
Fellow Seminar
94
Fellow Seminar •Topic: Vitamin D: a pleiotropic hormone Comment 洪洪洪 洪洪 : 洪洪洪洪: F2 洪洪洪 洪洪洪洪: 99-09-15
-
Upload
noelani-shelton -
Category
Documents
-
view
33 -
download
1
description
Fellow Seminar. Topic: Vitamin D: a pleiotropic hormone Comment :洪振傑 醫師 報告人員: F2 張春偉 報告時間: 99-09-15. OUTLINE. VITAMIN D – NORMAL METABOLISM VITAMIN D IN BONE & CALCIUM HOMEOSTASIS VITAMIN D & CANCER VITAMIN D AS IMMUNE MODULATOR CARDIOVASCULAR & METABOLIC ACTIONS RENAL PROTECTION - PowerPoint PPT Presentation
Transcript of Fellow Seminar
Fellow Seminar
• Topic: Vitamin D: a pleiotropic hormone
Comment :洪振傑 醫師 報告人員: F2 張春偉報告時間: 99-09-15
OUTLINE
• VITAMIN D – NORMAL METABOLISM• VITAMIN D IN BONE & CALCIUM
HOMEOSTASIS• VITAMIN D & CANCER• VITAMIN D AS IMMUNE MODULATOR• CARDIOVASCULAR & METABOLIC
ACTIONS• RENAL PROTECTION• CLINICAL PERSPECTIVES
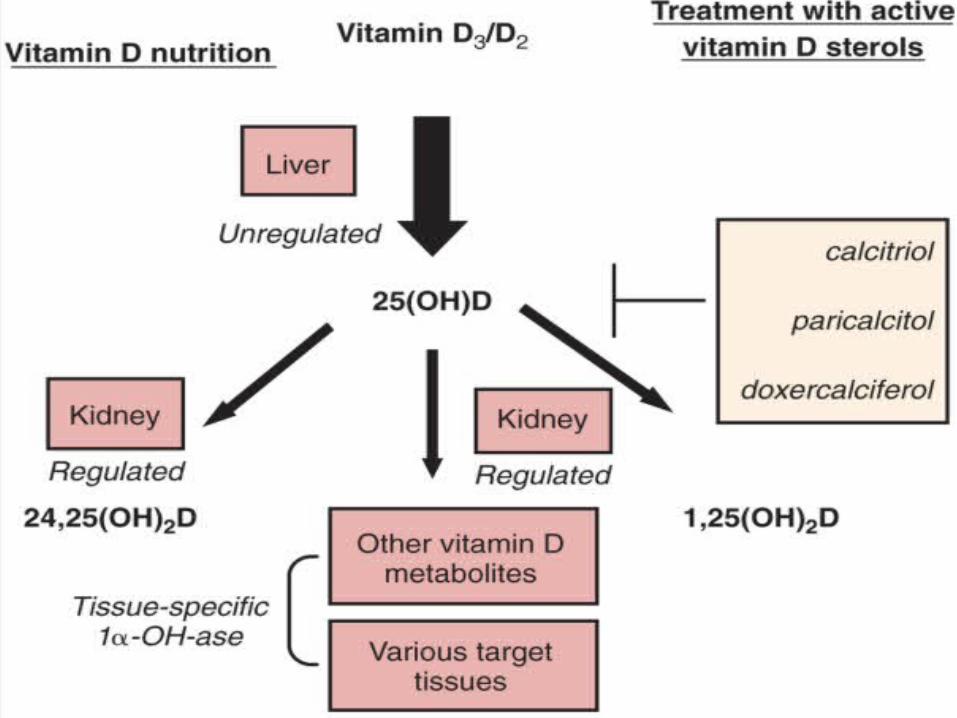
VITAMIN D - NORMAL METABOLISM
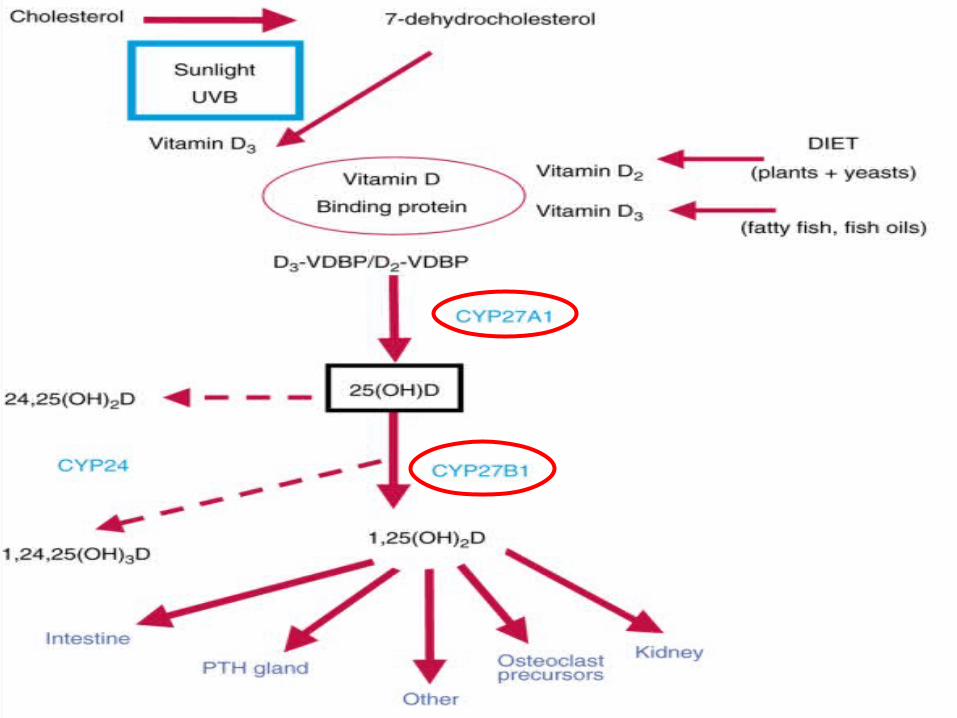
• In kidney, mitochondria of epithelial cells in the proximal nephron reabsorption of 25-hydroxyvitamin D + DBP from tubular fluid – By megalin-dependent mechanism
• Calcitriol is then released into peritubular blood– Circulates in plasma again bound to DBP
Vitamin D binding protein
• DBP
• ~ 58-kDa protein synthesized in the liver
• Human serum levels: 4 - 8 μM
• Half life: 3 days
• The parent vitamin D, 25(OH)D, & 1,25(OH)2D are carried in the circulation by DBP– But the greatest affinity is for 25(OH)D
Vitamin D binding protein
• Primary role– Maintain stable serum stores of vitamin D
metabolites & modulate the rates of bioavailability, activation, & end organ responsiveness
• Deficiency of DBP– Occur in nephrotic syndrome due to urinary
protein losses– Leading to low 25(OH)D serum levels
Genomic mechanism
• At the cellular level, receptor (megalin)–mediated endocytosis of both calcidiol & calcitriol
• Inside the cell, 1,25(OH)2D
– Inactivated by mitochondrial 24-hydroxylase – Or bind to the VDR in the cytoplasm
• VDR-ligand binding occurred => VDR translocates to the nucleus
• => Heterodimerizes with the retinoid X receptor
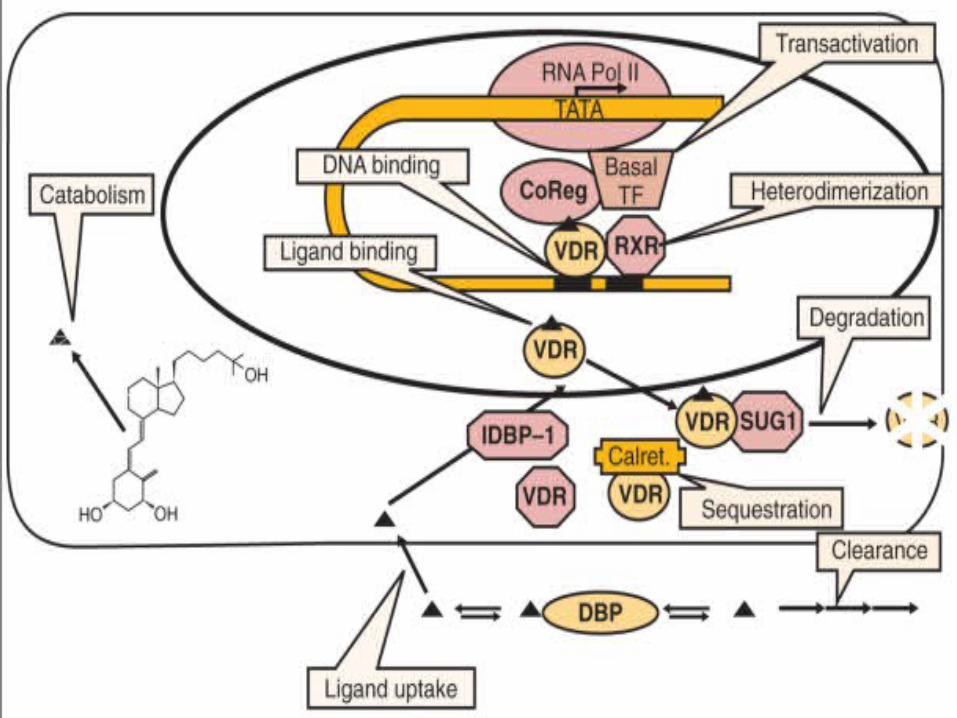
Genomic mechanism
