Fibroblast Growth Factor 23, Parathyroid Hormone, and 1α,25-Dihydroxyvitamin D in Surgically...
6
Mayo Clin Proc. • December 2004;79(12):1508-1513 • www.mayo.edu/proceedings 1508 ORIGINAL ARTICLE From the Division of Endocrinology, Diabetes, Metabolism, and Nutrition and Internal Medicine (P.J.T., B.L.C., R.K.), Department of Laboratory Medicine and Pathology (R.J.S.), and Division of Nephrology and Hypertension (R.K.), Mayo Clinic College of Medicine, Rochester, Minn. Address reprint requests and correspondence to Rajiv Kumar, MBBS, Division of Nephrology and Hypertension, Mayo Clinic College of Medicine, 200 First St SW, Rochester, MN 55905 (e-mail: [email protected]). © 2004 Mayo Foundation for Medical Education and Research Fibroblast Growth Factor 23, Parathyroid Hormone, and 1α,25-Dihydroxyvitamin D in Surgically Treated Primary Hyperparathyroidism PETER J. TEBBEN, MD; RAVINDER J. SINGH, PHD; BART L. CLARKE, MD; AND RAJIV KUMAR, MBBS OBJECTIVE: To determine whether fibroblast growth factor 23 (FGF23) contributes to the hypophosphatemia of primary hyper- parathyroidism. PATIENTS AND METHODS: Thirteen adult patients with primary hyperparathyroidism had serum collected before and after parathy- roidectomy for analysis of inorganic phosphorus, calcium, 1α,25- dihydroxyvitamin D (1α,25[OH] 2 D), parathyroid hormone (PTH), FGF23, creatinine, and bone-specific alkaline phosphatase (BSAP). Patients were recruited between July 24, 2003, and February 11, 2004. RESULTS: Before surgery, patients had elevated serum calcium and PTH concentrations. Serum phosphorus concentrations were in the low-normal range. The FGF23 concentrations were not elevated in patients with primary hyperparathyroidism compared with healthy controls. Within 24 hours of surgery, serum calcium, PTH, 1α,25(OH) 2 D, and BSAP concentrations were lower (P<.002 for all) and phosphorus concentrations were higher (P=.003) than in the preoperative state. The FGF23 concentrations were similar 1 day and 6 weeks after surgery. The FGF23 concentrations did not correlate with serum phosphorus, calcium, PTH, 1α,25(OH) 2 D, creatinine, or BSAP concentrations in the preoperative or postop- erative state. CONCLUSION: Parathyroid hormone is the major regulator of se- rum phosphorus concentrations in patients with primary hyperpara- thyroidism. Fibroblast growth factor 23 does not appear to play a role in phosphorus homeostasis in patients with surgically treated primary hyperparathyroidism. Mayo Clin Proc. 2004;79(12):1508-1513 1α,25(OH) 2 D = 1α,25-dihydroxyvitamin D; BSAP = bone-specific alka- line phosphatase; FGF23 = fibroblast growth factor 23; PTH = parathy- roid hormone P rimary hyperparathyroidism is characterized by ele- vated serum calcium concentrations and elevated or inappropriately normal parathyroid hormone (PTH) concentrations. 1-7 Patients with primary hyperparathy- roidism have hypercalcemia, low or low-normal phospho- rus levels, a decreased renal tubular maximum for phos- phate, and high or high-normal 1α,25-dihydroxyvitamin D (1α,25[OH] 2 D) concentrations. 1,6-11 Serum inorganic phos- phorus levels are generally low or in the low-normal range in such patients as a result of inhibition of renal proximal tubule phosphorus reabsorption, which is mediated by an increase in renal cyclic adenosine monophosphate genera- tion. 8,9,12-17 The increase in cyclic adenosine monophos- phate is associated with a reduction in the amount of the sodium phosphate IIa cotransporter in the brush border of the renal proximal tubule epithelium 18 and a routing of brush border sodium phosphate IIa cotransporter proteins to lysosomes for degradation. 19,20 Parathyroid hormone also stimulates the conversion of 25-hydroxyvitamin D to the biologically active metabolite 1α,25(OH) 2 D. 21-24 1α,25- Dihydroxyvitamin D enhances calcium and phosphorus absorption from the gastrointestinal tract and the renal tubule, thereby increasing serum calcium and phosphorus concentrations. 