三軍總醫院外科部實習醫學生臨床教學訓練計畫¤–科... · 三軍總醫院外科部實習醫學生臨床教學訓練計畫 100 年6 月1 日修訂(第11 版) 101
Upload
greta-wraggCategory
view
329download
8
Insulin Glargine in the Management of Hyperglycemia
in Type 2 Diabetes
林志慶 醫師 M.D. Ph.D.
國立陽明大學醫學院內科學系台北榮民總醫院內科部腎臟科

Outline
2

Outline
3

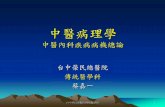
UKPDS: Improving HbA1c Control Reduced Diabetes-Related Complications
44
UKPDS=United Kingdom Prospective Diabetes Study. Data adjusted for age, sex, and ethnic group, expressed for white men aged 50–54 years at diagnosis and with mean duration of diabetes of 10 years. Stratton IM et al. UKPDS 35. BMJ 2000;321:405–412.
EVERY 1%
reduction in HbA1c
REDUCED RISK(P<0.0001)
1%
Diabetes-related deaths
Myocardial infarctions
Microvascular complications
Amputations or deaths from peripheral
vascular disorders
21%
14%
37%
43%
Relative RiskN=3642

2007 AJKD guidelines
55
Target HbA1c for people with diabetes should be < 7.0%, irrespective of the presence or absence of CKD. (A)
Lowering HbA1c levels to approximately 7.0% reduces the development of microalbuminuria. (Strong)

2007 AJKD guidelines
66
Lowering HbA1c levels to approximately 7.0% reduces the development of macroalbuminuria. (Moderate)
Lowering HbA1c levels to approximately 7.0% reduces the rate of decrease in GFR.(Weak)

Outline
7

糖尿病治療選擇 - 藥物治療
8
糖尿病有九大類治療藥物
口服1. 磺醯尿素類 Sulfonylurea(SU)2. Meglitinides3. 雙胍類 Biguanide4. Thiazolidinediones(TZD)5. α-glucosidase inhibitors6. 腸泌素增強劑 (DPP-4 inhibitor)固定劑量複方藥物
注射劑7. 胰島素 insulin8. 胰淀素 pramlintide*9.GLP-1 作用劑 (exenatide)
吸入型胰島素 (inhaled insulin)7.Exubera®** 未在台灣上市

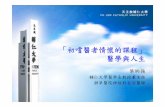
Major Targeted Sites of Oral Drug Classes
9Buse JB et al. In: Williams Textbook of Endocrinology. 10th ed. Philadelphia: WB Saunders; 2003:1427–1483; DeFronzo RA. Ann Intern Med. 1999;131:281–303; Inzucchi SE. JAMA 2002;287:360-372; Porte D et al. Clin Invest Med. 1995;18:247–254.
DPP-4=dipeptidyl peptidase 4; TZDs=thiazolidinediones.
Glucose absorption
Hepatic glucoseoverproduction
Impaired insulinsecretion
Insulinresistance
Pancreas
↓Glucose level
Muscle and fatLiver
Biguanides
TZDs Biguanides
Sulfonylureas
Meglitinides
TZDs
α-Glucosidase inhibitors
Gut
DPP-4 inhibitors
DPP-4 inhibitors
Biguanides
15

Sulfonylureas (SU) 2nd-generation作用機轉:胰島素分泌促進劑 (secretagogues)刺激尚有功能的 β 細胞釋放出胰島素
副作用 低血糖 ( 不論血糖高糖,皆會刺激胰島素分泌,因而增加低血糖發生率 )體重增加、光敏感、噁心、頭疼、皮疹
Drug Dose Daily dose/Frequency (mg)
Amaryl(glimepiride)
2mg 1~4mg qd
Glidiab/Minidiab(glipizide)
5mg 2.5~40mg /day qd or bid
Glurenorm(gliquidone)
30mg 15~120 mg qd
Euglucon/Daonil(glyburide)
5mg 1.25~20 mg /day qd or bid
Diamicron MR(gliclazide)
30mg80mg
30~120/day40~320/day
10

11
NameDuration
(hr)代謝
Glibenclamide(Diabitin®)
12-18原形由肝臟代謝為弱活性,代謝物60%由膽汁排泄, 40%由尿液排
泄
Gliclazide(Diamicron® MR)
12-18 原型由肝代謝為無活性,然後 60-80%由腎排出, 20%由糞便排出
Glipizide(Minidiab®)
12-18 原型由肝代謝為無活性,然後由腎排出
Glimepiride(Amaryl®)
24 原形由肝代謝成弱活性, 2/3由尿液排出, 1/3從糞便
Sulfonylureas (SU)

