Intermittent claudication
12
Systemic review of treatment of intermi1ent claudica5on in the lower extremi5es RFS Journal Primer
-
Upload
dmd213 -
Category
Health & Medicine
-
view
38 -
download
2
Transcript of Intermittent claudication
Systemic review of treatment of intermi1ent claudica5on in the lower extremi5es
RFS Journal Primer
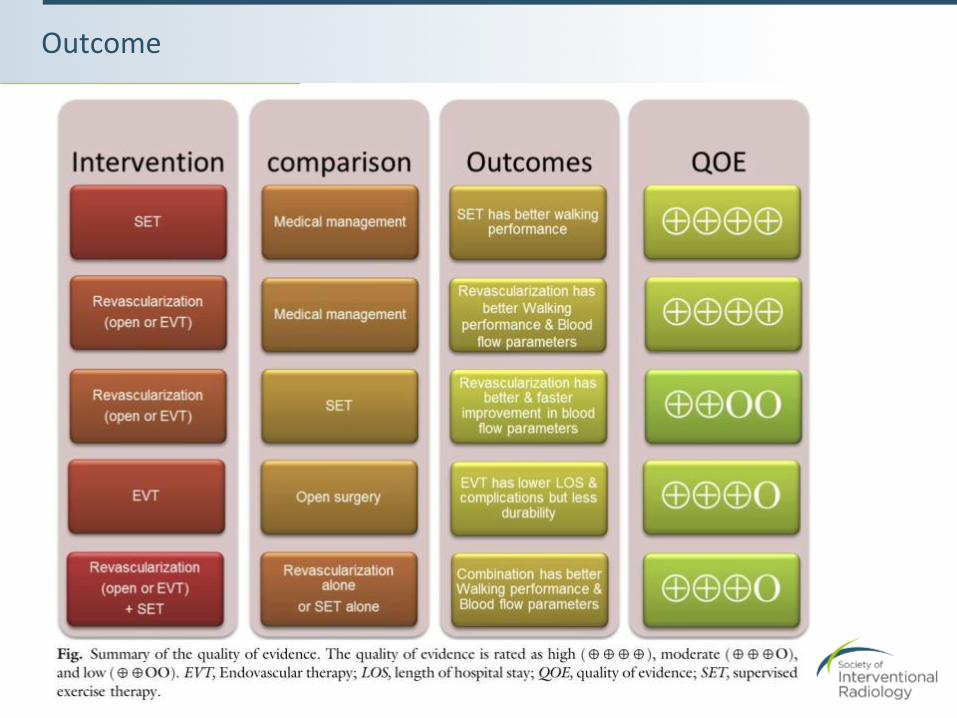
BOTTOM LINE • Given the limited research, supervised exercise therapy, endovascular therapy, and open surgery are
superior to medical management in terms of walking distance, pain, and claudication. • Blood Alow parameters (ABI) improved faster and better with both forms of revascularization, which
may not necessarily correlated with clinical improvement. MAJOR POINTS • High quality evidence from 2 Cochrane systematic trials favoring supervised exercise therapy (SET)
for improved walking performance • High quality evidence favoring revascularization as compared to optimal medical therapy (OMT) for
improved walking performance and blood Alow parameters • Low quality evidence showing better/faster improvement in ABI with revascularization (open or
PTA) as compared to SET • Moderate evidence showing increase in 30-‐day morbidity and mortality, longer length of stay, higher
complication rate, but increase in durability and patency in open surgery compared to PTA • Limited studies demonstrating higher mean cost of PTA compared to SET
CRITICISM
• Limited number of trials and systematic reviews from which to draw conclusions
Quick Summary
Meta-‐analysis of multiple RCTs and systematic reviews • A total of 1548 patients in a total of 12 trials. • A total of 8 systematic reviews were evaluated (3 Cochrane reviews on exercise
therapy, 2 on SET with endovascular therapy, and 3 of nonrandomized surgical case series)
• The median length of follow-‐up was 15 months
INCLUSION CRITERIA • Randomized trials or systematic reviews • Enrolled patients with claudication (ie, symptomatic patients with peripheral
vascular disease who had exertional pain with walking) • Evaluated open bypass, endovascular revascularization, or exercise therapy • Measured the outcomes of interest
EXCLUSION CRITERIA • Duplicates, no original data, or ab irrelevant population (ie: patients with CLI)
Study design

• To evaluate the available modalities currently in practice to treat patients with claudication with respect to their efAicacy.