25-29 Recently, a novel protein, fibroblast growth factor 23 (FGF23), was implicated in the pathogenesis of hypophos- phatemia and renal phosphate wasting in patients with autosomal dominant hypophosphatemic rickets, in some patients with X-linked hypophosphatemic rickets, and in patients with tumor-induced osteomalacia. 30-35 However, the role of FGF23 in normal phosphate homeostasis and in the disordered phosphate homeostasis in hyperparathyroid- ism remains unclear. A recent study showed that FGF23 does not increase in humans after administration of a high- phosphate diet. 36 We previously showed that serum FGF23 concentrations are elevated in patients with humoral hyper- calcemia of malignancy who have hypercalcemia and hypophosphatemia. 37 In that same report, we showed that FGF23 concentrations were higher in some patients with primary hyperparathyroidism, but as a group, the patients with primary hyperparathyroidism had FGF23 concentra- tions similar to those in healthy individuals. Interestingly, in the patients with primary hyperparathyroidism and hu- moral hypercalcemia of malignancy, there was no correla- tion between FGF23 and serum phosphorus concentra- tions. A recent report, published as an abstract, showed that 5 patients with primary hyperparathyroidism had concen- trations of FGF23 that were somewhat elevated compared with control values, but the increase was not statistically significant. 38 In these patients, however, parathyroidec- tomy was associated with a statistically significant de- crease in FGF23 concentrations. Thus, it is unclear whether For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Transcript of Fibroblast Growth Factor 23, Parathyroid Hormone, and 1α,25-Dihydroxyvitamin D in Surgically...

Mayo Clin Proc. • December 2004;79(12):1508-1513 • www.mayo.edu/proceedings1508
FGF23 IN PRIMARY HYPERPARATHYROIDISMORIGINAL ARTICLE
From the Division of Endocrinology, Diabetes, Metabolism, and Nutrition andInternal Medicine (P.J.T., B.L.C., R.K.), Department of Laboratory Medicineand Pathology (R.J.S.), and Division of Nephrology and Hypertension (R.K.),Mayo Clinic College of Medicine, Rochester, Minn.
Address reprint requests and correspondence to Rajiv Kumar, MBBS, Divisionof Nephrology and Hypertension, Mayo Clinic College of Medicine, 200 First StSW, Rochester, MN 55905 (e-mail: [email protected]).
© 2004 Mayo Foundation for Medical Education and Research
Fibroblast Growth Factor 23, Parathyroid Hormone,and 1ααααα,25-Dihydroxyvitamin D in
Surgically Treated Primary Hyperparathyroidism
PETER J. TEBBEN, MD; RAVINDER J. SINGH, PHD; BART L. CLARKE, MD; AND RAJIV KUMAR, MBBS
OBJECTIVE: To determine whether fibroblast growth factor 23(FGF23) contributes to the hypophosphatemia of primary hyper-parathyroidism.
PATIENTS AND METHODS: Thirteen adult patients with primaryhyperparathyroidism had serum collected before and after parathy-roidectomy for analysis of inorganic phosphorus, calcium, 1ααααα,25-dihydroxyvitamin D (1ααααα,25[OH]2D), parathyroid hormone (PTH),FGF23, creatinine, and bone-specific alkaline phosphatase(BSAP). Patients were recruited between July 24, 2003, andFebruary 11, 2004.
RESULTS: Before surgery, patients had elevated serum calciumand PTH concentrations. Serum phosphorus concentrations werein the low-normal range. The FGF23 concentrations were notelevated in patients with primary hyperparathyroidism comparedwith healthy controls. Within 24 hours of surgery, serum calcium,PTH, 1ααααα,25(OH)2D, and BSAP concentrations were lower (P<.002for all) and phosphorus concentrations were higher (P=.003) thanin the preoperative state. The FGF23 concentrations were similar1 day and 6 weeks after surgery. The FGF23 concentrations didnot correlate with serum phosphorus, calcium, PTH, 1ααααα,25(OH)2D,creatinine, or BSAP concentrations in the preoperative or postop-erative state.
CONCLUSION: Parathyroid hormone is the major regulator of se-rum phosphorus concentrations in patients with primary hyperpara-thyroidism. Fibroblast growth factor 23 does not appear to play arole in phosphorus homeostasis in patients with surgically treatedprimary hyperparathyroidism.
