Hypoxic spell - ped.si. · PDF file• Correct metabolic acidosis : Sodium bicarbonate 1-2...
60
Patient management Patient management Hypoxic spell Hypoxic spell ี ี พญ.สินีนาต ฑี ฆวาณิช พญ.ภัทรพร จําปาสัก คุณสุพรรณี หอมชะเอม อ.พญ. ชดชนก วิจารสรณ 22/4/58
Transcript of Hypoxic spell - ped.si. · PDF file• Correct metabolic acidosis : Sodium bicarbonate 1-2...
Patient managementPatient management
Hypoxic spellHypoxic spell
พญ.สนนาต ฑฆวาณชพญ.ภทรพร จาปาสก
คณสพรรณ หอมชะเอมอ.พญ. ชดชนก วจารสรณ
22/4/58
HistoryHistory
HistoryHistory
Case เดกหญงอาย 11 เดอน
• Underlying disease TOF with severe PS base line O2 • Underlying disease TOF with severe PS, base line O2
sat = 60-65%
• เคยม hypoxic spell มาแลว 3 ครง ICU
on propranolol 1 mg/kg/dayon propranolol 1 mg/kg/day
• 4 days : ม fever with URI อาการเขยวพอๆเดม ไมเหนอย
• 2 days : หอบมากขน กนไดนอย อาเจยน
• 30 mins: เหนอยมากขน เขยวมากขน มารพ ศรราช• 30 mins: เหนอยมากขน เขยวมากขน มารพ. ศรราช
Physical examinationPhysical examinationPhysical examinationPhysical examination
• V/S : T 38 ºC, RR 40/min, PR 170/min,
BP 118/80 BW 6 kBP 118/80, BW 6 kg
O2 sat 10 % on canula 5 LPM O sat 0 % o ca u a 5
O2 sat 40-50%
• GA : generalized cyanosis (central+peripheral)
marked agitation, not pale
• CVS: normal S1 single S2 no murmurCVS: normal S1, single S2, no murmur

Physical examinationPhysical examinationPhysical examinationPhysical examination
• RS : coarse crepitation both lung,
subcostal and suprasternal
retractionretraction
• Abd : soft , liver 1 cm BLCM
• Ext : equal movement
• POCT 122 mg %
P bl li tP bl li tProblem listProblem list
• U/D TOF with previous hypoxic p yp
spell
• Tachypnea and more cyanosis
• No murmur
• Fever with crepitation both lungs
Q ti ?Q ti ?Questions?Questions?
What is the most likel diagnosis?• What is the most likely diagnosis?
Wh t th i t • What are the appropriate
management?management?
DiagnosisDiagnosis