• This complex binds the vitamin D response element of target genes
• Recruits transcription factors & corepressors/activators that modulate the transcription
• These corepressors & coactivators appear to be specific for the ligand – Different forms & analogs of vitamin D may
produce different effects
Nongenomic
• Exert biologic effects over periods of time that are too short to be explained by genomic mechanisms
• A discrete receptor, or membrane-associated protein– Distinct from the VDR may mediate these
rapid nongenomic actions
Transcaltachia
• Increases in intestinal Ca transport within 10 - 15 minutes after adding 1,25-dihydroxyvitamin D to fluid used to perfuse the lumen of the proximal small intestine
Impact of Chronic Kidney Disease on Vitamin D Metabolism
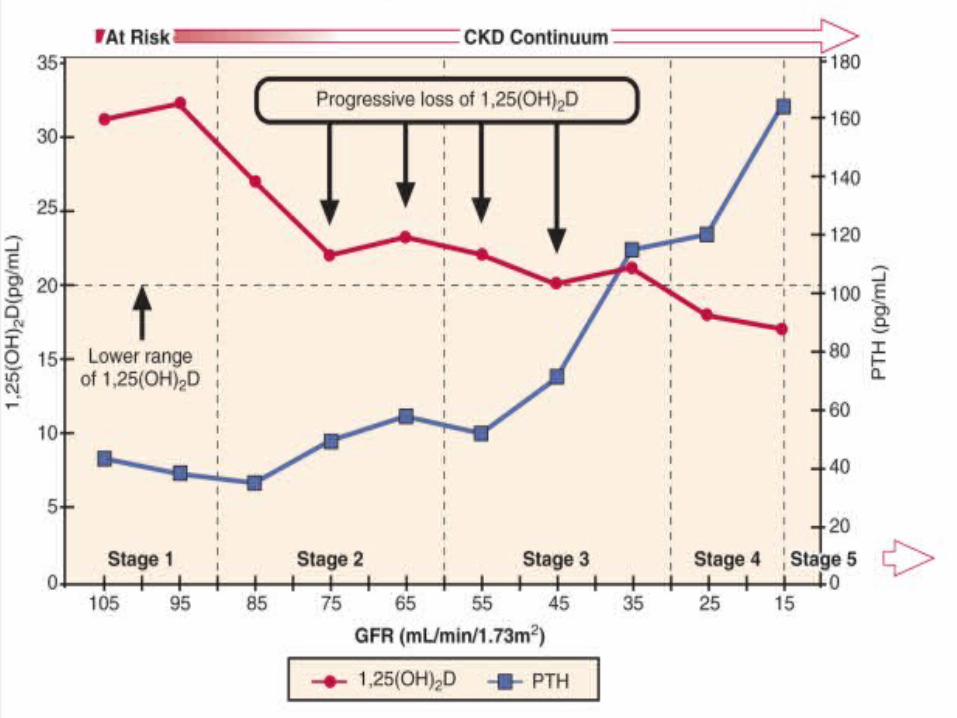
• Cross-sectional studies– 1,25-dihydroxyvitamin D decrease
progressively as renal function declines– Reductions in renal synthesis
• Adversely affects intestinal Ca absorption => modest reductions in serum Ca concentration
• => Hypocalciuria • Several mechanisms involved
Consequences of Impaired Renal Calcitriol Synthesis in
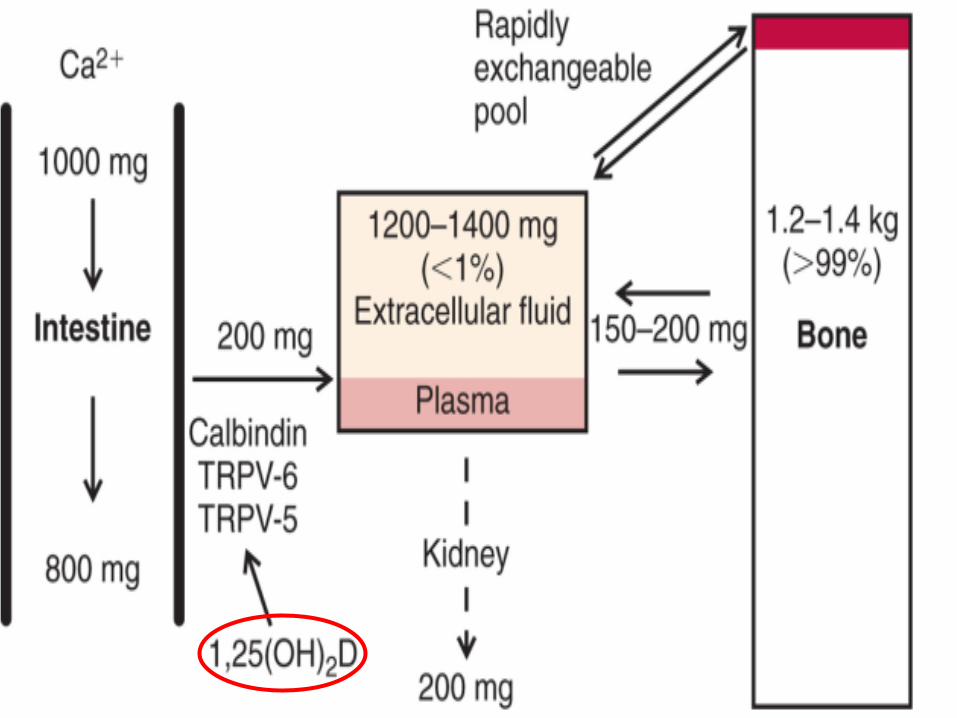
Chronic Kidney Disease• Calcitriol modulates the expression of
several key proteins responsible for the transepithelial movement of Ca– Not only in intestine but also in kidney
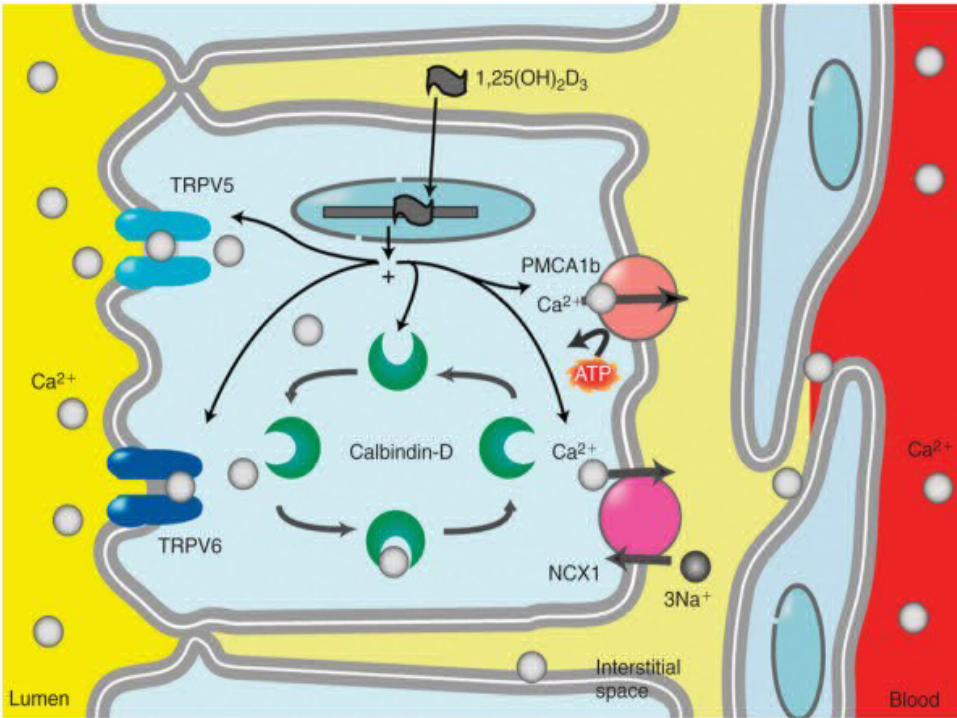
• Calbindins– Vitamin D-dependent proteins– Buffer free Ca within the cytoplasm of epithelial
cells in Ca-transporting epithelia– Translocation of Ca from the apical to the
basolateral cell membrane
• Calcitriol + Ca modulates the expression of 2 proteins
• Vanilloid family of transient receptor potential (TRP) proteins
• TRPV-5 & TRPV-6• Constitutively activated Ca channel• Mediates Ca uptake across the apical
membrane of renal & intestinal epithelial cells
Extrarenal Calcitriol Synthesis
• Other tissues also express the 25-hydroxyvitamin D-1-α-hydroxylase
• => 1,25-dihydroxyvitamin D synthesis regulated in a tissue-specific manner
• => serve as autocrine or paracrine
VITAMIN D IN BONE & CALCIUM HOMEOSTASIS
• 1,25(OH)2D3
– Major calcitropic hormone– Keep the plasma Ca2+ within narrow limits – Renal production regulated by 2 hormones
