Histological Study of the Normal Vertebral Artery
8
629 Received April 19, 2004; Accepted August 9, 2004 629 Neurol Med Chir (Tokyo) 44, 629¿636, 2004 Histological Study of the Normal Vertebral Artery —Etiology of Dissecting Aneurysms— Taku SATO, Tatsuya SASAKI, Kyouichi SUZUKI, Masato MATSUMOTO, Namio KODAMA, and Kouichi HIRAIWA* Departments of Neurosurgery and *Legal Medicine, Fukushima Medical University, Fukushima Abstract Histological evaluation of dissecting aneurysms of the cerebral arteries has suggested that defects in the internal elastic lamina (IEL) induce dissection of the arterial wall. Dissecting aneurysms occur most frequently in the vertebral artery (VA). The present study examined sections of the normal VA to elucidate the mechanisms of arterial dissection. Bilateral VAs (20 vessels) were obtained from 10 patients who died of causes other than intracranial lesions. The VAs were detached from the VA union to the site 10 mm proximal from the point penetrating the dura mater. The VAs were cut at 5-mm inter- vals, and each segment was observed using modified Masson's trichrome staining for elastic fibers. The thickness of the media and adventitia significantly thinned after the origin of the posterior inferior cerebellar artery (PICA). IEL defects were observed at 35 sites in 11 vessels from six subjects. There was a high incidence of IEL defects in the extradural portion and near the origin of the PICA, areas frequent- ly involved in arterial dissection. There was a high incidence of intimal thinning at areas of IEL defects (19 of 35), and thinning was particularly marked distal to the origin of the PICA. In the absence of intimal thickening, the vascular strength at the site of IEL defects may be reduced, which would promote the occurrence and progression of arterial dissection. Key words: histology, vertebral artery, dissecting aneurysm, elastic lamina Introduction Advances in imaging techniques have led to an increase in the detection of intracranial dissecting aneurysms. Dissecting aneurysms of the carotid artery system often result in cerebral infarction due to arterial stenosis or obstruction. Dissection of the vertebral artery (VA) system often leads to subarachnoid hemorrhage with high rebleeding rate and mortality. 1,3,14,27) Slight injury due to neck exercise or chiropractic manipulation 9,22) may cause VA dissection. Arteriosclerosis, fibromuscular dysplasia, 2,19) and degeneration of the media may be related to arterial dissection. Extracranial dissection of the VA occurs most frequently at the C1–2 levels of the spine, 22) whereas intracranial dissections are often located near the origin of the posterior inferior cerebellar artery (PICA). 10,18,26) Minimal neck injury has been suggested as a cause of dissecting aneurysms at the C1–2 levels, 22) but the preferential occurrence near the origin of the PICA remains to be elucidated. The etiology and pathology of dissecting aneurysms of the cerebral arteries remain largely unknown. The internal elastic lamina (IEL) is the strongest structure in the arterial wall and IEL defects may be a primary factor in intimal rup- ture. 15,16) Histological evaluation of dissecting aneurysms of the cerebral arteries has suggested that defects in the IEL or media, or degeneration of the media induce intimal changes, and rupture of the intima results in dissection of the arterial wall. 1,4,6,7,15,17–21) Other dissections were attributed to rupture of the vasa vasorum or a newly formed ves- sel in the vascular wall associated with degeneration of the media. 5,28) The intima and IEL at the opening of a dissection are washed away by blood, so preventing histological investigation. Dissecting aneurysms occur most frequently in the VA, 25) but few histological investigations of the normal VA have investigated the underlying etiologic mechan- isms. In particular, the thickness of the wall of the cervical and intracranial VA near the dura mater 12,24) and the presence of IEL defects are not well charac- terized. The present histological evaluation of the vascular
Transcript of Histological Study of the Normal Vertebral Artery

629
Received April 19, 2004; Accepted August 9, 2004
629
Neurol Med Chir (Tokyo) 44, 629¿636, 2004
Histological Study of the Normal Vertebral Artery
—Etiology of Dissecting Aneurysms—
Taku SATO, Tatsuya SASAKI, Kyouichi SUZUKI, Masato MATSUMOTO,Namio KODAMA, and Kouichi HIRAIWA*
Departments of Neurosurgery and *Legal Medicine, Fukushima Medical University, Fukushima