Mayo Clin Proc. 2004;79(12):1508-1513
1ααααα,25(OH)2D = 1ααααα,25-dihydroxyvitamin D; BSAP = bone-specific alka-line phosphatase; FGF23 = fibroblast growth factor 23; PTH = parathy-roid hormone
Primary hyperparathyroidism is characterized by ele-vated serum calcium concentrations and elevated
or inappropriately normal parathyroid hormone (PTH)concentrations.1-7 Patients with primary hyperparathy-roidism have hypercalcemia, low or low-normal phospho-rus levels, a decreased renal tubular maximum for phos-phate, and high or high-normal 1α,25-dihydroxyvitamin D(1α,25[OH]
2D) concentrations.1,6-11 Serum inorganic phos-
phorus levels are generally low or in the low-normal rangein such patients as a result of inhibition of renal proximaltubule phosphorus reabsorption, which is mediated by anincrease in renal cyclic adenosine monophosphate genera-tion.8,9,12-17 The increase in cyclic adenosine monophos-phate is associated with a reduction in the amount of thesodium phosphate IIa cotransporter in the brush border ofthe renal proximal tubule epithelium18 and a routing ofbrush border sodium phosphate IIa cotransporter proteinsto lysosomes for degradation.19,20 Parathyroid hormone alsostimulates the conversion of 25-hydroxyvitamin D to thebiologically active metabolite 1α,25(OH)
2D.21-24 1α,25-
Dihydroxyvitamin D enhances calcium and phosphorusabsorption from the gastrointestinal tract and the renaltubule, thereby increasing serum calcium and phosphorusconcentrations.25-29
Recently, a novel protein, fibroblast growth factor 23(FGF23), was implicated in the pathogenesis of hypophos-phatemia and renal phosphate wasting in patients withautosomal dominant hypophosphatemic rickets, in somepatients with X-linked hypophosphatemic rickets, and inpatients with tumor-induced osteomalacia.30-35 However,the role of FGF23 in normal phosphate homeostasis and inthe disordered phosphate homeostasis in hyperparathyroid-ism remains unclear. A recent study showed that FGF23does not increase in humans after administration of a high-phosphate diet.36 We previously showed that serum FGF23concentrations are elevated in patients with humoral hyper-calcemia of malignancy who have hypercalcemia andhypophosphatemia.37 In that same report, we showed thatFGF23 concentrations were higher in some patients withprimary hyperparathyroidism, but as a group, the patientswith primary hyperparathyroidism had FGF23 concentra-tions similar to those in healthy individuals. Interestingly,in the patients with primary hyperparathyroidism and hu-moral hypercalcemia of malignancy, there was no correla-tion between FGF23 and serum phosphorus concentra-tions. A recent report, published as an abstract, showed that5 patients with primary hyperparathyroidism had concen-trations of FGF23 that were somewhat elevated comparedwith control values, but the increase was not statisticallysignificant.38 In these patients, however, parathyroidec-tomy was associated with a statistically significant de-crease in FGF23 concentrations. Thus, it is unclear whether
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • December 2004;79(12):1508-1513 • www.mayo.edu/proceedings 1509
FGF23 IN PRIMARY HYPERPARATHYROIDISM
FGF23 plays a role in the hypophosphatemia of primaryhyperparathyroidism and in the altered synthesis of1α,25(OH)
2D seen in this condition. This study aims to
determine whether FGF23 contributes to the hypophos-phatemia of primary hyperparathyroidism.
PATIENTS AND METHODS
This study was approved by the Mayo Foundation Institu-tional Review Board, and all patients provided writteninformed consent. Thirteen adults with primary hyper-parathyroidism were recruited for the study and under-went physical and biochemical examination between July24, 2003, and February 11, 2004. These patients werepreviously scheduled for surgical treatment of their para-thyroid disease. We measured serum FGF23, phospho-rus, calcium, PTH, and 1α,25(OH)
2D concentrations in
these patients before and after surgery for removal ofadenomatous or hyperplastic parathyroid glands. Partici-pation required an elevated serum PTH level (referenceranges shown parenthetically) (1.0-5.2 pmol/L), an el-evated calcium level (8.9-10.1 mg/dL), and a normalcreatinine level (0.9-1.4 mg/dL in men and 0.7-1.2 mg/dLin women). Serum samples were collected before, themorning after, and at least 6 weeks after surgery. Serumwas stored at –80°C until analysis was performed. Datawere available for all patients before surgery and 1 dayafter surgery. Attempts were made to collect serum fromall patients 6 weeks after surgery; however, only 8 re-turned the final sample.
