Glucose Metabolism During Pregnancy Dr. M. Tohidi Surgical & clinical pathologist Research Institute...
51
-
Upload
hollie-lawrence -
Category
Documents
-
view
215 -
download
0
Transcript of Glucose Metabolism During Pregnancy Dr. M. Tohidi Surgical & clinical pathologist Research Institute...

Glucose Glucose Metabolism Metabolism
During During PregnancyPregnancyDr. M. TohidiDr. M. Tohidi
Surgical & clinical pathologistSurgical & clinical pathologistResearch Institute for Endocrine SciencesResearch Institute for Endocrine Sciences
Shaheed Beheshti University of Medical ScienceShaheed Beheshti University of Medical Science
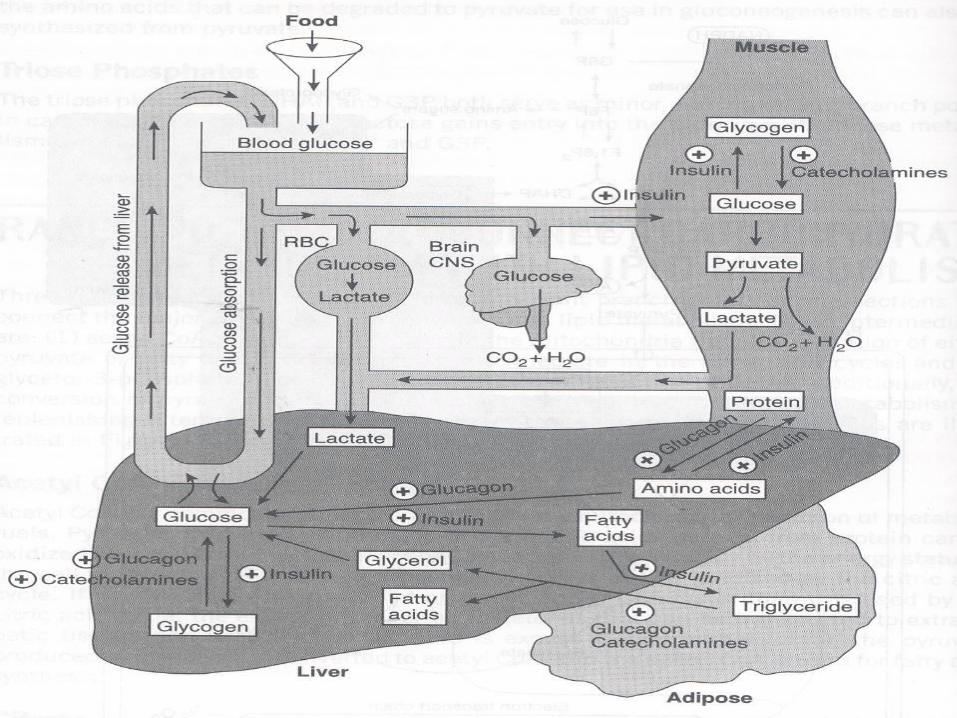
Carbohydrate Carbohydrate metabolism metabolism
Major consumer of glucose:Major consumer of glucose: RBCsRBCs CNSCNS
Organs involving in maintaining blood Organs involving in maintaining blood glucose levelglucose level
LiverLiver MuscleMuscle Adipose tissueAdipose tissue
LiverLiver
In the well-fed state:In the well-fed state:1- Excess glucose is converted to glycogen.1- Excess glucose is converted to glycogen.
Glucose GlycogenGlucose Glycogen Insulin +Insulin +2- Remaining glucose is used for fatty acid synthesis.2- Remaining glucose is used for fatty acid synthesis.
Glucose Fatty acidGlucose Fatty acid Insulin +Insulin +
LiverLiver
In the fasting state:In the fasting state:
1- Glycogenolysis1- Glycogenolysis
Glycogen GlucoseGlycogen Glucose
Glucagone +Glucagone +
Catecholamine +Catecholamine +
2- 2- GluconeogenesisGluconeogenesis
Glycerol from adipose tissueGlycerol from adipose tissue
Lactate from RBCs & muscle GlucoseLactate from RBCs & muscle Glucose
Aminoacids from muscleAminoacids from muscle
Major hormones in CHO Major hormones in CHO metabolismmetabolism
InsulinInsulin
Counterregulatory hormones :Counterregulatory hormones :
GlucagonGlucagon
CatecholaminesCatecholamines
CortisolCortisol
Growth hormoneGrowth hormone
InsulinInsulin
An anabolic hormoneAn anabolic hormone Secreted from beta- cells of pancreasSecreted from beta- cells of pancreas Functions:Functions: In the liver stimulates:In the liver stimulates: glycogenesisglycogenesis fatty acid synthsis fatty acid synthsis protein synthesis protein synthesis In adipose tissue stimulates:In adipose tissue stimulates: TG synthesisTG synthesis glucose uptake glucose uptake In muscles stimulates:In muscles stimulates: glucose uptake & glycogenesisglucose uptake & glycogenesis aminoacids uptakeaminoacids uptake
GlucagonGlucagon
An catabolic hormoneAn catabolic hormone Secreted from alpha- cells of pancreasSecreted from alpha- cells of pancreas Functions:Functions: In the liver stimulates:In the liver stimulates: GlycogenolysisGlycogenolysis GluconeogenesisGluconeogenesis In adipose tissue stimulates lypolysisIn adipose tissue stimulates lypolysis In muscles stimulates protein degradationIn muscles stimulates protein degradation
