ID Board Review May 1, 2009. If it’s in ORANGE, it’s in PREP.
35
ID Board Review May 1, 2009
-
Upload
dora-sparks -
Category
Documents
-
view
239 -
download
0
Transcript of ID Board Review May 1, 2009. If it’s in ORANGE, it’s in PREP.
ID Board Review
May 1, 2009
If it’s in ORANGE, it’s in PREP
2 day old infant presents with respiratory distress and fever of 101.
Which bugs should we be concerned about in the newborn period? E. coli GBS Listeria Coag. negative Staph (Staph epidermis)
What is the typical antibiotic therapy? Ampicillin + Gentamicin
Listeria Gram positive rod -- Listeria monocytogenes Common cause of neonatal sepsis Mode of transmission
Food borne (unpasteurized milk, soft cheeses, hot dogs, deli meats, undercooked poultry, unwashed raw vegetables)
Transplacental / Ascending (fecal/vaginal carrier) Clinical
Neonatal Early onset—Asymptomatic, Preterm, PNA, Septicemia,
Rash (erythematous granulomatous/papular) Late onset (after 1st wk) – meningitis
Immunocompromised – Meningitis, Parenchymal brain infection
Treatment: Ampicillin +/- Gentamicin
Group B Strep Mode of transmission
Maternal-fetus, contact GI/GU colonization
Clinical Early onset (0 - 6 days)
Sepsis, PNA, Meningitis (<10%) Late onset (7d - 3mos)
Occult bacteremia, meningitis, osteomyelitis, cellulitis Lab Diagnosis
Culture of blood, CSF, other fluid Most rapid method: Antigen detection
Treatment Ampicillin + Gentamicin GBS identified -- PCN G
GBS & Pregnancy When do we screen mothers for GBS?
35-37 WGA What are the risk factors for neonatal infection?
< 37 WGA PROM > 18 hrs Intrapartum fever Chorioamnionitis GBS UTI during pregnancy Previous infant w/invasive GBS disease
Prophylaxis Who, What, When, Where, How?????
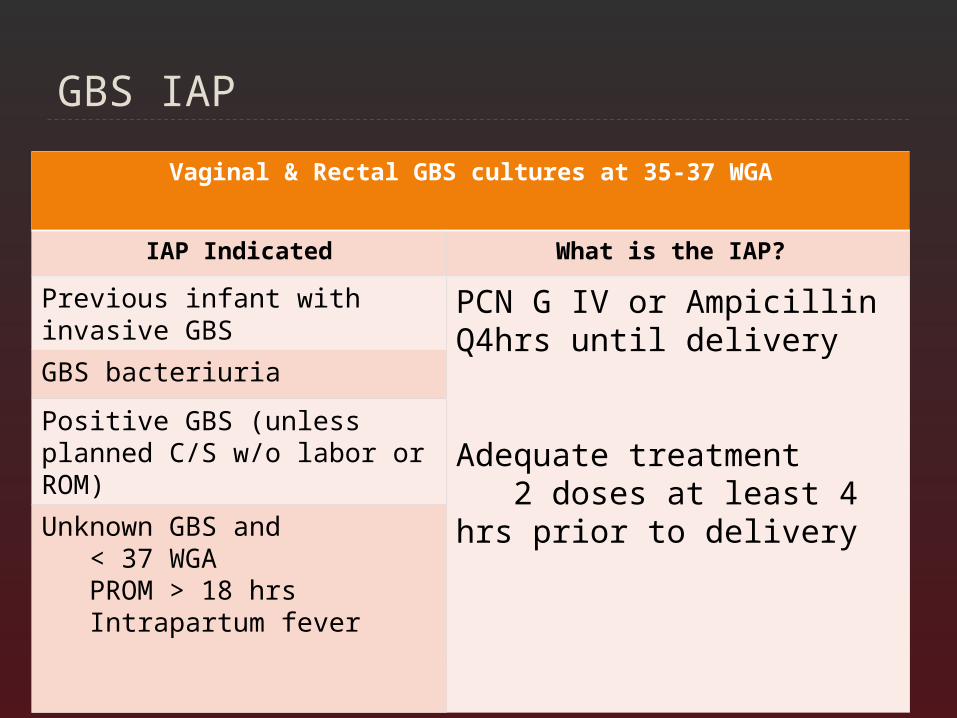
GBS IAP
Vaginal & Rectal GBS cultures at 35-37 WGA
IAP Indicated What is the IAP?
