Drugs used in pulmonary diseases Antiasthmatic drugs Antitussives Expectorants Yang yun-xia (...
44
Drugs used in pulmonary diseases Antiasthmatic drug s Antitussives Expectorants Yang yun-xia ( 杨杨杨)
-
Upload
gary-casey -
Category
Documents
-
view
253 -
download
4
Transcript of Drugs used in pulmonary diseases Antiasthmatic drugs Antitussives Expectorants Yang yun-xia (...
Drugs used in pulmonary diseases
Antiasthmatic drugs
Antitussives
Expectorants
Yang yun-xia ( 杨云霞)

Drugs used in pulmonary diseases
Coughing
Wheezing Sputum (phlegm)
Inflammation
Drugs used in pulmonary diseases
Coughing
Wheezing Sputum (phlegm)
Inflammation
Coughing
Wheezing Sputum (phlegm)
Inflammation

Pulmonary Pharmacology: Asthma
General disease characteristics:
increased tracheobronchial responsiveness to many stimuli
↓ physiological air passage narrowing ↓ paroxysmal dyspnea, coughing, wheezing,
chest tightness
Prevalence:
Very common disorder: 4-5% affected
Typically presents in early life:
50% of cases developed before age 10;
33% before age 40

Etiology-----two broad types
①Allergic asthma: (IgE)
• Ag-Ab → mast cell surface• → mediators release • → muscle contraction• vascular leakage• mucus hyper secretion•
Histamine
Trapase
Leukotrienes
Prostaglandins
PAF
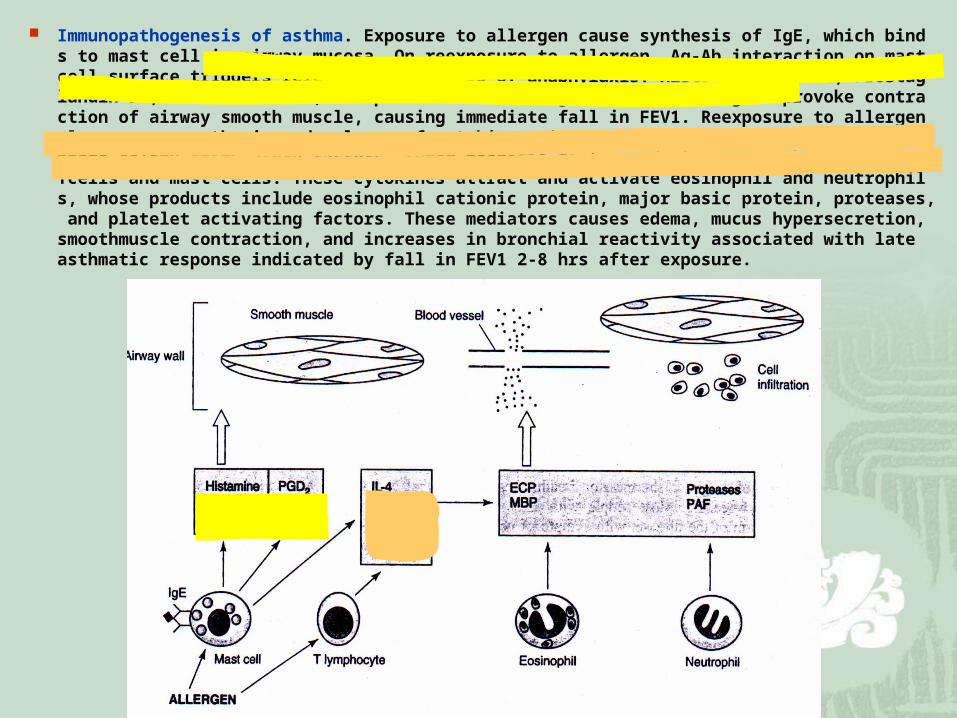