2007 AJKD guideline
12

Meglitinides 作用機轉 : 胰島素分泌促進劑 ; 隨餐血糖調節劑
與 SU 相近的方式刺激 insulin 分泌快速吸收與作用迅速而短暫 (faster onset and shorter duration vs. SU) ,必需在進食前服藥血糖量愈低,釋出的胰島素量愈少降低餐後血糖濃度
副作用低血糖 ( 但比 SU 比例少,因其為短效藥物 ) 、體重增加
製劑Drug Dose(mg) Daily dose/Frequency (mg)
Starlix(nateglinide)
120 120 3 times/day before meal
Novonorm(repaglinide)
1mg 0.5~4 administrated with meal 2,3,4 times/day
13

14
NameDuration
(hr)代謝
Nateglinide(Starlix®)
2-6 肝代謝, 16%原型由腎排出
Repaglinide(NovoNorm®)
2-6 完全肝代謝,膽汁排出
Meglitinides
CKD stage 3 and 4 CKD stage 5/ Dialysis

Brand name Novonorm (1mg) Starlix (120mg) Glufast (10mg)Product name Repaglinide Nateglinide MitiglinideDose 0.5-4 mg tid 60-120 mg tid 2.5-10 mg tid Administration time
Before meal, 15-30 min
Before meal,1-30 min
Before meal,5 min ; with meal
Tmax 0.5-1 hr 0.25-1 hr 17 minsT 1/2 1-1.8 hr 1.25-2.9 hr 72 minsMetabolite enzyme
CYP3A4 (major) 、 2C8 CYP 2C9 (70%) 、 3A4(30%)
CYP 2C9 < 25%UGT 1A 3 or 9 (74%)
Drug interaction Gemfibrozil, macrolide, cyclosporin, -conazole, CCB, ator- & sim-vastatin
Warfarin, phenytoin, Rosu- and flu-vastatin
No significant interaction
Metabolites in urine
8-10 % 80-83 % 93 % (inactive)
Safety - hypoglycemia - GI intolerance
16-31 %2-5 %
5.5 %3.2 %
5.6 %1.4 %
Efficacy - HbA1C
(0.25-4 mg tid, 12 wks); -1.7 %
(120 mg tid, 24 weeks); - 0.7 %
(5~10 mg tid, 52 weeks); - 1.5 %
BNHI price 4.98 6.5 4.87Daily cost 14.94 ~ 59.76 19.5 14.61 15

Biguanide Metformin 作用機轉
(1) 降低肝臟中的葡萄糖合成作用 (gluconeogenesis)(2) 降低或延遲腸道的葡萄糖吸收,減少飯後血糖上升(3) 增加週邊組織的胰島素敏感性
副作用常見初期腸胃不適 ( 噁心嘔吐、食慾不振 )腎功能不全者罕見的乳酸中毒報告
上市產品
Drug Dose(mg)
Daily dose and Frequency (mg)
Glucophage(metformin)
500 1000~2550mg/day bid or tid
16

Biguanide
17
NameDuration
(hr)代謝
Glucophage(metformin)
6-12 幾乎所有原型由腎排出

Thiazoldinediones (TZDs) 又稱為 PPAR-γ 作用劑 作用機轉 :
與脂肪、肌肉、肝臟細胞核的 PPAR-γ receptor 結合,來增加肝臟、脂肪、肌肉細胞的胰島素敏感性
副作用 : 與劑量相關的體重增加輕度至中度的水腫及水份滯留
特別注意 : 會引發體液滯留,不能用在第 III 及 IV 心衰竭病人應定期檢測肝功能 (ALT 上昇至 >2.5 倍 UNL)不可用於肝功能受損病人
上市產品 :
Drug Dose(mg) Daily dose /Frequency (mg)
Avandia (rosiglitazone) 4 or 8 4~8mg/day qd or bid
Actos (Pioglitazone) 30 15~45mg qd18
Thiazolidinediones (TZDs)

19
NameDuration 代謝
Avandia (rosiglitazone) Weeks
完全肝代謝成無活性產物,腎臟排出
Actos (Pioglitazone) Weeks
完全肝代謝成無或弱活性產物,腎臟排出
Thiazolidinediones (TZDs)

α-Glucosidase Inhibitor作用機轉抑制腸內 α-glucosidase的作用 ( 分解碳水化合物的一群酵素 ) ,使碳水化合物在腸道被分解為單糖和吸收延遲 ;可降低糖尿病患者飯後的血糖濃度
副作用腸胃副作用 ( 腹痛、腹瀉、脹氣 )
上市產品
Drug Dose(mg)
Daily dose and Frequency (mg)
Glucobay(acarbose)
50 50~100 mg tid
20

α-Glucosidase 抑制劑 : acarbose
21
NameDuration
(hrs)代謝
Acarbose 2-6 不被吸收
Miglitol 2-6 不被吸收
Information about the long-term use of acarbose in patients with reduced kidney function is sparse and its use in patients with later stage 3 and stages 4 and 5 CKDis not recommended.

