수두증의 평가를 위한 방사성동위원소 뇌조조영술 소견의 ... · 2016-12-26 ·...
11
1993 ; 29 (5) : Journal of Korean Radiological Society, September , 1993 : • • • • • • • - Abstract- Radioisotope Cisternographic Evaluation of Hydrocephalus: Comparison with CT, MRI, and Clinical Findings Soon Tae Kwon, M.D. , Cheong Hee Park, M.D. , Hyeong Yeol Ki m , M.D. , Dae Hong Ki m , M.D. , Kyung Suk Shin, M.D. , June Sik Cho, M.D. , Kang Wook Lee , M.D.*, Jae Moon Ki m , M.D.** 01 Radiology, College 01 Medicine, National University To evaluate the clinical usefulness of radionuclide(RI) cisternography in patients with hydrocephalus , we ret- rospectively analyzed RI cistemographic findings of 47 patients by using our classification which was modified from Baum’ s. and correlated them with CT(n=37) or MRI(n= 10) findings and clinical outcome in selected patients with hydrocephalus(n = 37). Modified RI cistemographic patterns of 37 patients were type 1 in three cases(8%) , type 11 in seven(18%) , type III- A in six(16%) , no case of type III-B, type IV- A in 12(32 %), and type IV- B in nine(24%). RI cisternography enabled to differentiate communicating hydrocephalus(27 cases , 73%) from noncommunicating hydrocephalus (10 cases , 27%). There was marked clinical improvement in 17 patients(46 %) , slight improvement in 11 patients(30%) , and no improvement in nine patients(24 %). clinical outcome of patients with RI cisternographic type IV- B was worse than that of other types. CT and MRI could neither predict the clinical outcome nor differentiate type IV-B from Type .05). Ventricular size index (VSI) was significantly higher in patients with type IV than that with other types(p < .001). RI cisternographic patterns of communicating hydrocephalus were relatively correlated with clinical outcome (r= 0.53 , p=.OOI) , VIS(r=0.59 , p= . OOI) , and dilatation offourth ventricle(r=0 .41 , p<.05) We suggest that our modified classification of RI cisternographic patterns can provide more strict physiological assessment of the CSF dynarnics and RI cisternography may be still useful to differentiate communicating hydrocephalus from noncommunicating hydrocephalus and to predict the clinical outcome in conjunction with CT/ MR findings and clinical presentation. Index Words: Hydrocephalus Brain, CT Brain, MR studies Brain , radionuclide studies * * 01 Internal Medicine, National University College 01 ** ** 01 National College 01 - 885-
Transcript of 수두증의 평가를 위한 방사성동위원소 뇌조조영술 소견의 ... · 2016-12-26 ·...

대 한 방 사 선 의 학 회 지 1993 ; 29 (5) : 885~895
Journal of Korean Radiological Society, September, 1993
수두증의 평가를 위한 방사성동위원소 뇌조조영술 소견의
유형적 분류 : 전산화단층촬영, 자기공명영상 및 임상 소견과의 비교
충남대학교 의과대학 진단방사선과학교실
권순태 • 박청희 • 김형열 • 김대흥 • 신경숙 • 조준식 • 이강욱* • 김재문**
- Abstract-
Radioisotope Cisternographic Evaluation of Hydrocephalus: Comparison with CT, MRI, and Clinical Findings
Soon Tae Kwon, M.D., Cheong Hee Park, M.D., Hyeong Yeol Kim, M.D., Dae Hong Kim , M.D. , Kyung Suk Shin, M.D. , June Sik Cho, M.D.,
Kang Wook Lee, M.D.*, Jae Moon Kim , M.D.**
Departητeηt 01 Radiology, College 01 Medicine, Chμngnam National University
To evaluate the clinical usefulness of radionuclide(RI) cisternography in patients with hydrocephalus, we ret
rospectively analyzed RI cistemographic findings of 47 patients by using our classification which was modified
from Baum’s. and correlated them with CT(n=37) or MRI(n= 10) findings and clinical outcome in selected
patients with hydrocephalus(n = 37). Modified RI cistemographic patterns of 37 patients were type 1 in three
cases(8%), type 11 in seven(18%) , type III- A in six(16%) , no case of type III- B, type IV- A in 12(32%), and
type IV- B in nine(24%). RI cisternography enabled to differentiate communicating hydrocephalus(27 cases , 73%) from noncommunicating hydrocephalus (10 cases , 27%). There was marked clinical improvement in 17
patients(46%) , slight improvement in 11 patients(30%) , and no improvement in nine patients(24%). Th~ clinical
outcome of patients with RI cisternographic type IV- B was worse than that of other types. CT and MRI could
neither predict the clinical outcome nor differentiate type IV- B from Type IV一A(p> .05). Ventricular size
index (VSI) was significantly higher in patients with type IV than that with other types(p < .001). RI
cisternographic patterns of communicating hydrocephalus were relatively correlated with clinical outcome (r=
0.53 , p=.OOI) , VIS(r=0.59 , p= .OOI) , and dilatation offourth ventricle(r=0 .41 , p<.05)
We suggest that our modified classification of RI cisternographic patterns can provide more strict
physiological assessment of the CSF dynarnics and RI cisternography may be still useful to differentiate
communicating hydrocephalus from noncommunicating hydrocephalus and to predict the clinical outcome in
conjunction with CT/ MR findings and clinical presentation.
Index Words: Hydrocephalus
Brain, CT
Brain, MR studies
Brain, radionuclide studies
* 충남대학교 의과대학 내과학교실 * Deparfmeηt 01 Internal Medicine, Chμngnam National University College 01 Mediciηe
** 충남대학교 의과대학 신경과학교실
** Departmeηt 01 Neμrology, Chμηgηam National U:ηiversity College 01 Mediciηe
이 논문은 1993년 6월 18일 접수하여 1993년 7월 22일에 채택되었음.