CatecholamineCatecholamine Secreted from adrenal medullaSecreted from adrenal medulla Functions:Functions: In the liver stimulates:In the liver stimulates: GlycogenolysisGlycogenolysis GluconeogenesisGluconeogenesis In adipose tissue stimulates lypolysisIn adipose tissue stimulates lypolysis In muscles stimulates release of AA & lactateIn muscles stimulates release of AA & lactate Stimulatory effect on glucagon release from alpha-cellsStimulatory effect on glucagon release from alpha-cells Inhibitory effect on release of insulin from beta-cellsInhibitory effect on release of insulin from beta-cells
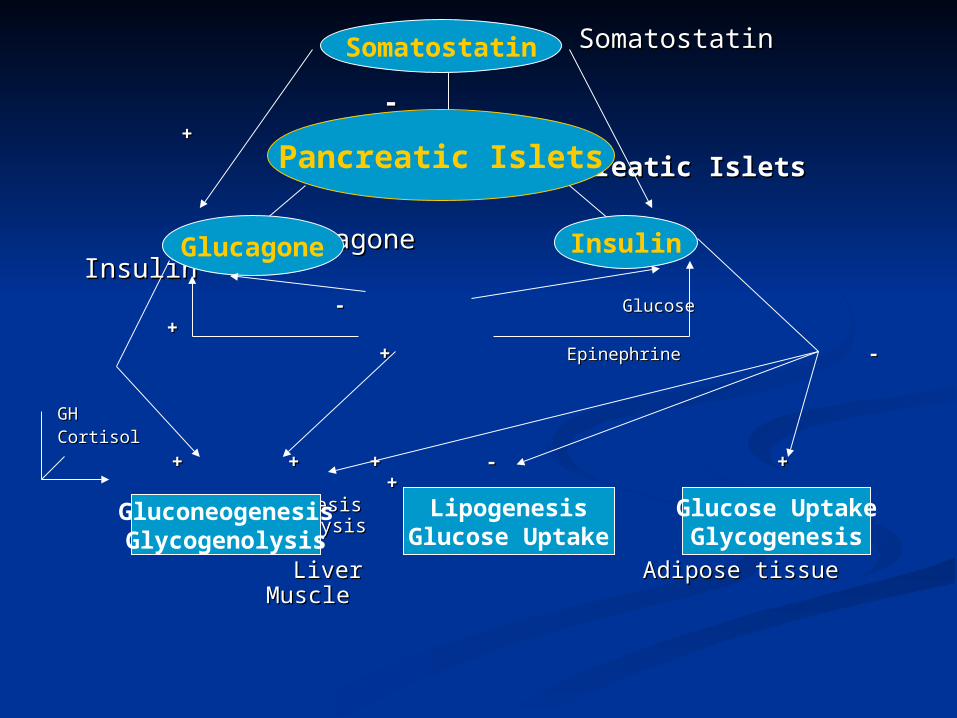
Somatostatin Somatostatin - - ++ Pancreatic IsletsPancreatic Islets
Glucagone InsulinGlucagone Insulin -- Glucose Glucose ++ ++ Epinephrine Epinephrine --
GHGHCortisolCortisol
+ + + - + + + + - + + +
GluconeogenesisGluconeogenesis GlycogenolysisGlycogenolysis
LiverLiver Adipose tissue Adipose tissue MuscleMuscle
GluconeogenesisGlycogenolysis
LipogenesisGlucose Uptake
Glucose UptakeGlycogenesis
Pancreatic Islets
Glucagone Insulin
Somatostatin
Glucose Metabolism Glucose Metabolism in normal pregnancyin normal pregnancy
Pregnancy is characterized by a Pregnancy is characterized by a complex endocrine - metabolic complex endocrine - metabolic adaptations, which don’t reflect adaptations, which don’t reflect a pathological condition. a pathological condition.
These adaptations are necessary These adaptations are necessary to meet the energy demand of to meet the energy demand of the fetus and to prepare the fetus and to prepare maternal organism for delivery maternal organism for delivery & lactation.& lactation.
Adaptations:Adaptations:
Impaired insulin sensitivityImpaired insulin sensitivity
Increased beta- cell responseIncreased beta- cell response
Moderate increase in blood glucose level Moderate increase in blood glucose level
(particularly after meal)(particularly after meal)
Change in circulatory FFAs, TGs, CHOL & Change in circulatory FFAs, TGs, CHOL &
phospholipids.phospholipids.
Insulin ResistanceInsulin Resistance
During the first trimester of pregnancy, insulin sensitivity is During the first trimester of pregnancy, insulin sensitivity is normal if not higher than normal.normal if not higher than normal.
As pregnancy progresses, a condition of insulin resistance sets As pregnancy progresses, a condition of insulin resistance sets in.in.
The impairment of insulin action being more pronounced at The impairment of insulin action being more pronounced at the level of skeletal muscle than adipose tissue.the level of skeletal muscle than adipose tissue.
The development of gestational diabetes is associated with a The development of gestational diabetes is associated with a much greater severity of insulin resistance. In these women, a much greater severity of insulin resistance. In these women, a lower insulin sensitivity is likely to be present both before and lower insulin sensitivity is likely to be present both before and after pregnancy. after pregnancy.
The degree of insulin resistance seems to be influenced by The degree of insulin resistance seems to be influenced by obesity & inheritance.obesity & inheritance.
