Haem metabolism
21
HAEM(HEME) METABOLISM LEVEL 200 OHENEBA HAGAN
-
Upload
oheneba-hagan -
Category
Education
-
view
363 -
download
0
Transcript of Haem metabolism

HAEM(HEME) METABOLISM
LEVEL 200
OHENEBA HAGAN

Objectives
• Haem synthesis• Regulation of haem synthesis• Catabolism of haem• Regulation of haem catabolism• Clinical importance of haem metabolism

Haem
Porphyrin+Fe
Some important human haemoproteins are; haemoglobin, myoglodin,cytochromes, catalase, tryptophan pyrrolase
In plants Porphyrin+Zinc- photosynthetic pigment chlorophyll

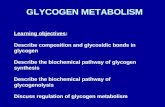
Haem SynthesisTakes place in the bone marrow and liver
Starts with condensation of glycine and succinyl CoA in the mitochondria
Condensation reaction is catalysed by a-aminolevulinate synthase (ALA synthase)
In the liver its ALA synthase I and in the bone marrow its ALA synthase II.
Co-factor needed for this reaction is pyridoxal phosphate
This reaction is the rate limiting step of haem synthesis
OOC CH 2 CH 2 C S-C oA
O
+ OOC CH 2 NH 3+
OOC CH 2 CH 2 C
O
CH 2 NH 3+
CO 2CoA-SH
H+succinyl-CoA glycine
-am inolevulinate (ALA)
-Aminolevulinic A cid Synthase

Haem synthesis
(cont.)

① It is regulated by repression mechanism. Heme inhibits the synthesis of ALA synthesis by acting as a corepressor. The feedback regulatory effect is a typical example of end-product inhibition.
1. ALA synthase
Major site of regulation is at the level of ALA synthase.
Regulation of heme synthesis

② ALA synthase is also allosterically inhibited by haematin.
When there is excess of free heme without globin chains to bind with, the Fe++ is oxidized to Fe+++ forming hematin. Haematin will inhibit ALA synthase to prevent excessive unwanted production of haem.
Haematin will also inhibit the translocation of ALA synthase from the cytoplasm into the mitochondria where its substrate, succinyl CoA is formed. thus heme synthesis is inhibited till there are sufficient globin chains to bind with.

③ Lack of Vit B6 will decrease the synthesis of ALA. Drugs like INH (isonicotinic acid hydrazide) that decrease
the availability of pyridoxal phosphate may also affect heme synthesis.
4. Drugs that induce cytochrome P450 eg barbiturates griseofulvin induce ALAS 1 synthesis. In patients with porphyria these drugs can precipitate attacks

2. Haem synthesis may be inhibited by heavy metals. the steps catalyzed by ALA dehydratase and ferrochelatase are inhibited by lead.
3. erythropoietin, EPO
The kidneys also secrete a hormone called erythropoietin. The function of erythropoietin is to stimulate the production of red blood cells. The kidney produces 85~95% of the body's erythropoietin so when the kidney is damaged (kidney disease or failure), not enough erythropoietin is produced to maintain normal red blood cell levels. This leads to anemia.

Clinical Correlates(Porphyria)
• Rare genetic diseases in which activity of one of the enzymes involved in heme synthesis is decreased (e.g., PBG Synthase, Porphobilinogen Deaminase, etc…)
• Usually inherited in autosomal dominant except congenital erythropoeitic porphyria
• Symptoms depend on enzyme
affected, organ involved
• Symptoms are usually acute or cutaneous
• Acute symptoms usually involves enzymes before uroporphobilinogen (accumulation of ALA, PBG). Includes abdominal pains and neuropsychiatric symptoms
• Cutaneous symptoms results from enzyme deficiencies from uroporphobilinogen. Substrates accumulate in skin leading to oxidized products. Photosensitvity –skin damage


Diagnosis and Treatment

• From family pedigree
• History of abdominal pain+neuropsychiatric symptoms
• Photosensitive skin rashes
• Urine which changes colour on exposure to sunlight (red)
• medical support for vomiting and pain
• hemin, decreases ALA synthase synthesis
• Consumption of large amounts of carbohydrates
• avoidance of sunlight and precipitating drugs, factors
• Avoid drugs that induce cytochrome P450 eg barbiturates

Haem catabolismCytochrome has high turnover rate
Red blood cells have life span of 60-120 days
When haemoproteins are destroyed they yield haem
70% of haem from red blood cells
Haem is eventually converted to bilirubin for excretion

Extravascular Pathway for RBC Destruction
(Liver, Bone marrow, & Spleen)
Haemoglobin
Globin
Amino acids
Amino acid pool
Haem Bilirubin
Fe2+
Excreted
Phagocytosis & Lysis

Haem degradation• Takes place in the ER of
reticuloendothelial system of spleen,liver,bone marrow
• CO monoxide produced is exhaled (can be used to quantify haem turnover rate)
• In birds and amphibians the green biliverdin is excreted
• Bilirubin is sparingly soluble and must be transported bound to albumin
• Bilirubin is transported to the liver for elimination

• Bilirubin is taken up in the liver by carrier-mediate transport into parenchymal cells
• In the cells bilirubin binds to Ligandin and protein Y
• Conjugation of bilirubin to make it polar is achieved by addition of mainly glucuronide. Others include xylose, sulfate and ribose
• Conjugation with glucuronide is catalysed by glucuronyltransferase (glucuronyl-UDP)
• Two glucuronic acid is conjugated to bilirubin (bilirubin diglucuronide)
• Conjugated bilirubin is secreted into the bile by an active transport mediated by multidrug resistance like protein 2 (MRP-2)

• Bile gets secreted into the intestine• At the terminal ileumand large intestine
bacterial glucuronidases remove the glucuronides to form
• The free bilirubin is reduced in the intestine to the colourless urobilinogen
• Urobilinogen/stercobilinogen is oxidized to the coloured urobilin/stercobilin (excreted in feaces- imparts red brown colour to stool)
• Some of the urobilinogen is taken up by the blood back to the liver to be re-excreted back into the bile (enterohepatic urobilinogen cycle)
• Urobilinogen excreted by the liver. Oxidized to urobilin (gives urine its unique straw colour

Hyperbilirubinaemia• Increases levels of bilirubin
(conjugated or unconjugated)
• Could be due to increased bilirubin production or decreased bilirubin secretion
• Classified as pre hepatic, intra-hepatic and post hepatic

Neonatal Jaundice
• Common, particularly in premature infants
• Transient (resolves in the first 10 days)
• Due to immaturity of the enzymes involved in bilirubin conjugation
• High levels of unconjugated bilirubin are toxic to the newborn – due to its hydrophobicity it can cross the blood-brain barrier and cause a type of mental retardation known as kernicterus
• If bilirubin levels are judged to be too high, then phototherapy with UV light is used to convert it to a water soluble, non-toxic form
• If necessary, exchange blood transfusion is used to remove excess bilirubin
• Phenobarbital is oftentimes administered to Mom prior to an induced labor of a premature infant – crosses the placenta and induces the synthesis of UDP glucuronyl transferase
• Jaundice within the first 24 hrs of life or which takes longer then 10 days to resolve is usually pathological and needs to be further investigated