Purpose
• RCTs and systematic reviews comparing medical management, supervised exercise therapy (SET), endovascular treatment, and open bypass
• Metrics evaluated were • Mortality/morbidity
• Amputation
• QOL
• Walking distance
• ABI
• Patency
• Cost
Interven7on
Outcome
• Exercise therapy • 2 systematic reviews, a total of 2818 patients from 44 RCTs
• Outcomes • Exercise signiAicantly improved maximal walking distance and time compared with usual care or
placebo (including pentoxifylline, iloprost, antiplatelet agents and vitamin E, or pneumatic calf compression). Improvements persisted over 2 years.
• Supervised therapy translated to an increase in walking distance of 180 meters as compared to non-‐supervised therapy
• Comparing endovascular therapy with medical management • MIMIC trial: PTA vs no PTA in patients already in SET programs, follow up for 24
months • PTA group had higher adjusted walking distance and ABI, but not QOL
• Creasy et al, 1990: PTA vs SET, follow-‐up 9-‐10 months • SET lead to better mean claudicating distance. PTA had initial improvement for 3 months
without subsequent improvement. SET continued to improved over 15 months.
• Nylaende et al, 2007: PTA + medical therapy vs medical therapy. 2 year follow up • Early management with PTA and medical therapy better than medical therapy alone with regards
to pain free walking distance , pain, and QOL. Greatest difference at 3 months. No difference at 2 years.
Outcome
• Comparing endovascular therapy with medical management (cont) • Hobbs et al, 2006: PTA superior to SET and best medical treatment on basis of ABI,
initial claudication distance, and absolute claudication distance at 6 months
• Perkins et al, 1996. Early improvement with SET, but no difference at long term follow up. PTA increased ABI.
• Spronk, et al, 2009. No difference between endovascular therapy and SET with respect to pain-‐free walking distance at 6 and 12 months, and 7 year follow-‐up. Somewhat faster improvement with PTA.
• Whyman, et al, 1997. Adding PTA to medical therapy (aspirin, smoking cessation, and exercise) did not result in signiAicant difference in walking, onset of claudication, walking distance, or ABI.
• CLEVER trial. Longer peak walking time at 6 months in the SET arm compared with optimal medical therapy (OMT) and stenting. ABI improved in the stenting group. • After 6 months, stent revascularization had better patient reported QOL as compared with SET
and OMT • ABI improved in the stenting group
• ERASE trial. Endovascular therapy + SET resulted in signiAicant greater improvement in pain-‐free and maximum walking disease and health-‐related QOL compared to SET alone
• 2 separate systematic reviews (Frans et al and Ahimastos et al) concluded that endovascular therapy and SET are likely equal • Combination of both is likely better than 1 approach alone
Outcome
• Comparing endovascular therapy with surgery • Van der Zaag et al, 2004: Bypass had higher clinical improvement in Rutherford
classiAication than PTA • Bypass had higher 1 year patency and less incidence of reocclusion
• Wolf et al, 1993. Both had improvement in functional status
• A systematic review (which also included CLI patients) with a total of 5358 patients showed that bypass was associated with longer hospital stay, higher complication rate, and 30-‐day mortality. Bypass had higher patency and durability. 2nd review showed increased 30-‐day morbidity, but no difference in mortality.
• Comparing any revascularization with medical management or exercise • Gelin et al, 2001. Invasive vascularization increases walking capacity and was more
effective than supervised training in alleviating illness speciAic symptoms compared to medical management or exercise
• Nordanstig et al, 2014. Invasive vascularization is associated with improved QOL and higher initial claudication distance, but not maximum walking distance
Outcome
• Cost utilization data. Very limited data due to most RCTs that included cost analysis also included CLI • Spronk et al, 2008. Higher cumulative cost per patient for endovascular therapy
compared to a hospital-‐based exercise program, despite similar outcomes at 12-‐months
• Bermingham et al, 2013. SET more cost effective than unsupervised therapy
• Mazari et al, 2013. SET with PTA is more cost effective than PTA alone
Outcome
Credits
SUMMARY BY: Alexander Lam M.D., R1 PGY2 Department of Radiological Sciences University of California, Irvine Medical Center Malgor RD, Alalahdab F, Elraiyah TA, et al. A systematic review of treatment of intermittent claudication in the lower extremities. Journal of vascular surgery. 2015;61(3 Suppl):54S-‐73S.
Society of Interven7onal Radiology 3975 Fair Ridge Drive | Suite 400 North Fairfax, VA 22033 (703) 460-‐5583
sirweb.org