- 885-

대한방사선의학회지 1993 ; 29 (5) : 885~895
서 론
방사성동위원소 뇌조조영술(이하 뇌조조영술) 은 1964
년 Di Chiro등(1) 에 의해 뇌척수액 유동의 양상과 뇌척
수 공간의 구조를 조영하는 유용한 검사방법으로 보고
된 이래 수두증의 예후 평가 및 치료방법의 선택에 있어
임상적인 유용성이 알려져 왔다(2-5) . 근래에는 해부학적
영상이 우월한 전산화단층촬영 (이하 CT) 및 자기공명영
상(이하 MRI)이 개발되면서 뇌조조영술은 임상적 이
용이 감소되고 있다(에 .
통상적 뇌조조영상의 분류인 Type IV는 지속적인 뇌
실역류와 함께 방사능 이동이 지연된 경우로 단락수술의
지표로 삼고 있지만 (6-7) , 이러한 분류만으로는 수두증에
서 단락수술후 입상적 증상이 호전되지 않은 예 (30
50%) 도 많이 보고되 고 있어 (6, 8, -10) 단락 수술후 예 후
를 예견하는데 어려움이 있다. 또한 국내에는 뇌조조영
상의 유형 적 분류와 검 토에 대 한 보고 (6, 11) 는 있으나
CT및 MRI소견과 비교한 보고가 없다.
이 에 저자들은 방사성동위원소를 이용한 뇌조조영상의
형태적 분류와 전산화단층촬영 및 자기공명영상 그리고
입상적 결과와의 상관관계를 비교분석하여 수두증의 예후
판정과 치료의 방침을 결정하는데 있어서 뇌조조영술의
임상적 유용성을 알아보기 위하여 본 연구를 시행하였다.
대상 및 방법
1986년 3월부터 1993년 4월까지 보행장애, 요실금, 치
매외에, 안구 운동장애, 뇌압증가에의한 증상등의 임상적
소 견 과 CT/ MRI 소 견 상 심 한 뇌 위 축 없 이 뇌 실 지 수
(ventricular size index, 이 하 VSI) 30 이 상의 뇌 실 확
장소견을 보여 수두증이 의심되는 각종 뇌질환 환자중 뇌
조조영술을 시행받은 37명을 대상으로 하였고, 남자가
25명 여자가 12명 (M/F=2. 1 : 1)이었으며 평균연령은 54
세 (8개월-81세) 였다. 이중 35명은 약물치료등 보전적
치료만을 받았고 2명은 수술적 치료를 받았다. 수두증의
원인질환으로, 뇌혈관 질환이 8예 , 특발성의 정상압 수두
증이 7예, 그리고 뇌막염이 5예로 전체의 54%를 차지하
였고 그외의 원인으로는 Table 2와 같이 다양하였다.
뇌조조영술은 요추천자 후 지주막하강에 Tc- 99m
HSA (human serum albumin, 1 992년까지)l-3mCi 또
는 Tc-99m DTP A (diethylenetriaminepentaacetic
acid, 1 992년 이 후) 5mCi를 주입 후 1, 6, 24시 간후 감마
카메라(pho/Gamma ZLC 75, Siemens) 로 통상적인 방
법으로 전후면과 양 측면 영상을 얻었으며 필요에 따라서
는 48시간의 지연영상을 얻었다. 뇌조조영상의 분류는
24시간에 얻은 상을 기준으로 방사화합물의 뇌실역류 유
무 및 지속 시간, 뇌궁륭부로의 이동에 따랴 T ype 1 ,
II, 및 1II는 Baum등의분류 ( 7, 6) 를따랐으며, Type IV의 경
우 저자들은 지속적인 뇌실역류와 함께 주사후 24시간
까지 대뇌구륭부에 지연된 이동을 보이는 경우를 Type
IV-A(Fig. 1)로, 24시간이 경과하여도 대뇌궁륭부로의
이동이 거의 없는 경우는 T ype IV-B (Fig. 2) 로 세분하
여 분류하였다(Table 1).
대상환자 37명은 뇌조조영술 시행과 비슷한 시기 ( 1
일 - 3주)에 37명에서 CT (GE-8800)를 10명에서는 MRI
(0.5T Toshiba, TR/ TE : 500/ 20 , 2000/80) 영 상 을 함
께 얻었고 측뇌실의 확장정도, 제 3 그러고 제 4 뇌실의 확
장유무, 뇌피질의 위축정도, 그리고 CT 또는 MRI에서
각각 뇌실주위 저밀도 음영 또는 T 2 강조영상에서 뇌실
주위의 고신호강도의 유무를 관찰 측정하였다 (9 - 10,
12-17). 측뇌실의 확장정도는 전두각비율 ( ventricular
s ize index : maximum wid th of b ifron t a l h orn
diameter/ bifrontal diameter at the same leveJ) 로 써
mild (30- 39%) , moderate (40 - 46%) , severe(above
47%) 로 구분하였고(18) , 뇌피질의 위축정도는 없는경우
(none) , 약간(mild) , 중등도 (moderate) 이상으로 위축정
도를 정하였다(10, 14).
임상적 결과의 평가는 평균 107B 월 (4-35개 월) 이상
추적검사에서 보행장애, 요실금, 그리고 치매등 소위 만
Table 1. Classification of RI Cisternographic Patterns
Type 1 : No ventrÎcular activity, normal
nugratlOn.
Type 11 : No ventricular activity, delayed
nugratlOn
Type III- A: Transient ventricular activity, clearance by usual rnigation
Type III-B: Transient ventricular activity, clearance without usual rnigration
Type IV-A: Persistent ventricular activity with
parasagittal rnigration at 24 hours. Type IV- B: Persistent ventricular activity
without parasagittal rnigration at 24 hrs.