Abstract
Histological evaluation of dissecting aneurysms of the cerebral arteries has suggested that defects in theinternal elastic lamina (IEL) induce dissection of the arterial wall. Dissecting aneurysms occur mostfrequently in the vertebral artery (VA). The present study examined sections of the normal VA toelucidate the mechanisms of arterial dissection. Bilateral VAs (20 vessels) were obtained from 10patients who died of causes other than intracranial lesions. The VAs were detached from the VA unionto the site 10 mm proximal from the point penetrating the dura mater. The VAs were cut at 5-mm inter-vals, and each segment was observed using modified Masson's trichrome staining for elastic fibers. Thethickness of the media and adventitia significantly thinned after the origin of the posterior inferiorcerebellar artery (PICA). IEL defects were observed at 35 sites in 11 vessels from six subjects. There wasa high incidence of IEL defects in the extradural portion and near the origin of the PICA, areas frequent-ly involved in arterial dissection. There was a high incidence of intimal thinning at areas of IEL defects(19 of 35), and thinning was particularly marked distal to the origin of the PICA. In the absence ofintimal thickening, the vascular strength at the site of IEL defects may be reduced, which wouldpromote the occurrence and progression of arterial dissection.
Key words: histology, vertebral artery, dissecting aneurysm, elastic lamina
Introduction
Advances in imaging techniques have led to anincrease in the detection of intracranial dissectinganeurysms. Dissecting aneurysms of the carotidartery system often result in cerebral infarction dueto arterial stenosis or obstruction. Dissection ofthe vertebral artery (VA) system often leads tosubarachnoid hemorrhage with high rebleedingrate and mortality.1,3,14,27) Slight injury due to neckexercise or chiropractic manipulation9,22) may causeVA dissection. Arteriosclerosis, fibromusculardysplasia,2,19) and degeneration of the media may berelated to arterial dissection. Extracranial dissectionof the VA occurs most frequently at the C1–2 levelsof the spine,22) whereas intracranial dissections areoften located near the origin of the posterior inferiorcerebellar artery (PICA).10,18,26) Minimal neck injuryhas been suggested as a cause of dissectinganeurysms at the C1–2 levels,22) but the preferentialoccurrence near the origin of the PICA remains tobe elucidated.
The etiology and pathology of dissectinganeurysms of the cerebral arteries remain largelyunknown. The internal elastic lamina (IEL) is thestrongest structure in the arterial wall and IELdefects may be a primary factor in intimal rup-ture.15,16) Histological evaluation of dissectinganeurysms of the cerebral arteries has suggestedthat defects in the IEL or media, or degeneration ofthe media induce intimal changes, and rupture ofthe intima results in dissection of the arterialwall.1,4,6,7,15,17–21) Other dissections were attributed torupture of the vasa vasorum or a newly formed ves-sel in the vascular wall associated with degenerationof the media.5,28) The intima and IEL at the openingof a dissection are washed away by blood, sopreventing histological investigation. Dissectinganeurysms occur most frequently in the VA,25) butfew histological investigations of the normal VAhave investigated the underlying etiologic mechan-isms. In particular, the thickness of the wall of thecervical and intracranial VA near the dura mater12,24)
and the presence of IEL defects are not well charac-terized.
The present histological evaluation of the vascular

630
Table 1 Summary of cases
CaseNo.
Age(yrs) Sex Cause of death
1 0.7 M sudden infant death syndrome2 27 M alcoholism3 28 F pulmonary infarction4 35 M bleeding due to injury of the
jugular vein5 51 M rupture of the thoracic aorta6 52 M heart failure7 64 F bleeding due to liver laceration8 67 M heart failure9 67 M hypothermia
10 92 F heart failure
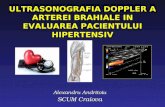
Fig. 1 Schematic drawing of the vertebral arteryspecimens. The point 10 mm toward theheart from the site where the vessel pene-trates the dura mater (dura) was defined asA, the point 5 mm distal to A as B, and thesite of penetration of the dura mater as C.Points D–J are at 5-mm intervals from pointC in the intradural portion. Serial sections4 mm in thickness (n= 20) were prepared atpoints A–J. PICA: posterior inferiorcerebellar artery.