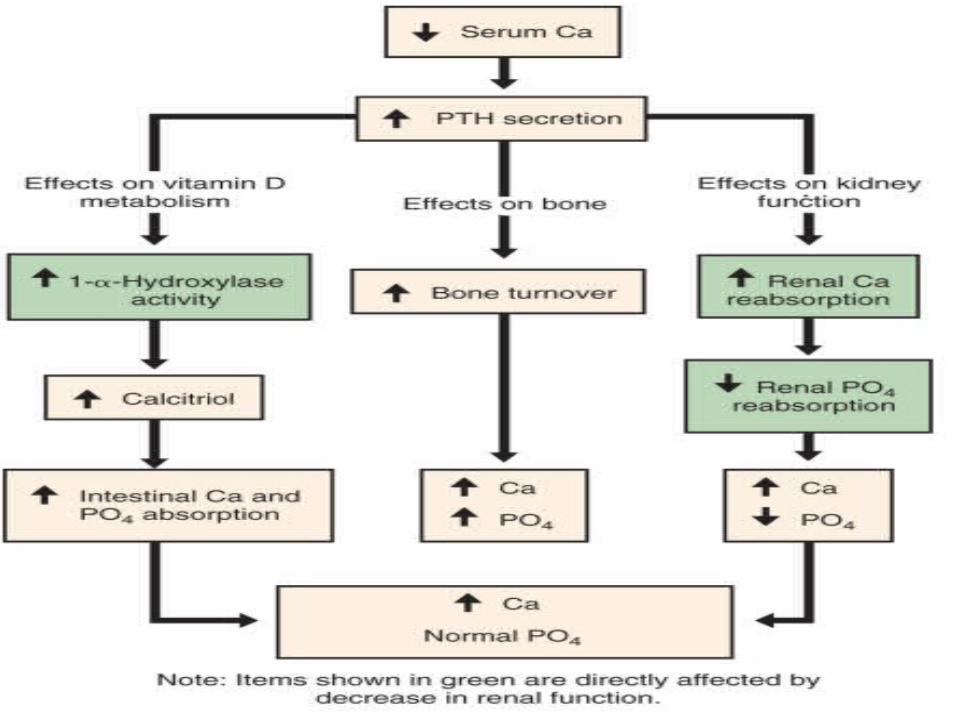
• PTH– Hypocalcemia => secretion of PTH by the
parathyroid gland– PTH targets the kidney
• Decrease Ca2+ excretion, inhibit phosphate reabsorption, & stimulate 1,25(OH)2D3 production
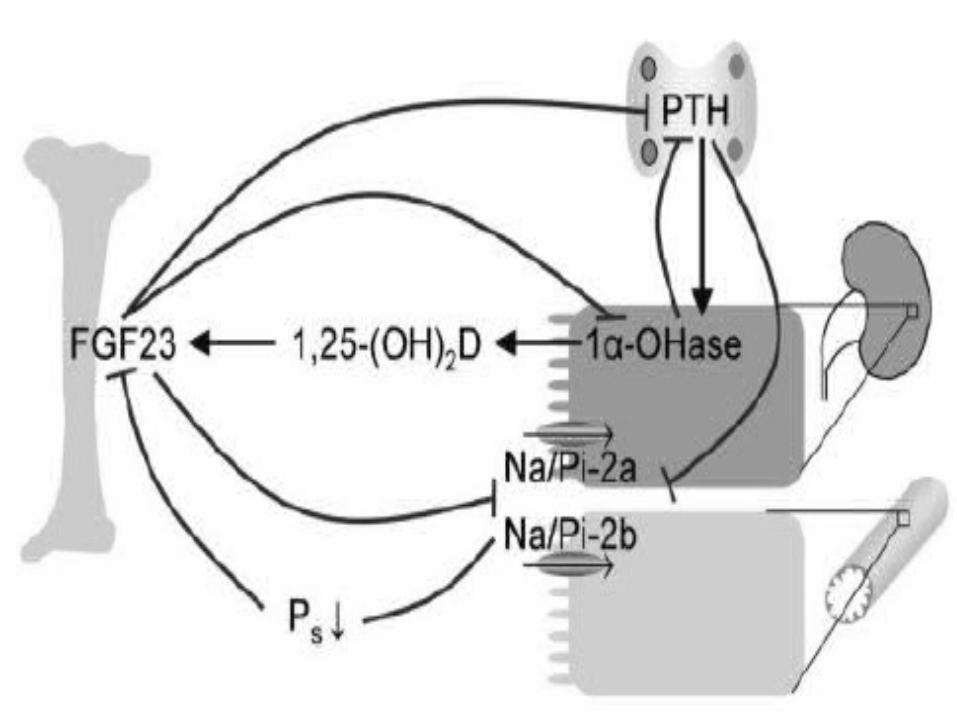
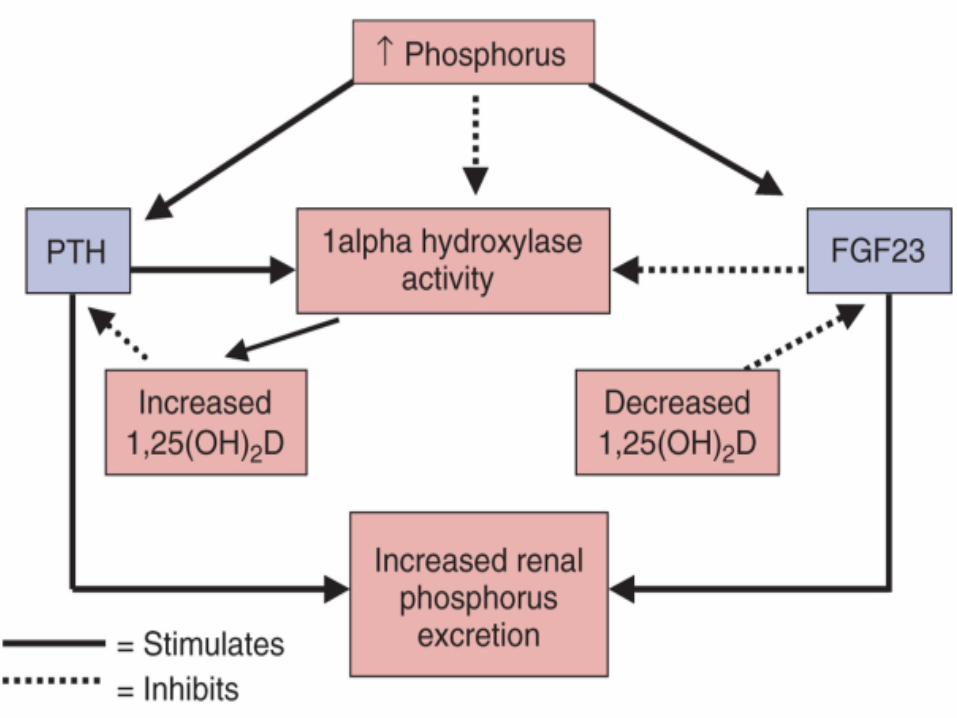
FGF23
• 1,25(OH)2D3 stimulates the secretion of FGF23 by the osteocytes
• Major phosphaturic hormone
• Inhibiting renal phosphate reabsorption
• By the specific transporter NaPiT2a
• Decrease renal production of 1,25(OH)2D3
• Genetic deficiencies in 1,25(OH)2D3
– Loss of CYP27B1 or VDR– => hypocalcemia, hyperparathyroidism,
hypophoshatemia, rickets, & osteomalacia
• The phenotype can largely be corrected by administration of a high Ca diet – Bypasses 1,25(OH)2D3 -mediated, Ca2+
absorption - Endocr Rev 2008;29: 726–776
• Reintroducing VDR in the intestine of VDR null mice rescued the hypocalcemia & the bone phenotype
- Gastroenterology 2009; 136:1317–1327
- J Bone Miner Res 2008; 23: S104
• The proteins involved in this active intestinal Ca2+ transport remain poorly defined.
• TRPV6, Calbindin– Main mediators of 1,25(OH)2D3 -induced
intestinal Ca2+ absorption
• Inactivation of TRPV6 & calbindin D9k not impair intestinal Ca2+ absorption when dietary Ca intake is normal– => compensatory proteins
• TRPV6 is critical for Ca2+ absorption when dietary Ca intake is low– Impaired intestinal Ca2t absorption in
TRPV6 null mice on a low Ca diet - J Bone Miner Res 2007; 22: 274–285
- Endocrinology 2008; 149: 3196–3205
• Hypothesis: 1,25(OH)2D3 action not only affects transcellular but also paracellular Ca2+ transport
• Regulate tight junction permeability in the intestine by modifying the expression of several tight junction proteins– Claudin-2 & claudin-12
- Mol Biol Cell 2008; 19: 1912–1921
• TRPV5 is definitely critical for renal Ca2+ reabsorption
• TRPV5 null mice – Profound Ca2+ wasting– With compensatory increased intestinal Ca2+
absorption
– Due to high 1,25(OH)2D3 serum levels, & normocalcemia as a result
- J Clin Invest 2003; 112: 1906–1914
Direct effect of 1,25(OH)2D3 on bone homeostasis?
