February 11, 2016 Tobacco Treatment 2016: Disclosures An...
23
1 Vermont Cardiac Network February 11, 2016 Tobacco Treatment 2016: An Evidence Based Approach Elizabeth Maislen, APRN, CTTS PHS 1 Disclosures None. I do not intend to discuss off label use of any products. I don’t smoke and I don’t vape or hookah. When patients ask, “Did YOU ever smoke?” I tell them “It’s not about me today, it’s all about YOU.” Thank you to Susanne Tanski, MD Cessation Treatments are Underused! The treatments recommended in the PHS guidelines are underused by smokers and health care providers. About 70% of smokers want to quit smoking, and about half try to quit each year. However, less than 10% succeed, in part because less than one-third of smokers who try to quit use proven cessation treatments. In 2010, less than half of smokers (48.3%) who saw a health professional in the past year reported receiving advice to quit The Surgeon General’s Report Cigarettes and other tobacco products have evolved into highly engineered, addictive and deadly products, containing thousands of harmful chemicals causing a wide range of diseases, cancers and premature deaths. 9 of 10 smokers regret ever having started. 60% of current smokers perceive themselves as “very addicted.” Health Consequences Smoking-50 years of Progress, UHDHHS, Report of Surgeon General 2014 What’s Different? Today’s cigarette smokers, especially women, have much higher risk for lung cancer, COPD and CVD, despite smoking fewer cigarettes. The design of the cigarette is different. More nicotine is absorbed when smoked. Combinations of products in cigarettes. International Tobacco Control Study S. Glantz et al, 2-8-14; 2002-2011 longitudinal study PHS-Sponsored Clinical Practice Guideline Treating Tobacco Use and Dependence: 2008 Update PHS
-
Upload
phungkhanh -
Category
Documents
-
view
218 -
download
6
Transcript of February 11, 2016 Tobacco Treatment 2016: Disclosures An...
1
Vermont Cardiac NetworkFebruary 11, 2016
Tobacco Treatment 2016: An Evidence Based Approach
Elizabeth Maislen, APRN, CTTS
PHS1
Disclosures
None. I do not intend to discuss off label use of
any products. I don’t smoke and I don’t vape or
hookah. When patients ask, “Did YOU ever
smoke?” I tell them “It’s not about me today, it’s all about YOU.”
Thank you to Susanne Tanski, MD
Cessation Treatments are Underused!
The treatments recommended in the PHS guidelines are underused by smokers and health care providers.
About 70% of smokers want to quit smoking, and about half try to quit each year.
However, less than 10% succeed, in part because less than one-third of smokers who try to quit use proven cessation treatments.
In 2010, less than half of smokers (48.3%) who saw a health professional in the past year reported receiving advice to quit
The Surgeon General’s Report
Cigarettes and other tobacco products have evolved into highly engineered, addictive and deadly products, containing thousands of y p gharmful chemicals causing a wide range of diseases, cancers and premature deaths.
9 of 10 smokers regret ever having started. 60% of current smokers perceive themselves as
“very addicted.”
Health Consequences Smoking-50 years of Progress, UHDHHS, Report of Surgeon General 2014
What’s Different?Today’s cigarette smokers, especially women, have much higher risk for lung cancer, COPD and CVD, despite smoking fewer cigarettes.
The design of the cigarette is different.
More nicotine is absorbed when smoked.
Combinations of products in cigarettes.
International Tobacco Control Study S. Glantz et al, 2-8-14; 2002-2011 longitudinal study
PHS-Sponsored Clinical Practice Guideline Treating Tobacco Use and Dependence: 2008 Update
PHS
2
NicotineNicotine
Where is it found?
– Tobacco plant
– Virtually all is from tobacco, even NRT
PHS
Chemical structure
– Readily crosses cell membranes
– Binds in brain and muscle
PHS
https://www.youtube.com/watch?v=nwVxu
PHS
u6Ugmg
The Health Consequences of Smoking:50 Years of Progress
A Report of the Surgeon General
1964 2014
3
PHS13
The Grim Statistics
Between 1964 and 2014:
Over 20 million Americans died because of smoking, including 2.5 million nonsmokers
More than 100,000 babies
Smoking is still the leading cause of preventable disease and death in the United States.
What We’ve Learned
The Killer Cigarette
Smoking risks are more deadly than 50 years ago.
Smokers inhale over 7,000 chemical compounds.
At least 70 CAUSE CANCERCANCER.
What We’ve Learned
The Killer Cigarette
Smoking causes disease in nearly every organ.
Secondhand smoke kills more than 41,000 nonsmokers every year.
There is no safe level of SHS exposure and NO SAFE CIGARETTECIGARETTE.
21st Century Tobacco UseBetween 2010 and 2014 smoking caused
Nearly half a million premature deaths a year
More than 87% of all lung cancer deaths
61% of all pulmonary deaths
32% of all coronary deaths
4
Smoking and Children Today about half of all children 3-18 years of age are
exposed regularly to cigarette smoke.