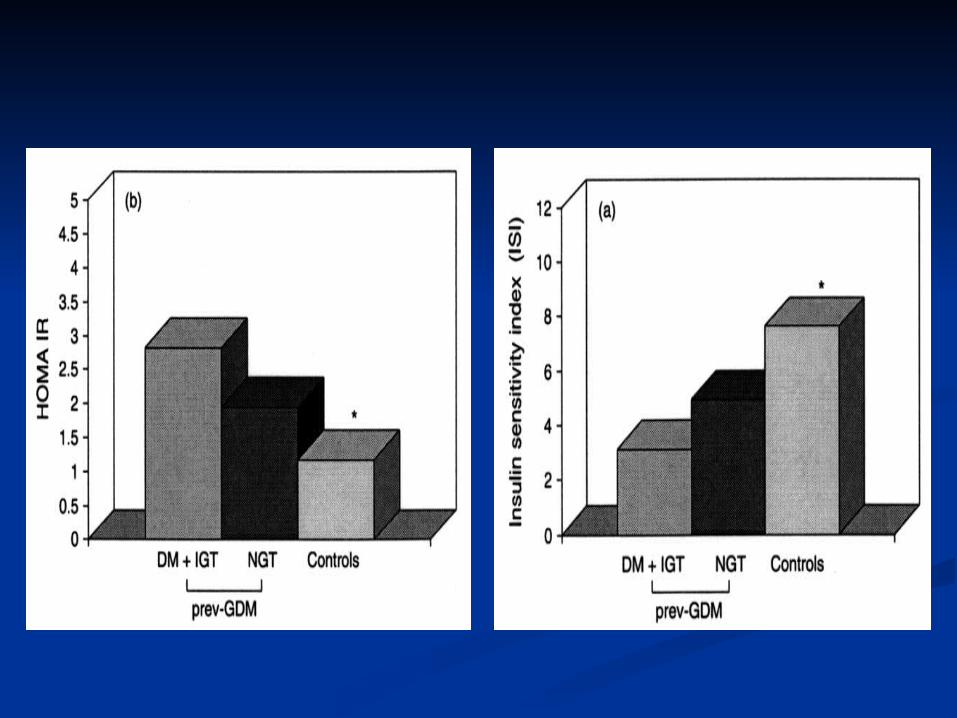
In Di Cianni et al. study:In Di Cianni et al. study:
women with previous gestational diabetes present, women with previous gestational diabetes present, compared to control women, a modification in the compared to control women, a modification in the indices of insulin sensitivity obtained both in basal indices of insulin sensitivity obtained both in basal conditions [homeostatic model assessment (HOMA)] conditions [homeostatic model assessment (HOMA)] and after oral administration of glucose [insulin and after oral administration of glucose [insulin sensitivity index].sensitivity index].
Diabetes Metab Res Rev 2003; 19: 259- 270Diabetes Metab Res Rev 2003; 19: 259- 270
Catalano Catalano et al.et al., using the euglycemic-, using the euglycemic-hyperinsulinemic clamp, estimated a 47% hyperinsulinemic clamp, estimated a 47% reduction in insulin sensitivity in obese women reduction in insulin sensitivity in obese women and a 56% reduction in normal-weight women and a 56% reduction in normal-weight women in the third trimester of gestation.in the third trimester of gestation.
Am J Obstet Gynecol 1991; 165: 1667-72.Am J Obstet Gynecol 1991; 165: 1667-72.
Am J Obstet Gynecol 1999; 180: 903- 16.Am J Obstet Gynecol 1999; 180: 903- 16.
According to other studies, with the According to other studies, with the progression of pregnancy, insulin sensitivity progression of pregnancy, insulin sensitivity can be reduced as much as 60 to 80%.can be reduced as much as 60 to 80%.
Why insulin Why insulin resistance?resistance?
A physiological event favoring glucose supplyA physiological event favoring glucose supply to the fetus.to the fetus.
The reduced insulin-mediated utilization of glucose The reduced insulin-mediated utilization of glucose switches the maternal energy metabolism from switches the maternal energy metabolism from carbohydrates to lipid substrates (free fatty acids), carbohydrates to lipid substrates (free fatty acids), redirecting carbohydrates toward the fetal tissues.redirecting carbohydrates toward the fetal tissues.
Even the slight, though prolonged, postprandial Even the slight, though prolonged, postprandial hyperglycemia associated with impaired insulin hyperglycemia associated with impaired insulin sensitivity can contribute to rerouting nutrients from sensitivity can contribute to rerouting nutrients from the mother to the fetus.the mother to the fetus.
Mechnism of insulin resistanceMechnism of insulin resistance in pregnancy in pregnancy
The cellular mechanism of The cellular mechanism of insulin resistance in pregnancy insulin resistance in pregnancy is is multifactorialmultifactorial and involves and involves several steps of the intracellular several steps of the intracellular generation and propagation of generation and propagation of the insulin signal. the insulin signal.
Reduced activity of Insulin Reduced activity of Insulin receptorreceptor
The study of the insulin binding has not The study of the insulin binding has not demonstrated significant modifications demonstrated significant modifications either in normal pregnancy or in GDM.either in normal pregnancy or in GDM.
A reduced activity (30-40%) of insulin A reduced activity (30-40%) of insulin receptor tyrosine kinase has been receptor tyrosine kinase has been observed in the skeletal muscle of observed in the skeletal muscle of obese women in both normal and obese women in both normal and diabetic pregnancy.diabetic pregnancy.
