Hand-sewn Bowel Anastomosis: The Only Correct Choice · Hand-sewn Bowel Anastomosis: The Only...
22
Hand-sewn Bowel Anastomosis: The Only Correct Choice Ashok Babu, M.D. Department of Surgery University of Colorado
Transcript of Hand-sewn Bowel Anastomosis: The Only Correct Choice · Hand-sewn Bowel Anastomosis: The Only...

Hand-sewn Bowel Anastomosis: The Only Correct Choice
Ashok Babu, M.D.Department of SurgeryUniversity of Colorado

Outline• History• Trial data in specific applications
– Colorectal– Ileocolic– Esophagogastric– Trauma
• Time efficiency• Cost efficiency
History• Sutureless anastomosis (compression)
– 1826: Donaus• Hand-sewn double layer
– 1882: Connel• Hand-sewn single layer
– 1887 Halsted, 1922 Schiassi, 1951 Gambee, 1975 Matheson
• Stapled– 1908—Hungary—Hultl– Early 1960’s—Moscow– Late 1960’s—USA—Ravitch
The Controversy

Colorectal—Meta-analysis
• 13 PRCT comparing handsewn vs stapled• No study independently showed significant
difference in leak rate, stricture, cancer recurrence, or mortality
MacRae et. al. Dis Colon Rectum 1998.
0.53-1.981.02Wound infection0.57-3.041.3Cancer rec.4.6-4915Tech Problem1.28-7.563.12Stricture0.55-2.931.27Mortality0.78-1.521.09LeakConf. IntervalOdds RatioComplication
ODDS RATIO LESS THAN 1 FAVORS STAPLED ANASTOMOSIS

Colorectal—Meta-analysis
• Cochrane Review—9 PRCT. 1233 patient– 622 stapled– 611 handsewn
• Indications included cancer, diverticulosis, prolapse
• Mostly EEA but some end to side
Lustosa et. al. Cochrane Database. 2001.
CISewnStapledComplicationNS7.1%6.3%LeakNS3.6%2.4%Mortality1.2%-8.1%
2%8%Stricture
NS4.3%5.9%Wound infection

Colorectal—Summary
• No difference between stapled vs. handsewn except for:– higher stricture and technical mishap rate in
stapled– Average of 8 minutes longer time for
handsewn (from one study)

Ileocolic• Very few trials• Largest PRMCT by Kracht et. al.• 440 patients—RADIOLOGIC leak detection• Randomized to side/side stapled (106) or 4
types of sutured– End to end interrupted/continuous (84/77)– End to side interrupted/continuous (82/91)
• 8.3% leak rate in all handsewn groups vs 3% stapled
• Not significant in subgroups
Kracht et. al. Int J Colorectal Dis. 1993

Ileocolic—Crohn’s
• Retrospective study• Wide lumen side to side stapled (69) compared
to Handsewn end to end (69)• Hypothesis: wide lumen leads to less stasis,
pressure, and ischemia resulting in lower leak, stricture , and recurrence rates
Munoz-Juarez. Dis Col Rectum. 2001
24% p=.0457%Recurrence
4% p=.01726%Stricture/fistula
Wide side/sideEnd to End

Ileocolic—Crohn’s
• Retrospective study• Wide lumen side to side stapled (71) compared
to Handsewn end to end (55)• Leak Rate 14.1% end to end vs 2% (p=0.02)
Resegotti. Dis Col Rectum. 2005.

Ileocolic—Summary
• These studies compare anastomoticconfiguration AND stapled vs. handsewntechnique simultaneously
• This makes the data uninterpretable

Esophagogastric anastomosis
• Meta-analysis 5 PRCT’s• Circular stapler vs. end-end hand-sewn• All patients underwent esophagectomy for
cancer and randomized to 2 techniques• No significant difference in leak or stricture
rate, though trend in favor of hand-sewn• RR Mortality 0.45 in hand-sewn (p=0.05)