Modified from Baum et. al. 1981
- 886

권순태 외 : 수두증의 평가를 위한 방사성동위원소 뇌조조영술 소견의 유형적 분류
a b c
.,..’
「
‘책 d e f g
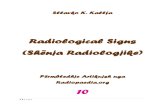
Fig. 1. 56 year-old male patient with suspicious NPH. CT scans(a-c) show moderately dilated frontal horn (VSI , 46) of the lateral ventricle , third ventricle , but fourth ventricle is not definitely dilated. There is periventricular lucency without cerebral cortical atrophy(c) . d- f. Type IV-A cisternograms. Anterior(d,f) and left lateral(e ,g) images obtained at 6 (d,e) and 24 hours(f,g) demonstrate ventricular reflux with stasis through 24 hours and flow over the parasagittal convexity.
성 수두증의 임상적 호전 정도를 주된 평가 기준으로 삼 및 MRI 소견과 뇌조조영술의 유형, 그리고 뇌조조영술
아 보행장애와 요실금의 증상이 현저하게 호전된 경우를 의 유형과 임상적 결과를 서로 비교 분석하였다. 주어진
‘현저한 호전 (Marked Împrovement) ’, 보행장애와 요실 자료의 분석과 통계적 검정 방법으로는 유의성 검정을 위
금이 약간 호전 이 있는 경 우를 ‘약간 호전 (Slight 한 x2-test와 상관관계 분석을 하였다.
improvement) ’, 그리고 임상증상의 호전이 전혀 없거나
악화된 경우를 ‘호전 없음 (N 0 Împrovement) ’으로 분류
하였고(14, 19) 이외에 발병당시 동반된 신경학적 증상의
호전 유무와 정도로써 평가하였다.
이상의 치료로 CT 및 MRI 소견과 입상적 결과, CT
?킥 E긍
대상환자중 뇌조조영 소견상 T ype 1 의 소견을 보인
- 887-

대한방사선의학회지 1993 ; 29 (5) : 885~895
a b
d e f
c
g
t
r ‘
‘ " ;..:p
~ r-
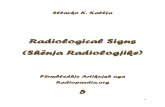
Fig. 2. 49 year-old male patient with Parkinsonism and suspicious NPH. CT scans(a, b) show moderately dilated lateral ventricle (VSI , 43) , third and fourth ventricles. There is periventricular lucency and mild cerebral cortical atrophy(c) . Type IV- B cisternograms. Anterior (d , f) and left lateral (e , g) images obtained at 6 (d , e) and 24 hours (f, g) demonstrate ventricular re f1ux with stasis , which continues until 48 hours and nearly no f10w over the parasagittal convexity.
환자는 3병 (8%), Type II 가 7명 (18%), Type III -A가
6명 (16%) , T ype III • B 가 0명, Type IV -A 가 1 2명
(32%), 그리 고 Type IV-B는 9명 (24%) 였으며 교통성
및 비 교통성 수두증 환자가 각각 27명 (73%) 및 10명
(27%) 이었다. 전후면 영상에서 비대칭적 뇌조조영상을
보인 5예중 두부외상이 4예 였으며 1예는 뇌낭미충증이
었다. 뇌벙변부위와 동측 뇌궁륭부로 방사화합물의 이동
이 지연된 2예 중 1예·는 CT상 동측에 뇌좌상의 소견을
보였고 1예는 동측에 Sylvian 조를 따라 뇌막 감염형 의
낭미충이 보였다 (Fig.4) 나머지 3예에서는 병변 반대측
대뇌반구의 방사화합물질 이동이 지연되었고 모두 복잡
함몰 두개골 골절이었다.
수두증환자 37병 중 17명 (46%) 은 경과중 임상증상이
상당히 호전되었고, 11명 (30%) 은 약간 호전되었으며 9
명 (24%)은 전혀 호전이 없었다 (Table 3,4) 임상증상의
호전이 없었던 9예는 평균 연령이 56세 였고 VSI는 평균
42로 측뇌실이 중등도의 확장소견을 보였고, 9예의 뇌조
조 영 상 Type 은 IV - B 가 7예, II 1예, IV- A 1예 였 다
(Table 5) 현저한 임상증상의 호전을 보인 17명의 경우
평균 연령은 46세 였고, VSI는 평균 37로 약간의 측뇌실
888 -

권순태 오1: 수두증의 평가를 위한 방사성동위원소 뇌조조영술 소견의 유형적 분류
Table 2. The Causes of Hydrocephalus and the Patterns of RI Cisternography
Total
C.V.A
Idiopathic NPH
Meningitis
Trauma
Cerebral atrophy
Sequelae of CO Poisoning
Neurocysticercosis
Aqueduct stenosis
Huntington’s disease
Alzheimer’s disease
Shy- Drager Synd.
Binswanger’s disease
Unknown*
8
[/
-n 9i
9-9-9-
1li
--4 1li
--4 1li
IV-B
。4
。3
n4
1i
IV- A
2
4
1
1
1
1
III-B III- A
2
1
1
1
II
2
1
Type Disease
4 1
37 9 12 0 6 7 3 Total
Table 3. Correlation between Cisternographic Patterns and CTjMRI , CTj MRI and Clinical Outcome in Patients with Hydrocephalus.(N = 37)
치 No definite symptoms and si망1S of normal pressure hydrocephalus.