Definition of Incretins
“Intestine-derived factors that increase
glucose-stimulated secretion of insulin ”
In ● cre
● tin
Intestine Secretion Insulin
Creutzfeldt. Diabetologia. 1985;28:565.22

Incretin Hormones Regulate Insulin and Glucagon Levels
GLP-1 = glucagon-like peptide-1; GIP = glucose insulinotropic polypeptide Adapted from Kieffer T. Endocrine Reviews. 1999;20:876–913. Drucker DJ. Diabetes CarAdapted with permission from Creutzfeldt W. Diabetologia. 1979;16:75–85. e. 2003;26:2929–2940. Nauck MA et al. Diabetologia. 1993;36:741–744.
PancreasGut
Nutrient signals
● Glucose
Hormonal signals• GLP-1• GIP
Glucagon(GLP-1)
Insulin (GLP-1,GIP)
Neural signals cells
cells
23

Time, min
IR I
nsu
lin
, mU
/L nm
ol/L
0.6
0.5
0.4
0.3
0.2
0.1
0
80
60
40
20
0
18060 1200
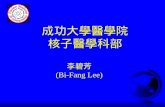
The Incretin Effect Is Diminished in Individuals With Type 2 Diabetes
Control Subjects (n=8)
Patients With Type 2 Diabetes (n=14)
Time, min
IR I
nsu
lin
, mU
/L nm
ol/L
0.6
0.5
0.4
0.3
0.2
0.1
0
80
60
40
20
0
18060 120 0
Oral glucose load Intravenous (IV) glucose infusion
Normal Incretin Effect Diminished Incretin Effect
IR = immunoreactiveAdapted with permission from Nauck M et al. Diabetologia 1986;29:46–52. Copyright © 1986 Springer-Verlag. Vilsbøll T, Holst JJ. Diabetologia 2004;47:357–366. 24

DPP-4 Inhibition作用機轉
上市產品
25
Drug Dose(mg)
Daily dose and Frequency (mg)
JANUVIA (sitagliptin) 100 100mg QD
ONGLYZA (saxagliptin)
2.5-5mg 2.5-5mg QD
釋出活性 IncretinGLP-1 與 GIP
進食
腸胃道
DPP-4 酵素
無活性GLP-1
XSitagliptin( DPP-4 抑制劑)
胰臟
無活性GIP
β細胞α細胞

DPP-4 Inhibition
26
NameDuration
(hrs)代謝
JANUVIA(Sitagliptin)
12-24hrs70-80%腎臟排出,無法被透析排
出ONGLYZA(Saxagliptin)
24hrs全由肝臟代謝成無或弱活性產物,後從腎臟排出,可以被透析洗出
Onglyza:Moderate or severe CKD, or ESRD under hemodialysis: 2.5mg QD(post-H/D)PD: no data
1#QD 0.5# QD 0.25# QD

GLP-1 Analogues
作用機轉產生類似 GLP-1的作用
副作用對照性臨床研究中,不論單一或合併療法,表現出良好耐受性,出現臨床不良反應而停藥者與安慰劑相當
上市產品
Drug Dose(mg)
Daily dose and Frequency (mg)
BYETTA (exenatide) 5-10mcg BID
27

GLP-1 Analogues
28
BYETTA is not recommended for use in patients with end-stage renal disease or severe renal impairment (creatinine clearance < 30 mL/min) caution in patients with renal transplantation.Moderate renal impairment (30-50 mL/min): caution should be applied when initiating or increasing doses of Byetta from 5 mcg to 10 mcg REFERENCE: U.S. Food and Drug Administration
?

Renal Side Effects of Exenatide
11/02/2009 FDA:From April 2005 through October 2008,
FDA received 78 cases of altered kidney function (62 cases of acute renal failure and 16 cases of renal insufficiency), in patients using Byetta. (total number: 6.6 million)
29

Outline
30

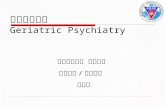
Insulin Action: Comparison of New Insulin Analogs
0
20
40
60
80
100
120
140
0 2 4 6 8 10 12 14 16
RegularRegular
Rapid (Lispro, Aspart)Rapid (Lispro, Aspart)
Insu
lin L
evel
(In
sulin
Lev
el (
U/m
l)U
/ml)
HoursHours
Intermediate (NPH)Intermediate (NPH)
Long Long
31

Preparations Onset(h) Peak(h) Duration(h)
Lispro/Aspart < 0.25 1 - 2 3 - 4
Regular 0.5 - 1 2 - 4 6 - 8
NPH 1 - 3 5 - 7 13 - 16
Ultralente 2 - 4 8 - 14 < 20
Glargine 1 - 2 > 24
Action Profiles
Modified after Leahy JL. In: Leahy JL, Cefalu WT, eds. Insulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002.