Every day over 3,200 kids try their first cigarette and another 2,100 youth and young adults become daily smokers.
Nearly 9 out of 10 smokers started before age 18.
Photo credit: Trinketsandtrash.org
Smoking and ChildrenEvery adult who dies early because of smoking is replaced by two new young smokers.
If they keep smoking, at least one of the two will also die early from smoking.
Smoking and Children The costs of smoking Annual smoking costs are more than $289 billion.
We spend at least $132 billion in yearly medical care for adults.
We lose at least $157 billion yearly in productivity costs when smokers get sick and die early.
The Power of Nicotine Addiction Nicotine is the primary addicting drug in cigarettes.
Nicotine keeps people smoking longer and that causes more damage to the body.
Nicotine patches, gum, and lozenges are safe when used as directed.
Nicotine
Nicotine is the primary addicting drug in cigarettes.
It can raise heart rate and blood pressure.
It can result in premature births and low birth weight babies in women who smoke during pregnancy.
It can be harmful to developing brains.

5
Smoking and Lung Cancer
Today’s smokers are more likely to develop lung cancer than smokers 50 years ago.
Lung cancer is the #1 cause of cancer death for men and women.
Nearly 9 out of 10 lung cancers are caused by smokingsmoking.
Smoking – The Cancer Trigger
Smoking is now known to cause
13 different types of cancer—
almost everywhere in the body.
1 out of 3 U.S. cancer deaths are tobacco-related.
New Cancer FindingsTWO more cancers are caused by smoking:
Liver cancer
Colorectal cancer –the second deadliest behind lung cancer
SMOKING keeps cancer treatments from working as well as they should.
Smoking – The Breath Blocker COPD rates have risen steadily since 1964.
Nearly 8 out of 10 COPD deaths are from smoking.
COPD patients have higher risk for lung cancer and heart disease.
Women who smoke are now dying from COPD in the same numbers as men who smoke.same numbers as men who smoke.
Smoking – The Heart StopperCardiovascular Disease (CVD)
CVD is the biggest killer in the U.S.
It causes more than 800,000 deaths every year.
Smoking is a major cause of CVD.
SHS increases the risk for heart attack or stroke, SHS increases the risk for heart attack or stroke, even for nonsmokers.
Cardiovascular disease includes:
Coronary heart disease
High blood pressure
Heart attack
Stroke
Abdominal aortic aneurysm
P i h l t i l di Peripheral arterial disease
6
Smoking – The Heart Stopper Smoking causes cells lining veins and arteries to
swell.
Narrower arteries mean reduced blood flow to the heart, brain, and organs.
Clots can block narrowed t i i h t tt karteries, causing heart attack,
stroke, and even sudden death.
Even occasional smoking damages blood vessels.
Smoking and ReproductionSmoking also causes reproductive issues for men:
Smoking can cause erectile dysfunction (ED).
Smoking damages DNA in sperm.
Smoking and DiabetesDiabetes is the 7th leading cause of death in the U.S.
Smoking causes type 2 diabetes.
Smokers are 30-40% more likely to develop type 2 diabetes than nonsmokers.
Smoking and DiabetesDiabetic smokers:
Have difficulty regulating insulin levels.
Have higher risk of heart disease, blindness, kidney failure, and nerve and blood vessel damage to feet and legs.
Smoking and the Immune System Smoking harms the immune system and causes
autoimmune disorders.
Smoking is a cause of rheumatoid arthritis (RA).
RA treatment can be less effective for smokers.
Smoking Today – The Persistent Epidemic
Cigarettes cause almost all tobacco-related disease and death.
Smoking claims nearly 500,000 lives every year.
More than 16 million people have at least one smoking-related disease.
88 million Americans continue to be exposed to SHS 88 million Americans continue to be exposed to SHS.

7
Smoking Today – The Persistent Epidemic Lower smoking rates have saved 8 million lives and
added about three years to average life expectancy.
50 years after the first SG report, 18% of Americans smoke compared to 43% in 1965.
Today 42 million adults and 3 million middle and high school students are smokers.
W h d b t th i till h We have made progress, but there is still so much more to do.
Saving Millions of Lives – Doing Much MoreWe know what works to lower smoking rates:
Smokefree policies in public places
Make smoking the exception – not the norm
Easy-to-get affordable smoking cessation treatments
Cessation – Lifeline to a Tobacco-Free Life Most smokers want to quit and half already have.
Cessation therapies improve your chances of quitting successfully.
Talk to your doctor, and call 1-800-QUIT-NOW or go to http://www.SmokeFree.gov for free help.
We Can Be Tobacco-Free
The time is NOW to begin a tobacco-free future.
We can break the cycle of sickness, disability and death caused by smoking.
We can reduce the disease and death caused by smoking until the scourge of the tobacco use epidemic becomes a minor public health nuisance.