Outcome +
Clinical ++
CT j MRI Findings Patterns N - A N-B
Ciπsternographic 1I m- A m- B
RI
%
삐 낌
(
(
1 ‘‘
9-ζJ
c‘
co
。3
nζ
m 페 이
…… %
이
Lateral ventricle(VSI)
Mild enlarged(n = 20)
Moderate(n= 13)
severe(n = 4) #
1i
h/
1i
4
6
2
co
nU
nU
7 2
o F
O
O
3rd. ventricle
not enlarged(n = 5)
enlarged(n = 32)
1 (11)
8 (89)
1 3(18)
14(82)
1 0
12
1 2
5 2 10
4th. ventricle
not enlarged(n=22)
enlarged(n= 15)
8 5
3 (33)
6 (67)
ζU r3
3(77)
4(23)
3
6
FhJ
[/
4 hl
nu 3
0 2
。/·1i
nU
3 (33)
5 (56)
1 (11)
4
5
2
10(59)
6(35)
1 ( 6)
Cortical atrophy
Non(n=17)
Mild(n= 16)
Moderate(n = 4)
At
At
1A
ra h-o
-3
nu
--
1i
44
9i
PVLDj PVH
Absent(n = 12)
Present(n = 25)
2 (22)
7 (78)
3
8
7(41)
10(59)
1
8 2
10
4 3 2
2 4
9(%)
- 889-
11
VSI; Ventricular size index, maximum width of bifrontal horn diameterφifrontal diameter at the same level, mild (30- 39%), moderate(40-46%) , severe (above 47%). *; V-P shunt, #; Extraventricular drainage PVLD; Periventricular low density, PVH; periventric띠ar hyperintensity on T2WI. + + ; Marked improvement, +; slight improvement, - ; no improvemen t.
17(%) Total 37 9 12 0 6 7 3

대한방사선의학회지 1993 ; 29 (5) ’ 885~895
55 r=0.53 1"'0.001
X'
ב ‘ ב :: • ×× ‘ X X × ‘ .‘ •
50 ‘ . 45
40 •• • ‘ 35 g ‘ ‘
--‘ • 30
X. • VSI
Type II I II-A I lI - B I V-A IV-B
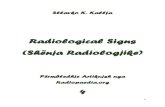
Fig. 3. Correlation between cisternographic patterns and clinical outcome, cisternographic patterns and VSI in patients with hydrocephalus(N = 37).RI cisternographic patterns of communicating hydrocephalus(Type III-A - > Type IV-A - > Type IV-B) are relatively correlated with VSI(r=0.59 , p= .OOl) and clinical outcome(r=-0.53 , p= .001). • Marked improvement, ‘ Slight improvement, X No improvement, *; V- P shunt , #; Extrav entricular drainage.
확장 소견을 보였으며 뇌조조영상의 Type은 다양하였고
T ype IV- B 1예 뿐이 었다.
CT 및 MRI 소 견 과 추 적 임 상 적 결 과 의 비 교 에 서
(Table 3) 통계적 유의성은 없었으나(p).05) 측뇌실의
확장이 경미할수록 그리고 대뇌피질의 위축이 없을수록
임상증상이 호전되는 경향을 보였다. 제 3, 4뇌실의 확장
유무와 뇌실주위 저밀도음영 또는 고신호강도 유무와 임
없었다 (p) .05) 수두증환자 37명 의 평 균 VSI는 39였고
뇌 조 조 영 상 Type, IV 의 소 견 을 보 였 던 21명 의 평 균
VSI는 42로 Type IV 이외의 소견을 보인 16명의 평균
VSI35보다 의 미 있게 높았다(p=.OO 1) , 그러 나 CT 및
MRI 소견으로는 T ype IV -A와 Type IV -B를 구별할
수 없었다(p) .0 5) .
뇌조조영상과 임상적 결과, 뇌조조영상과 CT 및 MRI
소견과의 비교에서 (Table 4, Fig. 3), 교통성 수두증의
뇌조조영상 유형과 임상증상 정도 (r= -0.53 , p= .001),
VSI(r = 0.59 , p= .001), 그리고 제 4뇌실의 확장소견 (r=
0.41, p<0.05) 과는 유의한 상관관계가 있었다.
수술을 시행한 2명의 환자중 Sylvius관의 협착이 의심
되 었던 8개월된 남아의 경우 뇌조조영상 T ype 1 및
VSI는 50이었고 뇌실 복막강 단락수술후 임상증상의 현
저한 호전을 보였다. 15년전 두부 총상으로 수두증과
뇌 실 감 염 이 있 었 던 34세 의 남 자 의 경 우 뇌 조 조 영 상
T ype IV- B 및 VSI는 50을 보였고 양측 뇌실에 뇌실외
배 액 술 (extraventricular drainage, EVD) 를 시 행 했 으
나 추적검사에서 임상증상의 호전은 없었다.
방사성동위원소 뇌조조영술의 부작용으로는 뇌조조영
술 시행후 5예 ( 10.4%) 에서 12시간내 체온이 1. 2-2. 5'C
까지 상승했으나 12시간 이내에 특별한 치료없이 좋아졌
고 이중 1 (2%) 예에서 뇌막자극 증상이 현저했던 무균성
뇌막염 소견을 보였으나 합병증없이 곧 소실되었다.