Reduced expression of Reduced expression of IRS-1IRS-1
Expression of IRS-1 is reduced in Expression of IRS-1 is reduced in experimental animals during experimental animals during pregnancy , a finding that has been pregnancy , a finding that has been confirmed in the skeletal muscle of confirmed in the skeletal muscle of normotolerant and GDM women in the normotolerant and GDM women in the last weeks of pregnancy: tyrosine last weeks of pregnancy: tyrosine phosphorylation of IRS-1 is reduced, phosphorylation of IRS-1 is reduced, compared to the prepregnancy state, by:compared to the prepregnancy state, by:
28% in normal pregnancy 28% in normal pregnancy 41% in a pregnancy with GDM 41% in a pregnancy with GDM
Insulin Receptor Substrate- 1 Insulin Receptor Substrate- 1
Phosphorylation on Tyrosine Phosphorylation on Tyrosine domain domain
Trigger recruitment of PI 3- Trigger recruitment of PI 3- kinasekinase
Stimulation of glucose transport Stimulation of glucose transport
Reduced GLUT4Reduced GLUT4
Reduction in GLUT4 in the late stage Reduction in GLUT4 in the late stage of pregnancy, and to a greater extent of pregnancy, and to a greater extent in GDM.in GDM.
The alterations of the insulin-signaling The alterations of the insulin-signaling cascade, modulated by humoral cascade, modulated by humoral factors:factors:
PC-1: modulate insulin action PC-1: modulate insulin action TNF- TNF- ::
TNF- TNF- The impairment in insulin action correlates The impairment in insulin action correlates
with TNF- levels (with TNF- levels (rr = -0.69; = -0.69; pp < 0.006) . When < 0.006) . When measured along with hCG, estradiol, measured along with hCG, estradiol, progesterone, hPL, and prolactin, TNF- progesterone, hPL, and prolactin, TNF- remains the only significant predictor of the remains the only significant predictor of the change in insulin sensitivity in late pregnancy change in insulin sensitivity in late pregnancy ((rr = -0.60; = -0.60; pp < 0.02). < 0.02).
Though the placenta can produce TNF-Though the placenta can produce TNF- , over , over 90% of the circulating TNF- is of maternal 90% of the circulating TNF- is of maternal origin. origin.
The rise in cytokines is associated with the The rise in cytokines is associated with the enlargement of the maternal fat massenlargement of the maternal fat mass. .
Kirwan et al.Diabetes 2002; 51: 2207-13Kirwan et al.Diabetes 2002; 51: 2207-13
THF-THF- / continue: / continue:
TNF-TNF- in plasma of obese patients is much in plasma of obese patients is much lower compared with that found in burn & lower compared with that found in burn & cachectic patients cachectic patients
Paracrine effect of TNF-Paracrine effect of TNF- on skeletal on skeletal muscle insulin resistance.muscle insulin resistance.
TNF-TNF- impairs insulin signaling by: impairs insulin signaling by: serine phosphorylation of IRS-1serine phosphorylation of IRS-1 IR tyrosine kinase activityIR tyrosine kinase activityBarbour et al. Diabetes care 2007; 30 S: s112-s119.Barbour et al. Diabetes care 2007; 30 S: s112-s119.
AdiponectinAdiponectin A protein synthesized exclusively in A protein synthesized exclusively in
adipocytes.adipocytes. Low plasma adiponectin concentration Low plasma adiponectin concentration
correlate highly with insulin resistance correlate highly with insulin resistance in obesity, DM II & GDM.in obesity, DM II & GDM.
Decline adiponectin secretion & its Decline adiponectin secretion & its mRNA level in white adipose tissue with mRNA level in white adipose tissue with advancing pregnancy evev in lean advancing pregnancy evev in lean women. ( due to pregnancy associated women. ( due to pregnancy associated factors)factors)
Catalano et al. Diabetologia 2006; 49: 1677-85.Catalano et al. Diabetologia 2006; 49: 1677-85.
Insulin Insulin SecretionSecretion
Both in normal pregnancy and in GDM, insulin Both in normal pregnancy and in GDM, insulin secretion increases steadily from the first secretion increases steadily from the first trimester and reaches a maximum in the third, trimester and reaches a maximum in the third, returning to normal values after delivery.returning to normal values after delivery.
The insulin response to the oral glucose intake The insulin response to the oral glucose intake is associated with a 120% increase in first-phase is associated with a 120% increase in first-phase insulin secretion by the 12th to 14th gestational insulin secretion by the 12th to 14th gestational week. week.
The second phase does not seem to be affected, The second phase does not seem to be affected, at least in the first weeks of pregnancy.at least in the first weeks of pregnancy.
The insulin response after an intravenous The insulin response after an intravenous glucose tolerance test (IVGTT) is increased with glucose tolerance test (IVGTT) is increased with respect to values observed before and after respect to values observed before and after pregnancy. pregnancy.
In GDM:In GDM:
There is a peculiar loss of first-phase There is a peculiar loss of first-phase insulin secretion in women with insulin secretion in women with GDM.GDM.
There is a delay in the peak of There is a delay in the peak of insulin concentration after oral insulin concentration after oral intake of glucose observed in GDM.intake of glucose observed in GDM.