We Can Be Tobacco-Free
is the chief, single, avoidable cause of death
“CIGARETTE “CIGARETTE SMOKING…SMOKING…
PHS
in our society and the most important public health
issue of our time.”C. Everett Koop, M.D., former U.S. Surgeon General
All forms of tobacco are harmful.

8
TRENDS in ADULT TRENDS in ADULT SMOKING, by SEXSMOKING, by SEX——U.S., U.S., 19551955––20092009
Trends in cigarette current smoking among persons aged 18 or older
t
Male
20.6% of adults are current
smokers
PHSGraph provided by the Centers for Disease Control and Prevention. 1955 Current Population Survey; 1965–2005 NHIS. Estimates since 1992 include some-day smoking.
Per
cen
t
70% want to quit70% want to quit
Female 23.5%17.9%
Year
PHS
Henry Waxman 1994Henry Waxman 1994It is sometimes easier to invent fiction than to
face the truth. The truth is that cigarettes are the
single most dangerous consumer product ever
sold Nearly a half million Americans die every
PHS
sold. Nearly a half million Americans die every
year as a result of tobacco. This is an
astounding, almost in- comprehensible statistic.
Imagine our Nation's outrage if two fully loaded
jumbo jets crashed each day, killing all aboard.
Yet that is the same number of Americans that
cigarettes kill every 24 hours.45
PHS46
PHS47
PHS48
9
PHS49
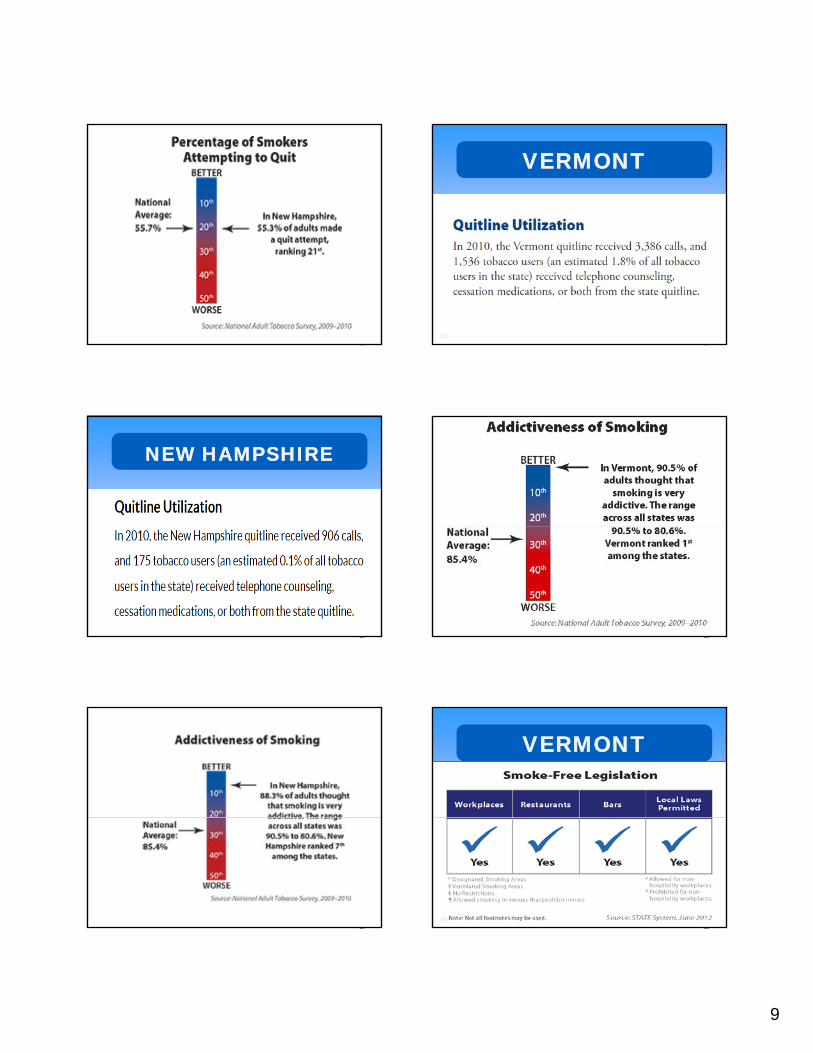
VERMONTVERMONT
PHS50
NEW HAMPSHIRENEW HAMPSHIRE
PHS51
PHS52
PHS53
VERMONTVERMONT
PHS54
10
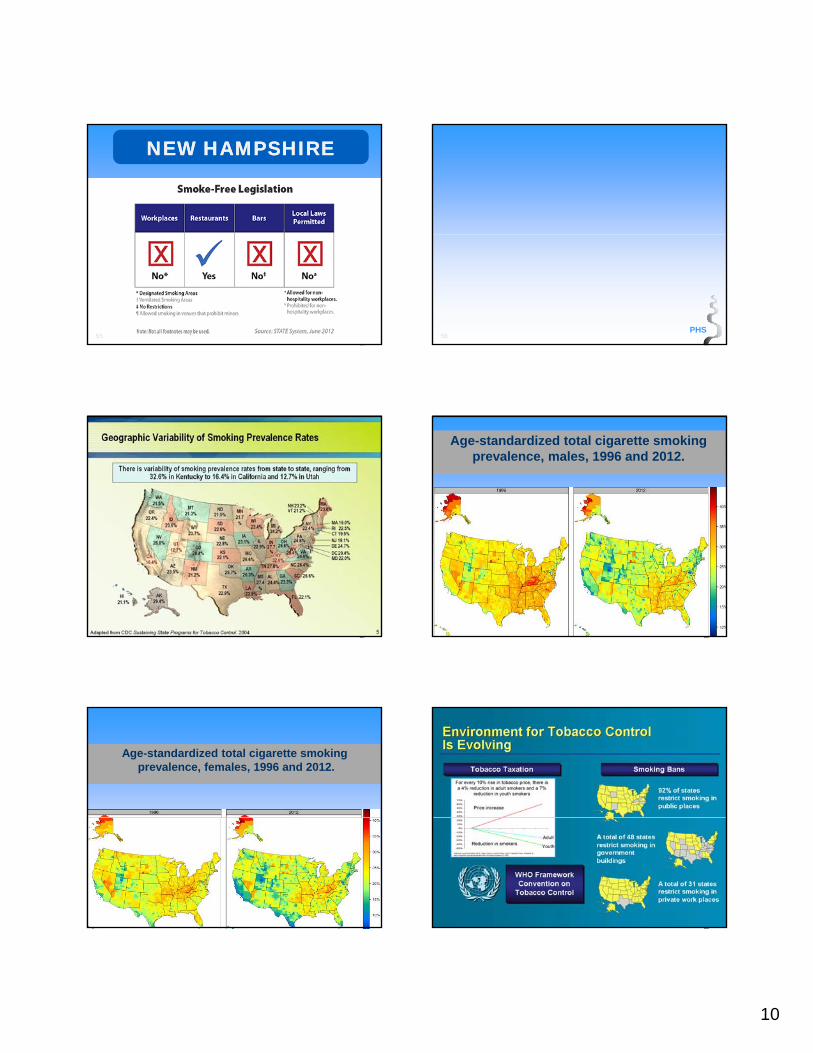
NEW HAMPSHIRENEW HAMPSHIRE
PHS55
PHS56
PHS
Age-standardized total cigarette smoking prevalence, males, 1996 and 2012.
PHS58
Age-standardized total cigarette smokingprevalence, females, 1996 and 2012.
PHS59
PHS

11
“Smoking will retard wound healing, whether the wound is surgical or the result of trauma or burns”
PHS
