Hum. Reprod. 2003 Parsanezhad 1432 7

of 6
Transcript of Hum. Reprod. 2003 Parsanezhad 1432 7
-
7/30/2019 Hum. Reprod. 2003 Parsanezhad 1432 7
1/6
Ovarian stromal blood ow changes after laparoscopicovarian cauterization in women with polycystic ovarysyndrome
Mohammad Ebrahim Parsanezhad1,4, Mohammad Hadi Bagheri1, Saeed Alborzi2 andErnst Heinrich Schmidt3
1Department of Obstetrics and Gynecology, School of Medicine and 2Department of Radiology, Medical School, Shiraz University
of Medical Sciences, Shiraz, Iran and3
Department of Obstetrics and Gynecology, evang. Diakonie teaching hospital, Gottingen
University, Bremen, Germany
4To whom correspondence should be addressed at: PO Box 713451657, Shiraz, Iran. E.mail: [email protected]
BACKGROUND: Women with PCOS have signicant differences in intra-ovarian and uterine artery haemo-
dynamics. The aims of this study were to compare the ovarian stromal blood ow before and after laparoscopic
ovarian diathermy, and to evaluate the value of these parameters in predicting the outcome of treatment in womenwith polycystic ovaries. METHODS: Colour Doppler blood ow within the ovarian stroma was recorded and serum
concentrations of FSH, LH and testosterone were measured in 52 women with polycystic ovaries before and after
laparoscopic ovarian diathermy. Ovulation was evaluated by folliculometry and progesterone assay in the rst men-
strual cycle after operation. RESULTS: Six to 10 weeks after the diathermy, serum concentrations of LH and testos-
terone decreased signicantly (P = 0.001). The mean TT SD peak systolic velocity decreased from 14.04 TT 6.28 to
12.49 TT 6.32 cm/s (P = 0.001), pulsatility index increased from 0.98 TT 0.36 to 1.78 TT 0.72 (P = 0.001), and resistance
index increased from 0.55TT 0.16 to 0.71 TT 19 (P = 0.001). A total of 73% of the women ovulated. There were signi-
cant negative correlations between pulsatility index and LH (r = 0.43, P = 0.001), pulsatility index and testosterone
(r = 0.40, P = 0.003) and pulsatility index and LH/FSH ratio (r = 0.53, P = 0.001). CONCLUSIONS: Laparoscopic
ovarian diathermy in women with polycystic ovary syndrome may result in a decrease in ovarian stromal blood ow
velocity. There was a signicant correlation between hormonal and ovarian stromal blood-ow changes. Changes in
the Doppler parameters were signicantly higher in women who ovulated. The measurement of ovarian stromalblood ow by colour Doppler may be of value in predicting the outcome of treatment.
Key words: blood ow/cauterization/Doppler haemodynamics/polycystic ovary
Introduction
Polycystic ovary syndrome (PCOS) is the most common cause
of anovulatory infertility accounting for >70% of cases
(Speroff et al., 1999; Kelestimur et al., 2000). This is a topic
more likely to generate greater controversy about aetiology or
pathogenesis than any other disease in gynaecological
endocrinology (Speroff et al., 1999). Recently, there hasbeen much interest regarding the potential role of transvaginal
colour and pulsed Doppler ultrasound in assessing the ovarian
and uterine blood ow of PCOS (Dolz et al., 1999). Most
investigators would agree that the blood ow and the vascular
pattern of an organ are directly related to the organ's
morphology and function (Collins et al., 1991). Women with
PCOS have signicant differences in intra-ovarian and uterine
artery haemodynamics compared with women with normal
ovaries (Battaglia et al., 1995; Aleem and Predanic, 1996;
Zaidi et al., 1998; Vralacnik-Bokal and Meden-Vrtovec, 1998).
