Elzouki An

of 39
-
Upload
yoser-thamtono -
Category
Documents
-
view
213 -
download
0
Transcript of Elzouki An
-
7/28/2019 Elzouki An
1/39
Clinical Management of Hepatocellular
Carcinoma: Current Options
Abdel-Naser Elzouki, MBChB, DTM&H, MSc, MD, PhD, FRCP (UK)
Professor & Sr. Consultant, Department of Medicine,
Hamad Medical corporation, Doha, Qatar
Email: [email protected]
mailto:[email protected]:[email protected] -
7/28/2019 Elzouki An
2/39
Hepatocellular Carcinoma (HCC): Content
Burden of HCC Diagnosis of HCC
Staging of HCC
Treatment of HCC:
- Very early / early HCC
- Intermediate HCC
- Advanced HCC
A Look to the future
-
7/28/2019 Elzouki An
3/39
HCC: Common and Increasing
694,000 deaths from liver cancer yearly worldwide
[1]
Age-adjusted US incidence has increased 2-fold from 1985
1998[2]
- Expected to continue to increase until 2015-2020[3]
American Cancer Society statistics for liver cancer in 2010[
- Estimated new cases: 24,120
- Estimated deaths: 18,910
- 5th leading cause of cancer deaths in males
1. GLOBOCAN 2008. 2. SEER stat fact sheets: liver and intrahepatic bile duct. 3. Llovet JM. J Gastroenterol.2005;40:225-235. 4. American Cancer Society. Cancer facts & figures 2010.
-
7/28/2019 Elzouki An
4/39
Evolving Guidelines for Clinical Management
of Hepatocellular Carcinoma
www.aasld.org
-
7/28/2019 Elzouki An
5/39
Radiological Diagnosis of Hepatocellular Carcinoma in Patien
With Cirrhosis: EASL/AASLD Guidelines
Imaging techniques contrast-enhanced US, contrast-enhanced spiral CTand gadolinium-enhanced MRI
Pathognomonic features wash-in followed by wash-out
< 2 cm node two concordant contrast imaging techniques
> 2 cm node one contrast imaging technique only
EASL, AASLD & JSH Conference, Barcelona 2005; AASLD Practice Guidelines 2007; *Forner et al 2008
Prospective validation* 89 patients with a 7-20 mm nodule
CE-US+MRI Sensitivity 33.3%
Specificity 100%
-
7/28/2019 Elzouki An
6/39
Abdominal tri-phasic spiral CT
Right lobe hepatic focal lesion 5 x 4.5 cm, with arterialenhancement and wash out in the porto-venous phase.
-
7/28/2019 Elzouki An
7/39
Ultrasound alone Ultrasound + AFP
Ultrasound Diagnosis of Early-stage HCC in Patients
with Cirrhosis. Meta-analysis
Singal et al Aliment Pharmacol Ther 2009;30:37-47
-
7/28/2019 Elzouki An
8/39
Liver nodule
< 1 cm > 1 cm
Reapeat US at 3 months
Growing/changing
characterStable
Investigateaccording to size
4 phase MDCT/dynamic
Contrast enhanced MRI
Arterial hypervascularity ANDvenous or delayed phase washout
Other contrast enhanced
Study (CT or MRI)
Arterial hypervascularity AND
venous or delayed phase washout
Yes No
Yes No
HCC Biopsy
2010 AASLD Algorithm for Investigation of Small Nodule
Found On Screening in Patients with Cirrhosis
Bruix J and Sherman M. AASLD Practice Guidelines 2010: Management of Hepatocellular Carcinoma; www.aasld.org
-
7/28/2019 Elzouki An
9/39
Staging Systems and Treatment Strategies
in Hepatocellular Carcinoma
-
7/28/2019 Elzouki An
10/39
Marrero JA, et al. Hepatology. 2005;41:707-716
Variables Used in HCC Staging Systems
System Tumor Staging Liver Function Endorsement
Europe-US
GETCH/
French
PVT; AFP < 35 or > 35 ug/L Bilirubin, alkaline phosphatase -
CLIP Number of nodules, tumor > or < 50% area of
liver, and PVT;
AFP< 400 or 400 ng/mL
CTP AHPBA
BCLC Tumor size, number of nodules, and PVT CTP AASLD, EASL
TNM Number of nodules, tumor size, presence of PVT,
and presence of metastasis
No AJCC
Asia
JIS TNM CTP -
Okuda/
Tokyo
Tumor > or < 50% of cross-sectional area of liver Ascites, albumin, and bilirubin -