Insulin therapy in renal disease
33

Insulin therapy in renal disease
34
BiesenbachG, Raml A, Schmekal B, Eichbauer-SturmG:Decreased insulin requirement in relation to GFR in nephropathic Type 1 and insulin-treated Type 2 diabetic patients. DiabetMed 20:642–645, 2003

Insulin therapy in renal diseaseThe American College of Physicians recommended:
35
GFR (mL/min) Insulin
50-10 mL/min 25% decrease
<10 mL/min 50% decrease
Haemodialysis require less exogenousinsulin ( peripheral insulin resistance ↓)

Insulin therapy in renal disease
OBJECTIVE— Type 2 diabetic patients with end-stage renal disease (ESRD) on maintenance hemodialysis.
CONCLUSIONS— The present study has demonstrated a significant
25% reduction in basal insulin requirements No significant change in boluses Overall the reduction of total insulin requirements was
15%
36

Insulin therapy in renal disease
↓GFR: RI (rapid-acting insulin analogs): ↑ half-life and maximal serum concentrations NPH (Caution!): long-acting ‘‘basal’’ insulin like glargine Insulin detemir : binding to serum albumin after injection so less predictable in patients with nephrotic syndrome and hypoalbuminema
37

The ADA Treatment The ADA Treatment Algorithm for the Initiation and Algorithm for the Initiation and
Adjustment of InsulinAdjustment of Insulin

ADA-EASD Guidelines
Achievement of normal glycemic goals Initial therapy with lifestyle intervention and
metformin Early addition of insulin therapy in patients who
do not meet target goals Rapid addition of and transition to new regimens,
when glycemic goals are not achieved

Management of Type 2 Diabetes ADA-EASD
Check HbA1c every 3 months until < 7% and then at least every 6 months
Insulin regimens under lifestyle and diet control
Initiation and intensification of insulin due to effectiveness and low expense although 3 oral agents can be used

New ADA/EASD algorithm for T2DM: Basal insulin is recommended for insulin initiation
Nathan et al. Diabetes Care 2008.
At diagnosis:Lifestyle + Metformin
Lifestyle + Metformin
+ Basal insulin
Lifestyle + Metformin
+ Sulfonylureas
Lifestyle + Metformin
+ Intensive insulin
Tier 1: well-validated therapies
STEP 1 STEP 2 STEP 3
Tier 2: Less well validated therapies
Lifestyle + Metformin+ Pioglitazone
No hypoglycaemiaOedema/CHF
Bone loss
Lifestyle + metformin+ GLP-1 agonistNo hypoglycaemia
Weight lossNausea/vomiting
Lifestyle + metformin+ Pioglitazone+ Sulfonylurea
Lifestyle + metformin+ Basal insulin
Nathan DM, et al. Diabetologia 2009;52:17−30

- Insulin is the most effective drug in lowering BG
- Insulin should be started with basal insulin
- Basal Insulin is proposed as early as after Metformin
- Then consider stepwise addition of bolus insulin starting with one shot at selected meal
- Premixes are not recommended as first line insulin therapy
ADA-EASD Consensus Key messages on insulin

The basal–bolus insulin regimen
Insu
lin (
mU
/L)
06:00 12:00 24:0018:000
15
30
45
06:00
Breakfast Lunch Dinner Physiological insulin
Basal insulinPrandial insulin
Time
Figure adapted from Kruszynska YT, et al. Diabetologia 1987;30:16–21
Normal Insulin Secretion: The Basal-Bolus Insulin Concept

Comparison of 24-hour glucose levels in control subjects vs patients with diabetes (p<0.001).Adapted from Hirsch I, et al. Clin Diabetes 2005;23:78–86.
Time of day (hours)
400
300
200
100
006.00 06.0010.00 14.00 18.00 22.00 02.00
Pla
sm
a g
lucose (
mg
/dl)
NormalMeal Meal Meal
20
15
10
5
0
Pla
sm
a g
lucose
(mm
ol/l)
Treating Fasting Hyperglycemia Lowers the Entire 24-hour Plasma Glucose Profile
Hyperglycaemia due to an increase in fasting glucose
T2DM