고 jξ} E므
상적 결과 사이에 통계적 유의성은 없었다(p) .05)
CT 및 MRI 소견과 뇌조조영 술의 소견의 비교에서 뇌척수액은 대부분 맥락막총 (80-90%) 에서 확산 및
(Table 3) 제 3, 4뇌실의 확장소견을 포항한 앞서 예시한 능동수송에의해 생성되며 소량의 뇌의 간질 상의세포와
CT 및 MRI 소견으로 뇌조조영상 교통성 수두증 소견을 연막의 모세혈관에서도 생성된다. 또한 생성된 뇌척수액
예견할 수 있었지만(특이도 100%, 양성예측도 100%), 은 지주막하강의 여러경로를 통하여 대부분 상시상정맥동
교통성 수두증 Type간에 감별은 통계적으로 유의성은 에 있는 지주막융모에서 흡수되며 그외 소량이 뇌, 척수,
Table 4. Correlation between RIC Pattems and Clinical Outcome, RIC Patterns and VSI in Patients with Hydrocephalus.(N= 37)
Clinical Outcome RI Cisternographic Patterns VSI R ill-A ill-B N- A N-B (Mean)
Marked improvement(n = 17) 2 4 4 0 6 1 37
Slight improvement(n = 11) 1 2 2 0 5 1 40
No improvement(n=9) 0 1 0 0 1 7 42
VSI(Mean, %) 42 35 34 41 43 39πotal)
RIC; Radioisotope cisternography, VSI; Ventricular size index, mild (30- 39%) , moderate(40-46%) , severe (above 47%)
- 890 -

권순태 오1 : 수두증의 평가를 위한 방사성동위원소 뇌조조영술 소견의 유형적 분류
;;::; ‘
a b c Fig. 4. 36 year-이d male patient with neurocysticercosis. CT scan(a) shows enlarged lateral ventricles (VSI, 44) and multiple aggregated cystic lesions with scolex within the cysts along right insular cistern. Another small cystic lesion can be seen on the left parietooccipital convexity. Type IV-A cisternograms with asymmetric ITÙgration. Anterior(a) and left lateral(b) images obtained at 24 hours demonstrate ventricular reflux with stasis and delayed or defected ITÙgration on ipsilateral to the lesion side and usual ITÙgration on the contralateral parasagittal convexity albeit inhomogeneous patchy ITÙgration.
A/S Disease
Table 5. Patients without Clinical Improvement(n = 9)
Ventricle VSI 3rd
50 + 40 + 31 + 43 + 48 + 45 + 41 + 40 + 38
42 (Mean)
1. 341M Pneumoventricle with infection
2. 371M Tuberculous meningitis
3. 391M Huntington’s disease
4 . 49/M Parkinsonism. r/ o NPH. CI
5. 66/ M NPH
6. 67/ M Multi- infarct dementia
7. 67/F Dementia
8. 67/M CI, Multiple lacunae
9 77/ M NPH.
56 (Mean)
4th
+ +
+ + +
+
Type
IV- B
IV-B
JI IV- B
IV- A
IV- B
IV- B
IV-B
IV-B
VSI; Ventricular size index CI; Cerebral infarct. +; Ventricular dilatation, - ; No ventricular dilatation. NPH; Idiopathic normal pressure hydrocephalus
신경근을 싸고 있는 연막과 뇌실계의 상의세포에서 흡수
된다(20, 21) . 뇌 척 수액 의 생성 및 흡수율은 분당 ι
35-0. 37ml이며 뇌척수공간은 뇌실이 25-35ml 그리고
지주막하강을 포함하여 성인이 평균 150ml이고 하루의
생성량이 약 500ml이므로 하루에 3번이상 교체된다고 알
려져 있다 (20) .
수두증이란 뇌척수강내 뇌척수액이 다양한 원인(18,
21)에 의해 상대적으로 증가한 상태로 정의하며 수두증의
가장 흔한 원인은 뇌척수액 이동경로의 폐쇄이며 폐쇄 부
위와 원인을 파악하는 것이 치료의 방침을 결정하는데 중
- 891 -

대한방사선의학회지 1993 ; 29 (5) : 885~895
요하다 (20 -22) . 저자들의 경우 수두증의 원인으로 뇌혈
관질환이 8예 (21%)로 가장 많았으며 특발성 정상압 수두
증이 7예(18%) , 뇌막염이 5예 ( 13%) 순으로 김, 박등 ( 11,
21) 의 결과와 비슷하였다.
정상압수두증이란 보행장애, 요실금, 치매의 임상적 삼
주징과 만성적 수두증, 그리고 정상 뇌압을 특정으로
1965년 Adams등 (23) 이 처음 기술하였다. James등 (22)
과 Alker등 (5) 도 정상압수두증은 단락수술로써 치료가능
한 치매로 CT소견상 뇌실질의 위축없이 뇌실의 확장소
견을 보이며, 뇌조조영술 소견상 방사성동위원소의 뇌실
로의 역류와 24시간 또는 48시간의 지연영상에서 대뇌
궁륭부로의 이동이 없거나 현저히 감소된 소견을 보인다
고 하였고 이러한 소견을 단락수술의 지표로 삼고있다.
그러나 실제 수술적 치료시 수술 자체의 심한 합병증도
35%이상 보고되고 있기 때문에 (9 - 10) CT / MRI 소견과
뇌조조영상뿐만 아니라 신경정신학적 평가, 뇌혈류 측정
(24-25) 등 다각적 평가가 요구되며 ( 14, 24) , 정확한 수술
의 적용기준을 정하여야 한다고 하였다 (8- 9). J acobs등
(19) 은 만성 수두증의 증상중 운동 기 능의 장애 가 제 일
중요하고 가장 특정적인 소견은 보행장애라고 하였다.
Petersen등 ( 14) 은 원인불명의 수두증의 연구에서 소위
정상압 수두증의 완전한 입상적 삼주징이 있는 환자에서
수술에 대한 반응이 좋았고 수술후에도 보행장애 (74%) ,
요실금 (65%)순으로 임상증상의 개선이 있었고 치매의 개
선 (57%) 이 제일 저조했다고 하였다. 저자들의 연구에사
도 수술을 하지 않은 환자에서 입상적 결과의 평가기준을
보행장애의 호전정도를 가장 중요한 지표로 삼아 호전 정
도를 분류하였고 그외의 동반된 신경학적 증상은 발병 당
시의 증상정도를 기준으로 하여 호전정도를 분류하였다.