• 1,25(OH)2D3 stimulate bone resorption
– Increasing the expression of osteoclastogenic factors in osteoblasts
• Receptor activator of nuclear factor kB ligand
• 1,25(OH)2D3 -mediated signaling in regulating the activity of chondrocytes & osteoblasts – During endochondral bone formation & bone
homeostasis
• Aberrant growth plate development in VDR-deficient mice appears before the onset of hypocalcemia
• High Ca diet corrected all aspects of the phenotype of CYP27B1-deficient mice, except long bone growth
- Endocr Rev 2008;29: 726–776
• Mice lacking VDR expression in chondrocytes– Normal growth plate– But develop a transient phenotype of
increased bone volume postnatally– Due to decreased expression of the
angiogenic factor VEGF & the osteoclastogenic factor receptor activator of nuclear factor kB ligand in chondrocytes
- J Clin Invest 2006; 116: 3150–3159
• 1,25(OH)2D3 -mediated signaling in chondrocytes
• Necessary for timely vascular invasion & osteoclastogenesis during bone growth
VITAMIN D & CANCER
• Several large-scale epidemiological studies have shown an inverse correlation between exposure to sunlight (the major source of vitamin D) or vitamin D intake & risk of colorectal, breast, & prostate cancer
Colorectal cancer risk
• Am J Prev Med 2007; 32: 210–216– Meta-analysis– 51% lower incidence of colorectal ca
• Highest serum 25(OH)D3 quintile (82 nmol/l) compared to the lowest quintile (<=30 nmol/l)
• Aliment Pharmacol Ther 2009; 30:113–125– Meta-analysis
– Lower serum 25(OH)D3 inversely associated with colorectal cancer
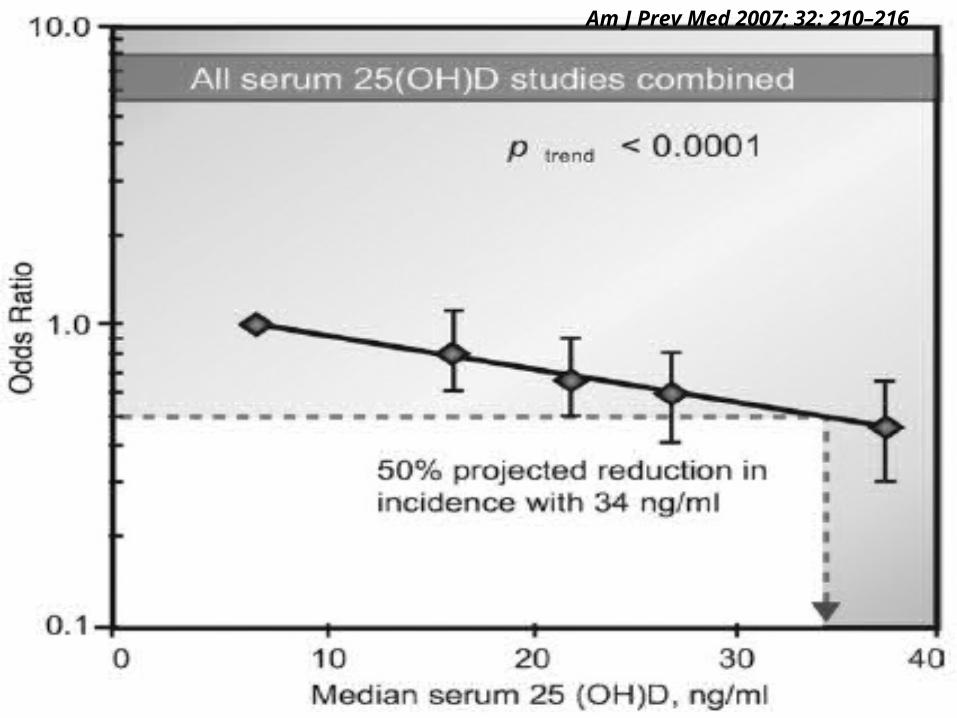
Am J Prev Med 2007; 32: 210–216
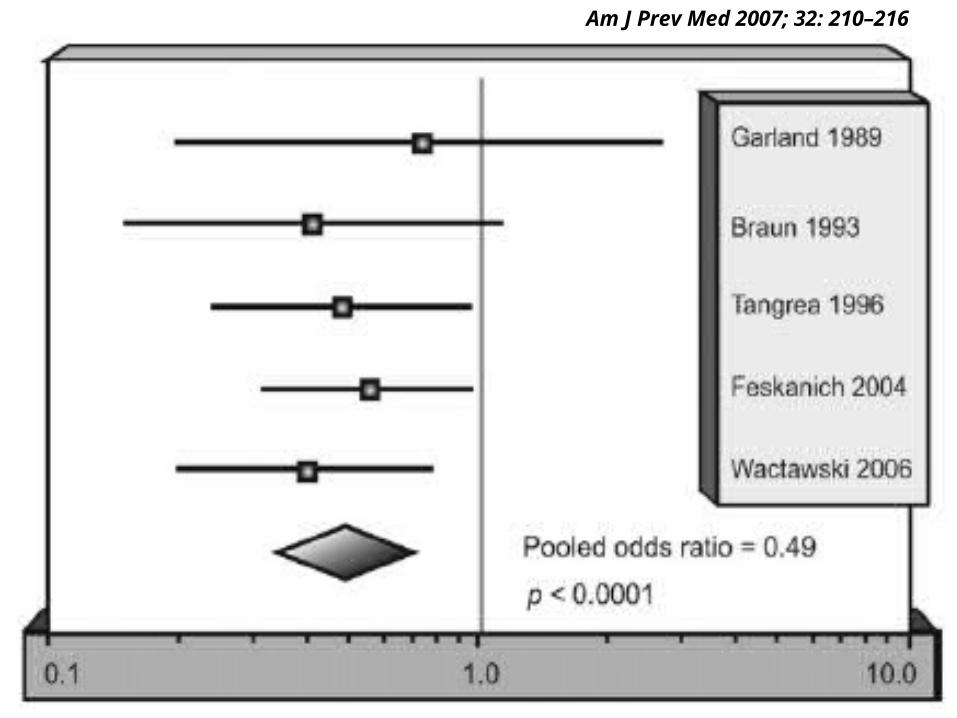
Am J Prev Med 2007; 32: 210–216
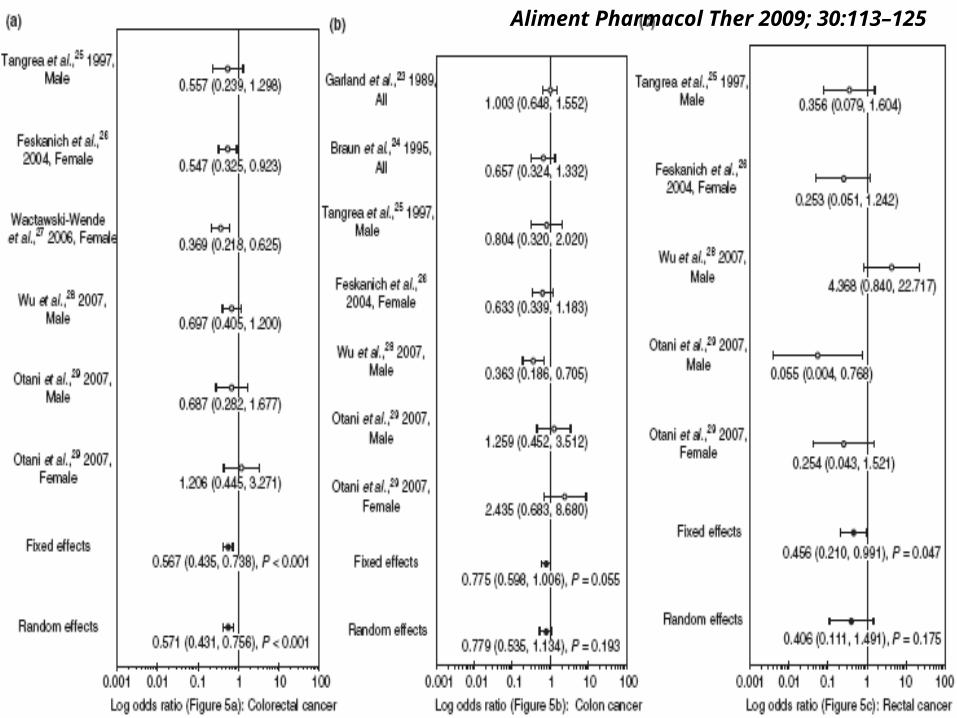
Aliment Pharmacol Ther 2009; 30:113–125
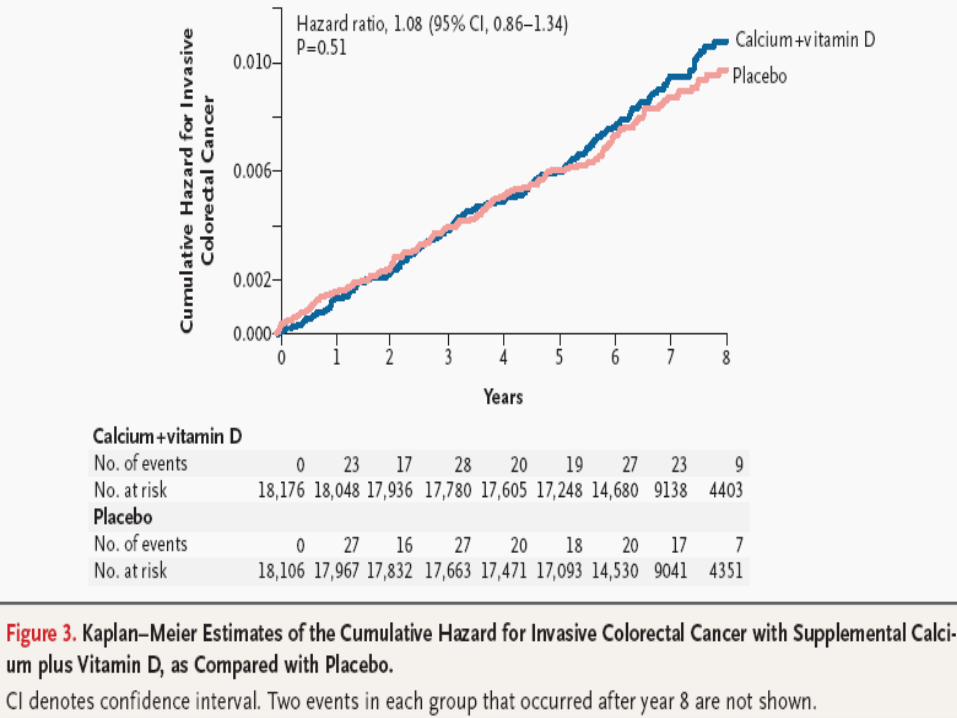
• NEJM 2006; 354: 684–696– Randomized, double-blind, placebo-controlled trial
involving 36,282 postmenopausal women from 40 Women’s Health Initiative centers, combined treatment of vitamin D3 (400 IU per day) & Ca
– Not decrease colon cancer risk