Silverstein P: Smoking and wound healing. Presented at the Medical Leadership Conference: Effects of Cigarette Smoking -- A Global Perspective,Washington, DC, July 18, 1991.
“Wound complications after breast reduction surgery or mastectomy are 30-50% higher in women who smoke”
PHS
Silverstein P: Smoking and wound healing. Presented at the Medical Leadership Conference: Effects of Cigarette Smoking -- A Global Perspective,Washington, DC, July 18, 1991.
“Patients who smoked regularly before surgery had twice the risk of wound infections as non-smokers”
PHS
Jones RM: Smoking before surgery: The case for stopping. BR Med J1985;290(6484):1763-1764
“Recovery room stays are 20% longerfor smokers than non-smokers”
PHS
Handlin DS, Baker T, Woolwich J: Effect of smoking on duration in recovery room.Anesthesiology 1990;73(8):1052.
“Smoking slows the healing of peptic duodenal ulcers and increases the rate of ulcer relapse”
PHS
Kuipers EJ, Hazenberg HJ, Quik RF, et al: Nizatidine versus ranitidine in the treatment of peptic ulcer disease: Report on the Dutch investigation as part of a European multi-centre trial. Neth J Med 1990;37(i-2):58-62.
“A smoker’s broken bones takealmost twice as long to healcompared to those of a non-smoker”
PHS
USA Today, February 1995

12
It pays to quit smokingIt pays to quit smoking--Literally!Literally!
Moderate smokers (1 ppd) = $8/day, $64/week,
$3328 a year, that’s $33,280 in 10 years!
H k (3 d) $24/d $168/ k
PHS
Heavy smoker (3 ppd) = $24/day, $168/week,
$8736 a year, that’s $87,360 in 10 years!
Smokers may spend up to 8% of their annual
income a year on the purchase of cigarettes,
which can profoundly affect the financial well
being of their families.
67
“Indeed it is difficult to identify any other condition that presents such a mix of lethality prevalence and
PHS
lethality, prevalence, and neglect, despite effective and readily available interventions.”