630
Neurol Med Chir (Tokyo) 44, December, 2004
T. Sato et al.
structure of the normal VA measured the thicknessof the three-layer structure in the apparently normalVA and studied the distribution of the IEL and thecondition of the intima at IEL defects to clarify theetiology and pathology of dissecting aneurysms ofthe cerebral artery.
Materials and Methods
Bilateral VAs (20 vessels) were obtained from 10patients, aged 8 months to 92 years, who died ofcauses other than intracranial lesions and under-went legal autopsy at our hospital (Table 1). Thebilateral VAs were detached intradurally from theunion (origin of the basilar artery) retrogradely towhere the VA penetrated the dura mater, and wereresected extradurally en bloc from where the VApenetrated the dura mater to 10 mm toward theheart.
Detached VAs were cut at 5-mm intervals, andeach segment was fixed in formalin and embeddedin paraffin. The point 10 mm toward the heart fromthe site where the VA penetrated the dura mater wasdefined as A, the point 5 mm distal to A as B, and thesite of penetration of the dura mater as C. Points D–Jwere assigned at 5-mm intervals from point C(Fig. 1). Twenty 4 mm-thick sections were preparedat points A–J and stained for elastic fibers usingmodified Masson's trichrome staining for examina-tion under a light microscope. Due to variations inthe length of the VAs among the 10 subjects, sixblocks were prepared in two vessels, seven blocks inone vessel, eight blocks in 11 vessels, nine blocks inthree vessels, and 10 blocks in three vessels. Theventral aspect of the cross-section of the artery wasmarked with India ink at harvest. The surface of thebasilar artery which came into contact with thebrainstem was regarded as the dorsal aspect. The
ventral, lateral, dorsal, and medial aspects of thevascular cross-sections were labeled a, b, c, and d tofacilitate orientation of each specimen. Since thepresence of the PICA, which usually branches firstfrom the intracranial VA, might affect the measure-ment results, the presence and the position of thebranching of the PICA relative to point C wererecorded.
The thicknesses of the intima (from the surface ofthe endothelial cells to the external aspect of theIEL), the media (thickness of smooth muscle fibers),and the adventitia (thickness of elastic fibers andcollagen fibers) were measured in aspects a, b, c, andd at points A to J in the 20 vessels. The mean value ofthe four aspects was calculated for each layer atpoints A–J. Since the length of the VA in the infant(Case 1) differed greatly from the adult cases,measurements were made only at points where therewas clear correspondence with adult VAs (e.g. pointC).
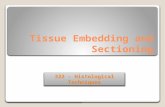
IEL defects with lengths of 25 mm or longer, whichwere detectable by light microscopy, were regardedas defects (Fig. 2), and the frequency was comparedat points A–J and aspects a–d in the 10 subjects. Thethickness of the intima at each IEL defect was deter-

631
Fig. 2 Photomicrograph showing a defect (aster-isk) in the internal elastic lamina. Defects25 mm or longer that were detectable by lightmicroscopy were considered defects. Mo-dified Masson's trichrome stain for elasticfibers, ×25.
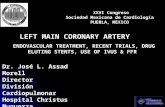
Fig. 3 Thicknesses of the intima (△), media (),and adventitia () of the 20 vertebralarteries. Values are mean± standarderror. PICA: posterior inferior cerebellarartery.
631
Neurol Med Chir (Tokyo) 44, December, 2004
Histology of the Normal VA
mined as the mean longitudinal diameter by divid-ing the area of the defect by its transverse diameter.The intimal area was measured using area-calculat-ing software (Scion Image; Scion Corp., Frederick,Md., U.S.A.). The intimal area was used because thethickness of the intima sometimes varied widelybetween the start and the end of the IEL defect, sothe mean longitudinal diameter yielded a moreaccurate representation. The degree of thickening ofthe intima at each IEL defect was calculated bydividing the thickness of the intima at the defect bythe thickness of the normal intima, which wasdetermined in advance as the reference value.