Immunopathogenesis of asthma. Exposure to allergen cause synthesis of IgE, which binds to mast cell in airway mucosa. On reexposure to allergen, Ag-Ab interaction on mast cell surface triggers release of mediators of anaphylaxis: Histamine,trypase, Prostaglandin D2, leukotriene C4, and platelet-activating factor. These agent provoke contraction of airway smooth muscle, causing immediate fall in FEV1. Reexposure to allergen also causes synthesis and release of cytokines: interleukins 4 & 5, granulocyte-macrophage colony stimulatory factors, tumor necrosis factor and tissue growth factor from Tcells and mast cells. These cytokines attract and activate eosinophil and neutrophils, whose products include eosinophil cationic protein, major basic protein, proteases, and platelet activating factors. These mediators causes edema, mucus hypersecretion, smoothmuscle contraction, and increases in bronchial reactivity associated with late asthmatic response indicated by fall in FEV1 2-8 hrs after exposure.
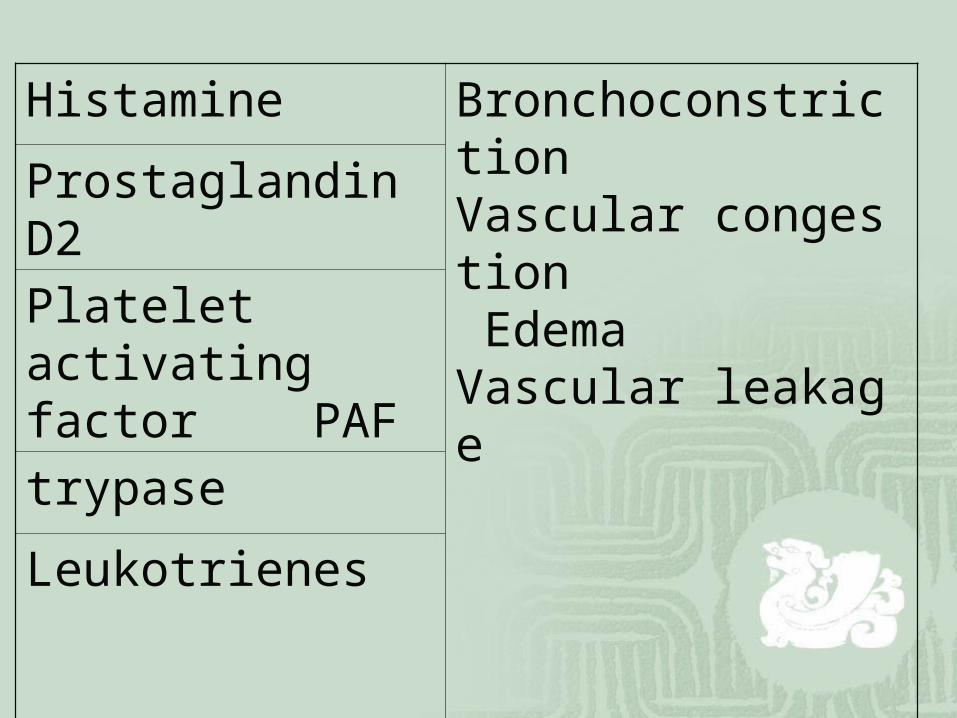
Histamine Bronchoconstriction Vascular congestion Edema Vascular leakage
Prostaglandin D2
Platelet activating factor PAF
trypase
Leukotrienes
②Idiosyncratic asthma: normal serum IgE Nonantigenic stimuli
Stimulation-induced exercises, inhaled irritants ect
Etiology