The ovarian stromal blood ow differences are likely to be due
to a primary disorder within the polycystic ovary, or vice-versa
(Zaidi et al., 1995). These women have an increased ovarian
stromal blood ow velocity in the early follicular phase of the
normal menstrual cycle (Zaidi et al., 1995; Battaglia et al.,
1997). This increase in ovarian stromal blood ow velocity has
also been observed after pituitary suppression and aftercontrolled superovulation in women undergoing IVF treatment
(Engmann et al., 1999a). Zaidi et al. (1995) have shown a
positive independent relationship between ovarian stromal
blood ow velocity in the early follicular phase and subsequent
ovarian follicular response, even in women with normal
ovaries. In this study, patients with peak systolic velocity,
(PSV) >10 cm/s had a better ovarian response and a higher
clinical pregnancy rate than those with diminished ovarian
stromal blood ow (PSV
-
7/30/2019 Hum. Reprod. 2003 Parsanezhad 1432 7
2/6
with PCOS who are clomiphene citrate (CC) resistant.
Laparoscopic ovarian diathermy (LOD) represents an effective
treatment for patients and possesses numerous advantages over
gonadotrophin therapy (Cohen, 1996).
Although a mechanism explaining the benecial effects of
LOD on PCOS has not yet been demonstrated (Al-Took, 1999),
one possible explanation is that LOD reduces androgen
production, which inhibits normal follicular development(Tulandi et al., 1997). The ovarian stromal blood ow
abnormalities in PCOS have been previously described
(Battaglia et al., 1995; Aleem et al., 1996; Zaidi et al., 1998;
Vralacnik-Bokal and Meden-Vrtovec, 1998), the possible
effects of medical induction of ovulation on ovarian blood
ow (Agrawal, 1998; Zaidi et al., 1998; Zaidi, 2000), effects of
LOD on ovarian steroidogenesis (Greenblatt and Casper, 1987;
Cohen, 1996; Felemban et al., 2000) and on ovarian stromal
echogenecity (Al-Tooket al., 1999) in CC-resistant PCOS have
been also described. The inuence of LOD on the ovarian
stromal blood ow has not as yet been studied. Evaluation of
ovarian stromal blood ow before and after LOD may be
considered a way to study the effects of this therapeutic
intervention, or the mechanism by which the ovary may
respond. The aims of this study were (i) to compare the ovarian
stromal blood ow before and after LOD and (ii) to evaluate the
value of these parameters in predicting the outcome of treatment.
Materials and methods
From December 1996 to April 2002, 79 women with PCOS were
studied in the Infertility and Reproductive Endocrinology Division,
Department of Obstetrics and Gynecology, Shiraz University of
Medical Sciences, Shiraz, Iran, the Department of Obstetrics and
Gynecology evang. Diakonie Teaching Hospital, Gottingen
University, Bremen, Germany and the Department of Radiology,
Shiraz University of Medical Sciences, Shiraz, Iran. Patients' ages
were 1932 years. Clinical evidence of hyperandrogenism was noted
in all patients. Serum levels of LH, FSH and testosterone were
measured in the early follicular phase (days 24 of the spontaneous or
induced menstrual cycle) using the radioimmunoassay technique
(RIA). Baseline transvaginal colour Doppler ultrasound scanning was
performed on days 24 of the cycle to assess ovarian stromal bloodow. Criteria for inclusion were the following: infertility secondary to
anovulation, as indicated by amenorrhoea or oligomenorrhoea,
elevated serum LH levels, normal or low FSH levels, elevated LH/
FSH ratio, clinical evidence of androgen excess (acne, hirsutism),
elevated serum levels of testosterone and ultrasound ndings of
enlarged ovaries with multiple small cysts scattered around the
periphery and highly echogenic stroma, and previously documented
anovulation by transvaginal ultrasound follicular monitoring while
taking clomiphene citrate (CC) in doses of b150 mg.
Hysterosalpingography, post-coital test and semen analysis were
normal in all subjects. The Ethics Review Committee for Human
Research at our university approved the study. Informed consent was
obtained from each individual. Laparoscopic ovarian diathermy was
performed using the two-puncture technique. We used an optic thathad an operative channel. The laparoscope was introduced through a
sub-umbilical incision and grasping forceps were introduced
suprapubically to stabilize the ovary by grasping the ovarian ligament.