CUPI TNM; AFP< 500 or 500 ng/mL Bilirubin, ascites, alkaline
phosphatase
-
-
7/28/2019 Elzouki An
11/39
Comparison of HCC Staging Systems
BCLC system uses key independent predictors of survival: Performance score, portal vein thrombosis, tumor diameter
Compared with other staging systems in cohort study
BCLC had best stratification of survival across all stages
BCLC was only system to have independent predictive value onsurvival
BCLC is the only staging system that stratifies patients into
treatment groups
Marrero JA, et al. Hepatology. 2005;41:707-716
-
7/28/2019 Elzouki An
12/39
The Barcelona Clinic Liver Cancer (BCLC) Staging Classificat
for Hepatocellular Carcinoma Is Endorsed by EASL/AASLD
A Very Early/Early
B Intermediate
CAdvanced
D End-stage
BCLC stage
0
0
1-2
3-4
Performance
status
Single < 5 cm or 3 nodes
< 3 cm each
Large/multinodular
Vascular invasion and/or
extrahepatic spread
Any of the above
Tumor volume,number
and invasiveness
A & B
A & B
A & B
C
Child-Pugh
Expected
survival
50-75% at 5 yr
16 months
6 months
< 3 months
-
7/28/2019 Elzouki An
13/39
Therapies used in the management of HCC
Surgery:
- Resection
- Liver transplantation
Locoregional therapy:
- Percutaneous ethanol injection
- Radiofrequancy thermal ablation
- Trans-Arterial Chemo-Emobilisation (TACE)
- Trans-Arterial Radio-Emobilisation (TACE)
Systemic therapy:
- Targeted molecular therapy
- Symptomatic treatment
-
7/28/2019 Elzouki An
14/39
Treatment ofVery Early / Early Stage HCC
-
7/28/2019 Elzouki An
15/39
The Barcelona Clinic Liver Cancer (BCLC) Staging Classificat
for Hepatocellular Carcinoma Is Endorsed by EASL/AASLD
A Very Early/Early
BCLC stage
0
Performance
status
Single < 5 cm or 3 nodes
< 3 cm each
Tumor volume,number
and invasiveness
A & B
Child-Pugh
Expected
survival
50-75% at 5 yr
-
7/28/2019 Elzouki An
16/39
Early Stage Hepatocellular Carcinoma: Survival after Resecti
Is Influenced by Portal Hypertension and Bilirubin
Best candidates for resection : Solitary HCC 5 cm
Child-Pugh A: Low portal hypertension
Normal bilirubin
0
20
40
60
80
100
0 12 24 36 48 60 72 84 96
< 10 mmHg HVPG (n= 35)
10 mmHg HVPG and normal bilirubin (n=15)
10 mmHg HVPG and Bilirubin >1 mg/dL (n=27)
Log Rank 0.00001
Survival(%
)
months
74%
50%
25%
Llovet JM et al, Hepatology 1999;30:1434-40
f CC
-
7/28/2019 Elzouki An
17/39
Liver Transplantation for HCC:
Milan Criteria (Stage 1 and 2)
+Absence of macroscopic vascular invasion,
absence of extrahepatic spread
Single tumor, not > 5 cm Up to 3 tumors, none > 3 cm
Ref: Mazzaferr o V, et al. N Eng l J Med. 1996;334:693-699.
Strategy to expand criteria include use of locoregional therapy to downstagepatients to Milan criteria
T t t f E l St HCC Li T l t ti i
-
7/28/2019 Elzouki An
18/39
Treatment of Early Stage HCC: Liver Transplantation in
Cirrhotic Patients Selected by Milan Criteria
Milan
Barcelona
Paris
Berlin
Center
Single 5 cm
3 nodes 3cm
Single 5 cm
3 nodes 3 cm
Single 5 cm
3 nodes 3 cm
HCC
48
79
45
120
Cases
Mazzaferro et al 199
Llovet et al 1998
Bismuth et al 1999
Jonas et al 2001
Reference5-yr survival Recurrence
8%
4%
11%
16%
75%*
75%
74%
71%
Explanted livers: 35 (73%) Milan (+) with 95% survival
13 (27%) Milan () with 59% survival
*
* 4-yr survival
P ti t ith Ci h i d HCC ithi Mil C it i
-
7/28/2019 Elzouki An
19/39
Patients with Cirrhosis and a HCC within Milan Criteria
Liver Resection or Transplantation
Poon RTP et al Ann Surg 2007;245:51-58
Survival predictors: HCV neg, 3 cm tumor, single tumor, no venous invasion.