뇌조조영술의 판독과 분류에 있어 방사성동위원소의 뇌
실역류의 지속기간과 대뇌궁륭부로의 지연된 이동을 24
시간을 기준으로 (7) 평가하는 경우 Type III -A와 Type
IV-A의 구분에는 문제가 없었으나 Type IV-A와 T ype IV
- B를 구분하는데에 있어 48시간의 지연영상을 위해 적당
한 계수율을 얻는데는 시간적으로나, 영상의 질에 있어서
전등 (6) 과 마찬가지로 판독하는데 어려움이 있었다. 저자
들의 경우 T ype III -B가 한예도 없었는데 McCullough
등 (3) 과 전등 (6) 의 보고에 의하면 T ype III-B 소견을 보
인 환자 모두가 두부외상 또는 두부수술을 받은 환자틀
이었고 이러한 소견의 기전으로는 뇌실 상피세포에 의한
대체흡수경로로 설명하였다 (3, 7) . 또한 이들 모두 수술을
받았으나 임상증상의 호전은 없었다.
비대칭성 뇌조조영상을 보인 5예중 4예 (80%)가 두부
외상 환자였는데 Salmon등(2 6) 도 두부외상을 받은 환자
들에서 빈번하게 비대칭적 공기 뇌조조영상이 보인다고
하였고 James등 (4) 도 두부외상시의 비대칭적 뇌조조영
상을 기술하고 있다. 저자들의 경우 병변과 반대측의 지
연 또는 결손된 영상은 병변측의 두개골절에 의한 감압,
반대측으로 뇌실질의 혈종 또는 부종의 압박에 의한 것으
로 추정되고 병변측의 지연 또는 결손된 영상은 두개골절
이 없는 두부외상인 경우 폐쇄공간에서 뇌진탕 또는 뇌좌
상으로 인한 뇌실질의 압박 또는 부종에 의한 것으로 추
측된다(4) . 또한 1예의 뇌낭미충증에의한 경우 동측의 지
주막 하강의 유착 또는 폐쇄와 관련이 있을 것으로 생각
된다.
임상적 결과를 평가 비교하는데에 있어 저자들의 경우
대부분이 수술을 받지 않은 환자가 대상이었는데 뇌조조
영상 T ype IV - B이면서 추적검사에서 임상적 호전이 없
었던 7예 (Table 5) 중 수술을 시행하지 않은 6예의 이유
로는 4예에서 일차적인 원인이 뇌혈관 질환과 결핵성 뇌
막염 이었고 정상압수두증을 보인 2명은 수술을 거부하였
다. Hughes등 (8) 은 수술을 하지 않았던 12명 의 특발성
교통성 수두증환자의 자연적 임상적 경과를 기술하고 있
는데 36개 월의 추적 검사시 6명 (50%) 에서 임상증세의
호전을 보였다고 하였다. Acetazolamide를 포함한 보전
적 치료의 효과에는 논란이 있지만(28) 본 연구의 경우
수두증의 다양한 원인에도 불구하고 보전적 치료로 평균
107~윌의 추적 검사에서 Type IV의 교통성 수두증 환자
21명중 13명 (61%) 에서 임상증상의 호전을 보였고 이중
Type IV -A가 11예 (84%), T ype IV-B는 2예 뿐이었다.
임상적 호전이 보전적 치료의 결과인지 혹은 교통성 수두
증의 자연경과인지에 관하여는 본 연구의 결과만으로는
판단할 수 없었다.
방사성동위원소 뇌조조영술은 근래에는 해부학적 영상
이 우월한 CT와 MRI의 이용으로 임상 응용의 범위가
많이 감소되고 있으며 (6, 12) 수두증의 평가에 있어서 뇌
조조영술의 유용성에 관하여 논란이 되고 있다 ( 9→ 10, 15,
26-27, 29-30).
CT 및 MRI 소견과 임상적 결과와의 비교에서 저자들
의 경우 임상적 결과를 예측할만한 특별한 소견을 발견할
수 없었다. Petersen등 (24)과 Enzmann등 (31)은 CT의
소견은 원인불명의 수두증의 진단과 추적검사에 중요하나
뇌실확장, 뇌실질의 위축 정도 또는 뇌실주위 저밀도음영
유무로는 단락수술후의 예후를 예측할 수 없었다고 했고
Jacobs 등 (1 5) 도 정상압 수두증의 임상적결과를 예견할
수 있는 특이할만한 MRI의 소견은 없다고 하였다. 그러
나 정상압수두증과의 감별진단으로 Alzheimer 병, 다경
색 치 매 (muliple- infarct dementia) , Binswanger 병 ,
- 892-

권순태 외 : 수두증의 평가를 위한 방사성동위원소 뇌조조영술 소견의 유형적 분류
그리고 Parkinsonism이 중요한데(8, 14, 19) 임상증상과
더불어 CT 및 MRI 소견이 도움이 되며 또한 단락수술
후의 합병증의 발견 및 추적 검사에 유용하다는 보고들이
있다(8, 14, 18). 뇌조조영술 T ype II환자 7명중 추적 임
상적 결과의 현저한 호전이 있었던 경우는 4영 (57%) 뿐
이 었 고 Sylvius관 의 협 착 이 의 심 되 었 던 뇌 조 조 영 상
Type 1 인 예에서도 추적 임상적 결과에 현저한 호전이
없어 원인질환의 심한정도에 따라 증상의 호전 정도와 치
료효과도 다르다고 생각되는데 이러한 경우 뇌조조영술만
으로 임상적 결과를 예측하기가 어렵고 CT/MRI와 임상
적 증상이 임상적 결과를 예측하는데 도움이 되 리라 생각
된다.
Gado등 (29) 은 뇌조조영술 소견중 방사성 동위원소의
뇌실내 역류는 교통성 수두증을 의미하며 교통성수두증의
CT 소견은 뇌구의 확장소견 없이 제& 제 4 뇌실을 포함
한 중등도 이상의 측뇌실 확장을 보인다고 하였는데, 저
자들의 경우에는 CT 및 MRI의 소견과 뇌조조영상의 유
형과의 비교에서 측뇌실의 VSI와 제 4뇌설의 확장소견만
이 뇌조조영상의 교통성 수두증을 예측할 수 있었다.