After assessment of the pelvic structures and tubal patency, an
insulated needle connected to a unipolar electrocautery unit was
inserted through the operative channel of the optic. Eight to 10 cautery
points 34 mm in diameter were created in each ovary with a current
of 4 mA applied through the laparoscopic-insulated needle. Hormonal
assay and blood ow assessment were performed 2 days after the
operation and repeated 610 weeks thereafter (in the early follicular
phase of the rst post-operative menstruation). Folliculometry was
performed on days 1517 and serum progesterone concentration was
measured on days 1921 (mid-luteal phase) of the same cycle. This
cycle was monitored to assess hormonal prole, ovarian stromalDoppler parameters and nally to detect ovulation. Ovulation was
considered when the mean diameter of the leading follicle was b15
mm and serum progesterone level b5 ng/ml. A single radiologist
performed all Doppler sonographies. Pulsatility index (PI), resistance
index (RI), and peak systolic velocity (PSV) were measured in each
scan. A colour Doppler ultrasound machine (Aloka Model SSD-1700)
with a 5 MHz transvaginal transducer was used. Stromal blood ow of
both ovaries was evaluated by colour and power Doppler
ultrasonography. By means of colour and power Doppler ow
imaging, colour signals were searched in the ovarian stroma away
from the ovarian surface or near the wall of a follicle. By placing the
colour Doppler gate over the ovarian stroma, areas of maximum
colour intensity, representing the greatest Doppler frequency shifts,
could be visualized, then selected for pulsed Doppler examination.Peak systolic blood ow velocity wave-forms were thus detected, and
optimal ow velocity wave-forms were selected for analysis after
angle correction. Then PI and RI were calculated in each selected
Doppler wave. Both right and left ovaries were observed and analysed
in each patient, revealing no statistical signicance in Doppler
parameters of ovarian stromal arteries. Therefore, the mean value for
all ovarian blood ow parameters was calculated and used in the
statistical analysis. The intra-ovarian blood ow of each ovary was
assessed by studying blood vessels in the ovarian stroma (small
arteries in the ovarian stroma not close to the surface of the ovary or
near the wall of a follicle).
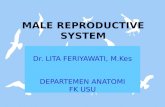
Figure 1. Pattern of hormonal and Doppler parameter changes inwomen with PCOS undergoing ovarian diathermy. * = Signicantdifferences of each variable (comparison of before and 610 weeksafter operation) (P < 0.05).
Ovarian stromal blood ow changes
1433
-
7/30/2019 Hum. Reprod. 2003 Parsanezhad 1432 7
3/6
Statistical methods
The relationship between ovarian stromal blood ow indices and
hormonal changes after LOD was examined by the Pearson correlation
test. Paired t-test was used to compare mean values. In order to
determine the correlation between Doppler indices and hormonal
changes including ovulation, we used t-test and Pearson correla-
tion test. The data were rst tested for normality using the
KolmogrovSmirnov test. P < 0.05 was considered statistically
signicant.
ResultsA total of 79 women was recruited but 27 cases were excluded
from the analysis because they had not completed the
measurements. Therefore, 52 patients were used for the nal
analysis. Data analysis showed a fall in the serum concentra-
tions of LH, testosterone and LH/FSH ratio starting on day 2
after LOD. Hormonal prole and Doppler parameters, before, 2
days and 610 weeks after the operation are shown in Figure 1.
LH decreased from 16.86 T 4.53 pre-operatively to 11.7 T
4.82 mIU/ml (610 weeks after operation) (P = 0.001). Mean
T SD serum concentrations of testosterone before and 610
weeks after the operation were 1.18T 0.32 and 0.72T 0.28 ng/
ml respectively (P = 0.001). When compared with pre-
operation levels, serum concentration of FSH increased from6.24 T 1.85 before operation to 7.55 T 1.98 mIU/ml 610
weeks after operation (P = 0.03). The mean T SD of PI and RI
(610 weeks after operation) were signicantly higher than
those in pre-operation values (P = 0.001), and that of PSV was
signicantly lower (P = 0.001). LH/FSH ratio decreased from
2.67T 0.55 before LOD to 1.59T 0.65, 610 weeks thereafter.