• Am J Clin Nutr 2007; 85: 1586–1591– Much smaller RCT– 1100 IU per day of vitamin D3 + Ca – Decreased the overall cancer risk
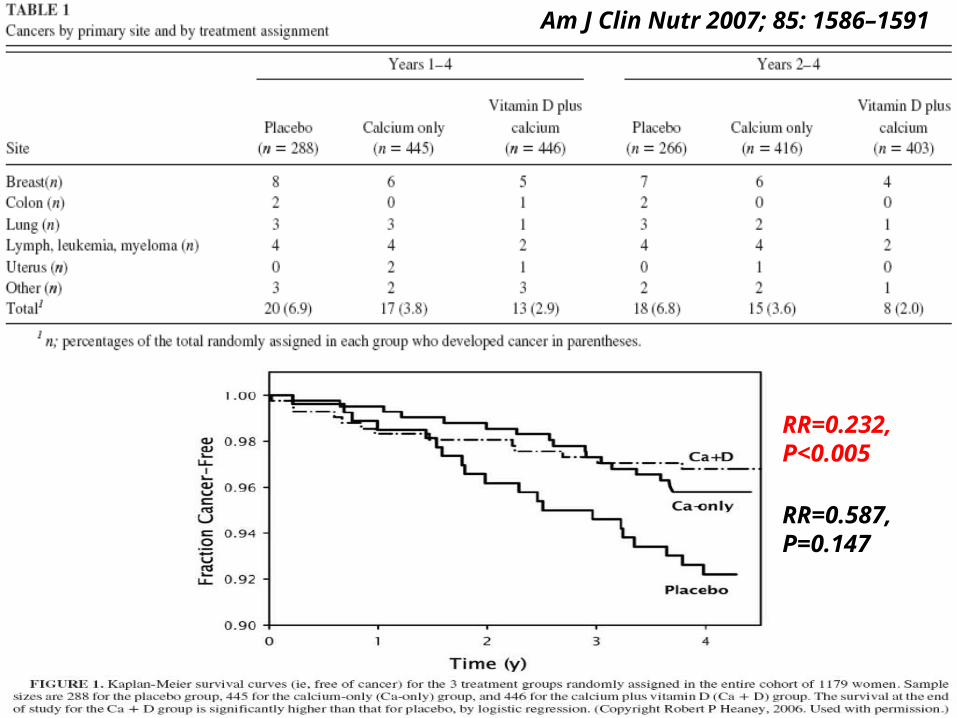
Am J Clin Nutr 2007; 85: 1586–1591
RR=0.232, P<0.005
RR=0.587, P=0.147
Breast cancer risk
• Positive study in the US & Europe
• Best Pract Res Clin Endocrinol Metab 2008; 22: 587–599– UK
– Women with 25(OH)D3 levels < 50nmol/l OR=3.54 for breast cancer risk compared with women with levels >50 nmol/l
• Negative in other epidemiological studies
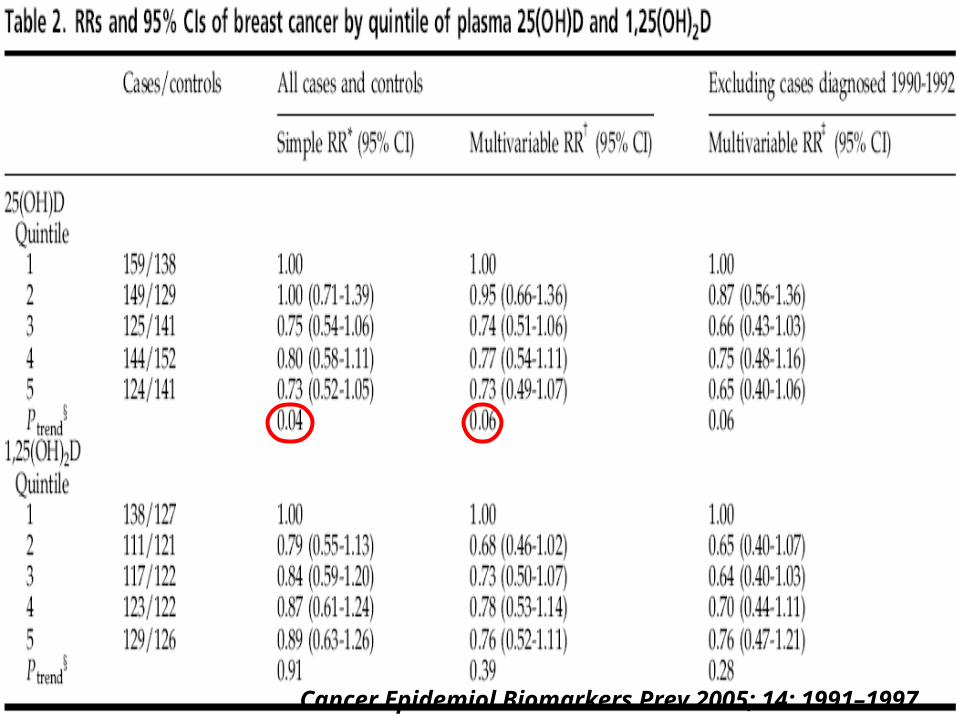
Cancer Epidemiol Biomarkers Prev 2005; 14: 1991–1997
• Prostate cancer– Association with 25(OH)D3 status less clear
than for colorectal cancer
• Overall cancer outcome– Association remains ambiguous
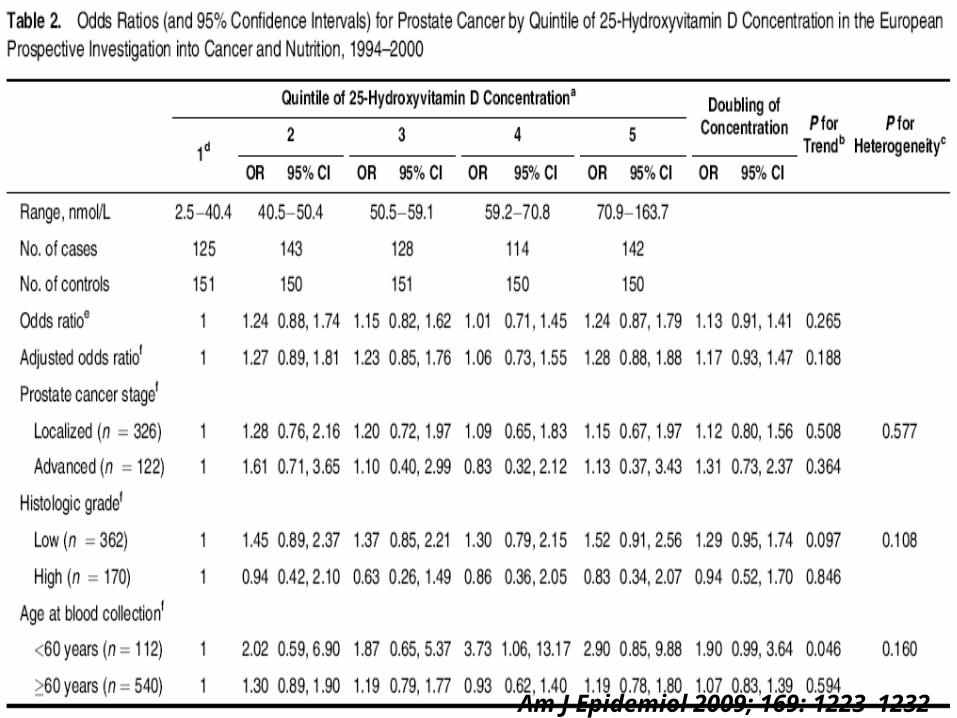
Am J Epidemiol 2009; 169: 1223–1232
• Supraphysiological doses of 1,25(OH)2D3
– Potent growth-inhibitory & pro-differentiating effects on a variety of cell types
• VDR-/- mice hyperproliferation in the colon & mammary gland– Not develop cancer spontaneously but
predisposed to cancer when challenged with carcinogenic agents
• 1,25(OH)2D3 inhibits cell growth by hampering the transition from the G1 to the S phase of the cell cycle
• 1,25(OH)2D3 accumulates cells in the G1 phase – Targeting cell-cycle regulators in a direct or
indirect way
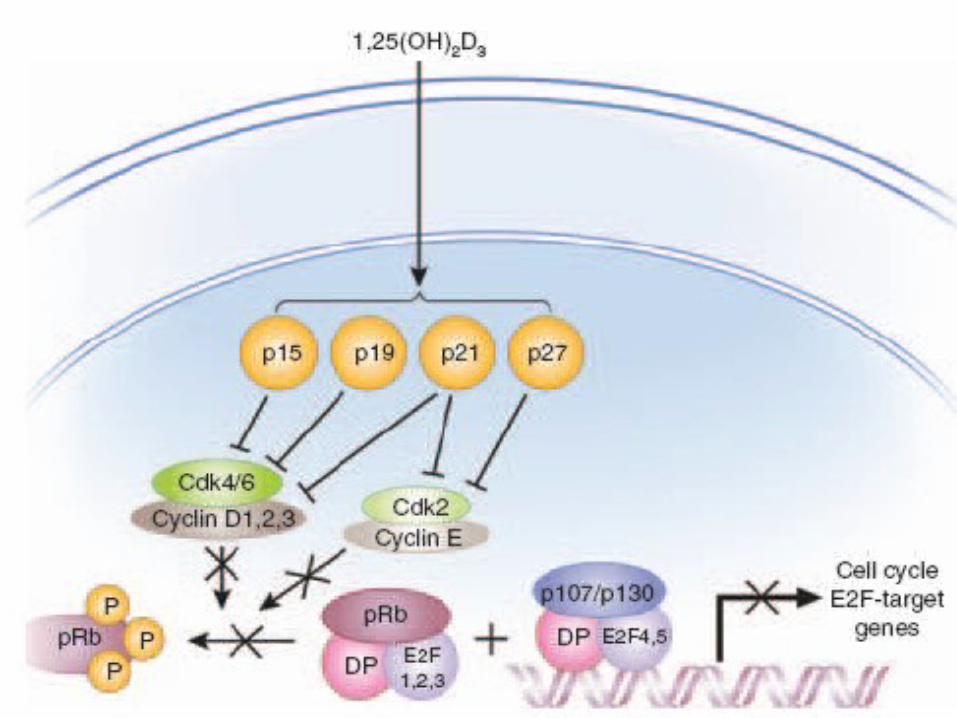
• Cyclin-dependent kinase inhibitor p21(waf1/cip1)
– Directly activated by 1,25(OH)2D3
– Through a vitamin D responsive element in its promoter region
• Increase of cyclin-dependent kinase inhibitor p27(kip1) protein levels – Posttranslational modifications
– 1,25(OH)2D3-induced repression of the miR181 family => accumulation of p27(kip1)
• Decrease cyclin D1 & cyclin E expression
• Decrease activity of complexes between cyclins & cyclindependent kinases – Influences the phosphorylation status of the
retinoblastoma pocket protein family– Preventing the release of the E2F transcription
factors 1, 2, 3– Keeps the inhibitory complexes of E2F4 &
E2F5 with p107 & p130 pocket proteins on the promoter of cell-cycle target genes