BIOCHEMICAL ANALYSES
Serum FGF23 was determined using a 2-site enzyme-linked immunosorbent assay according to the manu-facturer’s instructions (Immutopics, San Clemente, Calif).Epitopes for the capture and detection antibody are locatedwithin the carboxy-terminal portion of the protein. Theinterassay and intra-assay coefficient of variation was lessthan 8% for values between 50 and 150 relative units (RU)/mL. The sensitivity of the assay was 3.0 RU/mL. Thereference range for serum FGF23 concentrations was de-rived from 80 healthy controls (41 men and 39 women).
Serum PTH concentration was determined by animmunochemiluminometric assay.39 A plastic bead coatedwith the capture antibody against human PTH 44-68 wasincubated with the patients’ serum and a chemiluminescent-labeled antibody against PTH 1-34. The interassay and intra-assay coefficients of variation were 12.7% and 6.6%, respec-tively. The sensitivity of the assay was 0.2 pmol/L.
The 1α,25(OH)2D levels were measured using a radioim-
munoassay kit (DiaSorin, Stillwater, Minn). The interassayand intra-assay coefficients of variation were 15.4% and
12.4%, respectively, and the sensitivity was 10 pg/mL.Bone-specific alkaline phosphatase (BSAP) was measuredusing an immunoenzymatic assay (Beckman-Coulter,Brea, Calif). The interassay and intra-assay coefficients ofvariation were 8.4% and 4.7%, respectively, and the sensi-tivity was 2 µg/L. Serum creatinine, calcium, and phospho-rus were measured using standard laboratory techniques inthe Mayo Clinic laboratories in Rochester, Minn.
STATISTICAL ANALYSES
Statistical analysis was performed using the Wilcoxonsigned rank test, and P<.05 was considered statisticallysignificant. All data are expressed as mean ± SEM. Threepatients had PTH concentrations below the limit of detec-tion for the assay (0.2 pmol/L), and 1 patient had an FGF23concentration below the limit of detection for the assay (3RU/mL). The values of 0.2 pmol/L for PTH and 3 RU/mLfor FGF23 were used for these patients in the statisticalanalysis.
RESULTS
All patients had surgically proven primary hyperparathy-roidism; 10 patients had a solitary adenoma, and 3 hadparathyroid hyperplasia. Two patients with parathyroid hy-perplasia had 3 glands removed, and the other patient had 2glands removed. All patients were cured of their primaryhyperparathyroidism at surgery.
SERUM PTH, CALCIUM, AND PHOSPHORUS
As expected, a decrease in serum PTH and calcium concen-trations and an increase in phosphorus concentrations wereobserved after surgery (Table 1). The mean ± SEM preop-erative serum PTH level was 10.9±2.2 pmol/L. After sur-gery, the PTH level decreased to 0.9±0.2 pmol/L (P=.002)and then increased to 5.2±0.7 pmol/L (P=.04) 6 weeks aftersurgery (Figure 1). The mean serum calcium level beforesurgery was 11.0±0.2 mg/dL, which decreased to 9.4±0.2mg/dL (P=.002) and then to 8.7±0.2 mg/dL (P=.01) by 1day and 6 weeks postoperatively, respectively. The meanserum phosphorus level before surgery was 3.0±0.1 mg/dL,which increased to 3.6±0.2 mg/dL (P=.003) and 3.2±0.3mg/dL (P=.78) by 1 day and 6 weeks postoperatively,respectively.
1ααααα,25(OH)2D AND BSAPThe serum 1α,25(OH)
2D concentration before surgery was
56.8±7.3 pg/mL, which decreased by 39% (P=.002) 1 dayafter surgery to 34.9±5.1 pg/mL (Figure 1); at 6 weeks, the1α,25(OH)
2D concentration was 42.5±8.6 pg/mL. The se-
rum BSAP concentration before surgery was 19.5±2.1 µg/L, which decreased to 16.7±2.0 µg/L (P=.002) and then to
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • December 2004;79(12):1508-1513 • www.mayo.edu/proceedings1510
FGF23 IN PRIMARY HYPERPARATHYROIDISM
TABLE 1. Change in Serum Analytes After Surgical Treatment in PatientsWith Primary Hyperparathyroidism*†
Preoperative Mean change before Mean change before tovalues to 1 d after surgery P value 6 wk after surgery P value
PTH (pmol/L) 10.9 ±2.2 –10.0±2.1 .002 –5.7±1.4 .04Calcium (mg/dL) 11.0±0.2 –1.6±0.2 .002 –2.3±0.3 .01Phosphorus (mg/dL) 3.0±0.1 +0.6±0.1 .003 +0.2±0.4 .781α,25(OH)2D (pg/mL) 56.8±7.3 –21.9±3.0 .002 –14.3±7.4 .18BSAP (µg/L) 19.5±2.1 –2.8±0.5 .002 –5.6±0.7 .01FGF23 (RU/mL) 167±117 –49±86 .86 –37±121 .21Creatinine (mg/dL) 1.0±0.0 0±0 … 0±0 …
*Wilcoxon signed rank test was used to compare presurgical to 1-day and 6-week postsurgical values.†Values are mean ± SEM unless indicated otherwise. 1α,25(OH)2D = 1α,25-dihydroxyvitamin D; BSAP = bone-
specific alkaline phosphatase; FGF23 = fibroblast growth factor 23; PTH = parathyroid hormone.