Changes in serum hormonal concentrations and Doppler blood
ow velocity and 95% condence interval of the differences,
before and 610 weeks after LOD are shown in Table I. We
found signicant negative correlations between LH and PI ( r=
0.43, P = 0.001), testosterone and PI (r = 0.40, P = 0.003),
testosterone and RI (r= 0.30, P = 0.043), LH/FSH ratio and PI
(r= 0.53, P < 0.001) and RI (r= 0.43, P = 0.001). Correlations
between hormonal and Doppler parameter changes are shown
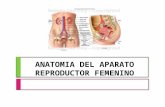
in Table II. Of all the women, 73.1% ovulated as indicated by
mid-luteal serum progesterone levels (b5 ng/ml) and leading
follicular diameter (b15 mm). After adjustment, PI increased
signicantly in women who ovulated after LOD (P = 0.001).
Although statistically insignicant, in the adjusted analyses, an
Table I. Pre-operative and post-operative serum hormone concentrations, Doppler blood ow velocity and 95% condence intervals of the differences inwomen with PCOS undergoing ovarian diathermy. Values are mean T SD
FSH (mIU/ml) LH (mIU/ml) LH/FSH T (ng/ml) PSV (cm/s) PI RI
Before operation 6.42 T 1.85 16.86 T 4.53 2.67 T 0.55 1.18 T 0.32 14.04 T 6.82 0.98 T 0.36 0.55 T 0.16610 weeks after operation 7.55 T 1.98 11.7 T 4.82 1.59 T 0.65 0.72 T 0.28 12.49 T 6.32 1.78 T 0.72 0.71 T 0.1995% CI (Upper) 0.40 6.64 1.32 0.58 2.05 0.63 0.1195% CI (Lower) 1.84 3.65 0.82 0.34 1.04 0.98 0.21P-value 0.003* 0.001* 0.001* 0.001* 0.001* 0.001* 0.001*
*= Signicant P-value.
Table II. Correlation between hormonal and Doppler parameter changes after operation in women with PCOS undergoing ovarian diathermy
Doppler parameters D-PSV D-PI D-RI
P-value r P-value r P-value rHormonal proleD-FSH 0.37 0.14 0.24 D-LH 0.20 0.001 0.43 0.054* D-LH/FSH 0.06* 0.000 0.53 0.001 0.43D-T 0.13 0.003 0.40 0.04 0.30
r = Correlation coefcient.D = Differences between values before and 610 weeks after operation.*Borderline signicance.
Figure 2. Mean hormonal and Doppler parameter changes in PCOSwomen undergoing ovarian diathermy who ovulated after operation.* = Signicant differences of each variable (comparison of beforeand 610 weeks after operation) (P < 0.05).
M.E.Parsanezhad et al.
1434
-
7/30/2019 Hum. Reprod. 2003 Parsanezhad 1432 7
4/6
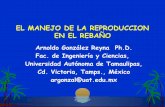
increase in RI was observed in women that ovulated after
operation (Figure 2). In post-operation analyses, the changes in
Doppler indices in women who did not ovulate were not
signicant when compared with their pre-operation values
(Figure 3). All variables (PSV, PI, RI, LH, FSH, testosterone,
age, progesterone, follicular size) had normal distribution.
Discussion
The results of this study demonstrate that ovarian stromal bloodow velocity declined after LOD in women with PCOS.
