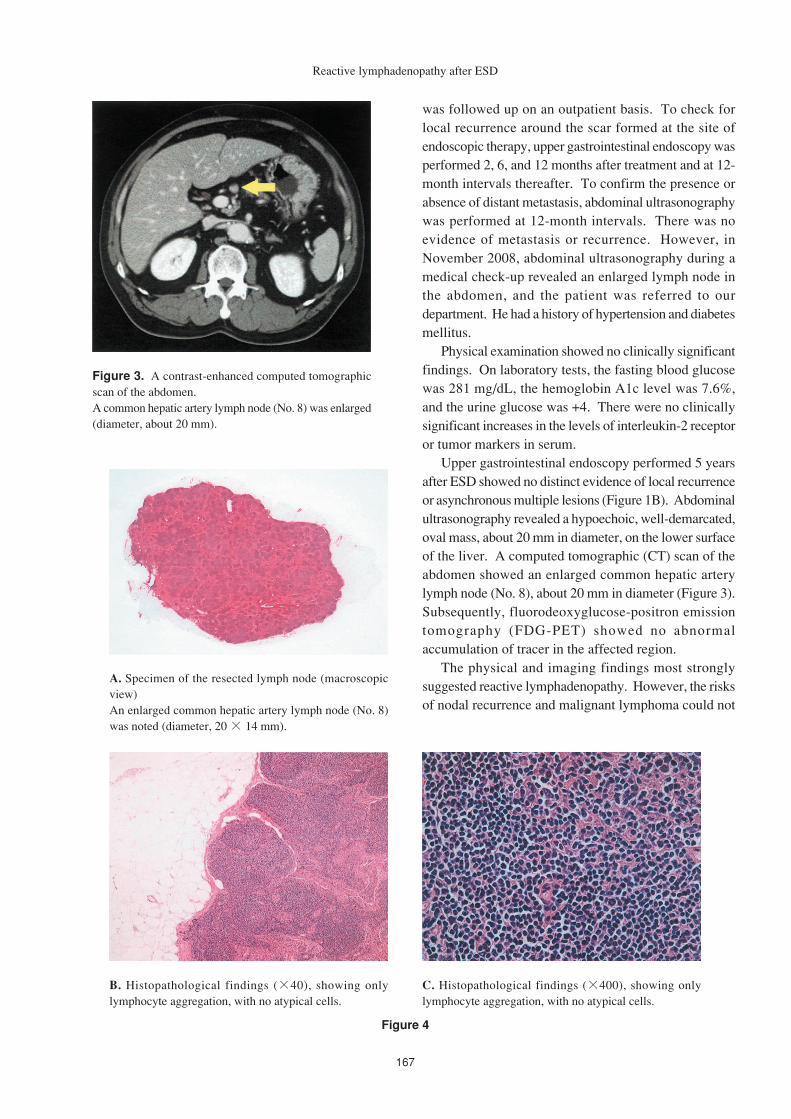
Upper gastrointestinal endoscopy performed 5 yearsafter ESD showed no distinct evidence of local recurrenceor asynchronous multiple lesions (Figure 1B). Abdominalultrasonography revealed a hypoechoic, well-demarcated,oval mass, about 20 mm in diameter, on the lower surfaceof the liver. A computed tomographic (CT) scan of theabdomen showed an enlarged common hepatic arterylymph node (No. 8), about 20 mm in diameter (Figure 3).Subsequently, fluorodeoxyglucose-positron emissiontomography (FDG-PET) showed no abnormalaccumulation of tracer in the affected region.
The physical and imaging findings most stronglysuggested reactive lymphadenopathy. However, the risksof nodal recurrence and malignant lymphoma could not
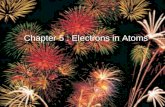
Figure 3. A contrast-enhanced computed tomographicscan of the abdomen.A common hepatic artery lymph node (No. 8) was enlarged(diameter, about 20 mm).
A. Specimen of the resected lymph node (macroscopicview)An enlarged common hepatic artery lymph node (No. 8)was noted (diameter, 20 × 14 mm).
B. Histopathological findings (×40), showing onlylymphocyte aggregation, with no atypical cells.
C. Histopathological findings (×400), showing onlylymphocyte aggregation, with no atypical cells.

168
be ruled out. We did not perform endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) or CT-guidedFNA in this patient because it was difficult to secure apuncture route. After receiving informed consent fromthe patient and his family, laparoscopic intra-abdominallymphadenectomy was performed to obtain a definitivediagnosis in August 2009. Histopathological examinationof the resected lymph node showed no distinctly atypicalcells. Only lymphocyte aggregation was present (Figure4A-C). Reactive lymphadenopathy was diagnosed onthe basis of these findings. The patient is currentlyfollowed up on an outpatient basis.