The values are shown as mean± standard error.Analysis of variance (Scheffe's post-hoc test) wasperformed at the p º 0.05 level of significance forcomparisons between sites.
Results
The PICA originated at the VA between points F andG in 17 of the 18 specimens from the nine adults.The mean distance from point C to the origin of thePICA was 15.9± 2.0 mm (range 0–33 mm).
The thickness of the intima, media, and adventitiaof the 20 VAs is shown in Fig. 3. There was no sig-nificant difference in the thickness of the intima ataspects a–d. The mean intimal thickness of the fouraspects was 60 mm or less at, or proximal to, point C,85 mm or more at points D–F, and 65 mm or less atpoint G. The thickness of the intima did not differsignificantly at any of the points of measurement.The thickness of the media was not significantlydifferent at aspects a–d. The thickness of the media
was greatest (253± 10 mm) at point B and decreasedmost sharply after point C, reducing to 192± 10 mmat point D. More distally, the thickness decreasedmore gradually. The media was significantly thinnerat point G than point B. The thickness of the adven-titia showed no significant differences at aspectsa–d. The thickness of the adventitia was greatest(247± 52 mm) at point C, decreased after point C to128± 11 mm at point D, and thinned more graduallyfurther distally. The adventitia was significantlythinner at points G–I than point A or B, at points E–Jthan point C, and at points F–I than point D.
IEL defects were observed at 35 sites in 11 vesselsfrom six subjects aged 51 years or older (Table 2),but not in the four subjects aged 35 years or younger.Case 10, a 92-year- old woman, had IEL defects at 14sites (Fig. 4 upper). The distribution of the defectsshowed 11 at point A or B, and 17 at point E, F, or G(Fig. 4 lower). Defects were located at aspects a and

632
Table 2 Degree of intimal thickening at the defectin the internal elastic lamina
CaseNo. Site Length of defect
(mm) Intimal thickness
5 A 86 1.77A 432 3.71B 1008 2.88B 864 1.22B 860 1.15B 140 0.99F 886 0.42G 234 0.08G 878 0.59
6 E 26 0.60G 52 0.40
7 C 650 0.71E 231 9.28G 286 0.60G 246 0.69
8 A 300 3.91E 60 1.99F 2100 2.05
9 E 169 0.43G 64 1.05H 26 1.07
10 A 450 0.31A 1588 0.86A 600 0.76A 185 0.83D 618 0.58F 133 1.10F 1330 1.34F 106 0.87G 82 0.98G 80 0.42H 78 0.42H 80 0.53J 1025 1.51J 213 0.35
Fig. 4 Distribution of defects in the internal elasticlamina (lower) shown as dots at 35 sites in11 vessels from six subjects aged 51 years orolder (upper).
632
Neurol Med Chir (Tokyo) 44, December, 2004
T. Sato et al.
b in 10 sections, c in four sections, and d in 11sections. There was no significant difference in theregional distribution of these defects.
The degree of intimal thickening was less than 0.9,or the intima was thinner than normal (Fig. 5 upperleft), at 19 of the 35 IEL defects; 0.9–1.1, or nearly thesame as in normal vessels, at five defects; and muchgreater than 1.1, or marked (Fig. 5 lower), at 11defects (Table 2). The intima was thickened at five ofthe 10 extracranial sites (points A and B), and wasthicker than the intima of normal vessels at three of16 intracranial sites (points F–H).

633
Fig. 5 Photomicrographs showing defects (aster-isks) in the internal elastic lamina. Thedegree of intimal thickening was less than0.9 (upper left) and much greater than 1.1(lower). Modified Masson's trichromestain for elastic fibers, ×10 (upper right)and ×100 (upper left and lower).