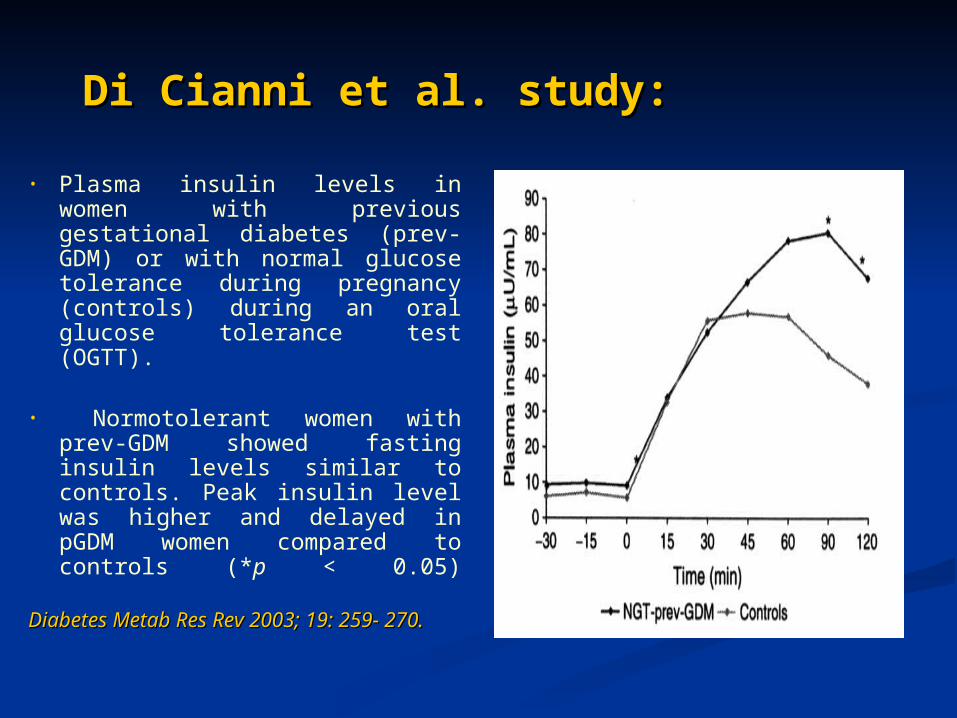
Di Cianni et al. study:Di Cianni et al. study:
• Plasma insulin levels in women with previous gestational diabetes (prev-GDM) or with normal glucose tolerance during pregnancy (controls) during an oral glucose tolerance test (OGTT).
• Normotolerant women with prev-GDM showed fasting insulin levels similar to controls. Peak insulin level was higher and delayed in pGDM women compared to controls (*p < 0.05)
Diabetes Metab Res Rev 2003; 19: 259- Diabetes Metab Res Rev 2003; 19: 259- 270.270.
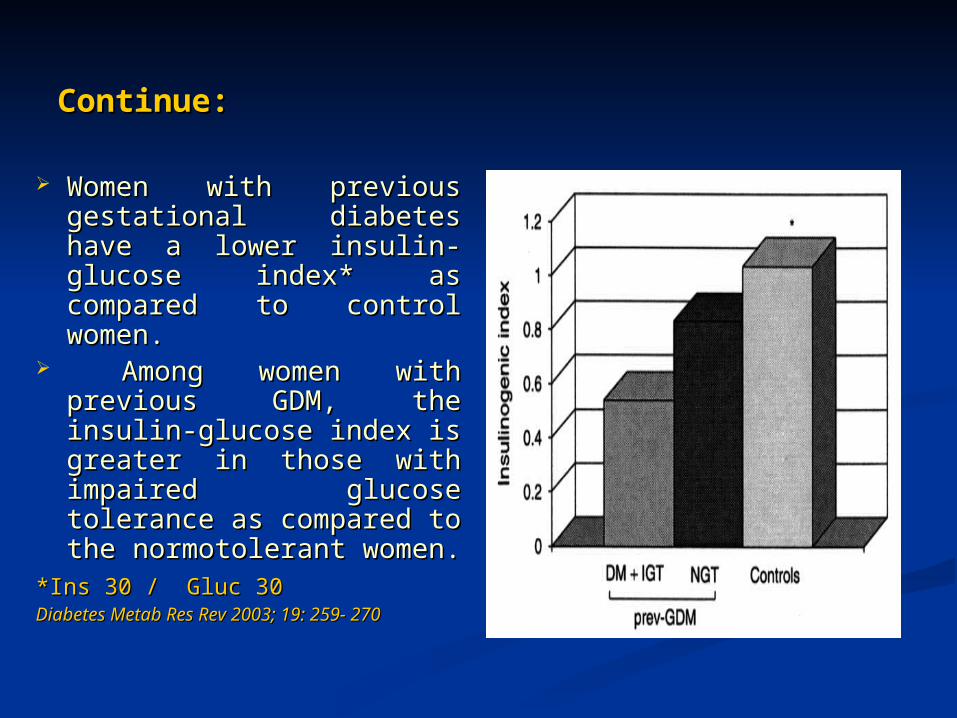
Continue:Continue: Women with previous Women with previous
gestational diabetes have gestational diabetes have a lower insulin-glucose a lower insulin-glucose index* as compared to index* as compared to control women.control women.
Among women with Among women with previous GDM, the previous GDM, the insulin-glucose index is insulin-glucose index is greater in those with greater in those with impaired glucose impaired glucose tolerance as compared to tolerance as compared to the normotolerant the normotolerant women.women.
**Ins 30 / Gluc 30Ins 30 / Gluc 30 Diabetes Metab Res Rev 2003; 19: 259- 270Diabetes Metab Res Rev 2003; 19: 259- 270
ProinsulinProinsulin
Fasting plasma proinsulin levels increase during Fasting plasma proinsulin levels increase during pregnancy to return to normal after delivery.pregnancy to return to normal after delivery.
Nonetheless, plasma proinsulin levels tend to remain Nonetheless, plasma proinsulin levels tend to remain slightly elevated even after delivery in women who slightly elevated even after delivery in women who had GDM. had GDM.
An increase in proinsulin concentration has been An increase in proinsulin concentration has been reported in nonpregnant women with type 2 diabetes reported in nonpregnant women with type 2 diabetes mellitus (DM) and IGT.mellitus (DM) and IGT.
suggesting a suggesting a secretory secretory -cell dysfunction-cell dysfunction.. The increase in plasma proinsulin concentration The increase in plasma proinsulin concentration
during pregnancy is likely to be the expression of a during pregnancy is likely to be the expression of a maturation blockmaturation block of insulin synthesis and release, of insulin synthesis and release, secondary to increased demand imposed by secondary to increased demand imposed by concomitant insulin resistance.concomitant insulin resistance.