Previous infant with invasive GBS
PCN G IV or Ampicillin Q4hrs until delivery
Adequate treatment 2 doses at least 4 hrs prior to delivery
GBS bacteriuria
Positive GBS (unless planned C/S w/o labor or ROM)
Unknown GBS and < 37 WGA PROM > 18 hrs Intrapartum fever
H. influenzae type B (Hib) Clinical
Before Hib vaccine, most common cause of bacterial meningitis
Since vaccine (1988), invasive disease has decreased by 99% in children < 5 yrs
Infection now occurs in un-/under- immunized or young PNA Sepsis / Occult Bacteremia Meningitis Epiglottitis OM Septic Arthritis Cellulitis Pericarditis
FYI Nontypeable strains cause infxn of respiratory tract Conjunctivitis, OM, sinusitis, PNA
Mode of transmission Inhalation of droplets, contact, neonatal
HIB Lab diagnosis
Culture of fluid (chocolate agar), CSF Latex DO serotyping
Treatment URI/OM/Sinusitis – Amoxil, Augmentin Invasive/Meningitis/Epiglottitis – Rocephin,
Claforan Prophylaxis??
Drug of choice – Rifampin +/- vaccine When / Who?
All household contacts if child < 4 who is un- / incompletely immunized, < 12 mos old child, IC child
Nursery / Daycares if > / = 2 cases within 60 days
7-month-old girl comes to see you because of runny nose and an occasional cough for most of the past week.
Nobody else in the home is sick except for the grandmother………
Mee Maw has had a severe cough for the past 2 weeks. In fact, the coughing fits were so violent that she would pass out.
What should you suspect? What do you want to do about this infant’s cold? Who should receive Ab prophylaxis?
WHOOPING COUGH
Pertussis (aka Whooping Cough) Adults are major reservoir Immunity not lifelong Mode of transmission
Close contact with aerosolized droplets Clinical manifestations
Catarrhal: 1- 2 weeks URI symptoms Paroxysmal: 2 - 6 weeks Cough increases in severity
Paroxysmal attacks Cough + gagging, cyanosis, post-tussive emesis, apnea Followed by whoop (forced inspiratory effort)
Convalescent: wks – mos Cough decreases Most contagious: catarrhal stage and first 2 weeks after