633
Neurol Med Chir (Tokyo) 44, December, 2004
Histology of the Normal VA
Discussion
Histological examination of the VA 1 cm proximaland distal to the site of penetration of the dura materfound that the adventitia and media thinned toapproximately half the thickness after penetrationbut that the thickness of the intima and IELremained unchanged.24) Histological study of ninesites in the normal cervical VA and one site in theintracranial VA showed that the mean thickness ofthe intima at the 10 sites increased with age.12) Sincethe thickness of the media was relatively unchanged,the ratio of intimal:medial thickness was examinedand found to be 1:30–1:50 in young persons and 1:2in individuals by the age of 60 years. The media was
thinner intracranially than extradurally in the studypopulation, but the difference was not remarkableand few age-related changes were noted. The adven-titia was thicker intracranially, but measurementswere obtained at only one unidentified site of theintracranial VA.
The present study examined the VA from 10 mmproximal to the site of penetration of the dura materto the union of the intracranial VAs by serial section-ing at 5-mm intervals. The intima thickened afterpenetration of the dura mater and thinned after thebranching of the PICA. The media thinned afterpenetration of the dura mater and was particularlythin distal to the branching of the PICA. We alsofound that the adventitia was thicker than the mediajust after penetration of the dura mater and thinnedafter the branching of the PICA. We suggest that thehigh incidence of rupture and bleeding near thebranching of the PICA, regardless of the position ofthe opening of the dissection lumen, may be relatedto the observed medial and adventitial thinning atthis site.
Pathological study of a large number of autopsycases with VA dissecting aneurysms suggested thatvascular dissection is attributable to IEL rupture.15)
Elastin, a structural protein that provides strength tothe vascular wall, is scarcely present in the media oradventitia, but is concentrated in the IEL, which isconsidered to be the strongest structure of the vascu-lar wall.23) Ligation of major cerebral arteries ob-tained at autopsy at both edges and exposure to con-tinuous air flow pressure found that the artery withthe intima and IEL tolerated up to 600 mmHg.8) Apostmortem study of human radial arteries showedthat the IEL was a single- or multiple-layer structurein young individuals but was stretched, ruptured, orabsent in some areas in older persons.11)
The present study observed IEL defects at 35 sitesin 11 vessels from six subjects, all of whom wereaged 51 years or older. Although our study popula-tion was small and age varied widely, the resultssuggest that the incidence of IEL defects increaseswith age. Defects were located more frequentlybefore penetration of the dura mater, and near thebranching of the PICA at 10–20 mm distal to the siteof penetration of the dura mater. The high incidenceof defects in these areas coincides with clinicalobservations that the VA at the C1–2 levels of thespine appears to be particularly prone to dissectionand obstructive circulatory impairment followingmild trauma because of the mobility of the structuresin that region,22) and that dissecting VA aneurysmsfrequently occur and often bleed near the branchingof the PICA.10,18,26) We suggest that IEL defectsbefore penetration of the dura mater and near the

634634
Neurol Med Chir (Tokyo) 44, December, 2004
T. Sato et al.
branching of the PICA may be related to the develop-ment of dissection at these sites.
Experimental IEL defects in rabbit femoral arterywere repaired by local intimal thickening.13)
However, intimal thickening due to atherosclerosiscan also lead to IEL defects. In fact, we observedmarked intimal thickening at 11 of the 35 sites withIEL defects and usually thin intima at 19 sites. Histo-logical examination disclosed intimal thickeningand a few atherosclerotic changes such as macro-phage infiltration at most defective IEL sites. In-timal thickening was observed at extracranial sites(points A and B) but not at intracranial sites (pointsF–H) despite the high incidence of IEL defects. Thismay be attributable to differences in the blood flowin the VA. The VA leaves the intervertebral foramenof C-1, runs a transverse course, then curves nearlyperpendicularly, and finally follows an anteriorcourse. Since point A was located immediately afterthe perpendicular curve, the observed intimal thick-ening may be attributable to biological reactions inresponse to turbulence and eddy currents in theblood flow. On the other hand, intimal thinning atsites of IEL defects, such as points F–H, is indicativeof weakening of the vascular wall. An event such asintimal detachment may readily lead to arterial dis-section, rupture, and hemorrhage.