Comparison of 24-hour glucose levels in control subjects vs patients with diabetes (p<0.001).Adapted from Hirsch I, et al. Clin Diabetes 2005;23:78–86.
Time of day (hours)
400
300
200
100
006.00 06.0010.00 14.00 18.00 22.00 02.00
Pla
sm
a g
lucose (
mg
/dl)
NormalMeal Meal Meal
20
15
10
5
0
Pla
sm
a g
lucose
(mm
ol/l)
Hyperglycaemia due to an increase in fasting glucose
T2DM
Long-acting basal insulin
Treating Fasting Hyperglycemia Lowers the Entire 24-hour Plasma Glucose Profile

ADA/EASD Consensus Algorithm for Type 2 Diabetes Mellitus
Nathan D, et al. Diabetologia 2006;49:1711−21.
Initiation of Basal Insulin:
•Start with bedtime intermediate-acting insulin, or bedtime or morning long-acting insulin
•Can initiate with 10 units or 0.2 units per kg
•↑ 2 units every 3 days, if 180> FBS >130 mg/dl
•↑ 4 units every 3 days if FBS >180 mg/dl
• If hypoglycaemia or FBS <70 mg/dl, ↓ bedtime
dose by 4 units, or 10% if dose >60 units

Insulin Therapy for Type 2 Diabetes: Rescue,
Augmentation, and Replacement of Beta-Cell Function

-C
ell
fun
cti
on
(%
)
PostprandialHyper-
glycemiaIGT
Type 2DiabetesPhase I
Type 2DiabetesPhase II
25
100
75
0
50
–12 –10 –6 –2 0 2 6 10 14
Years from diagnosis
Adapted from Lebovitz H. Diabetes Rev 1999;7:139-153.
Destiny of Type 2 Diabetes Pancreatic -Cell Decline Over Time in UKPDS
Type 2DiabetesPhase III
Insulin therapyRescue
Replacement
Augmentation

Rescue therapy Using replacement regimens for several weeks May reverse glucose toxicity
Augmentation therapy With basal insulin If some β- cell function remains Starting dose: 0.15-0.2u/kg/d or units of insulin/d = FBS (mmol) = FBS/18 (mg/dl) e.g. FPG 180mg/dl 10 units FPG 270mg/dl 15 units

Early Aggressive Insulin Therapy Study in Taiwan
60 newly diagnosed type 2 diabetic patients hospitalized patients with severe hyperglycemia were hospitalized and treated with intensive insulin injections for 10-14 days.
50 patients randomized to insulin therapy and oral antidiabetic drugs after discharge for 6 months and a follow-up for further 6 months
HbA1c and Beta-cell function were measured.
Chen HS, et al. Diabetes Care 2008; 31: 1927-1932.

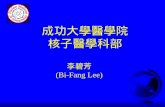
Effect of Insulin vs. OADs on HbA1c in Newly Diagnosed T2DM
Hb
A1c (
%)
8
6
4
2
0
P=0.002
10
Before therapy 6 months 12 months
Insulin group
Oral antidiabetic drug group
12
14P=0.009
6.33 7.50 6.78 7.84
11.89 11.33
Chen HS, et al. Diabetes Care 2008; 31: 1927-1932.

Significantly Improved β-cell Function with Basal Insulin Assessed by OGTT
Chen HS, et al. Diabetes Care 2008; 31: 1927-1932.
140
120
100
80
60
40
20
00 30 60 90 120
##
#
#
###
#
***
*
Time (minutes)
Pla
sma
insu
lin (U
/mL)
OAD group, after 6-month treatmentOAD group, at baselineInsulin group, after 6-month treatmentInsulin group, at baseline
*P<0.05 between groups#P<0.05 baseline vs. after treatment
Insulin group
OAD group

Replacement therapy
With basal - bolus insulin (MDI) Required for β- cell exhaustion
Starting dose : 0.5u/kg/dBasal 50-60% TDD Bolus 40-50% TDD
(% of estimated calories for each meal)
Fasting Preprandial Postprandial
Adjustment

When to Consider Prandial Insulin A1C Versus FPG
Target
Increase Increase BasalBasal
StartPrandialPrandial
240
210
180
150
120
76 8 9 10
A1C (%)
Fas
tin
g p
lasm
a g
luco
se (
mg
/dL
)
BiphasicBasal plusBasal/bolus

Early Insulin Replacement in Type 2 DM May Preserve Beta-cell Function
Glucose uptake
Insulin resistance Lipolysis
Glucose output
Early insulin replacement
Reduced strain ?
Reduced toxicity ?
-> Sustained insulin secretion
? +
After Gerstein & Rosenstock
“ Beta-cell rest ”

Lantus(Insulin Glargine)