Resection (n=204)
Transplantation(n=43)
p=0.017
Months after surgery
Cumulativesurvival
(%)
0 12 24 36 48 60
0
20
40
60
80
100
Per-Protocol Analysis
Cumulativesurvival(%)
Resection (n=228)
Transplantation(n=85)
p=0.088
Months
0 12 24 36 48 60
0
20
40
60
80
100
ITT Analysis
Hong-Kong, Queen Mary Hosp. Data-base: 1995-2004. Cirrhotics with HCC within Milan criteria
204 resected and 43 transplanted (30 LDLT). 218 (88%) HBsAg pos. 33 (13%) 2 or 3 nodules.
T t t f E l HCC th I iti l T V l
-
7/28/2019 Elzouki An
20/39
Treatment of Early HCC: the Initial Tumor Volume
Predicts Survival After Percutaneous Ablation
Sala M et al Hepatology 2004;40:1352-1360
0 12 24 36 48 60 72
34 32 26 17 13 9 7
87 78 52 31 19 10 5
0
10
20
30
40
5060
70
80
90
10097%
63%
32%
96%
56%
72%
Log-rank=.0075
Single 2 cm
Single 2.1-5 cm
Single 2 cm
Single 2.1-5 cm
months
Survival(
%)
Patients at risk
A retrospective study of 282 consecutive patients with a HCC within Milan criteria treated
at BCLC, Barcelona during a 15-yr period.
-
7/28/2019 Elzouki An
21/39
Ablation of HCC
Percutaneous ethanol injection (PEI)
Cryotherapy
Radiofrequency ablation (RFA)
S i it f R ti Al h l I j ti i th T t
-
7/28/2019 Elzouki An
22/39
Superiority of Resection vs Alcohol Injection in the Treatmen
of 2-5 cm HCC: A Nationwide Survey in Japan
Arii S et al, Hepatology 2000;32:1224-1229
Clinical stage 1: solitary node 2-5 cm size
Resection n=2722
PEIT n=587
0 12 24 36 48 60 72 84 960
10
20
30
40
50
60
70
80
90
100
months
survivalrate(%)
800 hospitals, patients with < 5 cm tumors
8,010 treated by hepatic resection4,037 treated by PEIT841 treated by chemoembolization
Clinical stage 1: Ascites noneBilirubin < 2.0 mg/dlAlbumin > 3.5 g/dlICGR 15 < 15%Protime > 80%
58%
39%
The Liver Cancer Study Group: 1988-1996
-
7/28/2019 Elzouki An
23/39
Radiofrequency vs Percutaneous Ethanol Injection Therapyfor Hepatocellular Carcinoma: a Meta-analysis
Germani G et al J Hepatol 2010;52:380-388
Mortality rates
-
7/28/2019 Elzouki An
24/39
-
7/28/2019 Elzouki An
25/39
Treatment ofIntermediate Stage HCC
The Barcelona Clinic Liver Cancer (BCLC) Staging Classificat
-
7/28/2019 Elzouki An
26/39
The Barcelona Clinic Liver Cancer (BCLC) Staging Classificat
for Hepatocellular Carcinoma Is Endorsed by EASL/AASLD
A Very Early/Early
B Intermediate
BCLC stage
0
0
Performance
status
Single < 5 cm or 3 nodes
< 3 cm each
Large/multinodular
Tumor volume,number
and invasiveness
A & B
A & B
Child-Pugh
Expected
survival
50-75% at 5 yr
16 months
T t t f HCC Ch b li ti
-
7/28/2019 Elzouki An
27/39
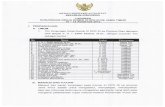
Treatment of HCC: Chemoembolization
Normal liver gets 75% of blood supply
from portal vein and 25% of blood
supply from hepatic artery
Tumor receives most of its blood supply
from the hepatic artery Injection into the hepatic artery spares
most of the normal liver
Embolization of the hepatic artery
induces ischemic necrosis of tumor
Tumor
Liver
Portal vein
Hepaticartery
Catheter placement forchemoembolization
Selective arterial radiotherapy with Y90 microspheres
Intermediate HCC: The Outcome of Chemoembolization
-
7/28/2019 Elzouki An
28/39
Intermediate HCC: The Outcome of Chemoembolization
A Meta-analysis
Bruix J et al, Gastroenterology 2004;127:S179-88
Lin , Gastroenterology 1988 63
GRETCH, NEJM 1995 96
Llovet, Lancet 2002 112
Pelletier, J Hepatol 1998 70
Bruix , Hepatology 1998 80
Overall 503
Heterogeneity: Q:7.73 P=0.14
Author,Journal year Patients
Lo, Hepatology 2002 79
Favors treatment Favors control
1010.10.01 1000.5 2
p=0.017
Random effects model (DerSimonian & Laird).