onset of cough Disease in infants
May have only cough w/associated apnea, cyanosis, feeding difficulties, tachypnea
More likely to have complications PNA, apnea, FTT, seizures, death
Whoooooopin’ Cough Lab diagnosis
Direct Fluorescent Antibody (DFA) Low sensitivity
PCR assay Gold standard: Culture
Treatment Does not alter the disease course, but decrease patient
infectivity Azithromycin x 5 d Alternatives: clarithromycin x 7d, erythromycin x 14 d, Bactrim
x 14 d
Prevention Droplet Precautions Antibiotic prophyalxis for close contacts No school/daycare until treated x 5 days
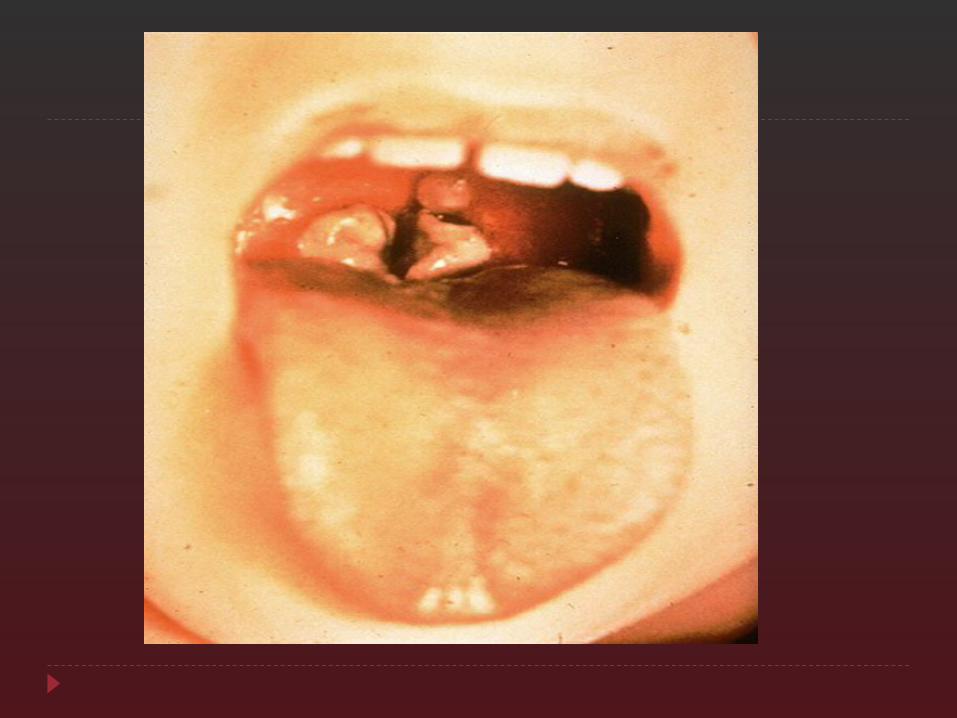
Diphtheria Clinical
Membranous nasopharyngitis or obstructive laryngotracheitis Rare: cutaneous, vaginal, conjunctival, otic infection,
myocarditis, peripheral neuropathies Transmission – respiratory droplets and/or contact Toxin mediated illness
Exotoxin A & B Treatment
Equine antitoxin (1o therapy) Erythromycin or PCNG to
Stop toxin production, eradicate C diptheriae, prevent transmission
Vaccination prevents disease (only effective control measure)
Working in a refugee camp when a mother brings in her 8 day old boy
States irritable x 2 days Now loud noises appear to cause him pain,
evidenced by muscle tightening and back arching causing his head to nearly touch his feet
On exam, you note dried packing on his umbilical cord, which is the local custom
MMMMM, VERY WEIRD……. WHAT DO YOU THINK IS GOING ON?
Tetanus Clostridium tetani Clinical
Gradual onset of trismus , severe muscle spasms Can be localized, cephalic (CN), or generalized Exacerbated by external stimuli (noise)
Toxin mediated illness Neurotoxin in a contaminated wound ** Poor umbilical cord care
Treatment Tetanus Ig, wound management, Metronidazole or PCN
G x 10-14 d Vaccination prevents disease (only effective control
measure)
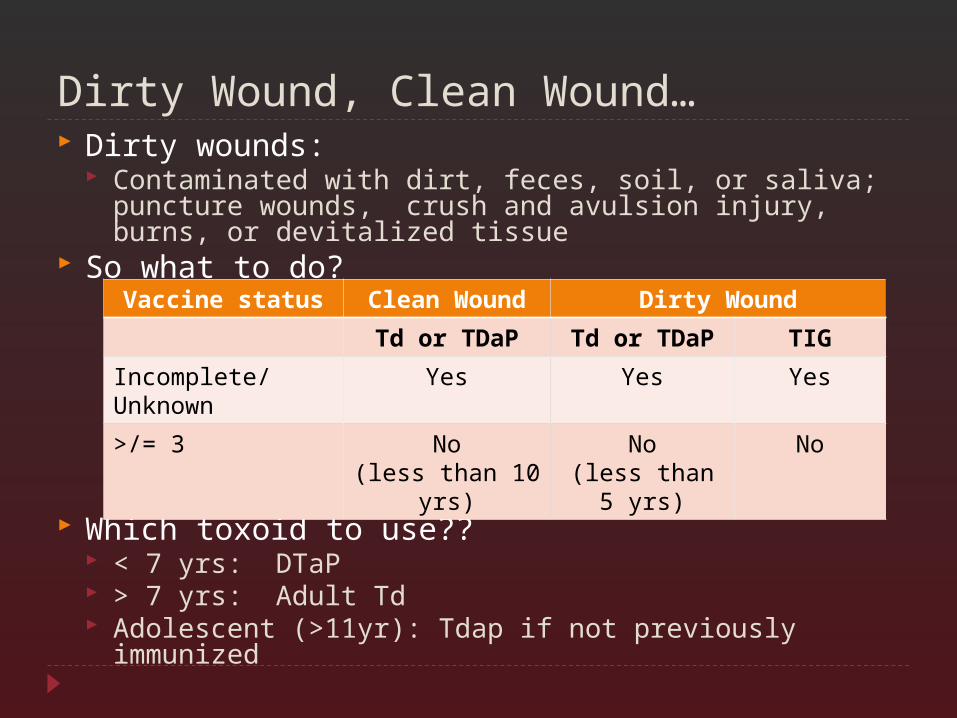
Dirty Wound, Clean Wound… Dirty wounds:
Contaminated with dirt, feces, soil, or saliva; puncture wounds, crush and avulsion injury, burns, or devitalized tissue
So what to do?