Insulin Glargine Structure
Asparagine at position A21 replaced by glycine– Provides stability
Addition of 2 arginines at the C-terminus of the B chain– Soluble at slightly acidic pH
Lantus® (insulin glargine) EMEA Summary of Product Characteristics. 2002.McKeage K et al. Drugs. 2001;61:1599-1624.
SubstitutionSubstitution
ExtensionExtension
A chainA chain
B chainB chain
11
1515101055
1010 1515
2020 AsnAsn
3030
GlyGly
ArgArg ArgArg
55 1010 1515 1919 2525
11

Insulin Glargine vs NPHclear solution vs suspension
NPH Glargine NPH NPH

Mechanism of ActionInjection of an acidic Injection of an acidic
solution (pH 4.0) solution (pH 4.0)
MicroprecipitationMicroprecipitation of of insulin glargine in sub-insulin glargine in sub-
cutaneous tissue (pH 7.4) cutaneous tissue (pH 7.4)
Slow dissolution of Slow dissolution of freefree insulin glargine insulin glargine hexamershexamers
from microprecipitates from microprecipitates (stabilised aggregates) (stabilised aggregates)
Protracted action Protracted action Kramer W. Exp Clin Endocrinol Diabetes. 1999;107(suppl 2):S52-S61.

Time-Action Profile of Lantus vs. NPH
12
10
8
0
16
8
24
mol
/Kg/
min
Time (hours)
sc injection
Glucose Infusion Rate
0 168 24
Time (hours)
0 168 24
mm
ol/l
Plasma Glucose
sc injection
NPHNPHNPH
glargineglargineglargine
Lepore et al. Diabetes 2000; 49: 2142-2148
Plasma glucose

LEAD STUDYLEAD STUDY LLantus antus EEvaluationvaluation in in AAsian type 2 sian type 2 DDiabeticsiabetics
Inclusion criteria:Inclusion criteria:
• Asian men and women with type 2 DM, insulin-naive
• Aged > 40 and 80 years
• Treatment with OADs for at least 3 months
–Any sulfonylurea, as monotherapy or in combination with metformin or acarbose
–Previous sulfonylurea dose glimepiride 3 mg
• HbA1c between 7.5% and 10.5%
• FBG >120 mg/dL (6.7 mmol/L)
• BMI 20-35 kg/m2
Pan C-Y et al. Diabetes Res Clin Pract 2007; 76:111-118

LEAD: Treatment regimenLEAD: Treatment regimen
Subjects (n=448) were randomized to receive
Bedtime insulin glargine+breakfast glimepiride (3mg)
Bedtime NPH insulin + breakfast glimepiride (3 mg)
Screening phase
Week –4 to week –1
Week 0 (baseline)
Week 24 (endpoint)
Treatment phase
Insulin starting dose: 0.15 U/kg/dayDose titration target: FBG < 120 mg/dL (6.7 mmol/L )
Pan C-Y et al. Diabetes Res Clin Pract 2007; 76:111-118

LEAD - Primary variable : change in HbA1cLEAD - Primary variable : change in HbA1c
- 0.99
- 0.77
p=0.0319
Insulin glargine(n=220)
NPH insulin(n=223)
Red
uct
ion
in
mea
n H
bA
1c (
%)
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
Pan C-Y et al. Diabetes Res Clin Pract 2007; 76:111-118

LEAD: change in mean dailyLEAD: change in mean daily blood glucose (FAS)blood glucose (FAS)
Baseline
Endpoint
Insulin glargine(214)
NPH insulin(219)
Mea
n d
aily
blo
od
glu
cose
(m
g/d
L)
276 269
p=0.0018
182 189
- 94 - 80
0
50
100
150
200
250
300
Pan C-Y et al. Diabetes Res Clin Pract 2007; 76:111-118

LEAD: Mean Basal Insulin DoseLEAD: Mean Basal Insulin Dose
Mean initial dose of basal insulin*
(IU/day)
Mean basal insulin dose at
endpoint (IU/day)
Insulin glargine 9.6 32.1
NPH insulin 9.8 32.8
* Start dose recommended by protocol: 0.15 U/kg/day
No difference between PP and FAS population
Pan C-Y et al. Diabetes Res Clin Pract 2007; 76:111-118

LEAD: Hypoglycemic EventsLEAD: Hypoglycemic Events
All Symptomatic Severe Nocturnal
p<0.004
p<0.0003
p<0.001
p<0.03
Insulin glargine NPH insulin
Nu
mb
er o
f h
ypo
gly
cem
ic e
pis
od
es
0
200
400
600
800
1000
1200
Pan C-Y et al. Diabetes Res Clin Pract 2007; 76:111-118