Trauma Suture is better• Retrospective cohort—Harborview, Seattle• Small bowel and large bowel, blunt and penet.• Hypothesis: bowel edema in trauma renders
fixed depth staple dangerous• Looked for clinically significant leaks
Brundage et. al. JOT 1999
11Fistula.132 (3%)6 (10%)IAA.0404 (7%)Leak
6058npSewnStapled
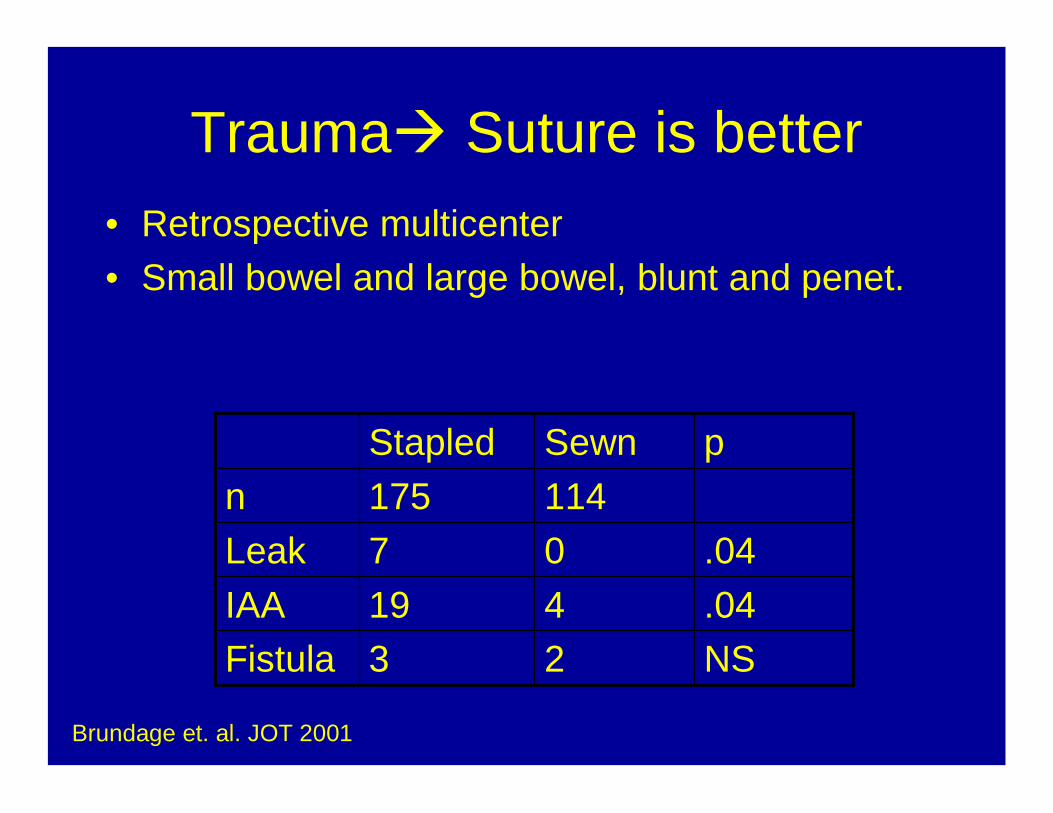
Trauma Suture is better• Retrospective multicenter• Small bowel and large bowel, blunt and penet.
Brundage et. al. JOT 2001
NS23Fistula.04419IAA.0407Leak
114175npSewnStapled

Trauma No Difference• Retrospective cohort—Minnesota group• Small bowel injury only, blunt and penet.• Compared resections with handsewn vs. stapled
reconstruction
Witzke et. al. JOT 2000
NS02FistulaNS1511IAANS30Leak
34110npSewnStapled

Trauma No Difference• Prospective multicenter nonrandomized• Penetrating colon injuries• Leaks defined as req. draining or operation
Demetriades, Moore et. al. JOT 2002
0.697.8%6.3%Leak0.83.1%3.8%Mortality
0.3915.6%20.3%IAA
12879n0.320.3%26.6%Infection
pSewnStapled

Heterogeneity• Shape
• Technique
• Technical
• Location
• Indication
End-to-EndEnd-to-SideSide-to-Side
StapledHandsewn
CircularLinearContinuousInterrupted
Single LayerDouble Layer
2nd layerNo reinforcement
TensionBlood SupplyTechnical execution
EsophagusStomachSmall bowelLarge bowel Cancer
IBDTraumaInfection
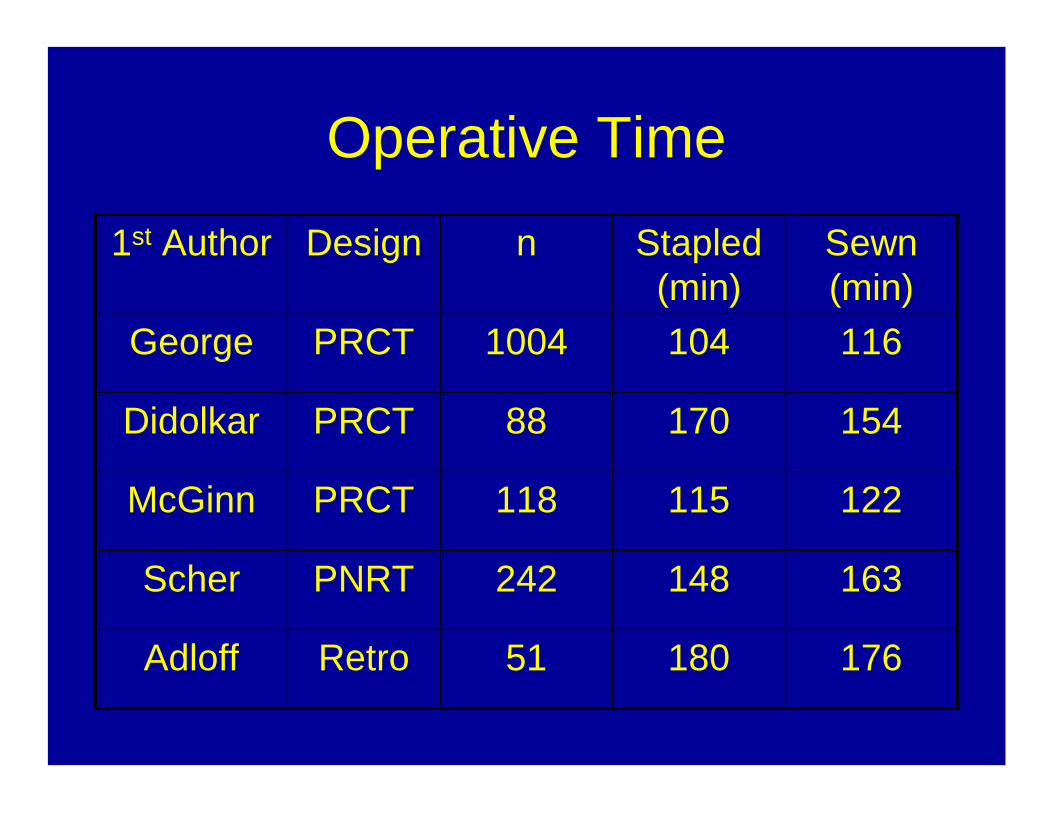
Operative Time
17618051RetroAdloff
163148242PNRTScher
122115118PRCTMcGinn
15417088PRCTDidolkar
1161041004PRCTGeorge
Sewn (min)
Stapled (min)
nDesign1st Author