To satisfy these needs during normal To satisfy these needs during normal pregnancy and in pregnancy with GDM:pregnancy and in pregnancy with GDM:
the the -cell undergoes significant structural -cell undergoes significant structural and functional changes including:and functional changes including:
(1) increased insulin secretion(1) increased insulin secretion
(2) increased insulin synthesis(2) increased insulin synthesis
(3) enhanced utilization and oxidation of (3) enhanced utilization and oxidation of glucoseglucose
(4) accelerated (4) accelerated -cell proliferation and -cell proliferation and increased islet volume increased islet volume
(5) higher cAMP metabolism(5) higher cAMP metabolism
HyperinsulinemiaHyperinsulinemia
Increased circulating immunoreactive Increased circulating immunoreactive insulin in late pregnancy compared with insulin in late pregnancy compared with nonpregnant women (intact form). nonpregnant women (intact form).
whole-body insulin kinetic are similar in whole-body insulin kinetic are similar in pregnant & nonpregnant women.pregnant & nonpregnant women.
No difference in hepatic insulin extraction.No difference in hepatic insulin extraction.
Hyperinsulinemia of pregnancy is due Hyperinsulinemia of pregnancy is due to enhanced pancrearic beta-cell to enhanced pancrearic beta-cell functionfunction
Hormones associated with modifications Hormones associated with modifications in insulin secretion and actionin insulin secretion and action
Estrogens Estrogens Insulin Insulin concentration concentration
Insulin bindingInsulin binding
Progesterone Progesterone Glucose Glucose transport transport
Insulin binding Insulin binding
Suppression of Suppression of insulin-induced hepatic insulin-induced hepatic gluconeogenesis gluconeogenesis
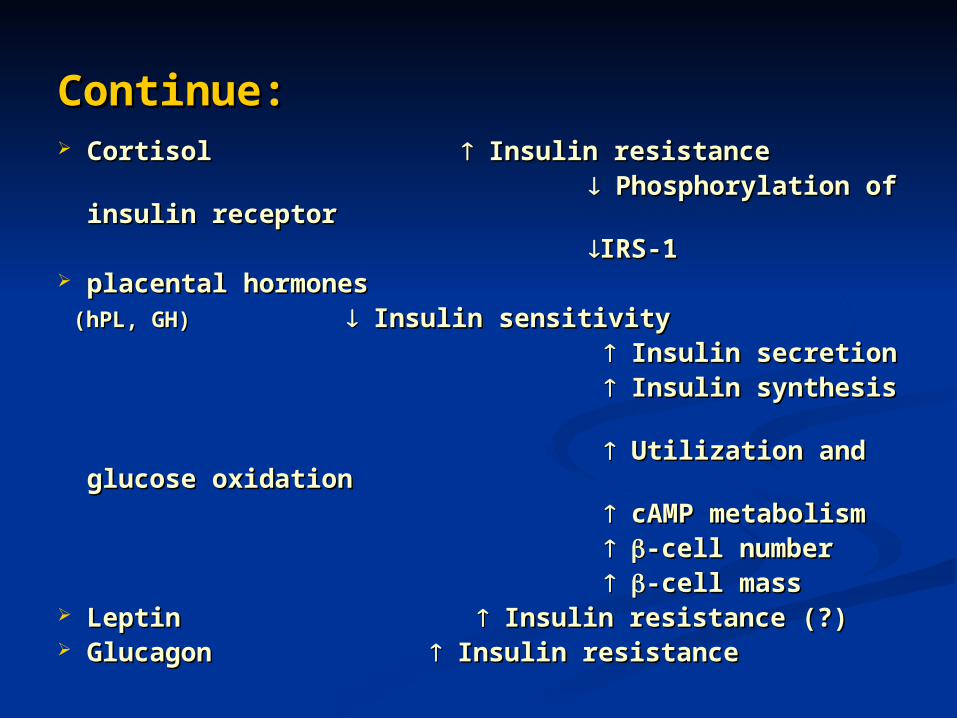
Continue:Continue: Cortisol Cortisol Insulin resistance Insulin resistance Phosphorylation of insulin Phosphorylation of insulin
receptorreceptor IRS-1 IRS-1 placental hormonesplacental hormones (hPL, GH)(hPL, GH) Insulin sensitivity Insulin sensitivity Insulin secretionInsulin secretion Insulin synthesis Insulin synthesis Utilization and glucose Utilization and glucose
