肺栓塞 --- 沉寂的 “ 杀手 ” 90% PE 患者血栓来自下肢 静脉 80% PE 患者起病时无临床 症状 2/3 PE 患者死亡在 2 小时内 发生.

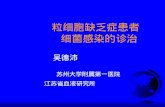
認知症関連外来に来る患者さん(疾患)と症状
物忘 物忘 外来 aMCI, AD, AGD, DLB行動異常 精神科 神経内科 FTD, DLB歩行障害 神経内科 内科 整形外科 BD, iNPH 全身病 総診 救急 内科 DLB, BD
aMCI: 軽度認知障害 AD: 病 AGD: 嗜銀顆粒認知症 経過 高齢者 AD 次 頻度 DLB: 小体型認知症 FTD:前頭側頭型認知症 BD: ―病 血管性認知症 主要型 iNPH:特発性正常圧水頭症
赤字は生活習慣病対策や抗認知症薬の効果が期待できる疾患
青字は降圧薬や外科療法が期待できる疾患
初発症状 訪 外来 疾患

細胞変性型認知症
病 取 繕
小体型認知症(幻覚 病
前頭 側頭型認知症(行動異常 性格変化 血管性認知症 病 歩行/嚥下障害 自発性低下 重症脳卒中 片麻痺/失語 寝 単発梗塞性健忘 脳梗塞 記憶障害
正常圧水頭症 二次性 加 認知症 割合 3:2:1
認知症 割合

3
特発性正常圧⽔頭症(iNPH)
高齢者 歳以上 多 臨床的 区別
前頭側頭型
加齢高齢化
清原裕 原図 秋口改変
病 他 大認知症 関係 前頭側頭型認知症 若年発症 他 認知症 共存

AD DL
B
FTD

前頭側頭型認知症 神経変性 認知症 一 脳 一部 前頭葉 側頭葉前方 委縮 細胞脱落 Tau 異常蛋白 蓄積 50 60歳代 比較的若 発症 65歳未満 起 若年性認知症 主 原因 2015年 厚生労働省 指定難病 認定
脳 中 前頭葉 人格 社会性 言語 側頭葉 記憶 聴覚 言語 前頭側頭葉型認知症 発症 他 認知症 違 特徴的 症状 示 社会性 欠如 万引 軽犯罪 起 身 無頓着 社会性 欠如 抑制 効 相手 対 遠慮 相手 対 暴力 度 越 同 繰 返 同 道順 歩 続 同 動作 取 続 常同行動 繰 返 感情 鈍麻 感情 他人 共感 感情移入 感情鈍麻 起 自発的 言葉 低下 相手 言 返 同 言葉 言 続
症状 緩徐 進行 発症後平均6 8年 寝 状態

Pick病/FTLD前頭側頭型皮質変性症概念 変遷
● 病 Pick1892,Onari & Spatz1926 嗜銀 球 (図 黒矢印;Alzheimer1911 細胞/腫大細胞 (後 CBD;Gibb1989) 単純変性所見(高頻度;Constantinidis1974 ●前頭型認知症 FLD of non AD, DFT/FLD, Brun/Neary1987/90 ●前頭側頭型認知症 FTD/FTLD, L&M group/Neary1994/1996 ●遺伝性前頭側頭型認知症 FTDP-17 1997;後 Tau/GRN変異
●進行性失語/意味性認知症 (PNFA/SD, Snowden/Hodges1992) ●進行性核上性麻痺/皮質基底核変性症(PSP/CBD, Mackenzie2011)●ALS 伴 FTL(TDP43/FUS;Okamoto1992,Arai2006,Vance2009)
●FTLD病理分類 Mackenzie2010, ●bvFTD診断基準 Rascovsky2011, ●進行性失語群分類 Gorno-Tempini2011, ●FTLD総説 Mann2017

