Fisiologi Tear Film

of 14
-
Upload
primita-ayu-damayanti -
Category
Documents
-
view
416 -
download
16
Transcript of Fisiologi Tear Film
-
7/26/2019 Fisiologi Tear Film
1/14
1.2.1 Fisiologi Tear Film
Tear film normal diperlukan untuk mempertahankan fungsi permukaan okuler.
Perubahan patologis yang terlihat pada dry eye disease mempengaruhi semua
komponen tear film,mengubah bagian permukaan okuler yang awalnya bersifat
ocular surface supportive menjadi pro - inflamatory(Khurana, 200!.
"olume terbesar air mata dihasilkan oleh kelenjar lakrimalis yang terletak di
fossa glandula la#rimalis yang terletak di kuadran temporal atas orbita. Kelenjar yang
berbentuk kenari ini dibagi oleh kornu lateral aponeurosis le$ator menjadi lobus orbita
yang lebih besar dan lobus palpebra yang lebih ke#il, masing%masing dengan sistem
duktulus yang bermuara ke forniks temporal superior (Khurana, 200!.
Persarafan kelenjar utama datang dari nu#leus la#rimalis di pons melalui ner$us
intermedius dan menempuh suatu jaras rumit #abang ma&illaris ner$us trigeminus.
Kelenjar lakrimal assesorius, walaupun hanya sepersepuluh dari massa kelenjar utama,
mempunyai peranan penting. 'truktur kelenjar Krause dan olfring identik dengan
kelenjar utama, namun tidak memiliki du#tus. Kelenjar%kelenjar ini terletak di dalam
konjungti$a, terutama di forniks superior. 'el%sel goblet uniseluler, yang juga tersebar di
konjungti$a, mensekresi glikoprotein dalam bentuk musin. )odifikasi kelenjar sebasea
meibom dan *eis ditepian palpebra memberi lipid pada air mata. Kelenjar )oll adalah
modifikasi kelenjar keringat yang ikut membentuk tear film. (Khurana, 200!.
+ambar 2. Produksi -ear film
(http//www.ad$o#urenf2.org/li$ingwithnf2ailments1#aredryeye.php !
http://www.advocurenf2.org/livingwithnf2_ailments+care_dryeye.phphttp://www.advocurenf2.org/livingwithnf2_ailments+care_dryeye.php -
7/26/2019 Fisiologi Tear Film
2/14
'ekresi kelenjar lakrimal dipi#u oleh emosi atau iritasi fisik dan menyebabkan air
mata mengalir melimpah melewati tepian palpebra (epifora!. Kelenjar lakrimal
assesorius dikenal sebagai pensekresi dasar. 'ekret yang dihasilkan normalnya
#ukup untuk memelihara kesehatan kornea. ilangnya sel goblet, berakibat
mengeringnya korena meskipun banyak airmata dari kelenjar lakrimal.(Khurana, 200!.
1.2.2 Fungsi Tear Film.
3ir mata membentuk lapisan tipis setebal %40 5m yang menutup epitel kornea
dankonjungti$a(Khurana, 200!.
6ungsi lapisan ultra tipis ini adalah
4! )embuat kornea menjadi permukaan optik yang li#in denganmeniadakan ketidakteraturan minimal di permukaan epitel. -ear film adalah
komponen penting dari the eyes optical system. -ear film dan permukaan
anterior kornea memiliki mekanisme untuk memfokuskan refraksi sekitar
07. 8ahkan sebuah perubahan ke#il pada kestabilan dan $olume tear film
akan sangatmempengaruhi kualitas penglihatan (khususnya pada sensiti$itas
pada kontras!. Tearbreak up menyebabkan aberasi optik yang akan
menurunkan kualitas fokus gambaranyang didapatkan retina. 9leh karena itu,
ketidakteraturan pada tear film preo#ular merupakan penyebab gejala $isual
fatiguedan fotofobia.2! )embasahi dan melindungi permukaan epitel kornea dan konjungti$a yang
lembut. Pergerakan kelopak mata dapat menimbulkan gaya : 4;0 dyne/#m
yang mempengaruhi tear film. ", alergen dan iritan. Tear filmharus memiliki stabilitas untuk
menghadapi paparan lingkungan tersebut. Komponen tear film yang
-
7/26/2019 Fisiologi Tear Film
3/14
berfungsi untuk perlindungan adalah ?g3, laktoferin, liso*im dan en*im
peroksidase yang dapat melawan infeksi bakteri maupun $irus.
