Hoarding disorder
30
Hoarding disorder
-
Upload
harsh-shah -
Category
Health & Medicine
-
view
1.026 -
download
0
Transcript of Hoarding disorder
Hoarding
disorder
“It is clear that between what a man calls me and what he
simply calls mine, the line is difficult to draw. We feel and act
about certain things that are ours very much as we feel and
act about ourselves.”
-William James
CONFUSION REGARDING OCD
AND HOARDING DISORDER
• Although hoarding is often considered a symptom of obsessive–
compulsive disorder (OCD), and is included in most structured
interviews and questionnaires of OCD symptoms, it is not directly
mentioned in DSM-IV-TR or in ICD-10 as a typical symptom of OCD.
• This can be confusing as clinicians may struggle deciding when a
diagnosis of OCD is appropriate, particularly when hoarding
appears in the absence of other prototypical OCD symptoms.
Depression and Anxiety 0:1–17, 2010.
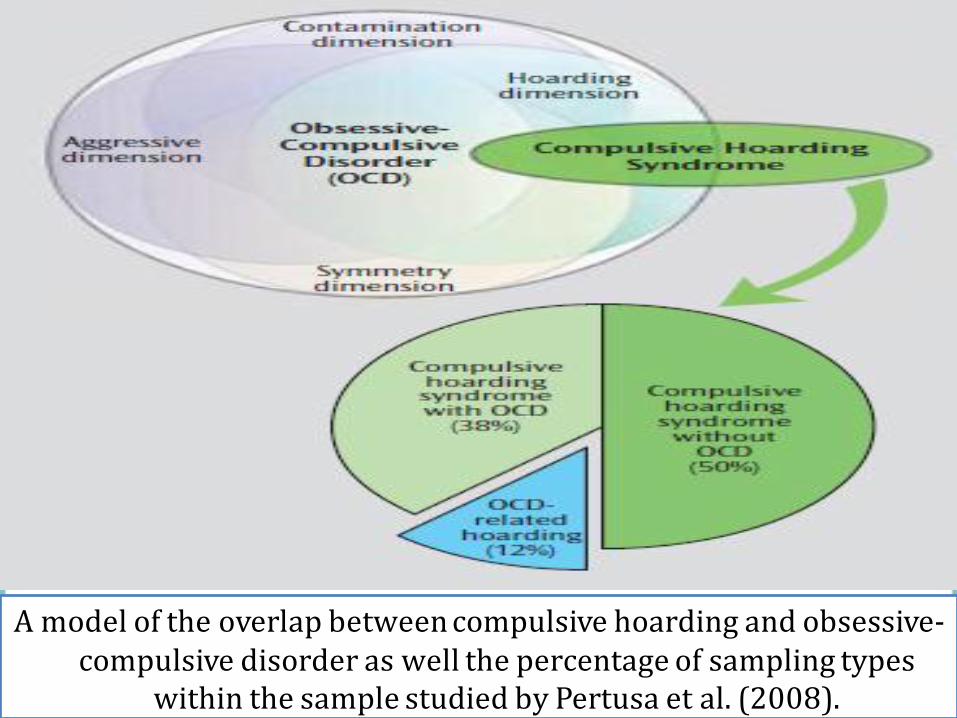
A model of the overlap between compulsive hoarding and obsessive-compulsive disorder as well the percentage of sampling types
within the sample studied by Pertusa et al. (2008).
Past and current
scenario
• Bratiotis et al. (2011) noted that published articles about
hoarding have increased approximately four-fold since
Frost and Hartl’s (1996) definitive work in which they
defined and operationalized research on compulsive
hoarding.
• Thanks to this upsurge in attention, there is now critical
information regarding the scope of the problem as well as the
consequences involved.
Epidemiology
• Current estimates indicate that 14% of the population will
engage in hoarding behaviors sometime in the life course
• Point prevalence studies indicate clinically significant
compulsive hoarding occurs in 1.5% to 4.6% of the
population comparable to other major psychiatric conditions,
and greater than the prevalence of OCD (1.2%)
Molecular Psychiatry, 2010:15(1), 53-63.
