Fibromyalgia
40
FIBROMYALGIA Dr Amit Kumar Mallik RIMS, Imphal (INDIA) 07/05/22 1
-
Upload
amit-mallik -
Category
Health & Medicine
-
view
62 -
download
0
Transcript of Fibromyalgia

FIBROMYALGIA
Dr Amit Kumar MallikRIMS, Imphal (INDIA)
05/01/23 1

Introduction
Characterized by chronic widespread musculoskeletal pain associated with considerable distress, generalized fatigue, disturbance of sleep, anxiety and depression.Also known as Neurasthenia or fibrositis
05/01/23 2

FM leads to significant decreased function and work capacity and the quality of life is seriously affected
Although defined primarily as pain syndromes there are associated neuropsychological symptoms
05/01/23 3

EpidemiologyPrevalence rate of 2-3%
Fibromyalgia affects predominantly women in a ratio of 9:1 compared to men
Most patients present with fibromyalgia between the ages of 30–50 years
This disorder is found in most countries, in most ethnic groups, and in all types of climate
05/01/23 4

Proposed etiology of Fibromyalgia
Emerging evidence of genetic component of FM
- Specific gene mutations may predispose individuals to FM
- Polymorphism in Catechol O-methyl transferase(COMT) enzyme gene and serotonin transporter are potentially associated with FM
05/01/23 5

Environmental factors that may trigger the onset of FM
- Physical trauma and injury - Infections (hepatitis C, lyme’s disease) - Psychological stressor
FM may occur concurrently with arthritis (OA), autoimmune diseases (RA,SLE)
05/01/23 6

PathophysiologyAbnormal pain processing
Hyperalgesia
Allodynia
05/01/23 7

Mechanism of decrease pain threshold
•Wind up
•Central sensitization
05/01/23 8

Wind Up• Drs. Price and Staud have demonstrated that
increasing repetitive nociceptive stimuli will activate a wide range of dorsal horn neuronal pain discharges in the CNS called “wind up”
• Temporal summation of pain on repetitive stimulation of peripheral nociceptive afferents
Price, D and Staud, R, J Rheumatol 2005:32(75):22-28
05/01/23 9

• “Wind up” involves recruitment of NMDA pain receptors in the CNS and neural plasticity of nociceptive spinal cord pathway in central sensitization
05/01/23 10

Central sensitization of FM patients
• Increased levels of excitatory neuro-transmitters glutamate and substance P
• Compared with normal controls, CSF levels of substance P are 3-fold higher in FM patients
• There are decreased levels of serotonin and norepinephrine which are needed for pain modulation
05/01/23 11

Neurotransmitters
◦Substance P, an excitatory neurotransmitter which is elevated in CSF of FM patients compared with controls
◦Glutamate acting at the Aᶞ and C ascending pain fibers
1. Russell IJ, et al. Arthritis Rheum. 1994;37:1593-1601. 4. Russell IJ, et al. J Rheumatol. 1992;19:104-109.2. Vaerøy H et al., Pain. 1988. 32:21-26. 5. Russell IJ, et al. Arthritis Rheum. 1992;35:550-556.3. Watkins LR, et al. Brain Res. 1994;664:17-24. 6. Fields HL, et al. Annu Rev Neurosci. 1991;14:219-
245.
05/01/23 12

Serotonin and Norepinephrine
• Serotonin and norepinephrine mediate pain modulation through the descending inhibitory pain pathways in the brain and dorsal horn of the spinal cord
• Dysfunction in fibromyalgia
05/01/23 13

Clinical features
Pain and tenderness “ Pain all over” typically above and below the waist
on both sides and involves the axial skeleton
Neuropshychological symptoms Fatigue, sleep disturbance, cognitive dysfunction,
anxiety and depression
05/01/23 14

Overlapping syndromes- Can overlap in presentation with other chronic
conditions
Comorbid conditions- Often associated with chronic musculoskeletal,
infectious, metabolic or psychiatric conditions
Functional impairment05/01/23 15

05/01/23 16

Associated with
• Chronic fatigue syndrome• Depression• Irritable bowel syndrome• Migraine• Headache• Irritable bladder• Temporomandibular joint pain
05/01/23 17

Diagnostic criteria
The American College of Rheumatology 1990:
(1) A history of widespread pain for 3 month or more
(2) Pain in at least 11 of 18 defined tender point sites on digital palpation with a force of 4 kg with thumb
05/01/23 18