-
7/26/2019 Fisiologi Tear Film
4/14
o ?nfeksi atau kerusakan berulang pada kelenjar ini (seperti hordeolum,
kala*ion serta blefaritis! akan menyebabkan gangguan lapisan lemak
sehingga terjadi Clipid deficiency dry eyeC akibat penguapan berlebihan.o 6ungsi
)enghambat penguapan lapisan air mata. )eningkatkan tekanan permukaan.
)elubrikasi kelopak mata.
-
7/26/2019 Fisiologi Tear Film
5/14
Eat anti bakteri la#toferin, lyso*yme, betalysin.
)emberikan permukaan optis yg halus.
)embersihkan debris.
o )ekanisme terbentuknya airmata
Pada saat mengedip dan saat mata terbuka di antara kedipan. Pada saat mata terbuka, lapisan air mata (aAuous! akan berkurang
akibat e$aporasi serta aliran keluar melalui pungtum dan duktus
nasolakrimal.
3pabila mata mulai terasa kering dan terjadi Cdry spotC pada kornea,
mata akan terasa perih, menimbulkan rangsangan pada saraf
sensoris dan terjadi refleks mengedip sehingga lapisan airmata
terbentuk lagi dan seterusnya.
-
7/26/2019 Fisiologi Tear Film
6/14
o
-
7/26/2019 Fisiologi Tear Film
7/14
non%liso*im lain, membentuk mekanisme pertahananpenting terhadap infeksi. Dn*im air
mata lain juga bisa berperan dalam diagnosis berbagaikondisi klinis tertentu, mis.,
he&oseaminidase untuk mendiagnosis penyakit -ay%'a#hs.("aughan, 200!
+ambar 2.44Komposisi air mata
(http//majiidsumardi.blogspot.#om/2044/44/air%mata.html !
Clinical features
Symptoms suggestive of dry eye include irritation,
foreign body (sandy) sensation, feeling of dryness,
itching, non-specific ocular discomfort and
chronically sore eyes not responding to a variety of
drops instilled earlier.Signs of dry eye include: presence of stringy mucus
and particulate matter in the tear film, lustureless
ocular surface, conjunctival xerosis, reduced or absent
marginal tear strip and corneal changes in the form of
punctate epithelial erosions and filaments.
Tear film tests
These include tear film break-up time (!T), "chirmer-# test, vital staining $ith %ose engal, tear levels of
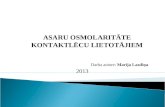
Fig. 15.3. &limination of tears by lacrimal pump mechanism.
lyso'yme and lactoferrin, tear osmolarity and
http://majiidsumardi.blogspot.com/2011/11/air-mata.htmlhttp://majiidsumardi.blogspot.com/2011/11/air-mata.html -
7/26/2019 Fisiologi Tear Film
8/14
dr. prashant goyal
366 Comprehensive *+T**/0
conjunctival impression cytology. *ut of these !T,
"chirmer-# test and %ose engal staining are mostimportant and $hen any t$o of these are positive,
diagnosis of dry eye syndrome is confirmed.
1. Tear film break-up (BUT). #t is the interval bet$een
a complete blink and appearance of first randomly
distributed dry spot on the cornea. #t is noted after
instilling a drop of fluorescein and examining in a
cobalt-blue light of a slit-lamp. !T is an indicator of
ade1uacy of mucin component of tears. #ts normalvalues range from 23 to 43 seconds. 5alues less than
26 seconds imply an unstable tear film.
2.Schirmer-I test. #t measures total tear secretions. #t
is performed $ith the help of a 3 7 43 mm strip of
8hatman-92 filter paper $hich is folded 3 mm from
one end and kept in the lo$er fornix at the junction of
lateral one-third and medial t$o-thirds. The patient isasked to look up and not to blink or close the eyes
(ig. 23.9). fter 3 minutes $etting of the filter paper
strip from the bent end is measured. ;ormal values of
"chirmer-# test are more than 23 mm. 5alues of 3-26
mm are suggestive of moderate to mild
keratoconjunctivitis sicca (? pattern represents mild or
early cases $ith fine punctate stains in the
-
7/26/2019 Fisiologi Tear Film
9/14
interpalpebral area@ >? the moderate cases $ith
extensive staining@ and >? the severe cases $ith
confluent staining of conjunctiva and cornea.
Treatmentt present, there is no cure for dry eye. The follo$ing
treatment modalities have been tried $ith variable
results:
1.Supplementation with tear substitutes. rtificial
tears remains the mainstay in the treatment of dry
eye. These are available as drops, ointments and slo$release
inserts. ostly available artificial tear drops
contain either cellulose derivatives (e.g., 6.A3 to 6.BCmethyl cellulose and 6.4C hypromellose) or polyvinyl
alcohol (2.9C).