WHAT IS IT?
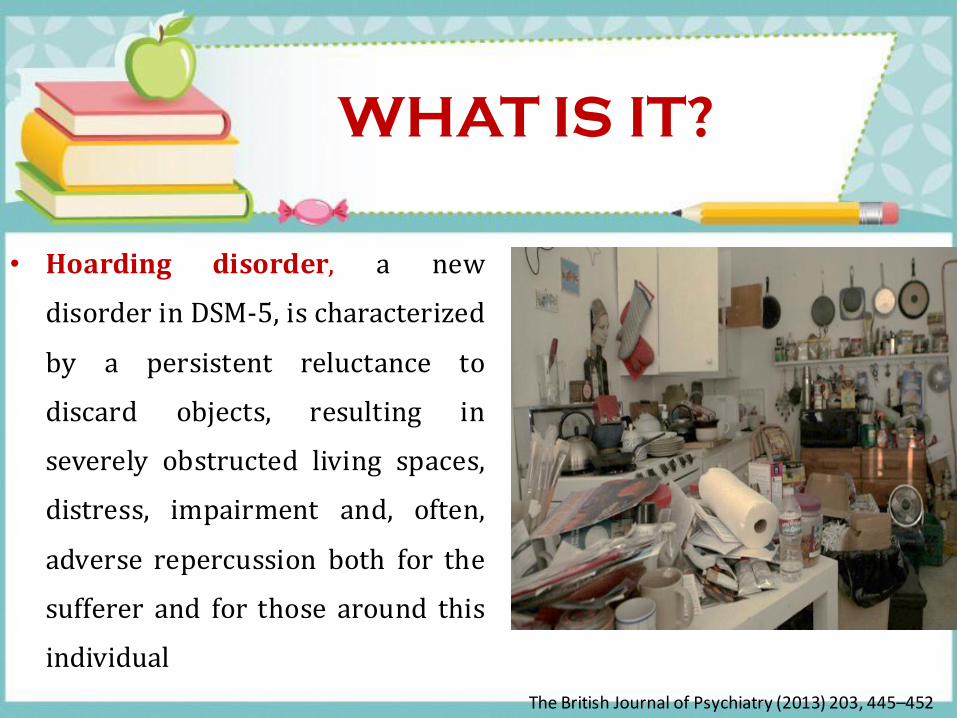
• Hoarding disorder, a new
disorder in DSM-5, is characterized
by a persistent reluctance to
discard objects, resulting in
severely obstructed living spaces,
distress, impairment and, often,
adverse repercussion both for the
sufferer and for those around this
individual
The British Journal of Psychiatry (2013) 203, 445–452
HOARDING
• Hoarding is not the same as collecting; collectors look for
specific items, such stamps, and may organize or display them.
• People with hoarding disorder often save random items and
store them haphazardly
• In most cases, people save items that they feel they may need
in the future, are valuable, or have sentimental value; some
may also feel safer surrounded by the things they save.