Fiore et al, U.S. Department of Health and Human Services June 2000
PHS
PHS PHS
13
PHS PHS
PHS
Peripheral Effects of NicotinePeripheral Effects of Nicotine Increased Heart rate
Increased Blood pressure
Vasoconstriction
Increased metabolic rate
PHS
Increased metabolic rate
Lipolysis
Skeletal muscle relaxation
EEG desynchronization
Increased ACTH Adrenal steroids
Psychological Effects of Psychological Effects of NicotineNicotine Stimulation
Arousal
Memory
Attention
I d d f i
PHS
Increased speed of processing
Relaxation
Anxiolytic/stress reduction
Analgesia
Mood improvement
Appetite suppression
Social facilitationPHS
14
ANNUAL SMOKINGANNUAL SMOKING--ATTRIBUTABLE ECONOMIC ATTRIBUTABLE ECONOMIC COSTSCOSTS
Health-care expenditures
Lost productivity costs
T t l f d l t t
$96.7 billion
$97.6 billion
PHS
0 50 100 150 200
Societal costs: $10.28 per pack of cigarettes smoked
Total economic burden of smoking, per year
Billions of US dollars
Centers for Disease Control and Prevention (CDC). (2008). MMWR 57:1226–1228.
Total Medicare program costs
Total federal-state Medicaid program costs $30.9 billion
$18.9 billion
$194 billion
2008 PHS Clinical Practice 2008 PHS Clinical Practice Guideline: Treating Tobacco Use Guideline: Treating Tobacco Use and Dependence Updateand Dependence UpdateHistory:
1. 1996—Initial Guideline published;
literature from 1975–1995;
PHS80
approximately 3,000 articles
2. 2000—Revised Guideline published;
literature from 1995–1999;
approximately 6,000 articles
3. 2008—Updated Guideline published;
literature from 1999–2007;
approximately 8,700 total articles
Combinations: Medication and Combinations: Medication and CounselingCounseling
Effectiveness of and estimated abstinence rates for the combination of counseling and medication versus counseling alone (n = 9 studies)
Estimated Estimated
PHS81
TreatmentNumber
of arms
Estimated
odds ratio
(95% C.I.)
Estimated
abstinence
rate (95% C.I.)
Counseling
alone11 1.0 14.6
Medication
and
counseling
131.7
(1.3, 2.1)
22.1
(18.1, 26.8)
ProPro--Active QuitlinesActive QuitlinesEffectiveness of and estimated abstinence rates for quitline counseling compared to minimal interventions, self-help or no counseling (n = 9 studies)
InterventionNumber
of arms
Estimated
odds ratio
Estimated
abstinence rate
PHS82
of arms(95% C.I.) (95% C.I.)
Minimal or
no counseling
or self-help
11 1.0 8.5
Quitline
counseling 11
1.6
(1.4, 1.8)
12.7
(11.3, 14.2)
Effectiveness of and estimated abstinence rates for quitline counseling and medication compared to medication alone (n = 6 studies)
InterventionNumber
of arms
Estimated
odds ratio
Estimated
abstinence rate
ProPro--Active QuitlinesActive Quitlines
PHS83
of arms(95% C.I.) (95% C.I.)
Medication alone 6 1.0 23.2
Medication and
quitline counseling 6
1.3
(1.1, 1.6)
28.1
(24.5, 32.0)
Medications are effective, but they are just one component of comprehensive treatment for tobacco cessation.
Behavior change is equally important.
PHS
CLOSE TO HOME © 2000 John McPherson. Reprinted with permission of UNIVERSAL PRESS SYNDICATE.
All rights reserved.
15
TOBACCO TOBACCO TREATMENTTREATMENT MedicationMedication
Seven first-line medications shown to be effective and recommended for use by the Guideline Panel:
– Nicotine Patch
PHS86
– Nicotine Gum– Nicotine Lozenge– Nicotine Inhaler– Nicotine Nasal Spray– Bupropion SR – Varenicline
Absorption of NicotineAbsorption of Nicotine
Nicotine is carried on tar droplets
Absorption depends on pH
Most cigarette smoke is acidic and absorbed
PHS
Most cigarette smoke is acidic and absorbed by the lungs, 1-2 mg nicotine/cigarette
Some tobacco smoke (pipe, cigar) is alkaline and absorbed through the mouth, amount absorbed is then highly variable.
TTS Course U Mass Medical School
Nicotine Patches1mg /1cigarette
21 mg14 mg7 mg7 g
PHS89
Nicotine InhalerNicotine Inhaler
PHS90
16
PHS91
PHS92
Medication RecommendationMedication RecommendationRecommendation: Certain combinations of first-line medications have been shown to be effective smoking cessation treatments. Therefore, clinicians should consider using these combinations of medications with their patients who are willing to quit. Effective combination medications are:
PHS93
combination medications are:
* Long-term (> 14 weeks) nicotine patch + other NRT (gum and spray)
* The nicotine patch + the nicotine inhaler
* The nicotine patch + bupropion SR.