LACE: prospective, randomized real-life study of glargine + glulisine vs premixes
n = 197
Randomization
Initial assessment Follow-up assessments
3 month 6 month 9 month
GLAR + GLU ± orals or ± other (as naturally occurring)
Premix ± orals or ± other (as naturally occurring)
• Age 18 years• HbA1c 7%• Type 2 diabetes• BMI ≥ 26• Excluded if already taking exenatide or pramlintide
Note: Inclusion – All patients eligible for BOTH insulin regimens Debit cards for all participants to cover additional, initial GLU copay so patients will have equal financial access to both treatment arms
Lee et al. Poster presentation PS 085. Abstract 1003. EASD 2008Wednesday 12.30, Poster session

LACE: glargine + glulisine vs premixes improved glycemic control with similar safety
Insulin pre-treated patients with T2DM (n=197)
Glargine + glulisine (n=106)
Premixes (n=91)
p
Baseline HbA1c (%) 9.25 9.25 –
Final adjusted HbA1c (%) 6.93 7.52 0.009Change in HbA1c (%) –2.27 –1.68 –
Patients with hypoglycemia (last month)
36% 43% NS
Total insulin dose/day (U) 74 85 0.267
Cost per day (all meds) 10.82 (USD) 12.06 (USD) 0.209
Total cost (6 months) 1933.20 (USD) 2158.74 (USD)
Cost difference –225 (USD) Lee et al. Poster presentation PS 085. Abstract 1003. EASD 2008

Before Lantus (2008/10/9)
After Lantus (2009/11/26)
FBS (mg/dl) / HbA1c (%)
237 / 13.2 103 / 5.9
BUN/Creatinine (mg/dl) 38 / 2.42 29 / 2.45eGFR (ml/min/1.73m2) 27.7 27Urine Protein/Cr ratio 1.3 1.49Cholesterol/TG (mg/dl) 148/323 125/111HDL/LDL (mg/dl) 26/76 28/80Na/K (mEq/L) 139/3.9 137/4P (mg/dl) 3.0 3.6Albumin (g/dl) 3.5 4
• Mr. King, 81 y/o male, diabetic nephropathy since 2008/10• 2008/10/14, initiating Lantus 24 units qd FBS 130~160 mg/dl• 2008/12/3, adding Novonorm 1.5# tid FBS 100~120 mg/dl• 2009/11/27, maintaining Lantus 26 units qd + Novonorm 1.5# tid
Case of DMN: Insulin as Initial therapy

The Basal / Basal Plus strategy for T2DM
Lifestyle changes
OHA monotherapy and combinations
BasalAdd basal insulin and titrate
Basal PlusAdd prandial insulin at main meal
Basal bolusBasal + three prandial
FBG at target
HbA1c above target
OHA=oral hypoglycemic agent Adapted from Raccah et al. Diabetes Metab Res Rev 2007;23:257−64
Progressive deterioration of ß-cell function
HbA1c above target
FBG above targetHbA1c above target
FBG at targetHbA1c above target
Stepwise intensification of treatment for continuity of control

Expected HbA1c Reduction in CKD
Interventions Expected decrease in HbA1c
Lifestyle 1 – 2 %
Insulin 1.5 – 3.5 %
Sulfonylureas (glurenorm) 1 – 2 %
Glinides 1 – 1.5 %
Sitagliptin 0.5 – 0.8 %
-glucosidase inhibitors 0.5 – 0.8 %
Pioglitazones 0.5 – 1.4 %
Nathan DM, et al. Diabetologia 2009;52:17−30

Summary: Treatment of DM in CKD
Novel diabetic medications are available in past few years.
Some require adjustment of dose or should be even avoided according to the patient’s renal function.
Metformin, 1st line Tx in patients with normal renal function, is contraindicated in CKD with Cr>1.5 (M) or 1.4 (F) mg/dL.
CKD stage 3/4: SU (glipizide, gliclazide, glimepiride), Glinides, TZD, DPP4i, α-glucosidase inhibitor, insulin
CKD stage 5 or ESRD: SU (glipizide, gliclazide), Glinide (repaglinide, mitiglinide), TZD, DPP4i, insulin
Judicious titration of medications and frequent monitoring of blood glucose to avoid severe adverse effects!

Summary for Basal Insulin Therapy
Tight glycemic control reduces risk of complications.
Earlier initiation of insulin helps achieve target of glycemic control.
Lantus, long-acting insulin analog, as a basal insulin therapy with:
– Once daily, peakless, 24 hours basal insulin– Consistent efficacy in glycemic control– Less hypoglycemia than NPH insulin and premixed
human insulin– Less adverse reactions than TZD add-on to OADs– Easy titration according to FPG to achieve target

Paradigm Link™
Paradigm 512™) ) ) ) ) ) ) ) ) )
) ) )
Wireless Diabetes Managing System: Insulin Pump (Paradigm 512) and
Blood Glucose Monitor (Paradigm Link)74

Thank You for Your Attention!