American Psychiatric Association www.psychiatry.org
CLINICAL
DEFINITION
Hoarding behaviour is, in fact, quite common but problematic hoarding
consists of three components:
• The acquisition of and failure to discard possessions that appear to
be of little use or value
• Living spaces sufficiently cluttered so as to preclude activities for
which those spaces were designed
• Significant distress or impairment in functioning caused by the
hoarding
Frost & Steketee, 1999


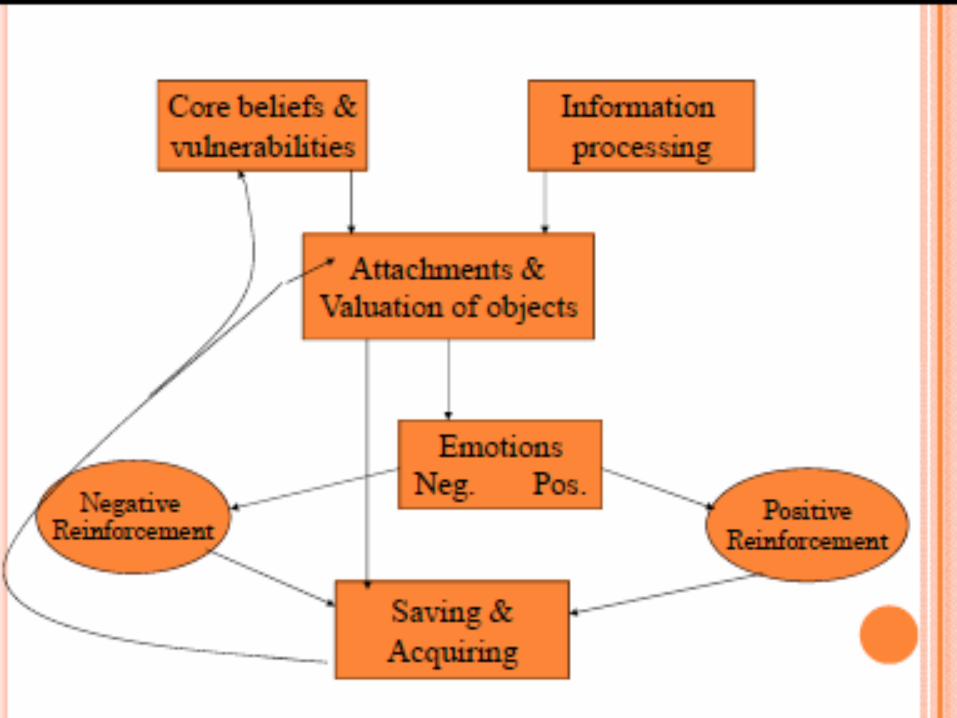
REASONS FOR SAVING
• Sentimental – “This represents my life. It’s part of me.”
• Instrumental – “I might need this. Somebody could use this.”
• Intrinsic – “This is beautiful. Think of the possibilities!”
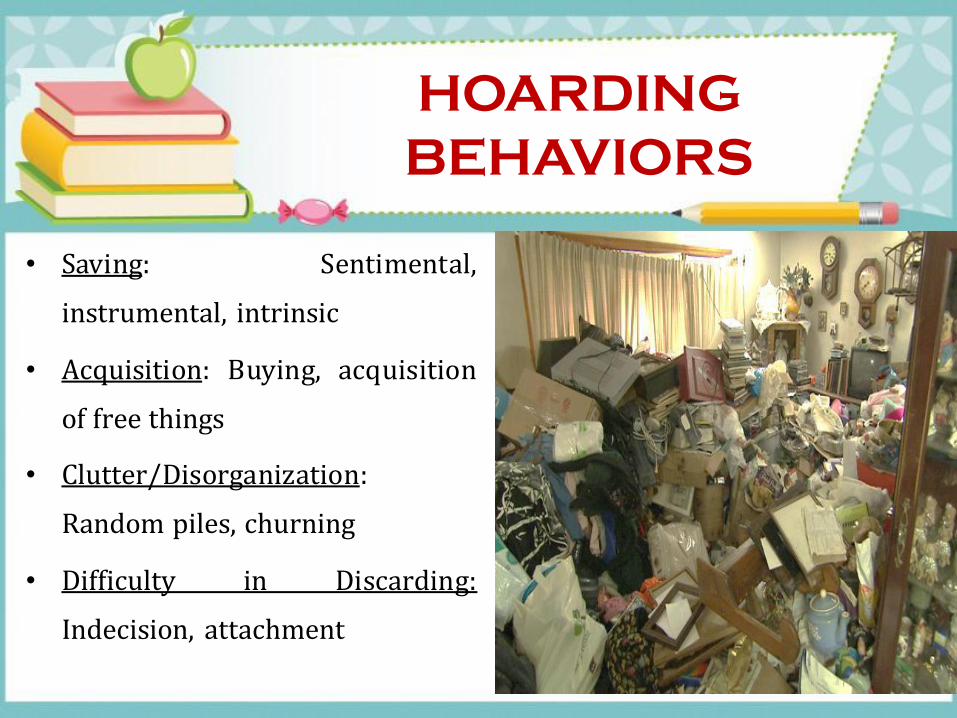
HOARDING
BEHAVIORS
• Saving: Sentimental,
instrumental, intrinsic
• Acquisition: Buying, acquisition
of free things
• Clutter/Disorganization:
Random piles, churning
• Difficulty in Discarding:
Indecision, attachment
March 2012 Satwant Singh
Manifestation of
hoarding
• Usually begins in childhood- long standing
• Compulsive acquisition
• Lack of organisation
• Saving behaviours and inability to discard
• Avoidance- dealing with the problem, others
• Trust issues- letting others help
• Lack of insight/acceptance of problem e.g. the place is too
small, I don’t have time to organise
consequences
• Impairment and distress to the individual
• Impairment to social functioning and relationship issues, social
isolation
• Health and safety- fire hazard, infestation, poor living conditions
(lack of heating etc), hazard to the environment e.g. building
with the lack of poor maintenance
• Mental health issues e.g. depression, psychosis etc
March 2012 Satwant Singh
REASONS FOR
HOARDING
• Usually begins in childhood, more common in males
• Family history of hoarding and OCD
• Often linked to some sort of trauma e.g. loss, abuse, divorce etc
• Material deprivation
• Severe and enduring mental illness and other mental health
problems
As noted by prominent researchers Frost and Steketee (2010)
in their recent book on compulsive hoarding,
“The boundaries between normal and abnormal blur when
it comes to hoarding. We all become attached to our
possessions and save things other people wouldn’t. So we all
share some of the hoarding orientation”
SIMILARITIES AND
DIFFERENCES
Hoarders and non hoarders save the same things but the
differences are:
- Quantity
- Emotional attachments (sentimental)