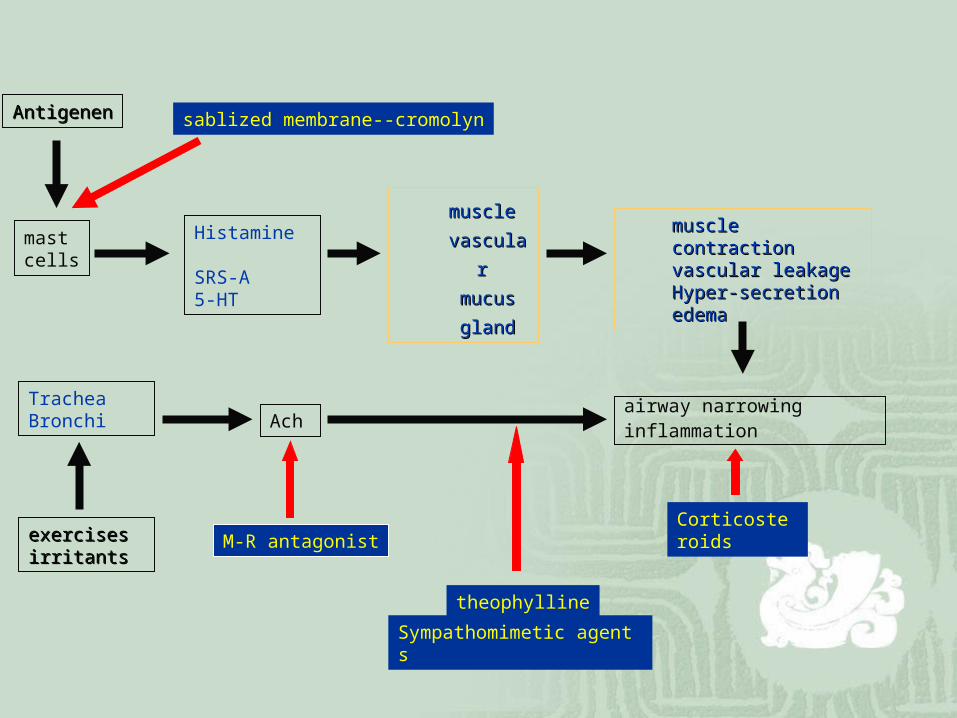
mast cells
Histamine SRS-A5-HT
Trachea Bronchi
muscle muscle
vascular vascular
mucusmucus
glandgland
muscle contractionmuscle contractionvascular leakagevascular leakageHyper-secretionHyper-secretionedemaedema
airway narrowinginflammation
exercisesexercisesirritantsirritants
AntigenenAntigenen
Ach
M-R antagonist
Sympathomimetic agents
Corticosteroids
theophylline
sablized membrane--cromolyn
Short-term pharmacological relief
bronchodilators (promote airway smooth muscle relaxation increased airway caliber )
ß—adrenoceptor agonistsTheophyllineAntimuscarinic drugs

Long-term(Antiinflammatory) pharmacological management:
Inhaled corticosteroids Leukotriene pathway inhibitors Inhibitors of mast cell degranulation (e.g.,
cromolyn 色甘酸 )
sympathomimetic drugs
β2-R→→smooth muscle→
→ cAMP↑ →→dilation β2-R →→ mast cells→
→mediators release ↓ α -R→ →microvascular constricting →→ edema↓
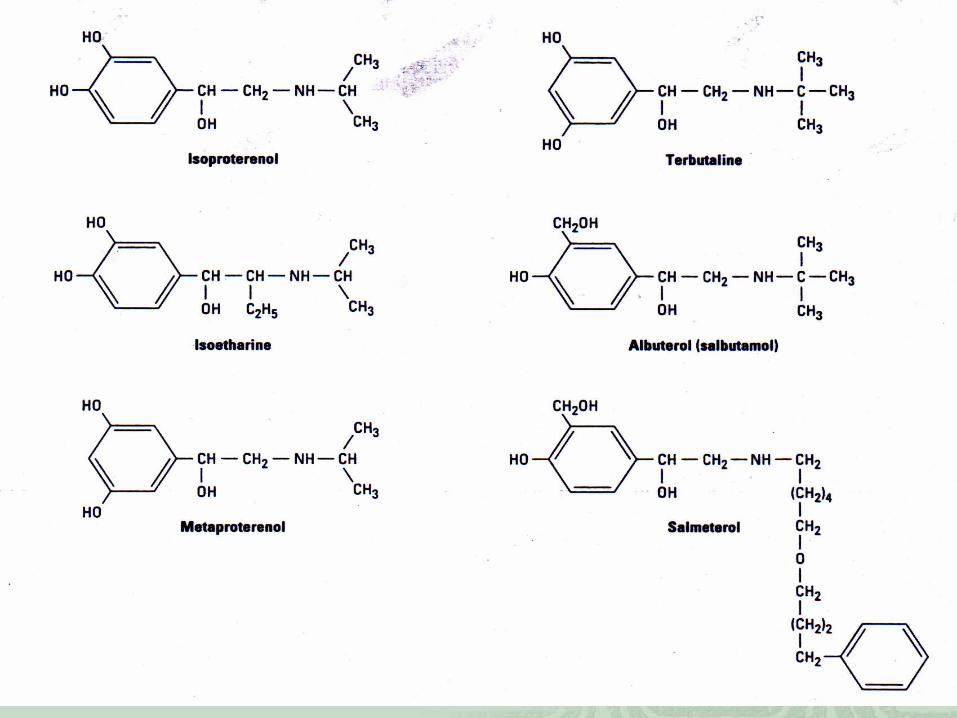
sympathomimetic drugsdrug Rece
p-toraction Admi-
nistra-tion
use Side action
Epineph-rine
αβ Rapidpotent
Sc, inhale
urgent Arrhyth-mias
nephrine αβ Long durationLess potent
Sc, IM
Pre treat-ment
CNS excitation
Isoprote-renol
β Rapidpotent
Inhale,oral
urgent Arrhyth-mias
Aibuterol, terbutaline
β2 potent Inhale, po, sc
regular Muscle tremorNervous