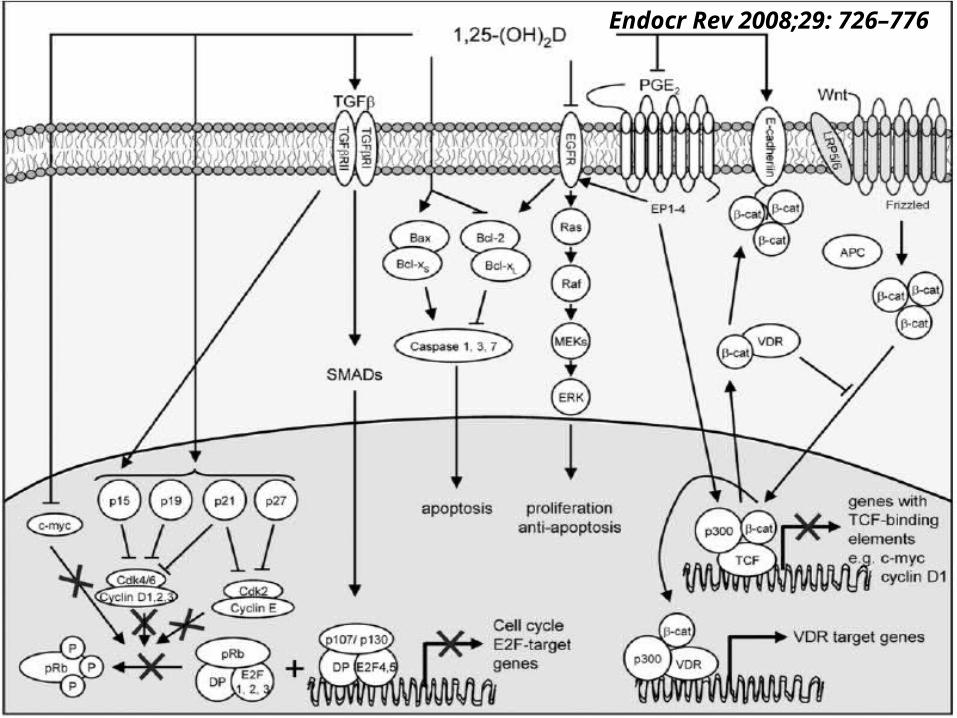
Endocr Rev 2008;29: 726–776
• Presence of the VDR in tumors + growth-regulatory effect of 1,25(OH)2D3
– Use of this compound in cancer prevention and/or treatment
• Small trials– High weekly dose of 1,25(OH)2D3 instead of
daily administration was safe & combination therapies were well tolerated
ASCENT phase III clinical trial
• Novacea, South San Francisco, CA, USA
• Large cohort of patients (950)
• Anrogenindependent prostate cancer
• Control arm: Taxotere every 3 weeks
• Weekly high dose of 1,25(OH)2D3 (DN-101) + once-weekly Taxotere
• Terminated 30 weeks earlier– Unexplained imbalance of deaths between the
treatment & control group
TX 522
• Inecalcitol; Hybrigenics, Paris, France
• Structural analogs of 1,25(OH)2D3
• Clear dissociation between antiproliferative & calcemic effects
• In phase II in patients with hormone-refractory prostate cancer
TX 522
• Preliminary results– 27 of the 31 patients– Inecalcitol (at different doses up to 600 mg
per day) & Taxotere during 18 weeks – Decrease in PSA levels >30% within 3
months of initiation of treatment– Without any changes in Ca parameters
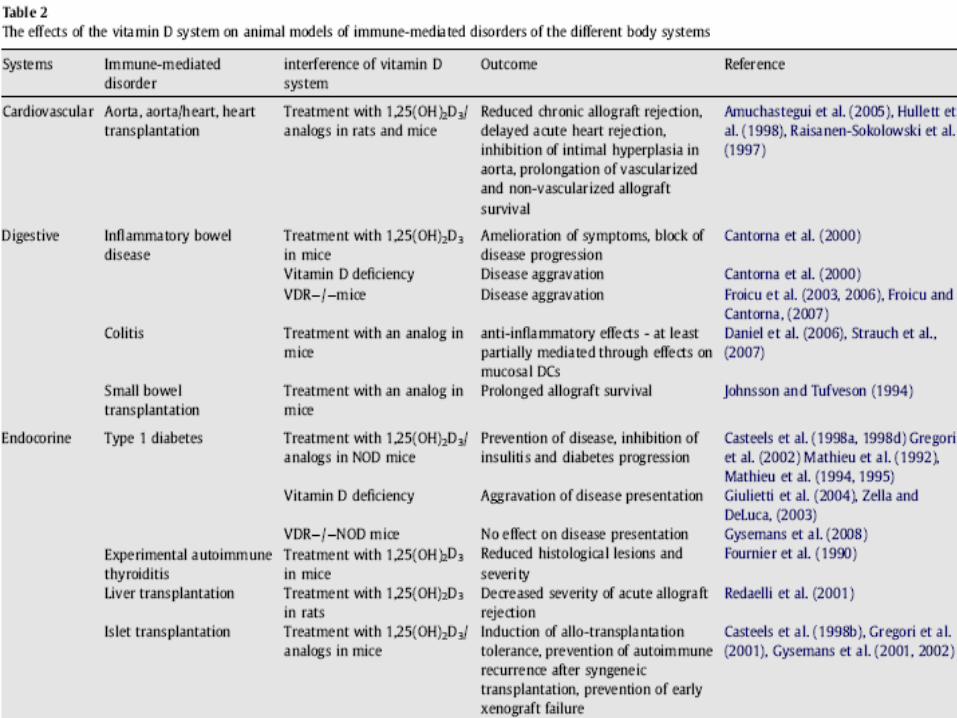
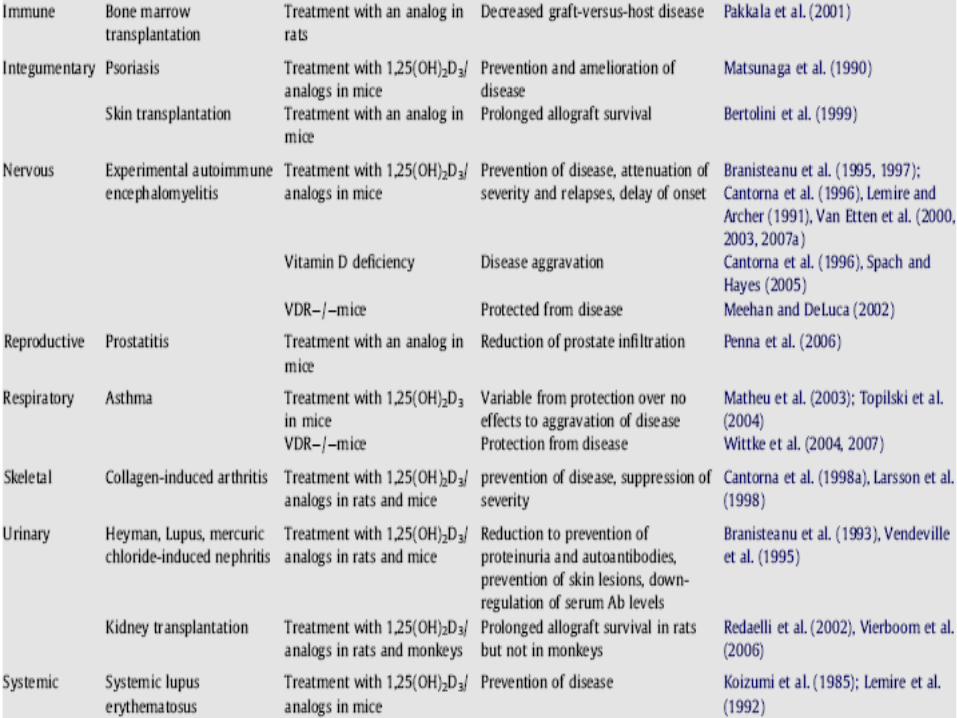
VITAMIN D AS IMMUNE MODULATOR
• Exposure of skin to UVB => immunosuppression
• Part of this effect is mediated through synthesis of vitamin D & activation to its active form 1,25(OH)2D3 under the influence of UVB
• Receptors for vitamin D have been described in most cells of the immune system & many immune cells
• Activate 25(OH)D3 to 1,25(OH)2D3
– Within the immune system a paracrine presence of 1,25(OH)2D3
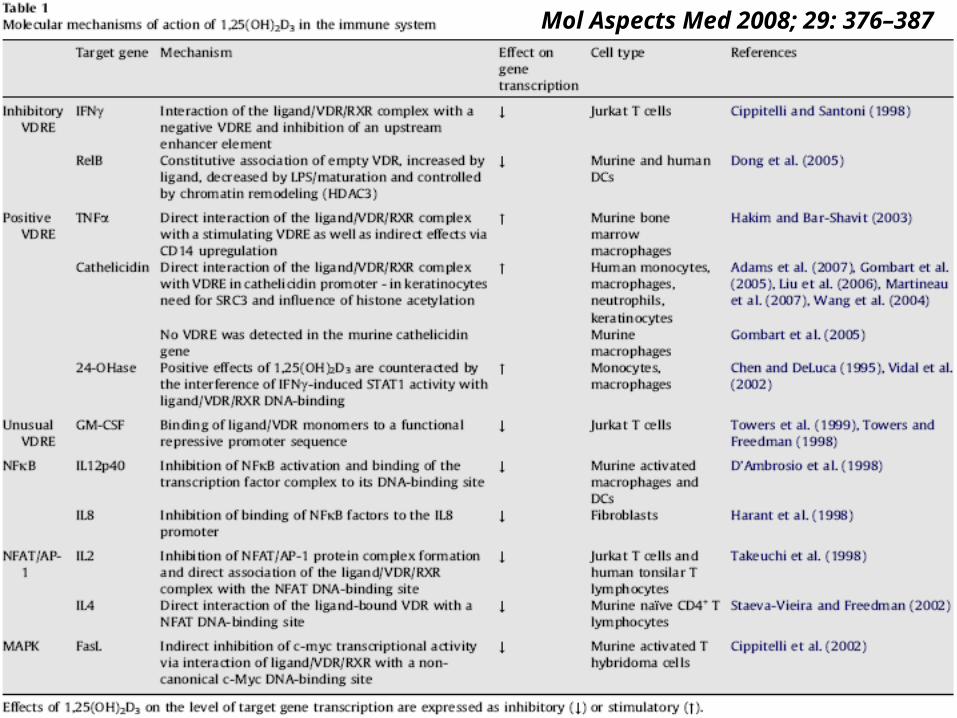
Mol Aspects Med 2008; 29: 376–387
• Immune stimuli => immune cell => secretion of 1,25(OH)2D3
• Crucial immune stimulus: interferon-gamma
• Other macrophage activators/differentiators simultaneously to activate a complex network of signaling pathways– LPS, phorbol myristate acetate, or TNF-α
• TLR4 activation & TLR2/1 triggering– Able to induce 1α-hydroxylase in human