• TOF with hypoxic spell
• Pneumonia
Common congenital cyanotic Common congenital cyanotic Common congenital cyanotic Common congenital cyanotic heart diseaseheart disease
• Tetralogy of Fallot (TOF)
• Transposition of great arteries (TGA)
• Truncus arteriosus
• Total anomalous pulmonary venous
return (TAPVR)
• Tricuspid valve abnormalities (TVA)
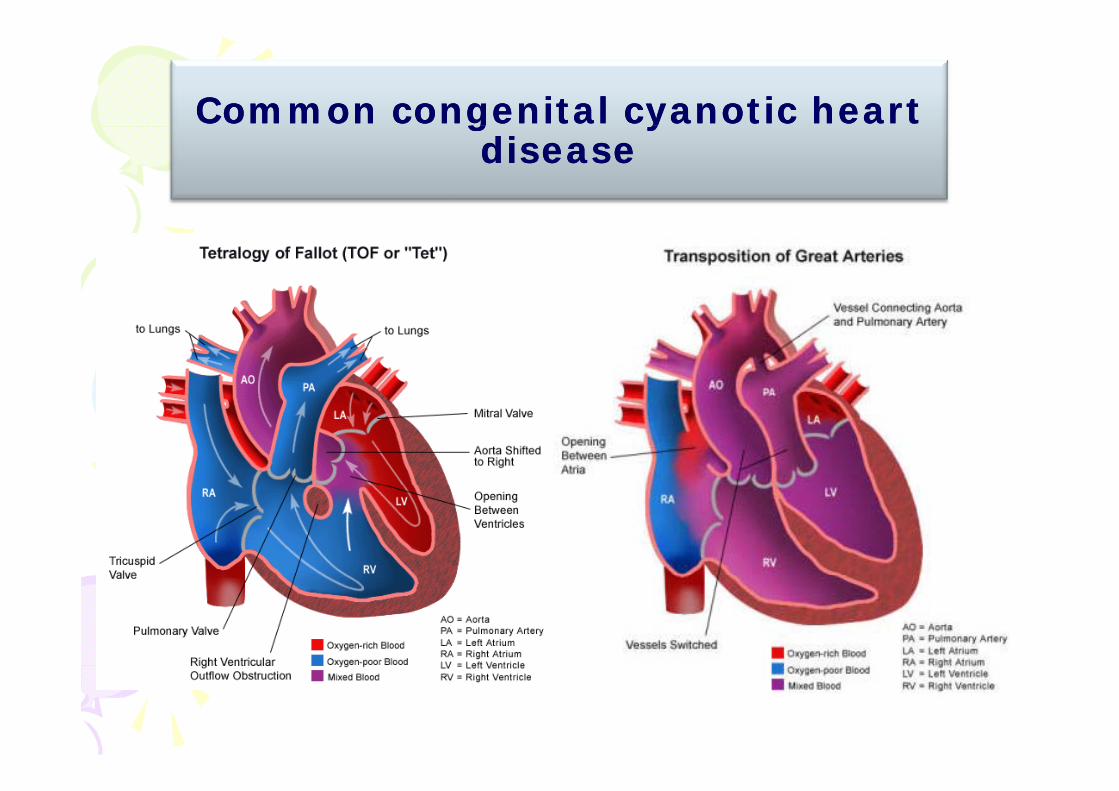
Common congenital cyanotic heart Common congenital cyanotic heart g yg ydiseasedisease

Common congenital cyanotic heart Common congenital cyanotic heart Common congenital cyanotic heart Common congenital cyanotic heart diseasedisease
Emergency in Pediatric Emergency in Pediatric di l di idi l di iCardiovascular ConditionsCardiovascular Conditions
• Cardiogenic shock
• Congestive heart failure
Hypoxic spell• Hypoxic spell
• Cardiac arrhythmia:y– Tachyarrhythmia
– Bradyarrhythmia
• Pulmonary hypertensive crisis• Pulmonary hypertensive crisis
Congenital cyanotic heart disease Congenital cyanotic heart disease Congenital cyanotic heart disease Congenital cyanotic heart disease with hypoxic spellwith hypoxic spell
• TOF• TOF
• Tricuspid atresiaTricuspid atresia
• Ebstein’s anomalyEbstein s anomaly
• PA/IVS
• Severe PS
Hypoxic spellHypoxic spellHypoxic spellHypoxic spell
Hypoxic spellHypoxic spellHypoxic spellHypoxic spell
• Paroxysmal hypoxic spell
• Hypercyanotic spell
• Tetralogy spell
• Paroxysmal dyspnea• Paroxysmal dyspnea
Required Required immediatedimmediated treatment treatment
due to serious CNS complicationdue to serious CNS complication
Pediatric cardiology for practitioners by Myung K.Park
Hypoxic spellHypoxic spell
D fi iti
Hypoxic spellHypoxic spell
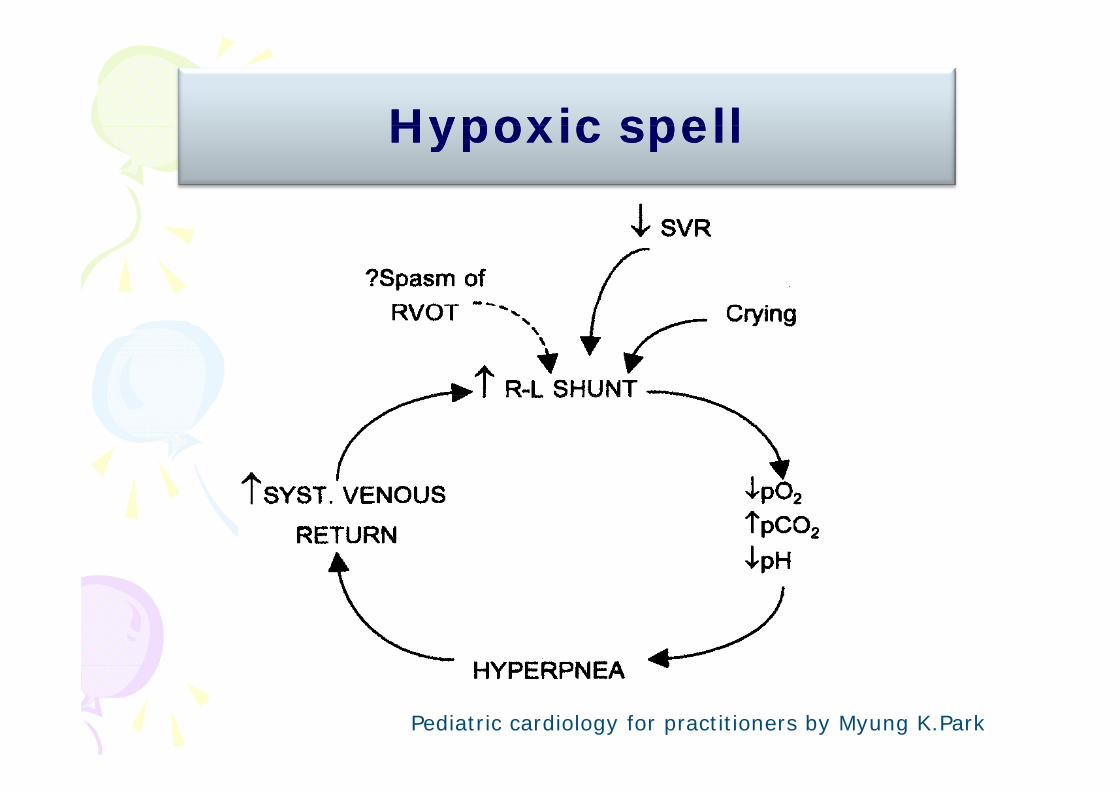
• Definition : Sudden and transient uncompensated
hypoxia in cyanotic heart diseases ( Rt. to Lt. shunt)
• TOF is the prototype
• Self limited in 15-20 mins.