Hormonal alteration that occurred after LOD in our patients
was consistent with previous reports (Naether, 1993; Liguri
et al., 1996). The ovulation and pregnancy rate after LOD
varied from 2080% (Greenblatt and Casper, 1993; Tiitinen
et al., 1993; Donesky and Adashi, 1995). Our study had been
designed to evaluate the Doppler parameters of ovarian stroma
and hormonal prole including ovulation before and after
LOD. Thus long-term follow-up and pregnancy rate were not
considered. Colour Doppler ultrasound permits accurate non-
invasive assessment of blood ow to the reproductive organs. It
has been used for the assessment of uterine and ovarian blood
ow in normal cycles (Sladkevicius et al., 1993; Zaidi, 2000),PCOS (Ajossa et al., 2001; Zaidi et al., 1995; 1998; Zaidi,
2000), and after IVF attempts (Faver et al., 1993; Balakier and
Stronell et al., 1994). The vascular changes observed during
the entire folliculogenesis process seem to play an important
role in ovulation (Campbell et al., 1993; Sladkevicius et al.,
1993; Balakier et al., 1994; Dolz et al., 1999). Regarding this
point, some reports now exist in the literature arguing that
ovulation in humans depends on changes in blood ow to the
follicle and that the main blood supply to the Graaan follicle
is directed predominantly to a wreath of blood vessels that lie
along the inner border of theca interna (Macchiarelli et al.,
1995). Our study is the rst study in the literature to report a
signicant correlation between some Doppler indices and
hormonal changes including ovulation after ovarian diathermy
(Table II). In this study, we have demonstrated a dramatic fall
in ovarian blood ow in parallel with LH and testosterone
level, and LH/FSH ratio 610 weeks after surgery (Table I).
We were also able to show that PI signicantly decreased in
women who ovulated after ovarian diathermy. Althoughstatistically not signicant, in the adjusted analyses, RI
increased (P > 0.05) when measured 610 weeks after
operation in subjects that ovulated after the operation but
PSV showed no change.
The pathophysiology of abnormal ovarian blood ow in
PCOS is not clearly understood. One possible explanation is
that serum estradiol (E2) might have a role as the moderator of
uterine and ovarian vascularity (Steer et al., 1990; de Ziegler
et al., 1991; Zaidi, 2000). Greenblatt and Casper (1987)
showed a fall in E2 level starting the rst day after LOD,
reaching the minimum level by day 4 after operation and
beginning to rise thereafter. Thus the hypothesis of any
correlation between serum E2 levels and ovarian blood owchanges remains elusive. On the other hand, a signicant
decrease in vascular impedance to blood ow in the ovarian
artery (Deutinger et al., 1989), and in vessels around the
follicles, in correlation with an increase in the number of
follicles and serum E2 concentration (Weiner et al., 1993), was
observed after ovarian stimulation with gonadotrophins. As we
demonstrated, ovarian blood ow decreased starting on day 2
following the operation and remained low for at least 2 months.
Considering these observations and the data reported by Schurz
et al. (1993), it seems that some factors other than E2 could be
the cause of increased ovarian stromal vascularity in PCOS.
Dolz et al. (1999) suggested that different mechanisms may be
responsible for the haemodynamic anomalies that are uni-formly observed in patients who do not undergo the type of
luteal conversion occurring in normally cycling women. They
suggested that the abnormal haemodynamic patterns may be
due to an abnormal timing of LH-dependent prostaglandin
release. Bourne and co-workers (1991) described a direct
correlation between LH levels, prostaglandin activity and
blood ow changes in the ovary. An alteration in the nely
tuned timing for release of specic prostaglandins is likely to
interfere with ovulation in humans. Engmann et al. (1999b)
showed that ovarian stromal artery blood ow velocity declines
after short term (23 weeks) treatment with GnRH agonist and
increases signicantly on the day of hCG administration. The
decline in ovarian artery blood ow velocity after GnRHagonist therapy is unlikely to be due to a hypoestrogenic effect.
There is evidence that GnRH agonist therapy has a direct
inhibitory effect on granulosa and luteal cell function and may
play an important role in processes such as follicular atresia and
luteal regression (Sharpe et al., 1982); therefore the ovaries are
quiescent after GnRH agonist therapy. Primordial or smaller
preantral follicles do not have any special vascular supply of
their own and derive their blood supply from stromal blood
vessels (Findaly, 1986). Subsequent growth of primary follicles
leads to development of a vascular network with increased
Figure 3. Mean hormonal and Doppler parameter changes in PCOSwomen undergoing ovarian diathermy who did not ovulate after
operation. * = Signicant differences of each variable (comparisonof before and 610 weeks after operation) (P < 0.05).