Arch Neurol. 1993 Aug;50(8):873-80.Frontal-subcortical circuits and human behavior.Cummings JL.OBJECTIVE:This synthetic review was performed to demonstrate the utility of frontal-subcortical circuits in the explanation of a wide range of human behavioral disorders.Reports of patients with degenerative disorders or focal lesions involving frontal lobe or linked subcortical structures were chosen from the English literature. Individual case reports and group investigations from peer-reviewed journals were evaluated.STUDY SELECTION:Studies were included if they described patient behavior in detail or reported pertinent neuropsy-chological findings and had compelling evidence of a disorder affecting frontal-subcortical circuits.Information was used if the report from which it was taken met study selection criteria.DATA SYNTHESIS:Five parallel segregated circuits link the frontal lobe and subcortical structures. Clinical syndromes observed with frontal lobe injury are recapitulated with lesions of subcortical member structures of the circuits. Each prefrontal circuit has a signature behavioral syndrome: executive function deficits occur with lesions of the dorsolateral prefrontal circuit, disinhibition with lesions of the orbitofrontal circuit, and apathy with injury to the anterior cingulate circuit. Depression, mania, and obsessive-compulsive disorder may also be mediated by frontal-subcotical circuits. Movement disorders identify involvement of the basal ganglia component of frontal-subcortical circuits.CONCLUSIONS:Frontal-subcortical circuits mediate many aspects of human behavior




前頭側頭葉変性症 精神症状 行動障害 言語障害 主徴 前頭葉 側頭葉前部 病変 有 神経細胞変性型 認知症 最初 出現 臨床症状 基 行動異常型前頭側頭認知症 意味性認知症 進行性非流暢性失語 分類 病変 前頭葉 中心 側頭葉前半 中心 病 異 脳後方部 保 進行 記憶障害 認 前頭葉 脱落症状 外側前頭葉 実行機能障害 底面 同情 共感性欠如 内側 意欲 自発性欠如 前頭葉 機能低下 脳 後下方 脱抑制症状 後連合野 脱抑制行動 反社会行動 注意転導性 辺縁系 多食 異食 偏食 基底核 常同運動 常同言語 周徊 顕 前頭葉機能 由来 行動異常 併 症状 出現 古典的 病 記載 出発点 症候群 言


前頭葉 機能低下 症状
病識 欠如 病初期 欠如 病感 全 失 感 多 自己 意識 社会的環境 自己 位置 認識 能力 “自己” 主観的意識 保 持 比 較 的 客 観 的 観 点 認 識 能 力 self-awareness 障害 障害 心 理論 障害 説明 試 FTD 臨床診断基準 重視 社会的対人行動 障害 自己行動 統制障害 情意鈍麻 病識 欠如 背景 共通 心的機構 心 理論 障害 捉 研究 注目 自発性低下 自発性 低下 FTD 病初期 常同行動 落 着 無 共存 多 昼寝 思 常同的 周遊 声 一日中同 場所 脳血管 性認知症 自発性低下 趣 異 近縁 症状 抑 状 態 混同 抑 状態 気分 思考面 変化 伴 悲哀感 不安 罪責感 存在 言動 微小妄想 思考面 異変 生 鑑別 可能

後方連合野 抑制障害 症状
被影響性 亢進 環境依存症候 被影響性 亢進 環境依存症候群 後方連合野 本来有 状況依存性 解放 結果 外的刺激 内 的要求 対 被刺激閾値 低下 処理 短絡的 反射的 無反省 理解 日常生活場面 介護者 首 同 首 反響 模倣行為 相手 言葉 返 応 反響言語 何 文 句 即座 歌 歌 出 他患 質問 先 応 視覚 入 看板 文字 読 上 強迫的音読 行為 表 検査場面 物品 検者 動作 提示 時 反応 指示 強迫的 応 物品 場合 呼称 検者 形 手 見 時 V 2 言語化 強迫的 言語応答 転導性 亢進維持困難 行為 持続 続 症状 後方連合野 本来有 状況依存性 解放 結果 外的刺激 内的要求 対 被刺激閾値 低下 注意障害 注意 維持困難 出現 考 Klüver-Bucy症候群 hypermetamorphosis 関連 論 必 外界 刺激 対 過剰 反応 外界 刺激 落 着

辺縁系 抑制障害 症状
脱抑制我 道 行 行動 反社会的 脱抑制 本能 行動 前方連合野 辺縁系 抑制 結果 理解 店頭 駄菓子 堂 万引 検査 取 組 真剣 考 不精 自分 気 答 診察 中 鼻歌 歌 関心 診察室 検査室 勝手 出 立 去 行動 表現 社会的 関係 周囲 配慮 過 指摘 悪 様子 患者本人 悪気 自動車運転 信号無視 高速道路 逆走 社会問題