• Depend on balance between pulmonary and systemic • Depend on balance between pulmonary and systemic
pressure and resistance
• Precipitating factors: crying, defecation , exercise, sudden fright
• Common in infants and young children
Hypoxic spellHypoxic spellHypoxic spellHypoxic spell
• Mechanism
– Infundibular spasm
– Decreased SVR
– Tachycardia
H– Hyperpnea
Hypoxic spellHypoxic spellHypoxic spellHypoxic spell
Pediatric cardiology for practitioners by Myung K.Park
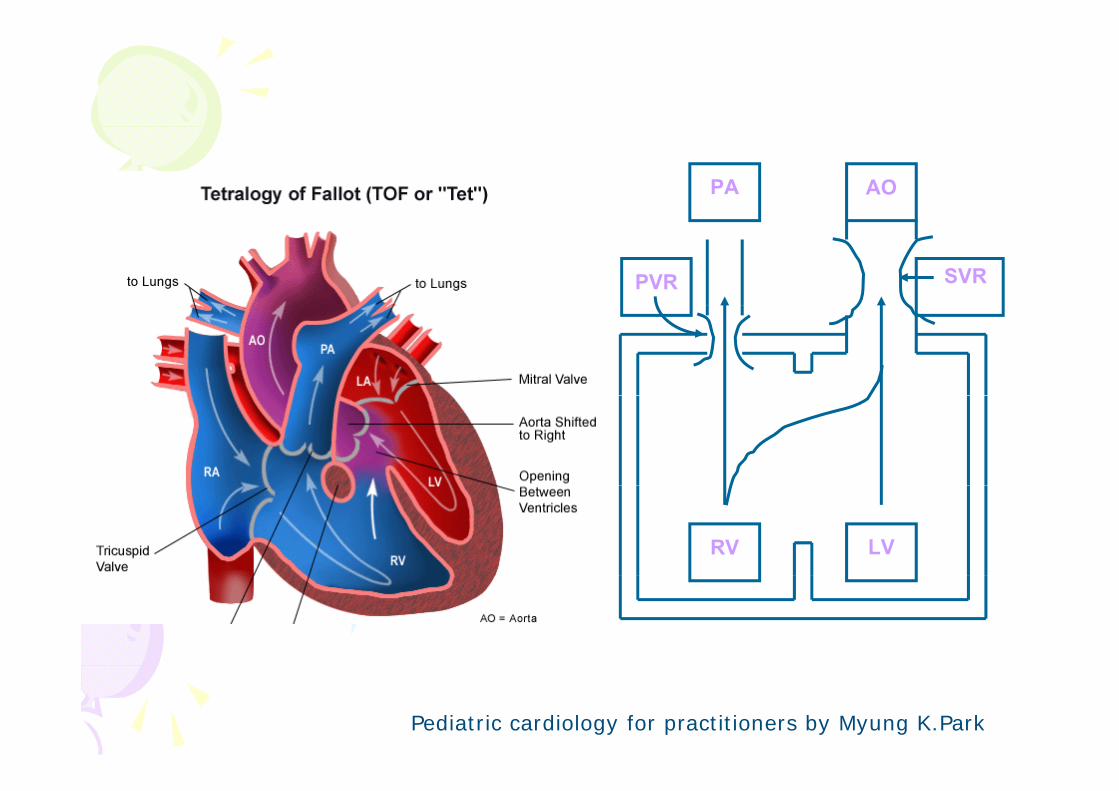
PA AO
PVR SVR
RV LV
Pediatric cardiology for practitioners by Myung K.Park
Sign and symptomsSign and symptomsg y pg y p
• Increase in cyanosis
• Hyperpnea, dyspneaHyperpnea, dyspnea
• Decrease intensity of SEM or murmur
disappear
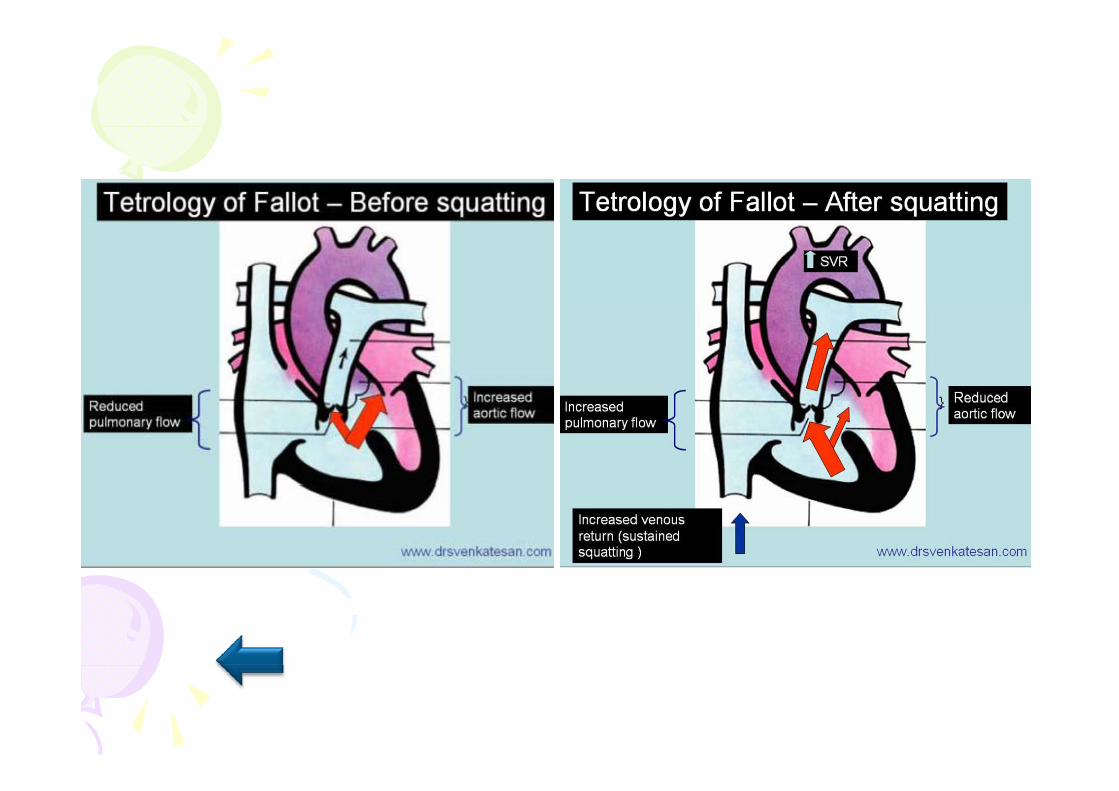
• Squatting • Squatting
• Hypotension
• Syncope, concious change
• Convulsion
In estigationIn estigationInvestigationInvestigation
• Oxygen saturation
• CBC
• UA
• CXR
• EKG
Management in hypoxic Management in hypoxic spell crisisspell crisisspell crisisspell crisis
Management in hypoxic spell Management in hypoxic spell Management in hypoxic spell Management in hypoxic spell crisiscrisis
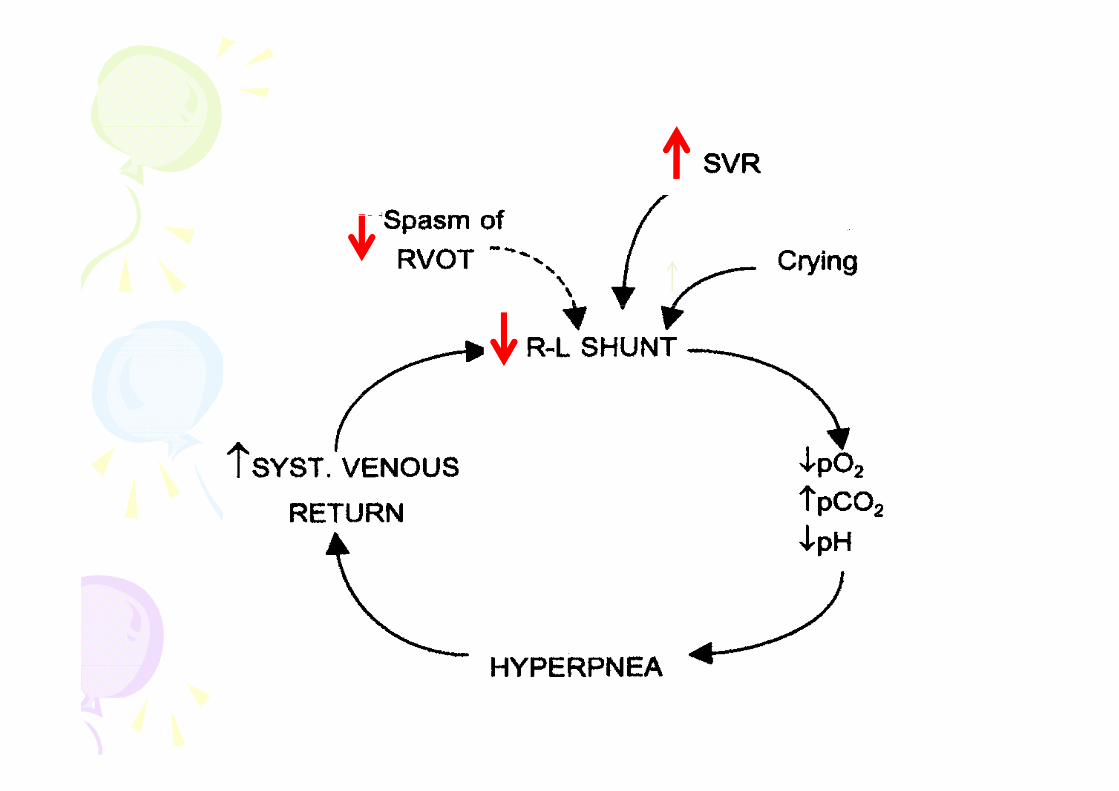
P i i l • Principle :
– Decrease RVOT obstruction (decrease Decrease RVOT obstruction (decrease
Rt to Lt shunt)
– Decrease sympatetic
I SVR– Increase SVR
Management in hypoxic spell crisisManagement in hypoxic spell crisis
K t h t iti ลด t เพม SVR
Management in hypoxic spell crisisManagement in hypoxic spell crisis
• Knee-to-chest position : ลด venous return, เพม SVR
• Oxygen supplement : ลด hypoxia
• Sedation :
- Morphine 0.05-0.1 mg/kg/dose dilute IV slowly push:
ลด venous return, infundibular muscle คลายตว
- Ketamine 1-3 mg/kg/dose IV : เพม SVR
t t i BP it i d i d ti- protect airway, BP monitoring during sedation
• Correct metabolic acidosis : Sodium bicarbonate
1-2 mEq/kg IV