oxidation oxidation cAMP metabolismcAMP metabolism -cell number -cell number -cell mass-cell mass Leptin Leptin Insulin resistance (?) Insulin resistance (?) Glucagon Glucagon Insulin resistance Insulin resistance
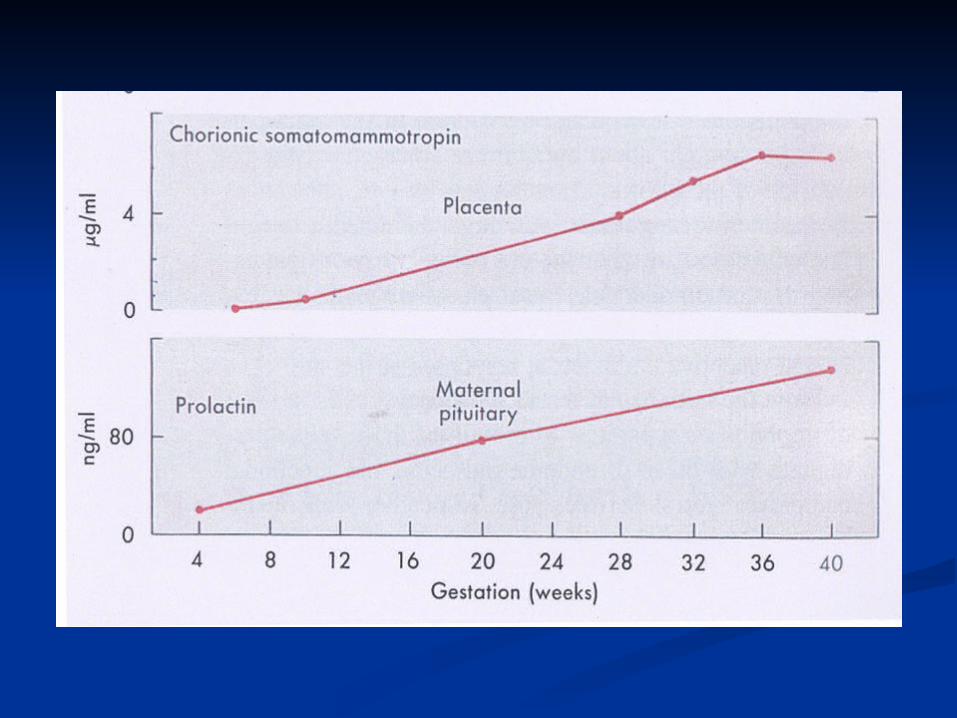
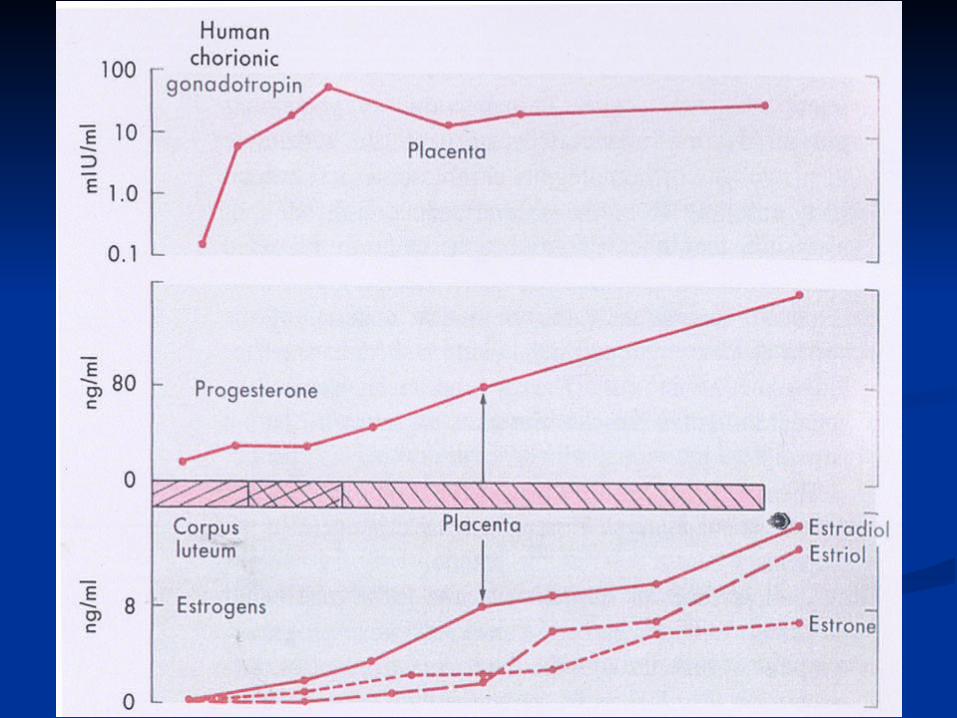
Human Placental Human Placental lactogen (hPL)lactogen (hPL)
Produced by syncytiotrphoblastsProduced by syncytiotrphoblasts Most strong antagonist of insulin Most strong antagonist of insulin
during pregnancyduring pregnancy Appeared about 10 weeks of gestationAppeared about 10 weeks of gestation Daily production at term: 1-2 g/dayDaily production at term: 1-2 g/day Growth hormone- like properties Growth hormone- like properties
(96% structural similarity)(96% structural similarity)
Other effects of hPL on glucose Other effects of hPL on glucose metabolismmetabolism
1- 1- Antagonistic effect to insulin-stimulated Antagonistic effect to insulin-stimulated
glucose uptakeglucose uptake 2- Enhanced lipolysis Free fatty 2- Enhanced lipolysis Free fatty
acidacid 3- Stimulation of gluconeogenesis3- Stimulation of gluconeogenesis 4- Promotes maternal production of insulin-4- Promotes maternal production of insulin-
like growth factors (IGFs)like growth factors (IGFs) 5- directing energy substrates toward the 5- directing energy substrates toward the
fetus fetus
ProlactinProlactin
Stimulated by rising titer of estrogenStimulated by rising titer of estrogen Structural similarity to GH Structural similarity to GH Effect on CHO metabolism in con. Effect on CHO metabolism in con.
>200ng/ml>200ng/ml Suppresion of prolactin level by high Suppresion of prolactin level by high
doses of pyridoxin in women with doses of pyridoxin in women with GDM , has improved glucose GDM , has improved glucose tolerance.tolerance.
LeptinLeptin It is secreted by the adipose tissue and acts at the hypothalamic level through the It is secreted by the adipose tissue and acts at the hypothalamic level through the
inhibition of neuropeptide Y and by stimulating thermogenesis.inhibition of neuropeptide Y and by stimulating thermogenesis.