Muscarinic Antagonists
Mechanism of Action: o M- R:1.contraction of airway smooth
muscle o 2.increased mucous secretion
Clinical Use— Antimuscarinic Drugs
Effective bronchodilators Antimuscarinic drugs are only capable of prev
enting the cholinergic-mediated bronchospasm( 支气管痉挛 )
o Preferred route of administration (enhanced organ selectivity): inhalation
o Antimuscarinic with limited systemic adverse effects: ipratropium bromide
Adverse Effects: o Local: dry mouth; pharyngeal irritation o Systemic: (dependent on extent of absorptio
n) o Urinary retention o Loss of ocular accommodation o Tachycardia( 心动过速 )
o May increase intraocular pressure in patients with glaucoma ( 青光眼 )

Theophylline( 茶碱 )
o Aminophyllineo Theophylline-ethylenediamine ( 乙二胺 ) complex Most commonly used is aminophylline( 氨茶碱 )
Theophyllineo It is slightly water-soluble; often administe
red as salts containing various amounts of theophylline base
o aminophylline: 86% theophylline oxtriphylline( 胆茶碱 ): 64% theophylline
mechanisms of theophylline
1.high concentrations : phosphodiesterase( 磷酸二酯酶 )inhibition
↓ intracellular cAMP↑
↓ cardiac stimulation smooth muscle relaxation
positive chronotropic

mechanisms of theophylline
• 2.inhibition of adenosine( 腺苷 )cell surface receptors modulators of adenylyl cyclase activity
Adenosine histamine release from lung cells
• airway smooth muscle contraction
钟乔
Vincent.Lan All rights reserved
Mechanisms of theophylline
3. Anti-inflammatory action: low-dose theophylline: inhibit late response to
antigenic challenge