ACR 201O• Widespread Pain Index (WPI)• Symptom Severity Score (SS)
05/01/23 19

Widespread Pain Index (WPI)Pain in any of the ff areas in the last 7 days
• R/L Jaw• Neck• R/L Shoulder• R/L Upper Arm• R/L Forearm• Upper Back
• Chest• Abdomen• Lower Back• R/L Hip• R/L Thighs• R/L Calves
05/01/23 20

Symptom Severity Score
Somatic Symptoms – Have you had any of the following in the last 6 months
• Blurred vision• Tinnitus• Mouth sores• Dry mouth• Headache• Dizziness• Fever• Chest pains• Dyspnea
• Wheezing• Anorexia• Nausea• Diarrhea• Constipation• Itching• Vomiting• Easy bruising• Hair loss
05/01/23 21

• WPI >7 and SS Score > 5• WPI 3-6 and SS Score > 9• Symptoms present for at least 3 months
05/01/23 22

a. Pain in the right side of the body b.Pain in the left side of the body
c. Pain above the waist
d. Pain below the waist
e. Trunk and extremities
05/01/23 23

Sites for control points• Mid forehead
• Junction of proximal 2/3rd and Distal 1/3rd of forearm
• Thumbnail
05/01/23 24

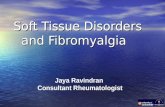
Sites for elicitation of tender points
Pain on digital palpation in at least 11 of the following 18 tender point sites
a. Occiput: bilateral, at the suboccipital muscle insertion
b. Low cervical: bilateral, at the anterior aspect of the intertransverse spaces at C5–7
c. Trapezius: bilateral, at the midpoint of the upper border
05/01/23 25

d. Supraspinatus: bilateral, at the origin, above the scapular spine near the medial border
e. Second rib: bilateral, at the second costochondral junction, just lateral to the junction on the upper surface
f. Lateral epicondyle: bilateral, 2 cm distal to the epicondyle
05/01/23 26

• g.Gluteal: bilateral, in the upper outer quadrant of the buttock
• h.Greater trochanter: bilateral, posterior to the trochanteric prominence
• i.Knee: bilateral, at the medial fat pad proximal to the joint line
05/01/23 27

Tender points
05/01/23 28

05/01/23 29

Differential diagnosis
Inflammatory
Infectious
Non inflammatory
Endocrine
Neurologic diseases
Psychiatric diseases
Drugs05/01/23 30

Investigations
Routine
- CBC, ESR, CRP, TSH
Guided by history and physical examination
-ANA, anti-SSA&SSB, Rh.factor, anti-CCP, CPK, viral and bacterial serologies, spine and joint radiographs
05/01/23 31

ManagementThink of FM as a multisystem disorder with multiple pathways creating dysfunction
◦Non-restorative sleep◦Myofascial pain◦Neuromuscular dysfunction/deconditioning◦Anxiety and reactive depression◦Abnormal pain processing◦Excess sympathetic tone and Autonomic
dysfunction
05/01/23 32

Treatment
Pharmacological treatment
Antidepressants - Amitryptiline - Duloxetine - Milnacipran
-Fluvoxetine
05/01/23 33

Anticonvulsants - Gabapentin - Pregabalin
Glucocorticoids or NSAIDs are not effective in FM
Utilization of single agents to treat multiple symptom domain is strongly encouraged
05/01/23 34

Non pharmacological treatment
1.Self-management strategies - Education and active participation with reassurance
2. Multi component therapy - Comprise of one educational or other psychological therapy and at least one exercise therapy
05/01/23 35

Rehabilitation of FM
Pain reduction modalities
•Cryotherapy
•Therapeutic heat
•Administration of local anesthetics
05/01/23 36

Aerobic and flexibility exercise• Exercise can activate endogenous opioids and reduce
“wind up”
• Low level of exercise
• Progress slowly
05/01/23 37

• Begin with gentle warm up
• Low impact aerobic exercise for atleast 3 time wkly
• Target exercise regimen- 4 to 5 times a wk for at least 20-30 minutes every session
05/01/23 38

Psychological rehabilitation
• Cognitive and behavioral therapy
• Relaxation training
• Biofeedback
• Stress management
05/01/23 39

05/01/23 40