(Strength of Evidence = A)
PHS94
VareniclineVareniclineEffectiveness and abstinence rates for various medications and medication combinations compared to placebo at 6-months post-quit (n = 86 studies)
M di tiNumber
Estimated
dd ti
Estimated
b ti t
PHS95
Medicationof arms
odds ratio
(95% C. I.)
abstinence rate
(95% C. I.)
Placebo 80 1.0 13.8
Varenicline
(2 mg/day)5
3.1
(2.5, 3.8)
33.2
(28.9, 37.8)
PHS96
17
PHS97
PHS98
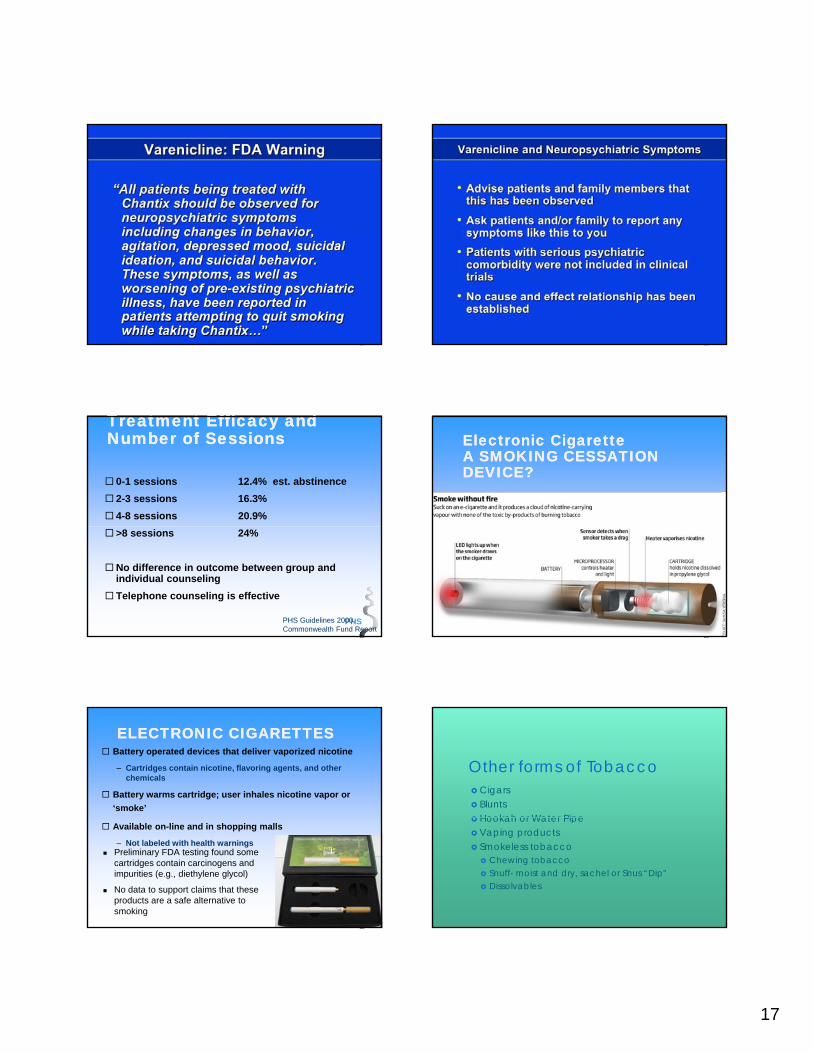
Treatment Efficacy and Treatment Efficacy and Number of SessionsNumber of Sessions
0-1 sessions 12.4% est. abstinence
2-3 sessions 16.3%
4-8 sessions 20.9%
PHS
>8 sessions 24%
No difference in outcome between group and individual counseling
Telephone counseling is effective
PHS Guidelines 2000,Commonwealth Fund Report
Electronic CigaretteElectronic CigaretteA SMOKING CESSATION A SMOKING CESSATION DEVICE?DEVICE?
PHS100
ELECTRONIC CIGARETTESELECTRONIC CIGARETTES Battery operated devices that deliver vaporized nicotine
– Cartridges contain nicotine, flavoring agents, and other chemicals
Battery warms cartridge; user inhales nicotine vapor or
‘smoke’
PHS
Available on-line and in shopping malls
– Not labeled with health warnings Preliminary FDA testing found some
cartridges contain carcinogens and impurities (e.g., diethylene glycol)
No data to support claims that these products are a safe alternative to smoking
Other forms of Tobacco Cigars Blunts Hookah or Water Pipe Hookah or Water Pipe Vaping products Smokeless tobacco
Chewing tobacco Snuff- moist and dry, sachel or Snus “Dip” Dissolvables

18
Dual Tobacco Use
Combustible plus non combustible tobacco types
Convenient packaging facilitates Convenient packaging facilitates availability and ease of using both types of products.