Single surgeon experienceBruno Cola, Bologna, Italy
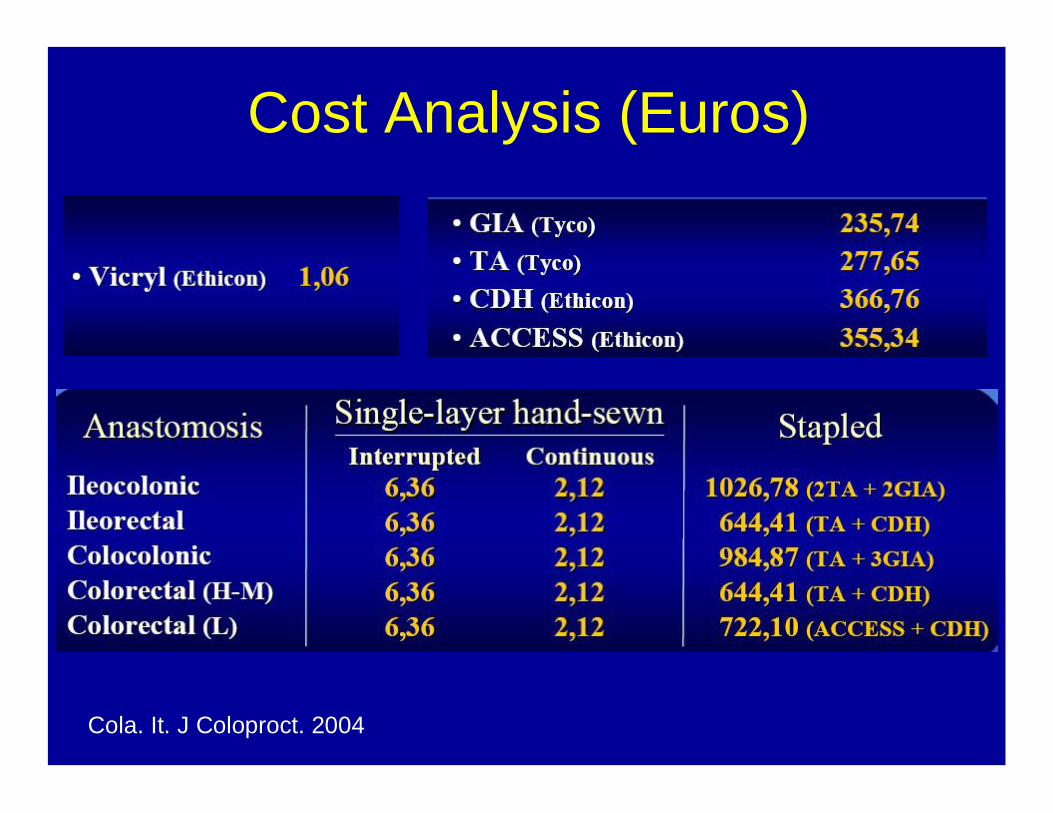
Cost Analysis (Euros)
Cola. It. J Coloproct. 2004

Cost Analysis (Euros)
Cola. It. J Coloproct. 2004
Conclusion
• No solid evidence for improved outcomes or decreased operative times with stapled anastomosis of any type
• In an era of morbidly expensive healthcare, the use of staplers for GI anastomosis should ONLY be considered in the setting of special circumstance (laparoscopy, etc.)