OR (95% IC)
Improved survival: from 16 to 20 months
-
7/28/2019 Elzouki An
29/39
Treatment ofAdvanced Stage HCC
The Barcelona Clinic Liver Cancer (BCLC) Staging Classificat
-
7/28/2019 Elzouki An
30/39
The Barcelona Clinic Liver Cancer (BCLC) Staging Classificat
for Hepatocellular Carcinoma Is Endorsed by EASL/AASLD
A Very Early/Early
B Intermediate
CAdvanced
BCLC stage
0
0
1-2
Performance
status
Single < 5 cm or 3 nodes
< 3 cm each
Large/multinodular
Vascular invasion and/or
extrahepatic spread
Tumor volume,number
and invasiveness
A & B
A & B
A & B
Child-Pugh
Expected
survival
50-75% at 5 yr
16 months
6 months
Levels of Evidence in the Assessment of Benefits in
-
7/28/2019 Elzouki An
31/39
Systemic treatment Benefit Evidence
Sorafenib Increased survival 1iA
Tamoxifen No benefit 1iA
Systemic chemotherapy No benefit 1iiA
Interferon No benefit 1iiA
the Treatment of Advanced HCC
LLovet JM et al JNCI 2008;100:698-711
Randomized Controlled Trials of Sorafenib in
-
7/28/2019 Elzouki An
32/39
Advanced Hepatocellular Carcinoma
Study characteristics SHARP Study1 Asia Study2
Median age 65 yrs 51 yrs
BCLC-B stage 18% 4%
Previous treatments 67% na
HBV etiology of cirrhosis 19% 71%
TTP (control) 5.5 mo. (2.8 mo.) 2.8 mo. (1.4 mo.)
Median survival (control) 10.7 mo. (7.9 mo.) 6.5 mo. (4.2 mo.)
Grade 3/4 toxicity 30% 24%
1 Llovet JM et al NEJM 2008;359:378-390; 2Cheng A et al Lancet Oncol 2009;10:25-34
-
7/28/2019 Elzouki An
33/39
Treatment ofTerminal Stage HCC
The Barcelona Clinic Liver Cancer (BCLC) Staging Classificat
-
7/28/2019 Elzouki An
34/39
( ) g g
for Hepatocellular Carcinoma Is Endorsed by EASL/AASLD
A Very Early/Early
B Intermediate
CAdvanced
D End-stage
BCLC stage
0
0
1-2
3-4
Performance
status
Single < 5 cm or 3 nodes
< 3 cm each
Large/multinodular
Vascular invasion and/or
extrahepatic spread
Any of the above
Tumor volume,number
and invasiveness
A & B
A & B
A & B
C
Child-Pugh
Expected
survival
50-75% at 5 yr
16 months
6 months
< 3 months
Tailoring Treatment According to the Clinical Stage of HC
-
7/28/2019 Elzouki An
35/39
Tailoring Treatment According to the Clinical Stage of HC
Very earlystage (0)
Earlystage (A)
Intermediatestage (B)
Advancedstage (C)
Terminalstage (D)
HCC
PEI/RFLiver transplantationResection Chemoembolization Sorafenib
RCTs (50-60%) Median survival untreated: 6-16 months
Symptomatictreatment (10%)
Survival
-
7/28/2019 Elzouki An
36/39
A Look To The Future
Molecular Therapies Under Evaluation for HCC in Phase III (2011)
-
7/28/2019 Elzouki An
37/39
Molecular Therapies Under Evaluation for HCC in Phase III (2011)
Targeted Population Phase III Comparison
Adjuvant Prevent recurrences 1. Sorafenib vs placebo
2. Retinoids vs placebo
Intermediate HCC Improve TACE 1. TACE sorafenib
2. TACE brivanib
Advanced HCC First line:
Second line:
1. Sorafenib erlotinib
2. Sorafenib vs brivanib3. Sorafenib vs sunitinib
4. Sorafenib vs lifitinib
5. Sorafenib Y90
6. Sorafenib doxorubicin
1. Brivanib vs placebo
2. Everolimus vs placebo
3. Ramucirumab vs placebo
NEGATIVE:ASCO 2010
HALTED:2010
Conclusion
-
7/28/2019 Elzouki An
38/39
Conclusion
Burden of HCC is increasing
Requirements for diagnosis depends on patient
characteristics and tumor characteristics
BCLC staging system recommended by US and
European guidelines BCLC system provides framework for selection of
treatment
Many studies ongoing for treatment of HCC
-
7/28/2019 Elzouki An
39/39