Snus package can fit just about anywhere, can be used in places where you cannot smoke.
From Cigarette to Vapor Pen, an evolution in technology
PHS-Sponsored Clinical Practice Guideline Treating Tobacco Use and Dependence: 2008 Update
PHS
Roll Your Own Cigarettes
Roll in rolling machine or by hand “rollies” Use increases when branded cigarette prices go up Pipe tobacco Pipe tobacco Greater tar and nicotine yields/cigarette Likely inhale differently or more deeply, depositing
smoke, nicotine and toxins in lungs Greater urinary concentrations of toxins Increases risks for lung and oral cancers Low cost=more affordable
Addict Biol, 14, 2009, page 315 Tobacco Control, June 1998, Darrall & Figgins, page 168.
Cloud Vape Pen
19
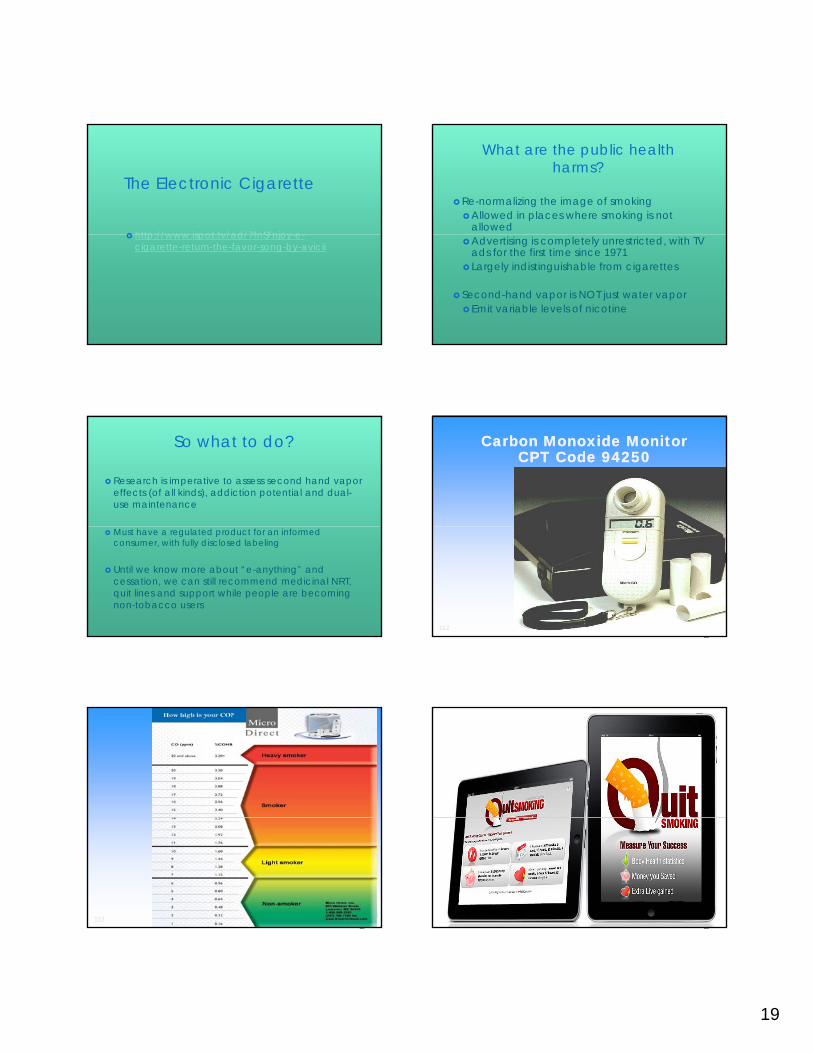
The Electronic Cigarette
http://www ispot tv/ad/7fnS/njoy e http://www.ispot.tv/ad/7fnS/njoy-e-cigarette-return-the-favor-song-by-avicii
What are the public health harms?
Re-normalizing the image of smokingAllowed in places where smoking is not
allowedAdvertising is completely unrestricted, with TV
ads for the first time since 1971 Largely indistinguishable from cigarettes
Second-hand vapor is NOT just water vaporEmit variable levels of nicotine
So what to do?
Research is imperative to assess second hand vapor effects (of all kinds), addiction potential and dual-use maintenance
Must have a regulated product for an informed consumer, with fully disclosed labeling
Until we know more about “e-anything” and cessation, we can still recommend medicinal NRT, quit lines and support while people are becoming non-tobacco users
Carbon Monoxide MonitorCarbon Monoxide MonitorCPT Code 94250CPT Code 94250
PHS112
PHS113
Type: PNG
•660 × 396 (Same size), 154KB•Search by imageImages may be subject to copyright.
PHS114
Type: PNG

20
PHS
Ask Ask about tobacco use. Identify and document tobacco use status for every patient at every visit.
AdviseAdvise to quit. In a clear, strong and personalized manner urge every tobacco user to quit.