Discussion
This patient had an enlarged intra-abdominal lymph node,about 20 mm in diameter, that developed 5 years aftercurative ESD for EGC. The incidence of lymph-nodemetastasis associated with intramucosal cancer is about3%.2,5 However, Gotoda et al.2,4 reported that differentiatedcancers unaccompanied by vascular invasion or an ulcerhave a negligible risk of lymph-node metastasis if thelesion is intramucosal, irrespective of tumor size. Thepatient had a differentiated type, intramucosal cancer, 15mm in diameter, with no ulcer or vascular invasion.Because the lesion complied with current guidelines andcould be completely resected en bloc, we considered therisk of lymph-node metastasis after ESD to be negligible.In our patient, intra-abdominal lymphadenopathy wasnot associated with distinct accumulation of tracer onFDG-PET. We therefore considered observation withno further treatment, but the shortest diameter of thetumor was 20 mm, and the possibility of a malignanttumor could not be excluded.
Intra-abdominal lymphadenopathy can be broadlyclassified into malignant lymphadenopathy and reactivelymphadenopathy. Malignant lymphadenopathy iscaused by metastasis from gastric cancer or other solidtumors or hematopoietic tumors, such as leukemia ormalignant lymphoma. Reactive lymphadenopathy iscaused by infection, such as bacteria or virus, tuberculosis,HIV (Human immunodeficiency virus) or inflammation,such as Crohn's disease or cholecystitis, pancreatitis, ordrug allergy.6 In this patient, histopathologicalexamination of lymph-node biopsy specimens showedno atypical cells, supporting the diagnosis of reactivelymphadenopathy. Although the underlying causesremain unclear, the patient's diabetes mellitus was poorlycontrolled, suggesting that increased susceptibility toinfection had a role in the development of reactivelymphadenopathy.
A recent study has reported that EUS-FNA biopsy ofabdominal lymph nodes can facilitate a definitivediagnosis.7 We did not perform EUS-FNA for this patientbecause it was difficult to secure a puncture route. Insteadwe performed a laparoscopic lymphadenectomy to resectthe enlarged lymph node. Because the presence of ametastatic tumor or malignant lymphoma would haverequired continued treatment, and both CT and PETsuggested an isolated solid tumor 20 mm in diameterwith no tumors at any other site, we decided to performminimally invasive laparoscopic lymphadenectomyrather than open surgery.8-12
The present case was a rare case of intra-abdominalreactive lymphadenopathy associated with a lymph nodeabout 20 mm in diameter that had developed 5 yearsafter curative ESD for EGC. We believe that laparoscopicintra-abdominal lymphadenectomy are useful techniquesfor a intra-abdominal lymph-node biopsy and a definitivediagnosis.
References
1. The Japanese Gastric Cancer Society: Guidelines fordiagnosis and treatment of carcinoma of the stomach.2010 edition.
2. Gotoda T, Yanagisawa A, Sasako M, et al. Incidenceof lymph node metastasis from early gastric cancer:estimation with a large number of cases at two largecenters. Gastric Cancer 2000; 3: 219-25.
3. Ono H, Kondo H, Gotoda T, et al. Endoscopicmucosal resection for treatment of early gastriccancer. Gut 2001; 48: 225-9.
4. Gotoda T. Endoscopic resection of early gastriccancer. Gastric Cancer 2007; 10: 1-11.
5. Yamao T, Shirao K, Ono H, et al. Risk factors forlymph node metastasis from intramucosal gastriccarcinoma. Cancer 1996; 77: 602-6.
6. Lucey BC, Stuhlfaut JW, Sato JA. Mesenteric lymphnodes seen at imaging: causes and significance.Radiographics 2005; 25: 351-65.
7. Nakahara O, Yamao K, Bhatia V, et al. Usefulnessof endoscopic ultrasound-guided fine needleaspiration (EUS-FNA) for undiagnosed intra-abdominal lymphadenopathy. J Gastroenterol 2009;44: 562-7.
8. Liao YT, Wu MH, Wang MY, et al. Gaslesslaparoscopy-assisted surgery for intraabdominal/retroperitonealtumor of unknown origin: a bridgebetween total laparoscopic surgery and conventionalopen surgery. J Laparoendosc Adv Surg Tech A2010; 20: 825-30.
Ishido, et al.

169
9. Hesselmann V, Zähringer M, Krug B, et al.Computed-tomography-guided percutaneous coreneedle biopsies of suspected malignant lymphomas:Impact of biopsy, lesion, and patient parameters ondiagnostic yield. Acta Radiol 2004; 45: 641-5.
10. Balestreri L, Morassut S, Bernardi D, et al. Efficacyof CT-guided percutaneous needle biopsy in thediagnosis of malignant lymphoma at firstpresentation. Clin Imaging 2005; 29: 123-7.
11. Diulus L, Chalikonda S, Pitt T, et al. Efficacy oflaparoscopic mesenteric/retroperitoneal lymph nodebiopsy. Surg Endosc 2009; 23: 389-93.
12. Strong VE, Devaud N, Allen PJ, et al. Laparoscopicv e r s u s o p e n s u b t o t a l g a s t r e c t o m y f o radenocarcinoma: a case-control study. Ann SurgOncol 2009; 16: 1507-13.
Reactive lymphadenopathy after ESD