Expected HbA1c Reduction
Interventions Expected decrease in HbA1c
Lifestyle 1 – 2 %
Insulin 1.5 – 3.5 %
Metformin 1 – 2 %
Sulfonylureas 1 – 2 %
Pioglitazones 0.5 – 1.4 %
-glucosidase inhibitors 0.5 – 0.8 %
Exenatide 0.5 – 1 %
Glinides 1 – 1.5 %
Pramlintide 0.5 – 1 %
Sitagliptin 0.5 – 0.8 %Nathan DM, et al. Diabetologia 2009;52:17−30

Late Stage T2DMIGT
Insulin resistance
T2D DiagnosisNGT
Beta-cell dysfunction
100%
100%
Relative Contributions of Diabetic Pathophysiologies Over Time
Those who develop DM have lost ~50% of beta-
cell function
Beta-cell dysfunction determines the onset of
hyperglycemia, glucose levels and disease progression, not
insulin resistance
Both beta-cell dysfunction + insulin resistance start years
before diagnosis
Hepatic glucose over-production
NGT = normal glucose tolerance, IGT = impaired glucose tolerance, T2D = type 2 diabetesBell D. Treat Endocrinol 2006; 5:131-137; Butler AE et al. Diabetes 2003;52:102-110; Del Prato S and Marchetti P. Diabetes Tech Therp 2004;6:719-731Gastaldelli A, et al Diabetologia 2004:47:31-39; Mitrakou A, et al. N Engl J Med 1992; 326:22-29; Halter JB, et al. Am J Med 1985;79S2B:6-12

HOMA= Homeostasis model assessment.UKPDS Group. Diabetes 1995;44:1249―58. Adapted from Holman RR. Diabetes Res Clin Pract 1998;40(suppl 1):S21―5.
Decline of -cell function determines the progressive nature of T2DM (UKPDS)
-
cel
l fu
nc
tio
n
% o
f N
orm
al b
y H
OM
A
Time (years)
0
20
40
60
80
100
―10 ―8 ―6 ―4 ―2 0 2 4 6
Time of diagnosis?
Pancreatic function= 50% of normal
- 5% per yr

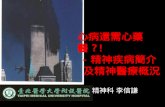
健健
康康
生生
活活
型型
態態
之之
飲飲
食食
及及
運運
動動
醣化血色素 < 9.0 % 之患者 醣化血色素 ≧ 9.0 % 之患者
使用一種或二種口服抗糖尿病藥物• 促胰島素分泌劑• 雙胍類藥物• 胰島素增敏劑• 阿爾發葡萄醣苷酶抑制劑• 二肽基肽酶 -4 抑製劑
使用二種或多種口服抗糖尿病藥物• 促胰島素分泌劑• 雙胍類藥物• 胰島素增敏劑• 阿爾發葡萄醣苷酶抑制劑• 二肽基肽酶 -4 抑製劑
使用基礎 ( 及 / 或 ) 餐前胰島素
未達到控制目標時
增加不同種類的口服抗糖尿病藥物 或單獨使用胰島素 ( 或合併使用 )• 促胰島素分泌劑• 雙胍類藥物• 胰島素增敏劑• 阿爾發葡萄醣苷酶抑制劑• 二肽基肽酶 -4 抑製劑
增加不同種類的口服抗糖尿病藥物 或使用胰島素
增加不同種類的口服抗糖尿病藥物 或單獨使用胰島素 ( 或合併使用 )• 雙胍類藥物• 胰島素增敏劑• 阿爾發葡萄醣苷酶抑制劑• 二肽基肽酶 -4 抑製劑
註 1: 適時調整口服糖尿病藥物和胰島素,希望使糖化血色素在 3-12 個月內達到治療的目標,若未達到治療目標,宜轉診至專科醫師。註 2: 選擇降血糖藥物需依照病人個別情況而定,避免藥物所引起的低血糖。註 3: 同時使用胰島素及胰島素增敏劑可能增加水腫的機會,並應同步注意病患的心臟功能變化。
使用基礎 ( 及 / 或 ) 餐前胰島素
增加不同種類的口服抗糖尿病藥物 或單獨使用胰島素• 雙胍類藥物• 胰島素增敏劑• 阿爾發葡萄醣苷酶抑制劑• 二肽基肽酶 -4 抑製劑
未達到控制目標時 未達到控制目標時 未達到控制目標時
2010 中華民國糖尿病學會臨床指引79