macrophages– Induction of an antimicrobial response
• 1,25(OH)2D3 -metabolizing enzyme, CYP24A1– 24-hydroxylation– Expressed by antigen-presenting cells
• 1,25(OH)2D3 enhanced capacity of innate antibacterial defense
• More tolerogenic profile toward autoimmune phenomena
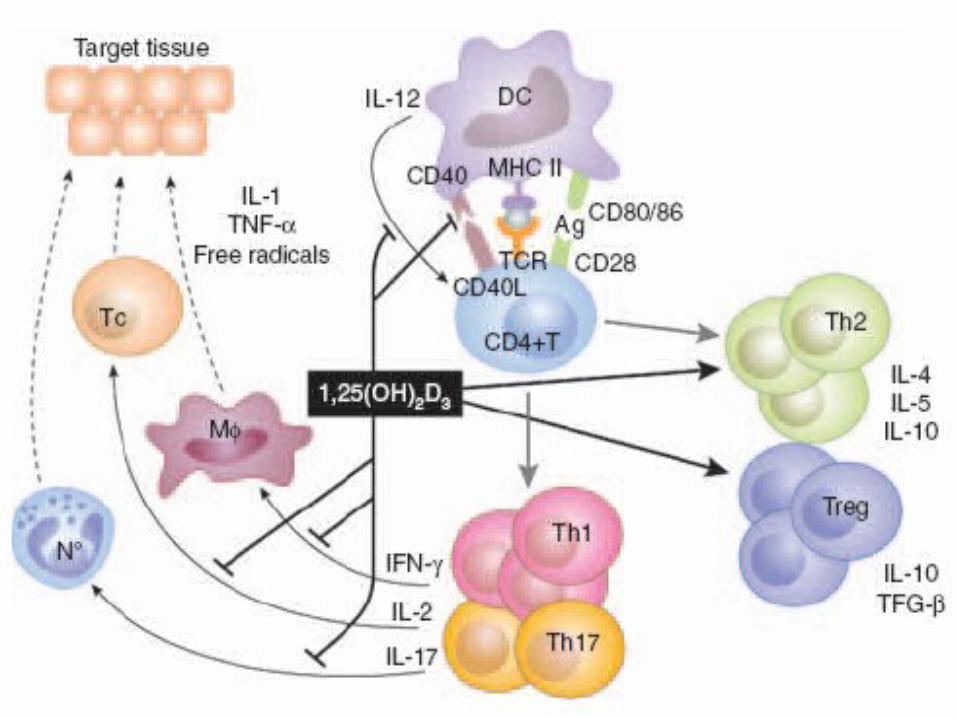
• Dendritic cell (DC) & other APCs– Langerhans cells in skin– Central to the effect of vitamin D
• Maturation, differentiation, & function of DCs affected, with downregulation of MHC class II & costimulatory molecules– CD40, CD80, & CD86
• => Tolerance-promoting phenotype
• DC alterations + effects on cytokine secretion by the DC– Favoring IL10 & inhibiting IL12
• => T-cell function affected– Promoting development of Th2 lymphocytes
within the CD4+ subset– Also affecting CD8+ CTL development
T lymphocytes
• Can be direct targets for 1,25(OH)2D3
– Inhibition of several cytokines, INF-r & IL-17– Stimulation of others such as IL-4
• 1,25(OH)2D3 affects the expression of chemokine receptors on the surface of T lymphocytes – Determine the target tissue where any
primed T lymphocytes will migrate to
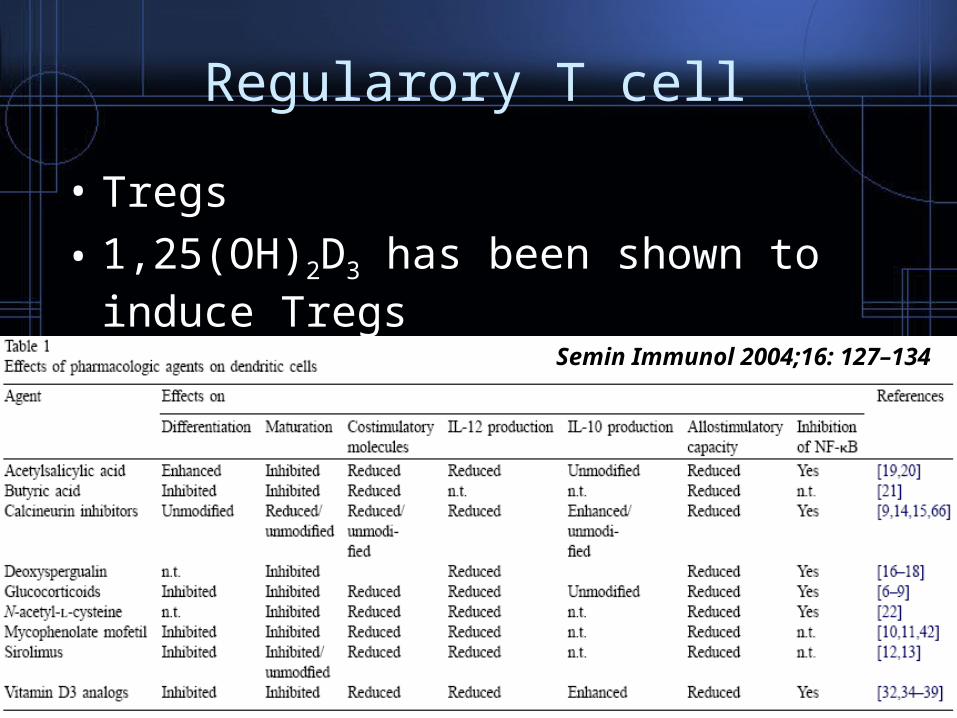
Regularory T cell
• Tregs
• 1,25(OH)2D3 has been shown to induce Tregs
Semin Immunol 2004;16: 127–134
Monocyte/macrophage
• Another important target cell of 1,25(OH)2D3
• TLR activation
• Responsible for antibacterial & antiviral defenses
• 1,25(OH)2D3 promote secretion of antibacterial products– Cathelicidin
- Science 2006; 311:1770–1773
Vitamin D deficiency & autoimmunity
• Epidemiological studies– Type 1 diabetes, multiple sclerosis,
inflammatory bowel disease
• Preclinical animal models– Vitamin D deficiency especially early in life
enhances such autoimmune diseases
• Need prospective intervention studies
CARDIOVASCULAR & METABOLIC ACTIONS

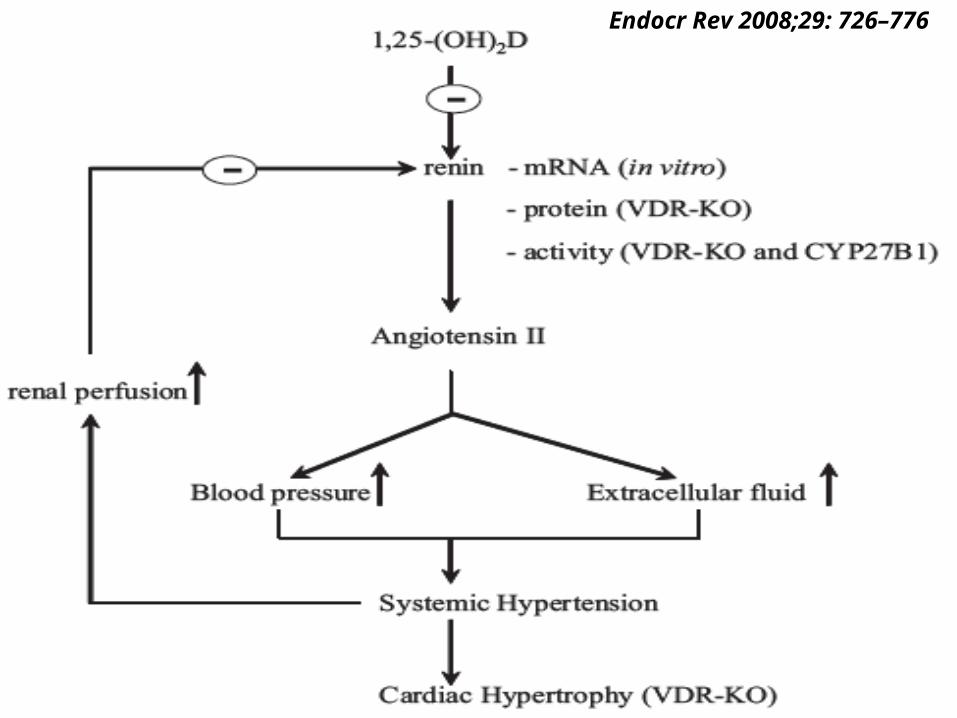
• Vitamin D-deficient rats or mice with deletion of VDR or 1α-hydroxylase – High renin hypertension with ultimately
cardiac hypertrophy
• Selective VDR deficiency in cardiac myocytes can reproduce the effects.