Ovarian stromal blood ow changes
1435
-
7/30/2019 Hum. Reprod. 2003 Parsanezhad 1432 7
5/6
follicular blood ow. Thus the stromal blood ow velocity in an
inactive or quiescent ovary may reect the baseline blood ow
perfusion. Laparoscopic ovarian diathermy may result in the
reduction in the number of small and intermediate follicles that
usually seen in PCOS, it has the same effect on ovarian stromal
tissue (Naether, 1993; Liguri et al., 1996). Regarding these
effects and the above-mentioned mechanism by which ovarian
stromal blood ow declined after GnRH agonist therapy
(Findaly, 1986), we can hypothesize that the decline in ovarianstromal blood ow velocity could be the result of the direct
electrical and/or thermal effects of LOD. Considering the
increased ovarian stromal blood ow velocity in PCOS
(Battaglia et al., 1995; Zaidi etal., 1995) and its possible effects
on ovarian steroidogenesis, there might be a possible benecial
effect of diminished ovarian stromal blood ow velocity on
ovarian steroidogenesis in PCOS. Ourdata shed no light on these
possibilities since we did not measure E2 or prostaglandins and
no data regarding the direct effect of diminished ovarian stromal
blood ow on ovarian steroidogenesis is available. In this study,
we reported our preliminary ndings regarding the effects of
LOD on ovarian stromal blood ow. The results show that
Doppler indices of ovarian stromal blood ow signicantlychanged after LOD and these changes are signicantly correl-
ated with hormonal changes and subsequent ovulation. Our
results provide a potential new avenue for evaluation of ovarian
stromal blood ow changes after LOD. These data also suggest
that the measurement of ovarian stromal blood ow by colour
Doppler may be of value in predicting the prognosis of PCOS
related problems after LOD. However, we believe that further
research on a larger sample size is needed to determine whether
an interaction occurs between LOD, ovarian stromal blood ow
and ovarian steroidogenesis.
AcknowledgementsWe wish to thank Miss Marzieh Dehbozorgian for her help withstatistical analyses.
References
Agrawal, R., Sladkevicius, P., Engmann, L., Conway, G.S., Payne, N.N.,Bekis, J., Tan, S.L., Campbell, S. and Jacobs, H.S. (1998) Serum vascularendothelial growth factor concentrations and ovarian stromal blood ow areincreased in women with polycystic ovaries. Hum. Reprod., 13, 651655.
Ajossa, S., Guerriero, S., Paoletti, A.M., Orru, M., Floris, S., Mannias, M. andMelis, G.B. (2001) Uterine perfusion and hormonal pattern in patients withpolycystic ovary syndrome. J. Assist. Reprod. Genet., 18, 436440.
Aleem, F.A. and Predanic, M. (1996) Transvaginal colour Dopplerdetermination of the ovarian and uterine blood ow characteristics in
polycystic ovary syndrome. Fertil. Steril., 65, 510516.Al-Took, S., Watkin, K., Tulandi, T. and Tan, S.L. (1999) Ovarian stromal
echogenicity in women with Clomiphene citrate-sensitive and clomiphenecitrate-resistant polycystic ovary syndrome. Fertil. Steril., 71, 925954.
Balakier, H. and Stronell, R.D. (1994) Color Doppler assessment offolliculogenesis in in vitro fertilization patients.Fertil. Steril., 62, 12111216.
Battaglia, C., Artini, P.G., D'Ambrogio,V D'G., Genazzani, A.D. andGenazzani, A.R. (1995) The role of color Doppler imaging in the diagnosisof polycystic ovary syndrome. Am. J. Obstet. Gynecol., 172, 108113.
Battaglia, C., Artini, P.G. and Genazzani, A.D. (1997) Color doppler analysisin oligo- and ammenorrheic women with polycystic ovary syndrome.Gynecol. Endocrinol., 11, 105110
Bourne, T.H., Reynolds, K., Waterstone, J., Okokon, E., Jurkovic, D. andCambell, S. (1991) Paracetamol-associated luteinized unruptured follicle
syndrome: effects on intrafollicular blood ow. Ultrasound Obstet.Gynecol., 1, 420425.