Which toxoid to use?? < 7 yrs: DTaP > 7 yrs: Adult Td Adolescent (>11yr): Tdap if not previously immunized
Vaccine status Clean Wound Dirty Wound
Td or TDaP Td or TDaP TIG
Incomplete/ Unknown
Yes Yes Yes
>/= 3
No(less than 10
yrs)
No(less than 5
yrs)
No
4 mos old female presents to clinic with poor feeding and constipation
Any thoughts??? On exam, note hypotonia (greatest in UE)
Ok, so what do we have? Other symptoms that may be present? What is the usual mode of acquistion?
Botulism Botulinum toxin …… Method of action???
Blocks release of acetylcholine into synapse
Characteristics of botulism Acute, afebrile, symmetric, descending flaccid
paralysis 3 Types:
Food borne – ingestion of preformed toxin Wound – systemic spread Infantile -- ingestion of spores intestinal colonization
Suspect in infant < 6 mos w/ constipation, listlessness, loss of facial expression, poor feeding, weak cry, decreased gag reflex, hypotonia (“floppy”), ptosis
Floppy baby eating honey….. Lab diagnosis of infantile botulism
C. botulinum in stool Treatment
Primarily supportive care Antitoxin NO Antibiotics – lysis of spores / release of more
toxin NOT GOOD
NO HONEY <12 MOS!!!!! AND NO….. BULGING CANS
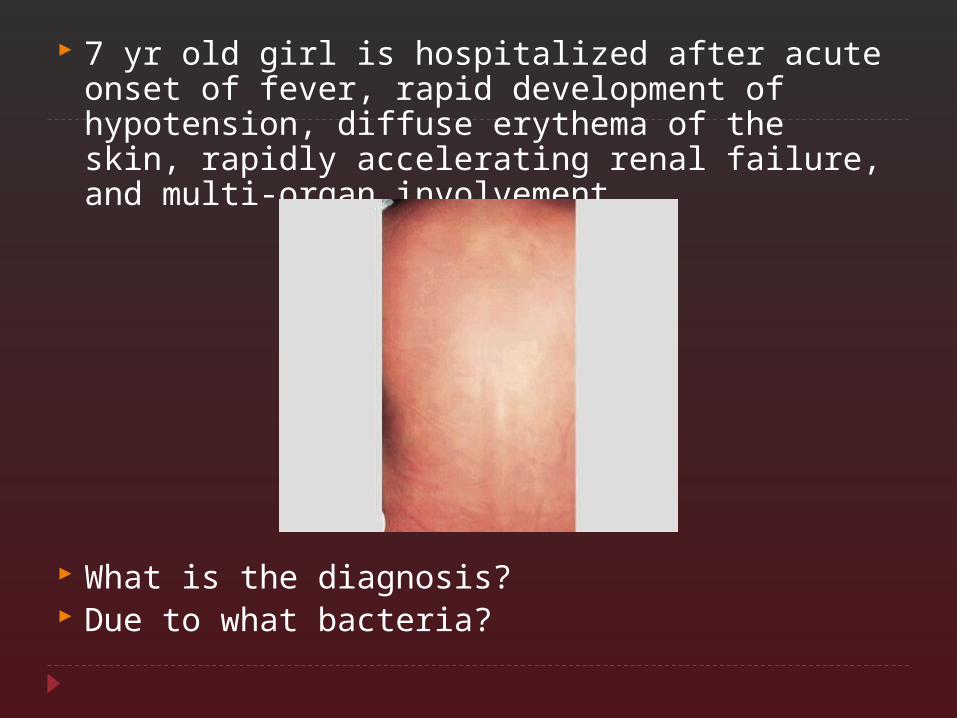
7 yr old girl is hospitalized after acute onset of fever, rapid development of hypotension, diffuse erythema of the skin, rapidly accelerating renal failure, and multi-organ involvement
What is the diagnosis? Due to what bacteria?