13.9±1.7 µg/L (P=.01) 1 day and 6 weeks postoperatively,respectively. The 1α,25(OH)
2D and BSAP concentrations
did not change significantly between the 1-day and 6-weekpostoperative values.
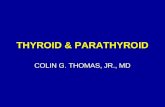
FIBROBLAST GROWTH FACTOR 23Preoperative, 1-day postoperative, and 6-week postopera-tive mean ± SEM serum FGF23 values were 167±117 RU/
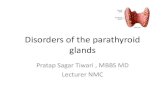
mL, 117±47 RU/mL, and 130±72 RU/mL, respectively.Changes in FGF23 concentrations for individual patientsare shown in Figure 2. There was no significant differencein the mean FGF23 concentration at any time point. Usinglog ratios of the preoperative and 1-day postoperative data,there was no correlation between FGF23 and serum PTH,phosphorus (Figure 3), calcium, 1α,25(OH)
2D, BSAP, or
creatinine. Some patients with primary hyperparathyroidism
FIGURE 1. Serum inorganic phosphorus (upper left), calcium (upper right), parathyroid hormone (PTH) (lower left), and 1α,25-dihydroxyvitamin D (1α,25[OH]2D) (lower right) concentrations before, 1 day after, and 6 weeks after parathyroidectomy.
0
1
2
3
4
Before
Phos
phor
us (
mg/
dL)
PTH
(pm
ol/L
)
Cal
cium
(m
g/dL
)1
α,25(O
H) 2
D (pg
/mL)
1 d after 6 wk after Before 1 d after 6 wk after
Before 1 d after 6 wk after Before 1 d after 6 wk after
P=.003
P=.78
0
2
4
6
8
10
12 P=.002
P=.01
0
2
4
6
8
10
12
14
16P=.002
P=.04
0
10
20
30
40
50
60
70 P=.18P=.002
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • December 2004;79(12):1508-1513 • www.mayo.edu/proceedings 1511
FGF23 IN PRIMARY HYPERPARATHYROIDISM
1
10
100
1000
10,000
Before (n=13)
FGF2
3 (
RU
/mL)
1 d after (n=13) 6 wk after (n=8)
had higher FGF23 concentrations compared with healthycontrols (35.6±27.4 RU/mL). However, as a group there wasno statistical difference between the patients before or aftersurgery compared with the healthy population.
DISCUSSION
After parathyroidectomy, mean serum PTH, calcium, and1α,25(OH)
2D concentrations decreased by 92%, 15%, and
39%, respectively, whereas phosphorus concentrations in-creased by 20%. The FGF23 concentrations did not changesignificantly. The increase in serum phosphorus concentra-tions after parathyroidectomy is likely due to a reduction inrenal phosphate excretion. The decrease in 1α,25(OH)
2D
concentrations 1 day after surgery is consistent with the
reduced PTH concentrations and increased circulatingphosphorus concentrations.21,40 One day after surgery, thedecrease in 1α,25(OH)
2D concentrations would be ex-
pected to reduce serum phosphorus concentrations by re-ducing intestinal phosphorus absorption and renal phos-phate conservation, but this effect is offset by the reductionin PTH concentrations. Of note, by 6 weeks, 1α,25(OH)
2D
concentrations increased along with PTH. The increase inPTH concentrations may have been secondary to inad-equate postoperative calcium and/or vitamin D supplemen-tation or a response to previously inadequate PTH secretionimmediately after surgery.
Some patients with primary hyperparathyroidism haveelevated FGF23 concentrations compared with healthycontrols. However, as a group, the concentrations are notstatistically different than those in controls. These resultsare similar to those previously published by us37 and byKelly et al,38 who showed that 5 patients with primaryhyperparathyroidism had FGF23 concentrations of205±117 RU/mL, a value statistically similar to that seenin controls.