Squatting/KneeSquatting/Knee toto chestchestSquatting/KneeSquatting/Knee--toto--chestchest
Management in hypoxic spell crisisManagement in hypoxic spell crisis
P l l 0 1 /k IV i f dib l l
g yp pg yp p
• Propranolol 0.1 mg/kg IV : infundibular muscle
คลายตวอาจลด SVR (monitor HR)( )
• Correct anemia
• Correct hypovolemia : Keep normal systemic BP :
IV load/ inotropeIV load/ inotrope
• Correct hypoglycemia : 25% glucose 1-2 cc/kg/dose
IV push
C i f i• Correct infection
Management in hypoxic spell crisisManagement in hypoxic spell crisis
• In severe case need deep sedation
( Paralyze and ventilate )
• Consult CVT for eemergencymergency shuntshunt
surgerysurgery
• Close follow up blood gas, correct acidosis
In this patientIn this patientIn this patientIn this patient

Management at ERManagement at ER
• Knee-chest position : ชวงแรกรองมากทาไมได ตอน
Management at ERManagement at ER
• Knee-chest position : ชวงแรกรองมากทาไมได ตอน
หลงสงบลง ทาไดโดยมารดา
ไ• Oxygen supplement : mask with bag 10 LPM ไมยอม
รองมาก corrugated tube 10 LPM
• Sedation :
- Chloral hydrate 1 ml/kg/dose oral บวนทง
- Morphine 0.1 mg/kg/dose IV x 3 dosesp g g
- Ketamine 1mg/kg/dose IV x 1 dose
- Valium 0.3mg/kg/dose IV x 1 dose
Management at ERManagement at ERManagement at ERManagement at ER
• Correct acidosis: 7.5%NaHCO3 1
mEq/kg/dose x 2 dosemEq/kg/dose x 2 dose
• Correct hypovolemia
- NSS 20 ml/kg IV load x 1 dose then MT
HR 150/min, BP 100/50 mmHg, oxygen sat 84%
Admit CCU• Admit CCU
Proper management after Proper management after hypoxic spell crisis hypoxic spell crisis hypoxic spell crisis hypoxic spell crisis
improveimprove

ป ป การพยาบาลผปวยเดกการพยาบาลผปวยเดกhypoxic spellhypoxic spellhypoxic spellhypoxic spell
สพรรณ หอมชะเอม
PCCU (อน.7) งานการพยาบาลกมารเวชศาสตร( )

N iN iNursing care at Nursing care at ccuccu To monitor the oxygenation & cardiovascular status
• รบกวนผปวยใหนอยทสด ลดสงกระตน (pain) ส ส (pa )
• ใหออกซเจน : cannula, blow-by