Campbell, S., Bourne, T.H., Waterstone, J., Reynolds, K., Crayford, T.J.B.,Jurkovic, D., Kokon, E.V. and Collins, W.P. (1993) Transvaginal colourow imaging of the periovulatory follicle. Fertil. Steril., 60, 433438.
Cohen, J. (1996) Laparoscopic procedures for treatment of infertility related topolycystic ovarian syndrome. Hum. Reprod. Update, 2, 337344.
Collins, W., Jurkovic, D., Bourne, T., Kurjak, A. and Campbell, S. (1991)Ovarian morphology, endocrine function, and Intrafollicular blood owduring the peri-ovulatory period. Hum. Reprod., 6, 319324.
Deutinger, J., Reinthaller, A. and Bernaschek, G. (1989) Transvaginal
pulsed Doppler measurement of blood ow velocity in the ovarianarteries during cycle stimulation and after follicle puncture. Fertil. Steril.,51, 466470.
de Ziegler, D., Bessis, R. and Frydman, R. (1991) Vascular resistance ofuterine arteries: physiological effects of estradiol and progesterone. Fertil.Steril., 55, 775779.
Dolz, M., Osborne, N.G., Balnes, J., Raga, F., Abad-Velasco, L., Villalobos,A., Pellicer, A. and Bonilla-Musoles, F. (1999) Polycystic ovary syndrome:Assessment with colour Doppler angiography and three-dimensionalultrasonography. J. Ultrasound Med., 18, 303313.
Donesky, B.W. and Adashi, E.Y. (1995) Surgically induced ovulation in in thepolycystic ovary syndrome:Wedge resection revisited in the age oflaparoscoy. Fertil. Steril., 63, 439462.
Engmann, L., Sladkevicius, P., Agrawal, R., Bekir, J., Campbell, S. and Tan,S.L. (1999a) The pattern of changes in ovarian stromal and uterine arteryblood ow velocities during IVF treatment and its relationship with
outcome of the cycle. Ultrasound Obstet. Gynecol., 13, 2633.Engmann, L., Sladkevicius, P., Agrawal, R., Bekir, J., Campbell, S and Tan,
S.L. (1999b) The value of ovarian stromal blood ow velocity measurementafter pituitary suppression in the prediction of ovarian responsiveness andoutcome of IVF treatment. Fertil. Steril., 71, 2229.
Faver, R., Bettahar, K., Grange, G., Ohl, J., Arbogast, E. and Moreau, L.(1993) Predictive value of transvaginal uterine Doppler assessment in anin vitro fertilization program. Ultrasound Obstet. Gynecol., 3, 350353.
Felemban, A., Tan, S.L. and Tulandi, T. (2000) Laparoscopic treatment ofpolycystic ovaries with insulated needle cautery: a reappraisal. Fertil.Steril., 73, 266269.
Findaly, J.K. (1986) Angiogenesis in reproductive tissue. J. Endocrinol., 111,357366.
Greenblatt, E.M. and Casper, R.F. (1987) Endocrine changes afterlaparoscopic ovarian cautery in polycystic ovarian syndrome. Am. J.Obstet. Gynecol., 156, 279285.
Greenblatt, E.M. and Casper, R.F. (1993) Adhesion formation afterlaparoscopic ovarian cautery For polycystic ovarian syndrome: lack ofcorrelation with pregnancy rate. Fertil. Steril., 60, 766770.
Kelestimur, F., Unluhizarci, K., Bayram, F., Sahin, Y. and Tutus, A. (2000)Metformin and polycystic ovary syndrome. J. Clin. Endocrinol. (Oxf), 52,244246.
Liguri, G., Tolino, A., Moccia, G., Scognamiglio, G. and Nappi, C. (1996)Laparoscopic ovarian treatment in infertile patients with polycystic ovariansyndrome (PCOS): endocrine changes and clinical outcome. Gynecol.Endocrinol., 10, 257264.