저자들의 경우 추적조사시 교통성 수두증 유형 (Type
III - A, IV- A, and IV-B)과 임 상증상 정 도 및 VSI와 유
의한 상관관계를 보였다 (Fig.3) 즉, 뇌조조영상 Type
III - A• Type IV-A• Type IV- B일수록 추적검사에서
임상적 증상의 호전율은 감소되었으며, 측뇌실과 제 4뇌
실이 확장되는 소견을 보였다. 이러한 결과는 T ype III
A의 소견이 교통성 수두증의 진행 또는 회복시에 보일
수 있다 (2 1) 는 것과 수두증환자의 뇌조조영상을 등급별로
파악한 Harwood- N ash의 분류에 따른 김 ( 11) 등의 임상
결과와도 유사하였다. 한편 저자들의 경우 추적 임상결과
가 비교적 단기간이었고 추적 뇌조조영술이 시행되지 않
아 교통성 수두증의 진행 과정에서의 T ype III -A인 경우
일률적으로 임상적 호전을 예측하기는 어렵다고 생각된
다.
방사성 동위원소 뇌조조영술의 부작용은 저자들의 경우
단순발열에서 무균성뇌막염의 경한증상에 그쳤으며 Tc
- 99m HSA 을 사 용 한 경 우 에 만 발 생 되 었 고 Tc- 99m
DTPA를 사용한 예에서는 없었다. 그러나 1975년 Coo
per등 ( 32) 에 의해 Limulus 검사로 HSA이 내독소로서
무균성 뇌막염의 가능성을 시사하고 그 빈도를 조사한바
에 의하면 14%까지 보고되었으며 또한 In- 111 DTPA
의 경우에도 무균성 뇌막염이 1. 5%에서 6%까지 보고되
고 있어 알부민만에 의한 부작용은 아닌것이라 주장했다.
또한 동물실험에서 내독소 (Endotoxin) 는 정맥주사보다
뇌척수액에서 1000배나 더 강하다고 하였고 뇌조조영술
에서의 부작용은 이에 의한 오염으로 추정하였다.
최 근 에 는 SPECT(single photon emission comput
ed tomography) 를 이용해 여러부위에서 뇌척수액의 방
사능 활동도를 연속적으로 측정하고 방사능 감쇄곡선을
얻 어 통 계 분 석 처 리 하 는 연 구 (33)와 MRI 에 서 소 위
CFVS(CSF flow void signal)로 비교통성 및 교통성수
두증을 비 롯한 뇌척수액의 동적연구가 시 도되고 있다
(34-36) . 또한 cine MRI 및 fluoroscopic MRI의 임상
이용으로 보다 정확한 뇌척수액의 역동과 양적인 평가에
대한 연구들이 진행되고 있다(37-38) .
저자들에 의한 방사성동위원소 뇌조조영술의 유형적 분
류는 대상환자의 숫자가 적어 단정적으로 결론 내리기는
어려우나 뇌조조영술상 Type IV를 Type IV-A와 Type
IV→B로 구별을 함으로써 임상적 결과를 더 정확히 예측
할 수 있었으며, 정상압수두증을 비롯한 교통성 수두증의
경우 CT 및 MRI 소견이 질병자체의 감별진단에는 도움
이 되나 임상적인 예후 판정과 치료방침의 결정에는 CT
및 MRI 소견보다는 뇌조조영술이 더 도움을 줄 것으로
사료된다. 결론적으로 방사성동위원소 뇌조조영술은 CT
및 MRI 그리고 임상증상의 소견과 더불어 수두증의 예
후판정과 치료의 방침을 결정하는데 유용하게 이용될 수
있을 것으로 생각된다.
참고문헌
1. Di Chiro G, Reames PM, Matthews WB. RISA
ventriculograhy and RISA-cisternography. Neu
rology 1964; 14:185- 191
2. Glasuer FE, Alker GJ, Leslie EV. Isotope
cisternography and ventriculography: evaluation
of hydrocephalus in children. Am J Dis Child.
1970; 120:109-114
3. McCullough DC, Harbert JC , Di Chiro G,
Ommaya AK. Prognostic criteria for cerebrospi
nal fluid shunting from isotope cisternography
in communicating hydrocephalus. Neurology
1970; 20 :594-598
4. James AE , New PFJ , Heinz ER, Hodges FJ ,
DeLand FH. A cisternographic classification of
hydrocephalus . AJR 1972; 115:39- 49
5. Alker GJ, Glasauer FE, Leslie EV. Long-term
experience with isotope cisternography. JAMA
1972; 219 :1005-1010
6 전범석, 명호진, 김상은, 정준기, 고창순. 방사성동위
- 893-

대한방사선의학회지 1993 ; 29 (5) : 885~895
원소 조조영술 소견의 유형적 분류 및 교통성수두증에
서 유형에 따른 단락수술의 치료효과의 차이. 대한신경
과학회지 1987 : 5 : 24- 29
7. Baum S, Vincent NR, Lyons KP , Wu S, Gurkin
SC. Radionuclide cisternography. In: Baum S, Vincent NR, lyons KP, Wu S, Gurkin SC(eds)
Atlas of nucler medicine imaging. New York, Appleton-Centmγ→}rofts. 1981; 171- 289
8. Hughes CP , Siegel BA, Coxe WS et al. Adult idi
opathic communicating hydrocephalus with and
without shunting. ] Neurol Neurosurg Psychiatr
1978; 41 :961 - 971
9. Vanneste ], Acker RV. Normal pressure
hydrocephalus: did publications alter manage
ment ? ] Neurol Neurosurg Psychiatr 1990; 53:
564-568
10. Benzel EC, Pelletier AL, Levy PG. Communicat
ing hydrocephalus in adults: Prediction of out
come after ventricular shunting procedures.