M it S O RR HR EKG BP & ti f i• Monitor : SpO2,RR, HR, EKG, BP & tissue perfusion
• ปลอบใหสงบ , Knee - chest position
• ดแลใหยาและสารนา chloral hydrate, morphine, dormicun, fentanyl
NaHCO3, esmolol, vasopressor, Inotrope, IVF
Nursing care at Nursing care at ccuccuNursing care at Nursing care at ccuccu
• ตดตามผลตรวจทางหองปฏบตการ : ABG, BS , CBC
• ดแลใหญาตเขาเยยม ใหและรบขอมลจากญาตผปวย ญ ญ
• Severe case (progressive hypoxemia)
i b i il CPR เตรยม intubation , ventilator, เตรยมพรอม CPR
ยา sedate, inotrope IV. Drip
ตดตอประสานงานกบหนวยงานทเกยวของ, ญาต
ป ป ป ไป เตรยมผปวย อปกรณ บคลากร เพอเคลอนยายผปวยไปผาตด
Proper Proper management at management at wardwardProper Proper management at management at wardward
• Minimal interrupt patient
• Need parent help to calm down patient• Need parent help to calm down patient
- Irritable/severe crying severe hypoxic spell
severe hypoxia convulsion/CVA, sudden cardiac arrestcardiac arrest
- Need sedation before procedure eg. chloral
hydrate before IV access
• Monitor oxygen saturation : keep > 75%
Proper Proper management at management at wardwardProper Proper management at management at wardward
• Monitor BP : keep normal BP, normal volume
statusstatus
• Work up cause
Infection : CBC,UA,CXR
Acidosis : blood gas keep pH 7.35—7.45
Anemia : Hct keep 50 60%Anemia : Hct keep 50-60%
Echocardiographyg p y
Pediatric cardiology for practitioners by Myung K.Park
Consequence and severe Consequence and severe Consequence and severe Consequence and severe complicationcomplication
• Brain abscess
• Cerebral infarction
• Thrombosis• Thrombosis
• Infective endocarditis
• Coagulopathy
• Polycythemia
Growth/development/nutrition• Growth/development/nutrition
Pediatric cardiology for practitioners by Myung K.Park
Proper management at wardProper management at ward
• Adequate Fe supplement: keep Hct 50-60%
p gp g
dequate e supp e e t eep ct 50 60%
(stop Fe if Hct >= 60%)
• Total correction
• Propranolol 1-2 mg/kg/day: prevent spellsPropranolol 1 2 mg/kg/day: prevent spells