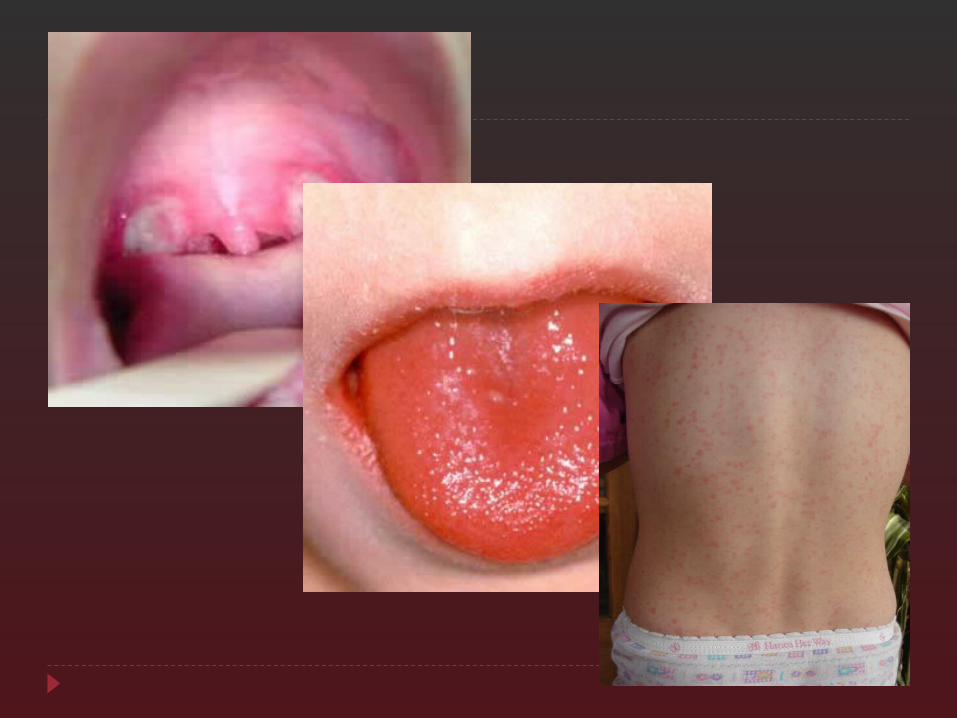
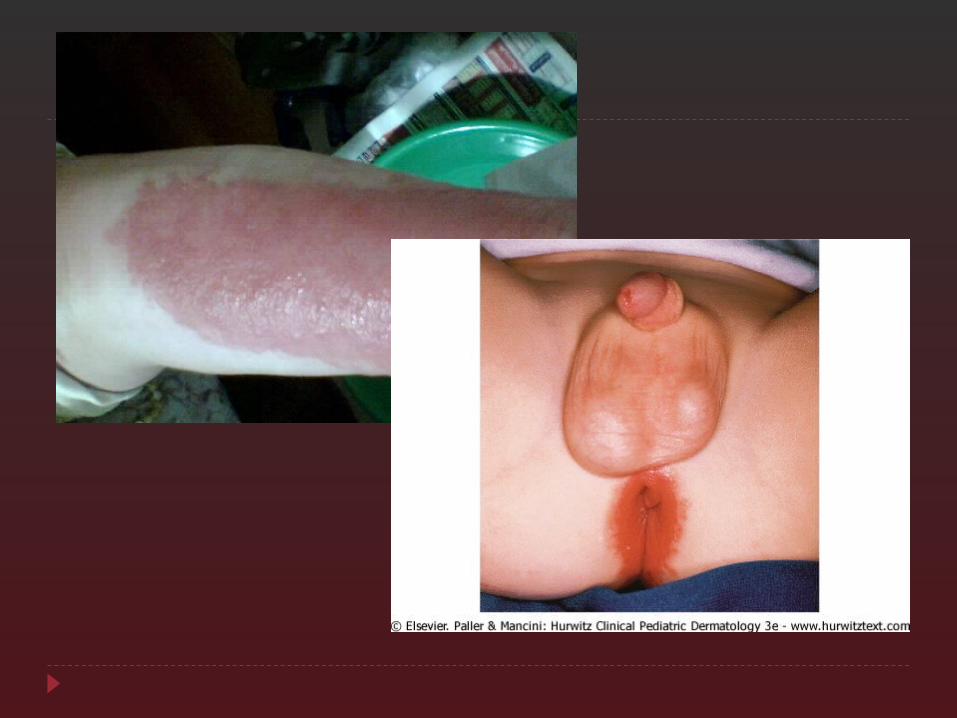
Group A Strep Streptococcus pyogenes Mode of transmission: Contact Clinical
Upper respiratory tract Acute pharyngitis & Scarlet Fever Serous rhinitis, OM, sinusitis, RPA, peritonsillar abscess,
cervical adenitis Skin
Impetigo, Erysipelas, Perianal cellulitis, Pyoderma Other
PNA, endocarditis, septic arthritis, cellulitis, necrotizing fasciitis, osteomyelitis, TSS
Treatment of choice PCN G IM or PCN V PO Marcolides for allergic patients
Return to School 24 hrs after treatment
GAS Nonsuppurative Sequelae (What?!?!) Rheumatic Fever
Follows pharyngitis NOT skin infections THE REASON WE TREAT JONES + Documented Strep infection (ASO)
Joints – Migratory polyarthritis -- Carditis (new murmur) Nodules – subcutaneous Erythema marginatum Sydenham chroea
What are the minor criteria??? Fever Arthralgia Elevated ESR/CRP Prolonged PR interval
Those Sequelae (cont…) Glomerulonephritis
Can follow pharyngitis (1-2 wks) or skin infection (3-6 wks)
Clinical Hematuria (RBC cast in urine) Proteinuria Edema HTN
Low C3
Streptococcus pneumonia Clinical
AOM, sinusitis, CA PNA, conjunctivitis, periorbital cellulitis osteomyelitis, endo-/peri- carditis, soft tissue infxn Before PCV7, most common cause of AOM
Most common cause of meningitis in children (along with meningococci)
Mode of transmission Contact (respiratory droplets
Treatment PCN G, Rocephin, Claforan, Vancomycin

What are we dealing with????