Macchiarelli, G., Nottola, S.A., Vizza, E., Correr, S. and Motta, P.M. (1995)Changes of ovarian microvasculature in hCG stimulated rabbits. A scanningelectron microscopic study of corrosion casts. Ital. J. Anat. Embryol., 100,(Suppl, 1), 469477.
Naether, O.G.J., Fischer, R., Weise, H.C., Geiger-Kotzler, L., Delfs, T. andRudolf, K. (1993) Laparoscopic electrocoagulation of the ovarian surface ininfertile patients with polycystic ovarian disease. Fertil. Steril., 60, 8894.
Schurz, B., Schon, H.J., Wenzl, R.E., Huber, J. and Reinold, E. (1993)Endovaginal Doppler ow measurements of the ovarian artery in patientswith a normal menstrual cycle and with polycystic ovary syndrome duringin vitro fertilization. J. Clin. Ultrasound, 21, 1924.
Sharpe, R.M. (1982) Cellular aspects of the inhibitory actions of LH-RH onthe ovary and testis. J. Reprod. Fertil., 64, 517527.
Sladkevicius, P., Valentin, L. and Larsal, K. (1993) Blood ow in the ovarianand uterine arteries during the normal menstrual cycle. Ultrasound Obstet.Gynecol., 3, 199208.
Speroff, L., Glass, R.H. and Kase, N.G. (1999) Anovulation and the polycysticovary syndrome. In Clinical Gynecologic Endocrinology and Infertility. 6thedn, Williams and Wilkins. Co, Baltimore, Maryland, USA. pp 487521,1105.
Steer, C.V., Campbell, S., Pampiglione, J.S., Kingsland, C.R., Mason, B.A.
M.E.Parsanezhad et al.
1436
-
7/30/2019 Hum. Reprod. 2003 Parsanezhad 1432 7
6/6
and Collins, W.P. (1990) Transvaginal colour ow imaging of theuterine arteries during the ovarian and menstrual cycles. Hum. Reprod., 5,391395.
Tiitinen, A., Tenhunen, A. and Seppala, M. (1993) Ovarianelectrocauterization causes LH-regulated not insulin-regulated endocrinechanges. Clin. Endocrinol. (Oxf), 39, 181184.
Tulandi, T., Watkin, K. and Tan, S.L. (1997) Reproductive performance andthree-dimensional ultrasound volume determination of polycystic ovariesfollowing laparoscopic ovarian drilling. Int. J. Fertil., 42, 436440.
Vralacnik-Bokal, E. and Meden-Vrtovec, H. (1998) Utero-ovarian arterialblood ow and hormonal prole in patients with polycystic ovary
syndrome. Hum. Reprod., 13, 815821.Weiner, Z., Thaler, I., Levron, J., Lewit, N. and Itskovitz-Eldor, J. (1993)
Assessment of ovarian and uterine blood ow by transvaginal colour
Doppler in ovarian-stimulated women: correlation with the number offollicles and steroid hormone levels. Fertil. Steril., 59, 743749.
Zaidi,J. (2000) Bloodow changes in theovarianand uterine arteriesin womenwith normal and polycystic ovaries. Hum. Fertil. (Camb.), 3, 194198.
Zaidi, J., Campbell, S., Pittrof, R., Kyei-Mensah, A., Shaker, A., Jacobs, H.S.and Tan, S.L. (1995) Ovarian stromal blood ow changes in women withpolycystic ovaries. A possible new marker for ultrasound diagnosis? Hum.
Reprod., 10, 19921996.
Zaidi, J., Jacobs, H.S., Campbell, S. and Tan S.L. (1998) Blood ow changesin the ovarian and uterine arteries in women with polycystic ovarysyndrome who respond to clomiphene citrate: correlation with serum
hormone concentrations. Ultrasound Obstet. Gynecol., 12, 188196.
Submitted on December 5, 2002; accepted on February 21, 2003
Ovarian stromal blood ow changes
1437