• Am J Hypertens 2009; 22: 816– Normotensive & hypertensive Caucasian,
Hispanic, or African Americans– Lower serum 25(OH)D with higher BP
• Endocr Rev 2008;29: 726–776– Normotensive & hypertensive patients– BP inversely correlated with plasma
1,25(OH)2D & renin concentrations
• Low 25(OH)D & metabolic syndrome– Obesity, insulin resistance, type 2 diabetes
• Only very small scale intervention studies using vitamin D or its active hormone on BP or other aspects of the metabolic syndrome
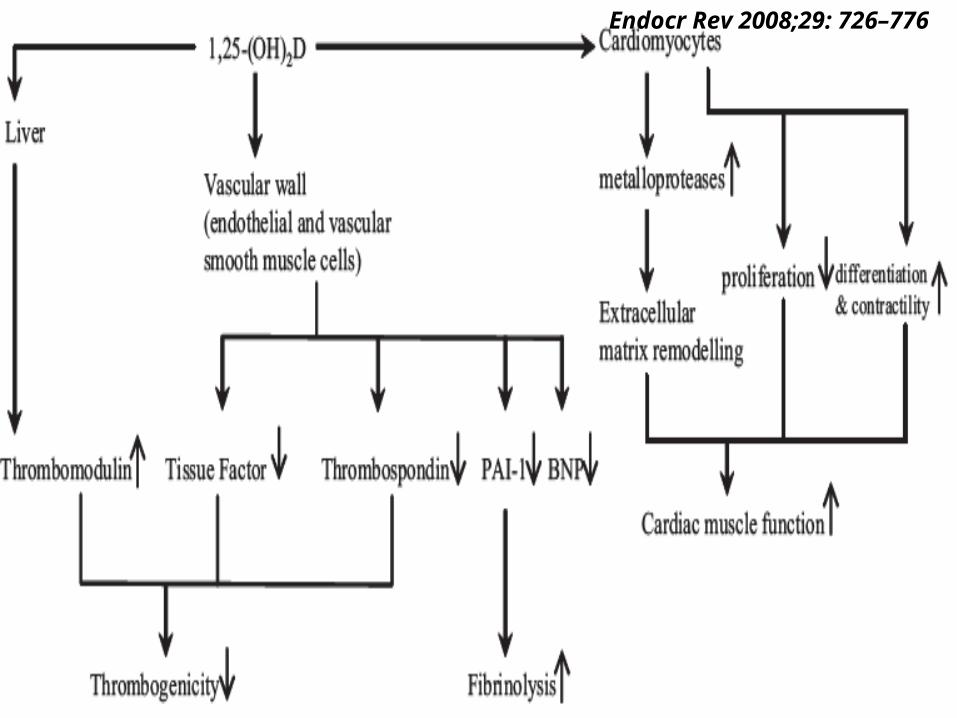
Endocr Rev 2008;29: 726–776
Endocr Rev 2008;29: 726–776

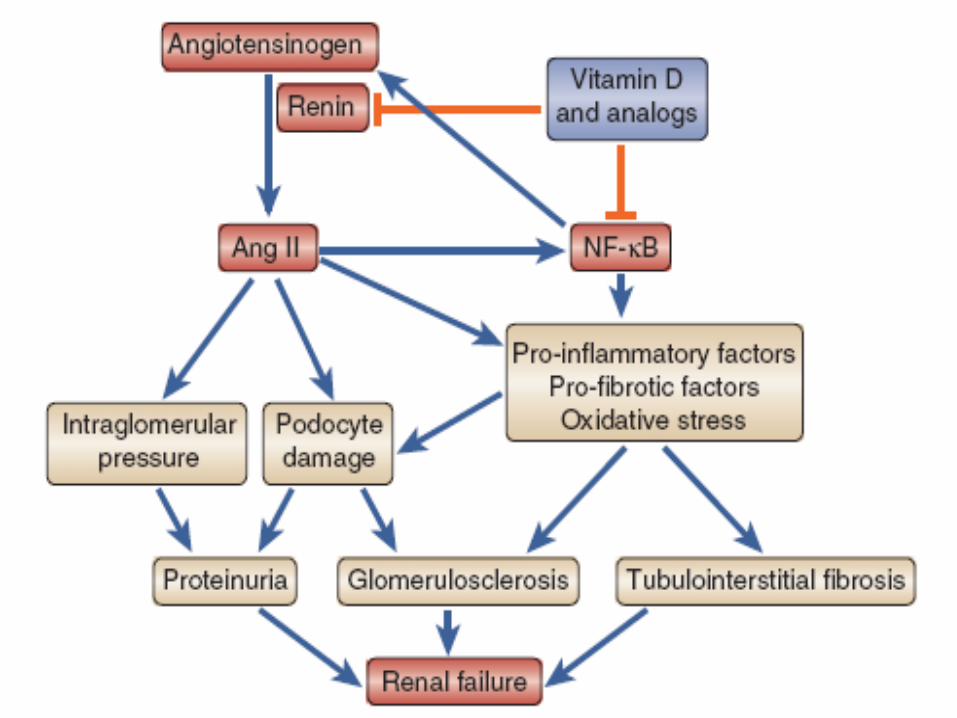
RENAL PROTECTION
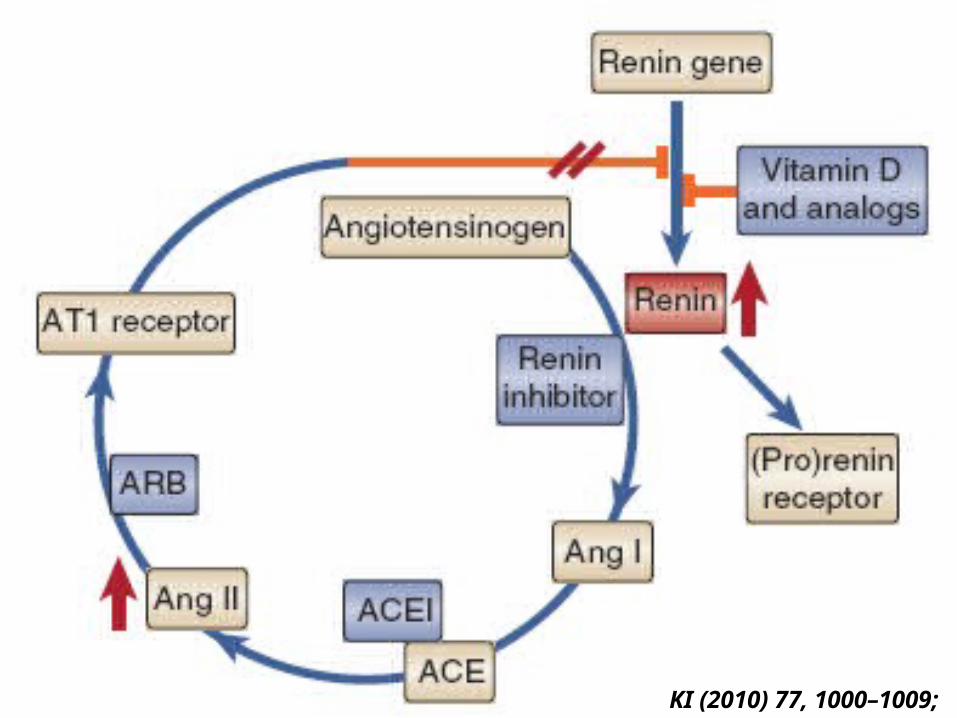
KI (2010) 77, 1000–1009;
CLINICAL PERSPECTIVES
• Major function of 1,25(OH)2D3 /VDR
– Control the Ca & bone homeostasis
• Combined presence of 25(OH)D3-1α-hydroxylase + VDR in several nonclassical tissues introduced the concept of a paracrine/autocrine function for 1,25(OH)2D3 outside the Ca & bone metabolism.
• 1,25(OH)2D3 capable of regulating cell differentiation & proliferation of normal (immune) cells & malignant cells
• Poor vitamin D status is linked with all major diseases causing the majority of human morbidity– Cancer, immune diseases, metabolic
syndrome, hypertension, & cardiovascular risk factors
• The optimal daily dosage is highly debated• Most RCTs used 600–1000 IU of vitamin
D3 per day– Decrease the risk of fractures & falls in the
elderly
• Serum 25(OH)D concentration– Should > 20 ng/ml (or 50 nmol/l)– Probably even 30 ng/ml (80 nmol/l) in patients
with impaired renal function
• Mean level of 25(OH)D around the world – ~ 20 ng/ml
• US NHANES IV – < 30 ng/ml
• Large part of the human population mildly vitamin D deficient
• Patients with CKD have a greater than normal risk for bone diseases, cancer, immune disorders, & increased CV mortality
• A number of observational studies have shown that treatment of hemodialysis patients with active vitamin D analogs decreases (cardiovascular) mortality.
• Overall contribution of combined impaired 25(OH)D3–1,25(OH)2D3 status on morbidity & mortality in patients with CKD may be substantial but needs further RCTs.
Endocr Rev 2008;29: 726–776

THANKS FOR YOUR LISTENING


