Treatment of MRSA Severe/Invasive: Vancomycin +/- Gentamicin +/- Rifampin Skin/soft tissue: Bactrim, Clindamycin PNA/Septic arthritis/osteomyelitis: Clindamycin
26 week old preterm infant has developed a line-associated Staph epidermidis sepsis
Does anyone know the most effective antibiotic regimen for this infant??? Ampicillin Ampicillin + Gentamicin Ceftriaxone Oxacillin + Gentamicin Vancomycin + Rifampin
Staphylococcus epidermidis Coagulase negative Staph Lab tests
Gram stain & culture (look at susceptibilities) DO NOT ASSUME CONTAMINATE in neonates, IC, prosthetic
device/hardware…….REPEAT & START EMPIRIC ABTX Clinical syndromes
If not a contaminate Health care associated infections #1 cause of VP shunt infections (ventriculitis) Infection of implanted hardware, catheters, shunts,
prosthetic devices Endocarditis, PD cath peritonitis, UTIs, Osteomyelitis
Sepsis in preterm infants, sepsis/bacteremia in IC children Treatment
Lots of resistance: Methicillin, Ceftriaxone, Clindamycin, Macrolides
Empiric treatment – Vancomycin +/- Rifampin or Gentamicin, Cipro
Remove foreign body
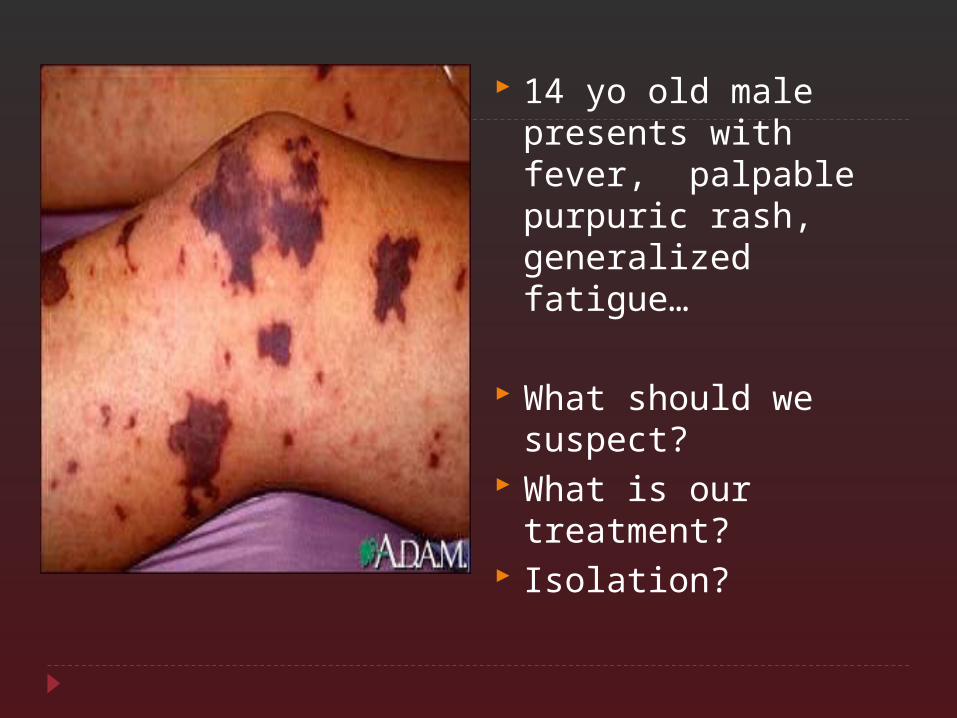
14 yo old male presents with fever, palpable purpuric rash, generalized fatigue…
What should we suspect?
What is our treatment?
Isolation?
Neisseria meningitidis Clinical syndromes
Meningococcemia and/or Meningitis Rapid onset of fever/chills, malaise, maculopap./petechial rash Waterhouse Friderichsen Syndrome – fulminant disease
Sequelae – hearing loss, neuro deficits, digit/limb amputation
Lab diagnosis Presumptive – gram negative diplococci sterile fluid Confirmed – isolation/culture from sterile site or clinical
(petechial/purpuric lesions + clinical illness) Treatment
PCN G Alternatives: Rocephin, Claforan, Ampicillin
Isolation: Droplet Prophylaxis
Close contacts Rifampin (children); Rifampin, Rocephin, Cipro (Adults)
2 yo old female with ALL has developed enterococcal bacteremia.
You begin treatment with vancomycin She remains febrile after 48 hrs of vancomycin
therapy
What should you be concerned about? What do you need to check?
Dealing with Vancomycin Resistant Enterococcus
What is the most effective treatment? A. Ampicillin B. Cipro C. Linezolid D. Ticarcillin
E. Vanc
Enterococcus Enterococcus faecalis & Enterococcus faecium Clinical
UTI, bacteremia, endocarditis, meningitis, device associated infections, intra-abdominal abscess, peritonitis
Treatment Ampicillin / Vancomycin +/- Gentamicin **Don’t forget resistance patterns Check
susceptibilities VRE (Vancomycin resistant) strains, ampicillin, &
cephalosporins VRE present treat with Linezolid
THAT’S ALL FOR ME!!!!!