大脳基底核 抑制障害 症状 常同行動 自発性 低下 無関心 前景 前 全例 認 病 鑑別 重要 症状 日常生活 常 同的周遊 常同的食行動異常 目立 多 一日中数 km 同 歩 続 数十 km 毎日周遊 途中 行 銭泥棒 花 果物 盗 軽犯罪 社会的 問題 決 少数 食品 料理 固執 常同的 食行動 女性 場合 調理 常同的 作 副食 種類 減少 味噌汁 具 変 言語面 何 聞 自分 名前 生年月日 同 語句 答 滞 続言語 同 内容 話 時計症状 形 出現 常同行動 時間軸上 展開 場合 時刻表的生活 絶 膝 手 擦 続 手 叩 反復行動



前頭側頭型認知症 3 主要臨床 病理 遺伝型
bvFTD(FTD) 行動障害型 脱抑制 無気力 常同行為;全病理遺伝型示 * PNFA 進行性非流暢失語 裂;言語表出障害 tau/TDP43蛋白異常
SD 意味性認知症 側頭極 言葉 意味 TDP-43蛋白異常
FTLD-Tau tau: product of MAPT; 細胞内輸送障害 関連 FTLD-TDP43 TDP43:核輸送蛋白/RNA代謝 ALS臨床型 関連 FTLD-FUS FUS:核輸送蛋白/RNA代謝 ALS臨床型 関連
MAPT:微小管関連蛋白 remove neurotoxic aggregates(tau/TDP-43) GRN:granulin;性分化誘導因子 cellular protein degradation machinery C9orf(open reading frame)72 cellular protein degradation machinery
Mann DMA & Snowden JS Brain Pathol 2017 改変
*ALS present:TDP-43 histologies familial ALS:C9orf72 expansions

21
ADE A連合野 D基底核 E辺縁系 脱抑制 陽性徴候 A 脱抑制行動 反社会(万引 ) 注意転導性(立 去 )D 保続 周徊 常同言語 返 E 多食 異食 偏食BCF B帯状回内側面 C底面 F穹窿部外側面 障害 陰性徴候 B self neglect 屋敷 C 同情 共感性欠如 KY 我 道 行 F 実行機能障害 作業

FTLD 陰性 陽性徴候 覚 前頭葉障害 陽性徴候 A後連合野 D基底核 E辺縁系 脱抑制 A 脱抑制行動 傍若無人) 反社会(万引 ) 注意転導性(立 去 )D 常同運動/姿勢 常同言語 周徊/時刻表行動 E 多食 異食 偏食 前頭葉障害 陰性徴候 B内側面前帯状回 C眼窩面 F背外側面 障害 陰性徴候 意:B self neglect 屋敷 情:C 同情 共感性欠如 情動調節障害 KY 知:F 実行機能障害 作業 側頭葉 皮質下障害 陰性徴候 運動/感覚失語 MND atypical parkinsonism PNFA進行性非流暢性失語/SD意味性認知症/ ALSD-TDP43/FUS, FALSDGuam Kii, PSP/CBD,FTLDP17前頭葉 前頭前野 解剖学的 背外側面 眼窩面 内側面 前帯状回 知 情 意 連合野 役割 各領域 後連合野 基底核 辺縁系 皮質下構造 間 異 神経回路 形成


治療的介入
FTD 上記 特徴的 精神症状 行動異常 対処 困難 疾患 考 行為自体 解体 無 本質的 記憶 保 検討 上 重要 常同行動 被影響性 亢進等 特徴的 症状 利用 可能 記憶 保 利用 担当 看護 OT 決 一貫 同 患者 受 持 場 決 立 去 行動 考 不精 目立 例 関係 十分可能 立 去 行動 激 例 作業療法導入時 予 取 掛 作業 道具 材料 机 上 準 備 立 去 速 道具 手渡 被影響性 亢進 利用 作業 導入 継続 重要 編 物 本人 趣味 一日 日課 組 入 被影響性 亢進 常同行動 固執傾向 患者 行為 没頭 化療法 .