The thickness of the intima, media, and adventitiaof normal VAs showed characteristic regionalchanges from the extradural portion to the union ofthe bilateral VAs, and the media and adventitiasignificantly thinned after the branching of thePICA. Considering that rupture and bleeding occurfrequently at this site, thinning of the media andadventitia may be involved in the vulnerability ofthis area to rupture following vascular dissection. Ahigh incidence of IEL defects was found in theextradural portion and near the branching of thePICA in normal VAs, areas frequently involved inarterial dissection. There was a high incidence ofintimal thinning at areas of IEL defects (19 of 35),and thinning was particularly marked distal to thebranching of the PICA. The vascular strength at thesite of IEL defects may be reduced in the absence ofintimal thickening, and this may be a factor in theoccurrence and progression of arterial dissection.IEL defects with intimal thickening were morefrequent in the extracranial segment of the VA.Since the extracranial VA curves nearly perpendicu-larly twice immediately before penetration of thedura mater, intimal thickening at that site is a resultof biological reactions to marked blood flow turbu-lence and eddy currents.
Acknowledgments
We are grateful to Mr. Takeshi Itakura for technicalassistance.
References
1) Adams HP Jr, Aschenbrener CA, Kassell NF,Ansbacher L, Cornell SH: Intracranial hemorrhageproduced by spontaneous dissecting intracranialaneurysm. Arch Neurol 39: 773–776, 1982
2) Anson J, Crowell RM: Cervicocranial arterial dissec-tion. Neurosurgery 29: 89–96, 1991
3) Aoki N, Sakai T: Rebleeding from intracranial dis-secting aneurysm in the vertebral artery. Stroke 21:1628–1631, 1990
4) Berger MS, Wilson CB: Intracranial dissectinganeurysms of the posterior circulation. Report of sixcases and review of the literature. J Neurosurg 61:882–894, 1984
5) Endo S, Nishijima M, Nomura H, Takaku A, OkadaE: A pathological study of intracranial posteriorcirculation dissecting aneurysms with subarachnoidhemorrhage: Report of three autopsied cases andreview of the literature. Neurosurgery 33: 732–738,1993
6) Farrell MA, Gilbert JJ, Kaufmann JC: Fatal in-tracranial artery dissection: Clinical pathologicalcorrelation. J Neurol Neurosurg Psychiatry 48:126–129, 1985
7) Friedman AH, Drake CG: Subarachnoid hemorrhagefrom intracranial dissecting aneurysm. J Neurosurg60: 325–334, 1984
8) Glynn LE: Medial defects in the circle of Willis andtheir relation to aneurysm formation. J Pathol Bac-teriol 51: 213–222, 1940
9) Haldeman S, Kohlbeck FJ, McGregor M: Risk factorsand precipitating neck movements causing ver-tebrobasilar artery dissection after cervical traumaand spinal manipulation. Spine 24: 785–794, 1999
10) Hasue M, Fukuda A, Nakajima S, Fukushima C,Haraoka J, Ito H: [Treatment of dissecting vertebralaneurysms]. Surgery for Cerebral Stroke 21: 361–367,1993 (Jpn)
11) Iwao Z: [Pathological study of arteriosclerosis of theradial artery]. Nagasaki Igakkai Zasshi 36: 379–393,1961 (Jpn)
12) Johnson CP, Lawler W, Burns J: Use of histomorpho-metry in the assessment of fatal vertebral arterydissection. J Clin Pathol 46: 1000–1003, 1993
13) Mitchell GM, MaCann JJ, Rogers IW, Hickey MJ,Morrison WA, O'Brien BMC: A morphological studyof the long-term repair process in experimentallystretched but unruptured arteries and veins. Br JPlast Surg 49: 30–34, 2001
14) Mizutani T, Aruga T, Kirino T, Miki Y, Saito I,Tsuchida T: Recurrent subarachnoid hemorrhagefrom untreated ruptured vertebrobasilar dissectinganeurysm. Neurosurgery 36: 905–913, 1995

635635
Neurol Med Chir (Tokyo) 44, December, 2004
Histology of the Normal VA