Plasma leptin levels increase significantly during pregnancy reaching a peak in the Plasma leptin levels increase significantly during pregnancy reaching a peak in the second trimester. At 36 weeks' gestation, it is 1.7-fold higher than it is postpartum.second trimester. At 36 weeks' gestation, it is 1.7-fold higher than it is postpartum.
Circulating plasma leptin levels correlate with plasma insulin concentration as well Circulating plasma leptin levels correlate with plasma insulin concentration as well as with maternal adipose mass. As such, it can be considered a marker of insulin as with maternal adipose mass. As such, it can be considered a marker of insulin resistance and obesity. resistance and obesity.
Recent data show that women with gestational diabetes have increased plasma Recent data show that women with gestational diabetes have increased plasma leptin concentrations during and after pregnancy.leptin concentrations during and after pregnancy.
Moreover, leptin concentration is positively related to HbA1Moreover, leptin concentration is positively related to HbA1cc and the newborn's and the newborn's body weight, suggesting that poor glycemic control may favor adipose tissue body weight, suggesting that poor glycemic control may favor adipose tissue accumulation in the newborn from women with GDM. accumulation in the newborn from women with GDM.
Cord leptin concentrations correlate with the fetus's weight at birth as well as with Cord leptin concentrations correlate with the fetus's weight at birth as well as with other fetal anthropometric indices. Thus, leptin is likely to play a role in fetal other fetal anthropometric indices. Thus, leptin is likely to play a role in fetal growth and can interfere with maternal glucose metabolism growth and can interfere with maternal glucose metabolism
GlucagonGlucagon Plasma glucagon concentrations increase during the Plasma glucagon concentrations increase during the
last trimester of pregnancy. last trimester of pregnancy. A slight increase may contribute to insulin resistance. A slight increase may contribute to insulin resistance. Plasma glucagon levels are even higher in women Plasma glucagon levels are even higher in women
with GDM.with GDM. It is not clear whether elevated glucagon levels have:It is not clear whether elevated glucagon levels have: any role in the pathogenesis of GDM any role in the pathogenesis of GDM
OrOr if they simply reflect the relative insulin deficiency if they simply reflect the relative insulin deficiency
of these women.of these women.
Insulin degradationInsulin degradation
Increased Insulin degradation during Increased Insulin degradation during pregnancy due to: pregnancy due to:
Placental enzymes with insulinase activityPlacental enzymes with insulinase activity
Membrane- associated insulin-degrading Membrane- associated insulin-degrading activityactivity
Glucose Metabolism Glucose Metabolism in normal pregnancyin normal pregnancy
Early pregnancyEarly pregnancy 1- Increased glucose-stimulated insulin secretion1- Increased glucose-stimulated insulin secretion 2- Unchanged or enhanced peripheral (muscle) 2- Unchanged or enhanced peripheral (muscle)
insulin sensitivityinsulin sensitivity 3- Unchanged basal hepatic glucose production3- Unchanged basal hepatic glucose production 4- Normal or slightly improved glucose tolerance4- Normal or slightly improved glucose tolerance 5- Normal sensitivity to the blood glucose–5- Normal sensitivity to the blood glucose–
lowering effect of exogenously administered insulin lowering effect of exogenously administered insulin
Continue:Continue:
6- Greater insulin responses to oral 6- Greater insulin responses to oral glucose in the first trimester than glucose in the first trimester than before pregnancy. before pregnancy.
120% increase at 12–14 wk gestation 120% increase at 12–14 wk gestation in the first phase of insulin response.in the first phase of insulin response.
7- No significant difference in the 7- No significant difference in the second phase of insulin response second phase of insulin response between early pregnancy & the between early pregnancy & the pregravid state.pregravid state.
Results:Results:
Basal fasting glucose and insulin concentrations Basal fasting glucose and insulin concentrations do not differ significantly from nongravid do not differ significantly from nongravid values.values.
Fat accumulation due to lipogenic effect of Fat accumulation due to lipogenic effect of insulininsulin
Late pregnancyLate pregnancy
1- Rising concentrations of several diabetogenic hormones1- Rising concentrations of several diabetogenic hormones2- Increased peripheral insulin resistance2- Increased peripheral insulin resistance3- Progressive increase in basal & postprandial insulin 3- Progressive increase in basal & postprandial insulin (up to 2 fold in (up to 2 fold in
third trimester) third trimester)
4- 50-70% lower insulin action in late normal pregnancy than in 4- 50-70% lower insulin action in late normal pregnancy than in nonpregnant womennonpregnant women
5- Basal endogenous hepatic glucose production increases by 16–5- Basal endogenous hepatic glucose production increases by 16–30%.( Increased total gluconeogenesis)30%.( Increased total gluconeogenesis)
* to meet the increasing needs of the placenta and fetus * to meet the increasing needs of the placenta and fetus * Glucose production increases with maternal body weight* Glucose production increases with maternal body weight6- Decreased CHO oxidation ( in obese women)6- Decreased CHO oxidation ( in obese women)7- Decreased suppression of endogenous glucose production ( in obese women)7- Decreased suppression of endogenous glucose production ( in obese women)
Results:Results:
Plasma glucose tends to decrease by 10 to 15 Plasma glucose tends to decrease by 10 to 15 mg/dL.mg/dL.
Significantly elevated postprandial Significantly elevated postprandial glucose concentrations glucose concentrations
Prolonged glucose peak Prolonged glucose peak
Presence of a twofold increase in plasma insulin Presence of a twofold increase in plasma insulin concentration.concentration.
Depletion of maternal adipose tissue depotsDepletion of maternal adipose tissue depots

Thank you for your attention