We previously showed that FGF23 concentrations arenot related to serum phosphorus concentrations in patientswith primary hyperparathyroidism.37 In the current report,we confirm our previous findings and show that FGF23values do not change after surgical cure of primary hyper-parathyroidism. However, Kelly et al38 showed a decreasein serum FGF23 levels after surgical treatment of primaryhyperparathyroidism. The difference in the 2 studies couldbe due to differences in the populations studied. The diag-nostic criteria used to define primary hyperparathyroidismand other patient characteristics are unclear in the abstract
FIGURE 2. Change in serum fibroblast growth factor 23 (FGF23)concentration in each patient after parathyroidectomy. RU = relativeunit.
FIGURE 3. Correlations are expressed as the log of the ratio between the preoperative and postoperative values. P=.69 for thecorrelation between fibroblast growth factor 23 (FGF23) and parathyroid hormone (PTH) (left) and P=.82 for the correlation betweenFGF23 and phosphorus (right). RU = relative unit.
–0.20
–0.15
–0.10
–0.05
0.00
0.05
–0.80 –0.60 –0.40 –0.20 0.00 0.20 0.40 0.60
Log FGF23 (RU/mL)
Log
phos
phor
us (
mg/
dL)
R=0.0747
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
–0.80 –0.60 –0.40 –0.20 0.00 0.20 0.40 0.60
Log FGF23 (RU/mL)
Log
PTH
(pm
ol/L
)
R=0.1298
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • December 2004;79(12):1508-1513 • www.mayo.edu/proceedings1512
FGF23 IN PRIMARY HYPERPARATHYROIDISM
by Kelly et al.38 In vivo studies suggest that FGF23 inhibitsthe expected increase in 25-hydroxyvitamin D 1α-hydroxy-lase activity and 1α,25(OH)
2D concentrations in response to
hypophosphatemia.41,42 The lack of correlation betweenFGF23 and 1α,25(OH)
2D concentrations in the current study
implies that vitamin D metabolism is not affected by FGF23in patients with primary hyperparathyroidism.
Although FGF23 is clearly involved in the pathogenesisof disorders associated with hypophosphatemia,33,34,43-45 therole of FGF23 in normal physiology has not yet beenestablished clearly. A recent report involving 6 healthymales failed to show any changes in serum FGF23 concen-trations after either a high- or low-phosphate diet.36 This isin contrast to a previous report of FGF23 concentrationsincreasing slightly with escalating oral phosphate intake inhealthy volunteers.46 The FGF23 concentrations are corre-lated with phosphorus in patients with various degrees ofrenal failure, but it is unknown if this is due to a physiologi-cal response to hyperphosphatemia, a decreased renalclearance of FGF23, or increased circulating concentra-tions of FGF23 fragments.36
CONCLUSION
Our data show that FGF23 concentrations do not decreaseafter surgical cure of hyperparathyroidism, thus demon-strating that FGF23 is not regulated by PTH in patientswith primary hyperparathyroidism. In patients with surgi-cally treated primary hyperparathyroidism, PTH is the ma-jor regulator of serum phosphorus concentrations.
REFERENCES1. Albright F. A page out of the history of hyperparathyroidism. J Clin
Endocrinol Metab. 1948;8:637-657.2. Arnaud CD, Tsao HS, Littledike T. Radioimmunoassay of human para-
thyroid hormone in serum. J Clin Invest. 1971;50:21-34.3. Duh QY, Arnaud CD, Levin KE, Clark OH. Parathyroid hormone:
before and after parathyroidectomy. Surgery. 1986;100:1021-1031.4. Manning RM, Hendy GN, Papapoulos SE, O’Riordan JL. Development
of homologous immunological assays for human parathyroid hormone. JEndocrinol. 1980;85:161-170.
5. Abbott SR, Nissenson RA, Teitelbaum AP, Clark OH, Arnaud CD.Biologically active parathyroid hormone in human hyperparathyroid serum:assay and characterization. Trans Assoc Am Physicians. 1980;93:192-202.
6. Arnaud CD. Parathyroid hormone: coming of age in clinical medicine[editorial]. Am J Med. 1973;55:577-581.
7. Bauer W, Federman DD. Hyperparathyroidism epitomized: the case ofCaptain Charles E. Martell. Metabolism. 1962;11:21-29.