# A novel mutation at position +11 in the intron following exon 10 of the tau gene in FTDP-17.Kowalska A, Hasegawa M, Miyamoto K, Akiguchi I, Ikemoto A, Takahashi K, Araki W, Tabira T.J Appl Genet. 2002;43:535-43.# Familial frontotemporal dementia and parkinsonism with a novel mutation at an intron 10+11-splice site in the tau gene.Miyamoto K, Kowalska A, Hasegawa M, Tabira T, Takahashi K, Araki W, Akiguchi I, Ikemoto A.Ann Neurol. 2001;50:117-20.# A case of frontotemporal dementia and parkinsonism of early onset with psp-like features.Miyamoto K, Ikemoto A, Akiguchi I, Kohno R, Imura T, Fujita Y.Clin Neuropathol. 2001;20:8-12. # Neuropathology of ALS with extra-motor system degeneration: characteristics in the molecular pathology between ALS with dementia and Guamanian ALS. Ikemoto A, Hirano A, Akiguchi I. ALS Other Motor Neuron Disord. 2000;1:97-104.# Comparative study of ubiquitin immunoreactivity of hippocampal granular cells in ALSwith dementia, Guamanian ALS and Guamanian parkinsonism-dementia complex.Ikemoto A, Hirano A, Akiguchi I, Kimura J. Acta Neuropathol. 1997;93:265-70. # Ubiquitin-related cytoskeletal abnormality in frontotemporal dementia: immunohistochemical and immunoelectron microscope studies.Kinoshita A, Tomimoto H, Suenaga T, Akiguchi I, Kimura J. Acta Neuropathol. 1997;94:67-72. # A case of primary progressive aphasia with ubiquitinated neurites in the cerebral cortex.Kinoshita A, Tomimoto H, Tachibana N, Suenaga T, Kawamata T, Kimura T, Akiguchi I, Kimura J.Acta Neuropathol. 1996;92:520-4.# Neurofibrillary tangles in the neurons of spinal dorsal root ganglia of patients with PSP.Nishimura M, Namba Y, Ikeda K, Akiguchi I, Oda M. Acta Neuropathol. 1993;85:453-7.





Brain Pathol. 2017 Jan 18 [Epub ahead of print]Frontotemporal lobar degeneration: Pathogenesis, pathology and pathways to phenotype.Mann DMA, Snowden JS.Frontotemporal Lobar Degeneration (FTLD) is a clinically, pathologically and genetically heterogeneous group of disorders that affect principally the frontal and temporal lobes of the brain. There are three major associated clinical syndromes, behavioral variant frontotemporal dementia (bvFTD), semantic dementia (SD) and progressive non-fluent aphasia (PNFA); three principal histologies, involving tau, TDP-43 and FUS proteins; and mutations in three major genes, MAPT, GRN and C9orf72, along with several other less common gene mutations. All three clinical syndromes can exist separately or in combination with Amyotrophic Lateral Sclerosis (ALS). SD is exclusively a TDP-43 proteinopathy, and PNFA may be so, with both showing tight clinical, histological and genetic inter-relationships. bvFTD is more of a challenge with overlapping histological and genetic features, involvement of any of the three aggregating proteins, and changes in any of the three major genes. However, when ALS is present, all cases show a clear histological phenotype with TDP-43 aggregated proteins, and familial forms are associated with expansions in C9orf72. TDP-43 and FUS are nuclear carrier proteins involved in the regulation of RNA metabolism, whereas tau protein - the product of MAPT - is responsible for the assembly/disassembly of microtubules, which are vital for intracellular transport. Mutations in TDP-43 and FUS genes are linked to clinical ALS rather than FTLD (with or without ALS), suggesting that clinical ALS may be a disorder of RNA metabolism. Conversely, the protein products of GRN and C9orf72, along with those of the other minor genes, appear to form part of the cellular protein degradation machinery. It is possible therefore that FTLD is a reflection of dysfunction within lysosomal/proteasomal systems resulting in failure to remove potentially neurotoxic (TDP-43 and tau) aggregates, which ultimately overwhelm capacity to function. Spread of aggregates along distinct pathways may account for the different clinical phenotypes, and patterns of progression of disease.