Neurosurgery 1990; 26:655-660
1 l. 김용수, 박창윤, 정 태섭 등. 방사성동위원소를 이용한
뇌조조영술의 진단적 의의. 대 한방사선의 학회 지
1989: 25(6) : 35-842
12. Huckman MS. Normal pressure hydrocephalus:
evaluation of diagnostic and prognostic tests.
A]NR 1981; 2:385- 395
13. Harbert ]C, McCullough DC, Schellinger D.
Computed cranial tomography and radionuclide
cistemography in hydrocephalus. SellÙn Nucl
Med 1977; 7:197- 200
14. Petersen RC , Mokri B, Laws ER, ]r. Surgical
treatment of idiopathic hydroceph띠us in elderly
patients. Neurology 1985; 35:307-311
15. ]acobs M, Mantil J , Peiglin D, Andrews J. Radionuclide cisternography and MRI in the
evaluation of normal pressure hydrocephalus. ]
Nucl Med 1988; 29:836- 837
16. Tamaki N , Shirakuni T , Ehara K, Matsumoto S.
Characterization of periventricular edema in
normal pressure hydrocephalus by measurement
of water proton relaxation times. J Neurosurg
1990; 73:864-870
17. Jack CR, Morki B, Laws ER, Houser OW, Baker
HL, Petersen RC. MR findir황 in normal- pres
sure hydrocephalus: significance and comparison
with other froms of dementia. J Comput Assist
Tomogr 1987; 11 :923- 931
18. Rao K C.V.G. The CSF space. In: Lee SH, Rao
K C.V.G., Zimmerman RA. Cranial MRI and
CT. 3rd ed. McGraw- Hill, Inc. 1992; 227- 294
19. ]acobs L, Conti D, Kinkel WR, Manning EJ. Norma1-pressure " hydrocepha1us relationship of
clinica1 and radiographic findings to improve
ment following shunt surgery. JAMA 1976; 235:
510-512
20. McComb JG. Recent research into the nature of
cerebrospina1 f1uid formation and absorption. J
Neurosurg 1983; 59:369- 383
21 박석건, 이명철. 방사성동위원소 조조영술. 고창순 편
저. 핵의학, 초간, 고려의학. 1992 : 191- 201
22. James AE , DeLand FH , Hodges FJ , Henry NW
Norma1 pressure hydrocepha1us: role of
cisternography in diagnosis. JAMA 1970; 213:
1615- 1622
23. Adams RD , Fisher CM , Hakim S, Ojemann RG,
Sweet WH. Symptomatic occult hydrocepha1us
with "Normal " cerebrospin외 f1uid pressure.
New EngJ Med 1965; 273(3):117- 126
24. Graff-Radford NR, Rezai K, Codersky JC,
Es1inger P, Damasio H , Kirchner RT. Regional
cerebra1 blood f10w in norma1 pressure
hydrocepha1us. J Neurol Neurosurg Psychiatr
1987; 50:1589- 1596
25. Kushner M, Younkin D, Weinberger J , Hurtig
H , Gldberg H , Reivich M. Cerebral hemody
nallÙcs in the diagnosis of normal pressure
hydrocepha1us. Neurology 1984; 34:96- 99
26. Sa1mon JH. Adult hydrocephalus: evaluation of
shunt theraphy in 80 patients. J. Neurosurg
1972; 37:425-42827. Larson A, Moonen M, Bergh AC, lindberg S. Predictive va1ue of quan
titative cisternography in the norma1 pressure
hydrocepha1us. Acta Neurol Scand 1990; 81:
327- 332
28. Shinner S, Gammon K, Bergman EW, et a1.
Management of hydrocepha1us in infancy: Use
of acetazolanùde and furose llÙde to avoid cere
brospinal f1uid shunt. J pediatr 1985; 107:31- 37
29. Gado MH , Coleman RE, Lee KS , Mikhael MA,
Alderson PO, Archer CR. Correlation between
computerized transaxial tomography and
radionuclide cisternography in dementia. Neu-
- 894-

권순태 외 : 수두증의 평가를 위한 방사성동위원소 뇌조조영술 소견의 유형적 분류
rology 1976; 555-560
30. Vanneste ], Au맑st낀 P, Davies GAG, Dirven
Clemens, Tan WF. Normal-pressure
hydrocephalus: is cisternography still useful in
selecting patients for shunt? Arch Neurol 1992;
49:366- 370
31. Enzmann DR, Norman David, Price DC, Newton
TH. Metrizamide and radionuclide
cisternography in communicating hydrocephalus.
Radiology 1979; 130:681 - 686
32 . Cooper ]F, Harbert ]C. Endotoxin as a cause of
aseptic meningitis after radionuclide
cisternography. ] Nucl Med 1973; 16:809-813
33. Kuchiwaki H , Nagasaka M, Takada S, Ishiguri
H , Kamey킹na H , Aoyama Y. Clinical study of
radioisotope clearance from the cerebrospinal
fluid space using single photon emission com
puted tomography. Neuroradiology 1989; 31 :
226-231
34. ]olesz FA, Patz S, Hawkes RC, et al . Fast imag-
ing of CSF flow j motion pattern using steady
state free precession. Invest Radiol 1987; 22 :
761 - 777
35. Feinverg DA, Mark AS. Human brain motion
and cerebrospin떠 fluid circulation demonstrated
with MR velocity imaging. Radiology 1987; 163:
793-799
36. Enzman DR, Norbert ]P. Normal flow patterns
of intracranial and spinal fluid defined with
phase-contrast cine MR imaging. Radiology
1991; 178 :467- 474
37. Bradley WG, Kortman KE, Burgoyne B, Eng D.
Flowing cerebrospinal fluid in normal and
hydrocephalic states: appearance on MR images.
Radiology 1986; 1q59:611- 616
38. Enzmann DR, Pelc NJ. Normal flow patterns of
intracranial and spinal CSF defined with phase
contrast cine MR imaging. Radiology 1991; 178:
467- 464
- 895 -