• If discharge
- Teach parent how to detect hypoxic spells
and initial managementg
- IE prophylaxis before invasive procedure
- Good oral hygiene care : correct dental caries

P iP iProgressionProgression
• Streptococcus pneumoniae pneumonia
PIP/TAZ x 14 day- PIP/TAZ x 14 day
- Ventolin + Combivent NB
• Deep sedation
- Fentanyl IV drip
Mid l IV d i- Midazolam IV drip
- Rocuronium IV dripp
ProgressionProgressionProgressionProgression
• Set OR for RMBTSRMBTS no complication
• Post op : heparin IV drip x 3 day
then ASA(81) ½ tab oral OD
• Oxygen saturation 91%
SurgerySurgerySurgerySurgery
• Palliative (systemic to pulmonary shunt)
f Modified Blalock-Taussig shunt
(subclavian artery - pulmonary artery)(subclavian artery - pulmonary artery)
• Definite ( total correction )( )
- BW > 10 kg
- McGoon ratio > 1.5
Common cardiovascular diseases from pediatrics to adults,รศ.พญ.จารพมพ สงสวาง, รศ.นพ. กฤตยวกรม ดรงคพสษฏกล

P lli ti P lli ti M difi d Bl l kM difi d Bl l kPalliative Palliative Modified BlalockModified Blalock--TaussigTaussig shuntshunt
IndicationIndicationIndicationIndication
• BW < 2.5 kg + severe cyanosisBW 2.5 kg severe cyanosis
• Hct >= 65%
• Pulmonary artery ขนาดเลก
• Severe hypoxic spell
Common cardiovascular diseases from pediatrics to adults,รศ.พญ.จารพมพ สงสวาง, รศ.นพ. กฤตยวกรม ดรงคพสษฏกล
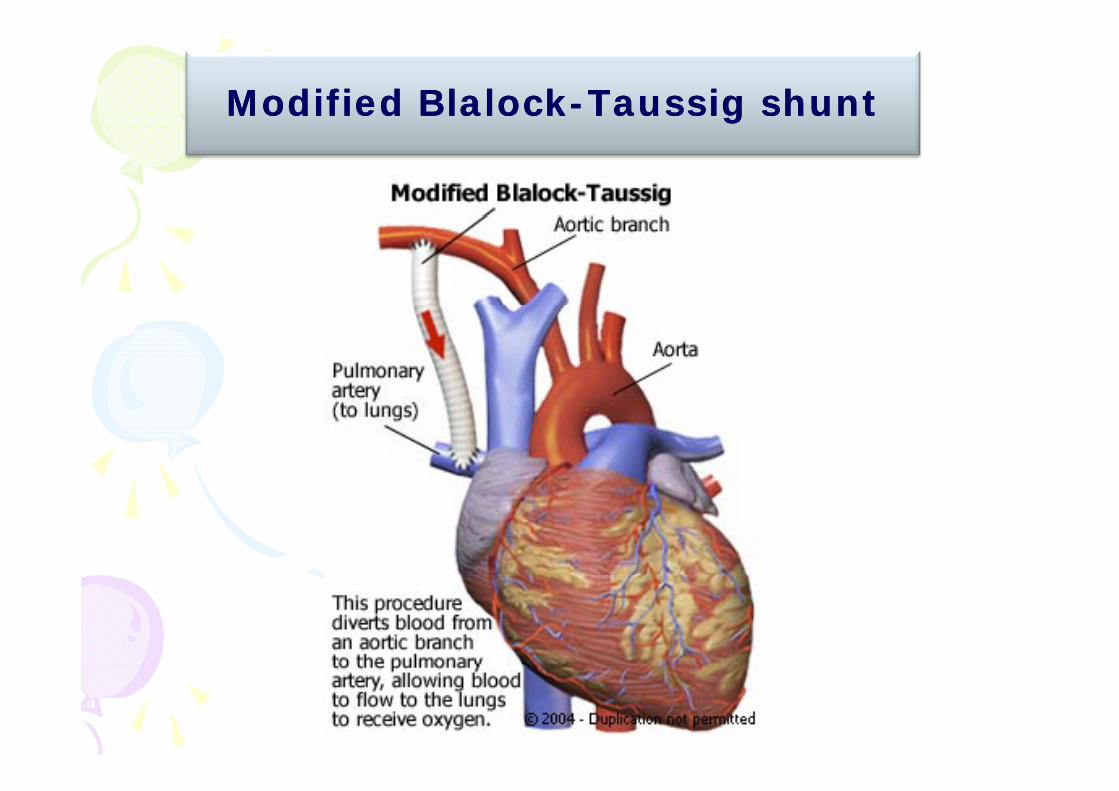
Modified BlalockModified Blalock--TaussigTaussig shuntshunt
Post operation MBTSPost operation MBTSPost operation MBTSPost operation MBTS
• Size graft selection: 3.5-6 mm
• If graft <= 4 mm : Heparin IV 10 unit/kg/hr allIf graft <= 4 mm : Heparin IV 10 unit/kg/hr all
graft = 5 mm : Heparin IV 10 unit/kg/hr in
high risk case
graft >= 6 mm: no heparing p
• ASA 5 mkday
• Keep oxygen saturation: < 6 mo 85-90%
> 6 mo 90-95%
Congenital heart disease,พรเทพ เลศทรพยเจรญ,วชย เบญจชลมาศ
DesaturationDesaturation after MBTSafter MBTS
• Diferrential diagnosis ?