- Perceived use of object (instrumental)
- Over valued beliefs
- The object as an extension of self
March 2012 Satwant Singh
Understanding of
condition
Different from OCD and other conditions as:
• Do not view their behaviour as unusual
• Less insight into their behaviour
• Have reasons why they need to “save” “I need this just in
case” “It reminds me of marriage, good times in my life”
HOARDING ASSESSMENT
SCALES
• UCLA Hoarding Severity Scale (Saxena et al, 2007)
• Saving Inventory-revised (Frost et al, 2004)
• Hoarding Rating Scale-Interview (Tolin et al, 2010)
American Psychiatric Association www.psychiatry.org
DIAGNOSING
HOARDING DISORDER
An assessment for hoarding may include questions such as
• Do you have trouble discarding things that most other people
would get rid of?
• Because of the clutter or number of possessions, how difficult is
it to use the rooms and surfaces in your home?
• To what extent do you buy items or acquire free things that you
do not need or have enough space for?
American Psychiatric Association www.psychiatry.org
DIAGNOSING
HOARDING DISORDER
• To what extent do your hoarding, saving, acquisition, and clutter
affect your daily functioning?
• How much do these symptoms interfere with school, work, or
social or family life?
• How much distress do these symptoms cause you?
American Psychiatric Association www.psychiatry.org
MANAGEMENT OPTION
• Cognitive-behavioral therapy (CBT)
• Medication
American Psychiatric Association www.psychiatry.org
INEFFECTIVE
INTERVENTION
STRATEGIES
Make decisions (about a plan of action) for a tenant
Argue or Persuade
Pressure the tenant to discard
Tell the tenant how to feel
Give verbal and non-verbal cues that are judgmental or
negative in nature
EFFECTIVE INTERVENTION
STRATEGIES
Be clear about expectations and limitations
Ask open-ended questions
Reflectively listen
Use respectful, non-judgmental language
Mirror the language used by the tenant
“Work with” the tenant instead of “doing for”
• During CBT, individuals gradually learn to discard unnecessary
possessions with less distress, diminishing their exaggerated
perceived need or desire to save for these possessions.
• They also learn to improve skills such as organization, decision-
making, and relaxation.
• For many people, certain anti-depressant medications may be
helpful and may produce more rapid improvement American Psychiatric Association www.psychiatry.org

Thank you