8. Diaz-Buxo JA, Knox FG. Effects of parathyroid hormone on renalfunction. Mayo Clin Proc. 1975;50:537-541.
9. Knox FG, Greger RF, Lang FC, Marchand GR. Renal handling ofphosphate: update. Adv Exp Med Biol. 1977;81:3-14.
10. Broadus AE, Horst RL, Lang R, Littledike ET, Rasmussen H. Theimportance of circulating 1,25-dihydroxyvitamin D in the pathogenesis ofhypercalciuria and renal-stone formation in primary hyperparathyroidism. NEngl J Med. 1980;302:421-426.
11. Broadus AE, Horst RL, Littledike ET, Mahaffey JE, Rasmussen H.Primary hyperparathyroidism with intermittent hypercalcaemia: serial obser-
vations and simple diagnosis by means of an oral calcium tolerance test. ClinEndocrinol (Oxf). 1980;12:225-235.
12. Chase LR, Aurbach GD. Renal adenyl cyclase: anatomically separatesites for parathyroid hormone and vasopressin. Science. 1968;159:545-547.
13. Chase LR, Melson GL, Aurbach GD. Pseudohypoparathyroidism: defec-tive excretion of 3',5'-AMP in response to parathyroid hormone. J Clin Invest.1969;48:1832-1844.
14. Aurbach GD, Keutmann HT, Niall HD, et al. Structure, synthesis, andmechanism of action of parathyroid hormone. Recent Prog Horm Res. 1972;28:353-398.
15. Mallette LE, Bilezikian JP, Heath DA, Aurbach GD. Primary hyperpara-thyroidism: clinical and biochemical features. Medicine (Baltimore). 1974;53:127-146.
16. Knox FG, Schneider EG, Willis LR, Strandhoy JW, Ott CE. Site andcontrol of phosphate reabsorption by the kidney [editorial]. Kidney Int. 1973;3:347-353.
17. Knox FG, Osswald H, Marchand GR, et al. Phosphate transport along thenephron. Am J Physiol. 1977;233:F261-F268.
18. Traebert M, Roth J, Biber J, Murer H, Kaissling B. Internalization ofproximal tubular type II Na-P(i) cotransporter by PTH: immunogold electronmicroscopy. Am J Physiol Renal Physiol. 2000;278:F148-F154.
19. Pfister MF, Ruf I, Stange G, et al. Parathyroid hormone leads to thelysosomal degradation of the renal type II Na/Pi cotransporter. Proc Natl AcadSci U S A. 1998;95:1909-1914.
20. Keusch I, Traebert M, Lotscher M, Kaissling B, Murer H, Biber J.Parathyroid hormone and dietary phosphate provoke a lysosomal routingof the proximal tubular Na/Pi-cotransporter type II. Kidney Int. 1998;54:1224-1232.
21. Murayama A, Takeyama K, Kitanaka S, et al. Positive and negativeregulations of the renal 25-hydroxyvitamin D3 1alpha-hydroxylase gene byparathyroid hormone, calcitonin, and 1alpha,25(OH)2D3 in intact animals.Endocrinology. 1999;140:2224-2231.
22. Garabedian M, Holick MF, DeLuca HF, Boyle IT. Control of 25-hydroxycholecalciferol metabolism by parathyroid glands. Proc Natl Acad SciU S A. 1972;69:1673-1676.
23. DeLuca HF, Schnoes HK. Metabolism and mechanism of action ofvitamin D. Annu Rev Biochem. 1976;45:631-666.
24. DeLuca HF, Schnoes HK. Vitamin D: recent advances. Annu RevBiochem. 1983;52:411-439.
25. Tanaka Y, DeLuca HF, Omdahl J, Holick MF. Mechanism of action of1,25-dihydroxycholecalciferol on intestinal calcium transport. Proc Natl AcadSci U S A. 1971;68:1286-1288.
26. Omdahl J, Holick M, Suda T, Tanaka Y, DeLuca HF. Biological activityof 1,25-dihydroxycholecalciferol. Biochemistry. 1971;10:2935-2940.
27. Tanaka Y, DeLuca HF. Role of 1,25-dihydroxyvitamin D3 in maintain-ing serum phosphorus and curing rickets. Proc Natl Acad Sci U S A. 1974;71:1040-1044.
28. Johnson JA, Kumar R. Renal and intestinal calcium transport: roles ofvitamin D and vitamin D-dependent calcium binding proteins. Semin Nephrol.1994;14:119-128.