Early complication post shuntEarly complication post shunt
• Bleeding : Hemothorax
y p py p p
g
Cardiac tamponade
• Pneumothorax
• Shunt thrombosis• Shunt thrombosis
• Low flow shunt: hypoxia, acidosis
• High flow shunt: CHF
• Aspiration, hoarseness of voice
• SeromaSeroma
Congenital heart disease,พรเทพ เลศทรพยเจรญ,วชย เบญจชลมาศ
Late complication post shuntLate complication post shunt
• Pericardial effusion, delayed cardiac , y
tamponade
• Recurrent pleural effusion (seroma)
• Shunt thrombosis or stenosis
• Infective endocarditis
Congenital heart disease,พรเทพ เลศทรพยเจรญ,วชย เบญจชลมาศ
M t h M t h Management when Management when desaturationdesaturation
• V/S
• BP
• CXR
Nursing Nursing care post RMBTScare post RMBTSNursing Nursing care post RMBTScare post RMBTS
Assess, monitor to intervene effectively – Respiratory care : oxygenationRespiratory care : oxygenation– Hemodynamic status– Wound ICD : bleeding?Wound , ICD : bleeding?– Pain management– CNS : consciousness seizureCNS : consciousness, seizure– Fluid & elecrtrolyte replacement– Renal function– Renal function– Thermal regulation
Nursing Nursing care post RMBTScare post RMBTSNursing Nursing care post RMBTScare post RMBTS
Clinical monitoring (shunt thrombosis)
SpO2 < 80%
BP <คาปกต pulse pressure <20 or 1/3 SBP BP <คาปกต, pulse pressure <20 or 1/3 SBP
sign of irritable, hyperpnea ti f i poor tissue perfusion urine output < 1 ml/kg/hr

SirirajSiriraj concurrent trigger toolconcurrent trigger toolSirirajSiriraj concurrent trigger toolconcurrent trigger tool
• การบรหารความเสยงเชงรก เพอเพมความ
ปลอดภยใหกบผปวย
โ • จดทาเครองมอโดยทมสหสาขา