2. Topical cyclosporine (6.63C, 6.2C) is reported to
be very effective drug for dry eye in many recent
studies. #t helps by reducing the cell-mediated
inflammation of the lacrimal tissue.
3.ucolytics, such as 3 percent acetylcystine used9 times a day help by dispersing the mucus threads
and decreasing tear viscosity.
4. Topical retinoi!s have recently been reported to
be useful in reversing the cellular changes (s1uamous
metaplasia) occurring in the conjunctiva of dry eye
patients.
5."reser#ation of e$isting tears by re!ucing
e#aporation an! !ecreasing !rainage.
DEvaporation can be reducedby decreasing room
temperature, use of moist chambers and protective
glasses.
DPunctal occlusion to decrease drainage can be
-
7/26/2019 Fisiologi Tear Film
10/14
carried out by collagen implants, cynoacrylate
tissue adhesives, electrocauterisation, argon laser
occlusion and surgical occlusion to decrease the
drainage of tears in patients $ith very severedry eye. (kurana)
acrimal "ystem =ysfunction
4.9.2
-
7/26/2019 Fisiologi Tear Film
11/14
destruction of the lacrimal gland.
G Altered composition of the tear film. The composition
of the tear film can
alter due to vitamin deficiency, medications (such asoral contraceptives
and retinoids), or certain environmental influences (such
as nicotine,
smog, or air conditioning). The tear film breaks up too
1uickly and causes
corneal drying.
=ry eyes can represent a disorder in and of itself.
"ymptoms: +atients complain of burning, reddened eyes,
and excessive lacrimation
(reflex lacrimation) from only slight environmental causes
such as
$ind, cold, lo$humidity, or reading for an extended
period of time. foreignbody sensation is also present. These symptoms may be
accompanied by
intense pain. &yesight is usually minimally compromised
if at all.
=iagnostic considerations: *ften there is a discrepancy
bet$een the minimal
clinical findings that the ophthalmologist can establishand the intense
symptoms reported by the patient. %esults fromSchirmer
tear testing usually
-
7/26/2019 Fisiologi Tear Film
12/14
sho$ reductions of the $atery component of tears, and the
tear rea!"up
time ($hich provides information about the mucin
content of the tear film$hich is important for its stability) is reduced. 5alues of
at least 26 seconds
are normal@ the tear break-up time in keratoconjunctivitis
sicca is less than 3
seconds.
Slit lamp examination$ill reveal dilated conjunctival
vessels and minimal
pericorneal injection. tear film meniscus cannot be
demonstrated on the
lo$er eyelid margin, and the lo$er eyelid $ill push the
conjunctiva along in
folds in front of it.
4 acrimal "ystemang, *phthalmology I A666 Thieme
ll rights reserved. !sage subject to terms and conditions
of license.
F4
#nsevere cases the eye $ill be reddened, and the tear film
$ill contain thick
mucus and small filaments that proceed from a superficialepithelial lesion
(filamentary keratitis@ see ig. 3.11). The corneal lesion
can be demonstrated
-
7/26/2019 Fisiologi Tear Film
13/14
$ith fluorescein d#e. #n less severe cases the eye $ill
only be reddened,
although application of fluorescein dye $ill reveal corneal
lesions (superficialpunctate keratitis@ see p. 24E). The rose engal test (see
p. 3A) and impression
c#tolog# (see p. 34) are additional diagnostic tests that are
useful in evaluating
persistent cases.
Treatment: =epending on the severity of findings,
artificial tear solutions in
varying viscosities are prescribed. These range
fromeyedrops to high-viscosity
long-acting gels that may be applied every hour or every
half hour,
depending on the severity of the disorder. #n persistent
cases, the puncta canbe temporarily closed $ith silicone punctal plugs (ig.
4.11) to at least retain
the fe$tears that are still produced. Surgical oliteration
of the puncta may
be indicated in severe cases.
+atients should also be informed about the possibility of
installing an airhumidifier in the home and redirecting blo$ers in
automobiles to avoid
further drying of the eyes. =ry eyes in $omen may also
be due to hormonal
-
7/26/2019 Fisiologi Tear Film
14/14
changes, and a g#necologist should e consulted
regarding the patient?s hormonal
status.
+rognosis: The prognosis is good for those treatmentsdiscussed here.
o$ever, the disorder cannot be completely healed.
Treatment of dr# e#es.
ig. 4.11 Treatment
can be augmented
by temporarily
closing
the puncta $ith
silicone punctal
plugs.
4.9 acrimal "ystem =ysfunction