AssessAssess willingness to make a quit attempt Is the tobacco user
The "5 A's" Model for Treating The "5 A's" Model for Treating Tobacco Use and Dependence Tobacco Use and Dependence --20002000
PHS116
AssessAssess willingness to make a quit attempt. Is the tobacco user willing to make a quit attempt at this time?
Assist Assist in quit attempt. For the patient willing to make a quit attempt, use counseling or pharmacotherapy to help him or her quit.
ArrangeArrange followup. Schedule followup contact, preferably within the first week after the quit date.
BRIEF COUNSELING: BRIEF COUNSELING: ASK, ADVISE, REFERASK, ADVISE, REFER
ASK about tobacco USE
ADVISE tobacco users to QUIT
PHS
REFER to other resources
ASSIST
ARRANGE
Patient receives assistance, with follow-up counseling
arranged, from other resources such as the
tobacco quitline
Brief interventions have been shown to be
effective
In the absence of time or expertise:
BRIEF COUNSELING: BRIEF COUNSELING: ASK, ADVISE, REFER ASK, ADVISE, REFER (cont’d)(cont’d)
PHS
In the absence of time or expertise:
– Ask, advise, and refer to other resources, such as local group programs or the toll-free quitline1-800-QUIT-NOW This brief
intervention can be achieved in less than 3 minutes.
30
ence
at
s
n = 29 studies
With help from a clinician, the odds of quitting approximately doubles.
Compared to patients who receive no assistance from a clinician, patients who receive assistance are 1.7–2.2 times as likely to quit successfully for 5 or more months.
CLINICIANS CAN MAKE a CLINICIANS CAN MAKE a DIFFERENCEDIFFERENCE
PHS
0
10
20
No clinician Self-helpmaterial
Nonphysicianclinician
Physicianclinician
Type of Clinician
Esti
mat
ed a
bsti
ne5+
mon
ths
1.0 1.11.7
2.2
Fiore et al. (2008). Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, May 2008.
WHAT ARE WHAT ARE “TOBACCO QUITLINES”?“TOBACCO QUITLINES”?
Tobacco cessation counseling, provided at no
cost via telephone to all Americans
Staffed by trained specialists
PHS
Staffed by trained specialists
Up to 4–6 personalized sessions (varies by
state)
Some state quitlines offer pharmacotherapy at
no cost (or reduced cost)
Up to 30% success rate for patients who
complete sessionsMost health-care providers, and most patients,
are not familiar with tobacco quitlines.
21
PHS121
PHS122
PHS
Insurance Coverage of Cessation Treatments is Cost Effective
Cessation treatments are both clinically effective and highly cost-effective relative to interventions for other clinical disorders.
Cost-effectiveness analyses have shown that tobacco dependence treatment that tobacco dependence treatment compares favorably with routinely reimbursed medical interventions such as the treatment of hypertension and high cholesterol, as well as preventive screening interventions such as periodic mammography and PAP tests.
Current Status of Cessation Coverage
Nine states have laws or regulations in place requiring at least some private insurance plans to cover certain cessation treatments.
(Colorado, Illinois, Maryland, New Jersey, New Mexico, North Dakota, Oregon, Rhode Island, and Vermont)
Medicaid Coverage and the ACA
Section 4107 of the Affordable Care Act requires all state Medicaid programs to provide a comprehensive tobacco cessation benefit as defined by the USPHS guidelines to pregnant women who are enrolled in Medicaid, effective October 2010
As of January 2014, Section 2502 of the law bars state Medicaid programs from excluding cessation medications, including over-the-counter medications, from coverage.

22
Medicare Coverage Medicare recipients have access to individual
cessation counseling and prescription cessation medications.
Th b fit t it tt t d The benefit covers two quit attempts a year and four counseling sessions per quit attempt.
Medicare copayment, coinsurance, and deductibles for cessation treatments are waived under the Affordable Care Act, effective January 1, 2011.
HELPING PATIENTS QUIT HELPING PATIENTS QUIT IS a CLINICIAN’S IS a CLINICIAN’S RESPONSIBILITYRESPONSIBILITY
TOBACCO USERS DON’T PLAN TO FAIL.MOST FAIL TO PLAN.
PHSTHE DECISION TO QUIT LIES IN THE HANDS OF EACH PATIENT.
Clinicians have a professional obligation to address tobacco use and can have an important role in helping patients
plan for their quit attempts.
PHS129
PHS130
FIVE YEAR SURVIVAL65 year old patients with:
• Early stage non-small cell lung CA33% for continued smokers70% for smokers who quit
PHS131
70% for smokers who quit
• Limited stage small cell lung CA29% for continued smokers63% for smokers who quit

23
Tobacco Dependence Tobacco dependence is a chronic disease,
with most smokers making multiple quit attempts before succeeding.
Many of these smokers require repeated intervention.
PHS
THANK YOU!(For not smoking)(For not smoking)