• กาหนด Modified Early Warning Sign (MEWS) กาหนด Modified Early Warning Sign (MEWS)
และจดทาแนวทางเพอบรหารความเสยงนนๆ
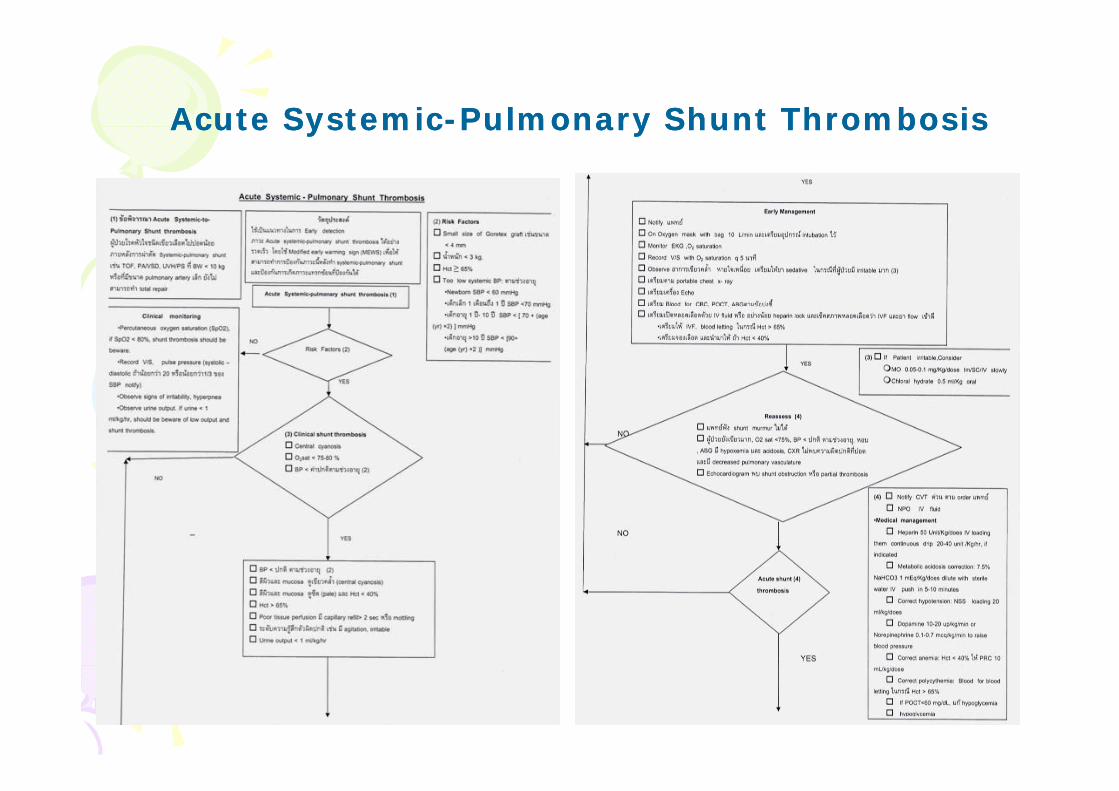
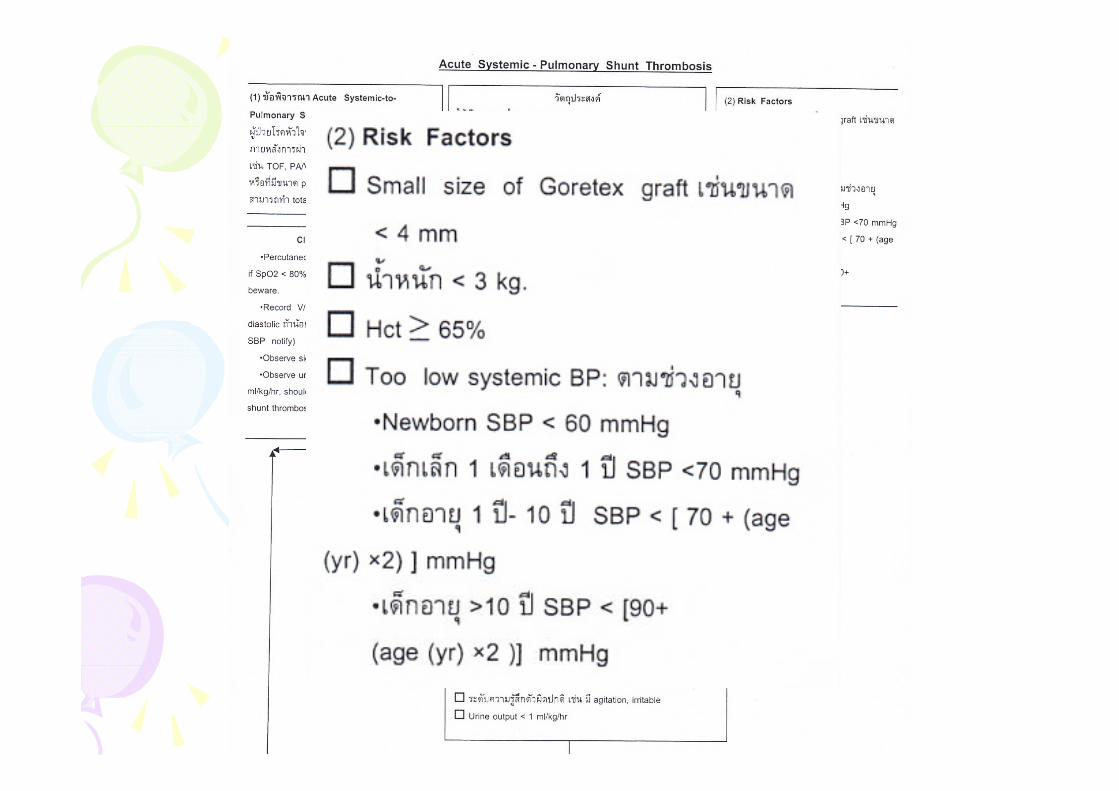
Acute SystemicAcute Systemic--Pulmonary Shunt ThrombosisPulmonary Shunt ThrombosisAcute SystemicAcute Systemic Pulmonary Shunt ThrombosisPulmonary Shunt Thrombosis

Post operation MBTSPost operation MBTSPost operation MBTSPost operation MBTS
• Monitor sign of shunt thrombosis
- Shunt murmur decreased/absent
- DesaturationDesaturation
- CXR : decrease blood flow
• Mx: loading heparin 1 unit/kg/hr IV
NaHCO3 keep BE > -3
Inotropic drugInotropic drug
Congenital heart disease,พรเทพ เลศทรพยเจรญ,วชย เบญจชลมาศ
Long term complication after surgeryLong term complication after surgery
• Endocarditis
Long term complication after surgeryLong term complication after surgery
• Endocarditis
• Aortic regurgitation, Residual pulmonary
regurgitation
• LV dysfunction, RV dysfunctiony , y
• Residual RVOT obstruction
• Exercise intolerance
• Heart block, tachyarrhythmia, ventricular y y
tachycardia
S dd di d th• Sudden cardiac death
Risk factor for morbidity and Risk factor for morbidity and Risk factor for morbidity and Risk factor for morbidity and mortality after total correctionmortality after total correction
• Age < 8 mo
• Transannular patch ผาน pulmonic annulus
• Abnormal pulmonic valve/size < 50%• Abnormal pulmonic valve/size < 50%
• ผาตดผาน ventricle เปนรอยใหญ
• RV pressure/LV pressure in post op 24 hr >0.7
(residual RVOTO)(residual RVOTO)
• Pulmonary regurgitation
Common cardiovascular diseases from pediatrics to adults,รศ.พญ.จารพมพ สงสวาง, รศ.นพ. กฤตยวกรม ดรงคพสษฏกล