29. Kaune R, Kassianoff I, Schroder B, Harmeyer J. The effects of 1,25-dihydroxyvitamin D-3 deficiency on Ca(2+)-transport and Ca(2+)-uptake intobrush-border membrane vesicles from pig small intestine. Biochim BiophysActa. 1992;1109:187-194.
30. Jonsson KB, Zahradnik R, Larsson T, et al. Fibroblast growth factor 23 inoncogenic osteomalacia and X-linked hypophosphatemia. N Engl J Med. 2003;348:1656-1663.
31. Hoogendoorn EH, White KE, Econs MJ, Hermus AR. Hypophos-phatemia, osteomalacia and proximal muscle weakness treated by surgery[letter]. Clin Endocrinol (Oxf). 2003;58:796-797.
32. Nelson AE, Bligh RC, Mirams M, et al. Fibroblast growth factor 23: anew clinical marker for oncogenic osteomalacia. J Clin Endocrinol Metab.2003;88:4088-4094.
33. Schiavi SC, Kumar R. The phosphatonin pathway: new insights inphosphate homeostasis. Kidney Int. 2004;65:1-14.
34. Kumar R. New insights into phosphate homeostasis: fibroblast growthfactor 23 and frizzled-related protein-4 are phosphaturic factors derived fromtumors associated with osteomalacia. Curr Opin Nephrol Hypertens. 2002;11:547-553.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • December 2004;79(12):1508-1513 • www.mayo.edu/proceedings 1513
FGF23 IN PRIMARY HYPERPARATHYROIDISM
35. Quarles LD. FGF23, PHEX, and MEPE regulation of phosphate homeo-stasis and skeletal mineralization. Am J Physiol Endocrinol Metab. 2003;285:E1-E9.
36. Larsson T, Nisbeth U, Ljunggren O, Juppner H, Jonsson KB. Circu-lating concentration of FGF-23 increases as renal function declines in patientswith chronic kidney disease, but does not change in response to variation inphosphate intake in healthy volunteers. Kidney Int. 2003;64:2272-2279.
37. Singh RJ, Kumar R. Fibroblast growth factor 23 concentrations in hu-moral hypercalcemia of malignancy and hyperparathyroidism. Mayo ClinProc. 2003;78:826-829.
38. Kelly TG, Mitnick M, Insogna KL, Carpenter TO. FGF23 in rickets andprimary hyperparathyroidism: evidence for PTH regulation of circulatingFGF23 levels [abstract]. Presented at: The Endocrine Society 85th AnnualMeeting; Philadelphia, Pa; June 19-22, 2003.
39. Klee GG, Preissner CM, Schryver PG, Taylor RL, Kao PC. Multisiteimmunochemiluminometric assay for simultaneously measuring whole-mol-ecule and amino-terminal fragments of human parathyrin. Clin Chem.1992;38:628-635.
40. Tanaka Y, DeLuca HF. The control of 25-hydroxyvitamin D metabolismby inorganic phosphorus. Arch Biochem Biophys. 1973;154:566-574.
41. Bai XY, Miao D, Goltzman D, Karaplis AC. The autosomal dominanthypophosphatemic rickets R176Q mutation in fibroblast growth factor 23resists proteolytic cleavage and enhances in vivo biological potency. J BiolChem. 2003;278:9843-9849.
42. Saito H, Kusano K, Kinosaki M, et al. Human fibroblast growth factor-23 mutants suppress Na+-dependent phosphate co-transport activity and1alpha,25-dihydroxyvitamin D3 production. J Biol Chem. 2003;278:2206-2211.
43. Bowe AE, Finnegan R, Jan de Beur SM, et al. FGF-23 inhibits renaltubular phosphate transport and is a PHEX substrate. Biochem Biophys ResCommun. 2001;284:977-981.
44. Kumar R. Tumor-induced osteomalacia and the regulation of phosphatehomeostasis. Bone. 2000;27:333-338.
45. Kumar R. Phosphatonin—a new phosphaturetic hormone? (lessons fromtumour-induced osteomalacia and X-linked hypophosphataemia) [editorial].Nephrol Dial Transplant. 1997;12:11-13.
46. Allen HC, Whybro A, Barker ME, Eastell R, Blumsohn A. Endocrineresponse to escalating-dose phosphate supplementation in men: is FGF-23phosphatonin? [abstract]. J Bone Miner Res. 2002;17(suppl 1):S159. Ab-stract 1144.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.