15) Mizutani T, Kojima H, Asamoto S, Miki Y: Pathologi-cal mechanism and three-dimensional structure ofcerebral dissecting aneurysms. J Neurosurg 94:712–717, 2001
16) Mizutani T, Miki Y, Kojima H, Suzuki H: Proposedclassification of nonatherosclerotic cerebral fusiformand dissecting aneurysms. Neurosurgery 45: 253–260,1999
17) Nass R, Hays A, Chutorian A: Intracranial dissectinganeurysms in childhood. Stroke 13: 204–207, 1982
18) Ono J, Yamaura A, Kubota M, Hirai S, Miyata A:[Management of 42 patients with ruptured dissectinganeurysms in vertebrobasilar system. Significance ofrebleeding]. Surgery for Cerebral Stroke 24: 51–56,1996 (Jpn)
19) Pilz P, Hartjes HJ: Fibromuscular dysplasia andmultiple dissecting aneurysms of intracranial arte-ries. Stroke 7: 393–398, 1976
20) Sasaki O, Ogawa H, Koike T, Koizumi T, Tanaka R: Aclinicopathological study of dissecting aneurysms ofthe intracranial vertebral artery. J Neurosurg 75:874–882, 1991
21) Scott GE, Neubuerger KT, Denst J: Dissectinganeurysm of intracranial arteries. Neurology 10:22–27, 1960
22) Shimizu J, Nakagawa Y, Fuji Y, Nakase H, MannenT: [Wallenberg's syndrome due to vertebral arterydissection following minimal neck injury. Report oftwo cases]. Rinsho Shinkeigaku 32: 430–435, 1992(Jpn, with Eng abstract)
23) Stehbens WE: Pathology of the Cerebral BloodVessels. St Louis, CV Mosby, 1972, pp 60–97
24) Wilkinson IMS: The vertebral artery. Extracranialand intracranial structure. Arch Neurol 27: 392–396,1972
25) Yamaura A: Non traumatic intracranial arterialdissection. Natural history, diagnosis, and treatment.Contemp Neurosurg 16: 1–6, 1994
26) Yamaura A, Watanabe Y, Saeki N: Dissectinganeurysms of the intracranial vertebral artery. JNeurosurg 72: 183–187, 1990
27) Yasui T, Kishi H, Komiyama M, Iwai Y, Yamanaka K,Nishikawa M, Nakajima H, Morikawa T: [Rerupturemechanism of ruptured intracranial dissectinganeurysm in the vertebral artery following proximalocclusion]. No Shinkei Geka 28: 345–349, 2000 (Jpn,with Eng abstract)
28) Yonas H, Agamanolis D, Takaoka Y, White RJ:Dissecting intracranial aneurysms. Surg Neurol 8:407–415, 1977
Address reprint requests to: T. Sato, M.D., Department ofNeurosurgery, Fukushima Medical University, 1Hikarigaoka, Fukushima 960–1295, Japan.e-mail: tak-s@fmu.ac.jp
Commentary on this paper appears on the next page.

636636
Neurol Med Chir (Tokyo) 44, December, 2004
T. Sato et al.
Commentary
Sato et al. present an interesting histological evalua-tion of the vertebral artery wall in non-dissectedsubjects as an attempt to explain the most frequentsites of dissection in this artery. The extraduralportion of the vertebral artery and the portion of theartery located near the origin of the PICA were theprincipal sites of defects in the internal elastic lamina(IEL) observed in 55% of the vessels studied. Thesesites are involved frequently in vertebral artery dissec-tions, as pointed out by the authors. In 54% of thecases the defect zones in the IEL mentioned aboveappear concurrently with thinning of the intimallayer. These two alterations can determine reduced
strength of the arterial wall and a possible site thatwill promote the occurrence and progression of avertebral dissection. All the subjects with these altera-tions were aged over 50 years old, suggesting that theIEL defects increase with age. The IEL defect withintimal thickening observed in the extracranialportion of the VA can be a reparative mechanismreactive to the flow turbulence in the curves of thisartery at that level. This paper is an attractive effort toform an eventual explanation for the prevalence ofsome sites among others in VA dissections.
Jorge MURA, M.D., David ROJAS-ZALAZAR, M.D.,and Evandro de OLIVEIRA, M.D.
Instituto de Ci âencias Neurol áogicasS ãao Paulo, Brazil