Cardiovascular Effects: o Direct positive chronotropic o Direct enhanced myocardial contractility
low doses: increased catecholamine release
high doses: enhanced calcium influx
Renal Effects:
o weak diuretics-- not therapeutically important
increased glomerular filtration reduced tubular sodium reabsorption
Smooth Muscle Effects:
o Major Therapeutic Effect: Bronchodilation Adverse Effects: dose limiting
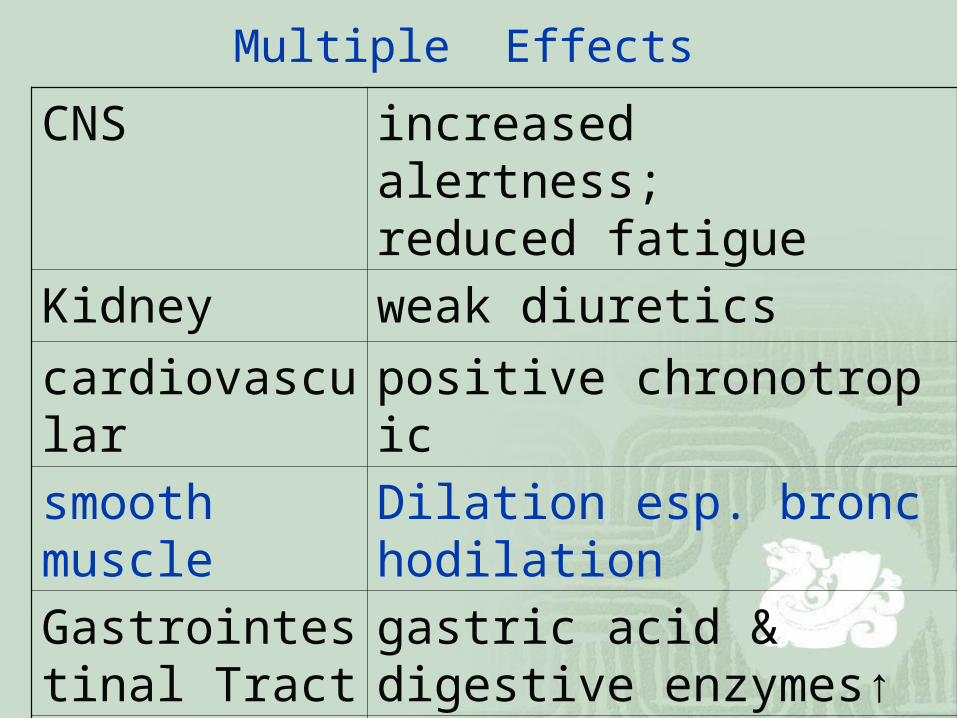
Multiple Effects
CNS increased alertness;reduced fatigue
Kidney weak diuretics
cardiovascular positive chronotropic
smooth muscle
Dilation esp. bronchodilation
Gastrointestinal Tract
gastric acid & digestive enzymes↑
skeletal muscle
enhanced contraction
Theophylline Clinical Use
most effective bronchodilator o Relieves airway obstruction in acute
asthma o decreased frequency and severity of
symptoms in chronic asthma

Theophylline Therapeutic/toxic effects: related to plasma conce
ntration o 5-20 mg/L ---improvement pulmonary functiono > 20 mg/L—nausea, vomiting, headache, anxiety,
anorexiao > 40 mg/L—seizures, arrhythmias
Corticosteroids
Corticosteroid Effects: o Diminish bronchial reactivity o Increase airway diameter o Reduced frequency of asthma
attacks

corticosteroids
Mechanisms of Action:o primary: o anti-inflammatory action------o inhibition of cytokine productiono secondary: o enhancement of beta-receptor
agonist effects
Clinical Use: Corticosteroids
management of acutely ill patients • patients not adequately maintained with
bronchodilators • patients whose symptoms are worsening,
despite reasonable maintenance treatment

Cromolyn & Nedocromil ----action
o inhibit: antigen or exercise-induced asthma
o reduce bronchial reactivity no direct effect on airway smooth muscle tone and will not reverse asthmatic bronchospasm( 支气
管痉挛 )
Cromolyn -------------Mechanism of Action:
alters function of delayed chloride channels→ inhibits cell activation
Airway nerves------cough Mast cells -------degranulation Eosinophils---------inflammatory

Cromolyn------------ Pharmacokinetics
o poorly absorbed o administered by microfine powder
inhalation or aerosol( 雾化 ) o -------- throat irritation
Cromolyn & nedocromil Clinical Use: o pre-treatment: o blocks bronchoconstriction o antigen inhalation aspirin-induced blocks environmental agents

Cromolyn
o Reduces o bronchodilators medication o requirements o symptomatic severityo reducing symptoms allergic o rhinitis

cromolyn
o ◆Adverse/Side effects: o --------minor and localizedo throat irritation cough mouth dryness wheezing chest tightness

Leukotriene Pathway Inhibitors arachidonic acid
5-lipoxygenase( 脂肪氧化酶 ) by eosinophils,
macrophages,basophils
o Leukotriene LTB4--chemattractant LTD4--bronchoconstriction LTC4 mucosal edema mucus hyper-secretion bronchial reactivity↑
Zeleuton( 齐留通 )
Zafirlukast
Montelukast
Other drug groups
o calcium channel blockers o nitric oxide donors o potassium channel activators o Anti-IgE Monoclonal Antibodies
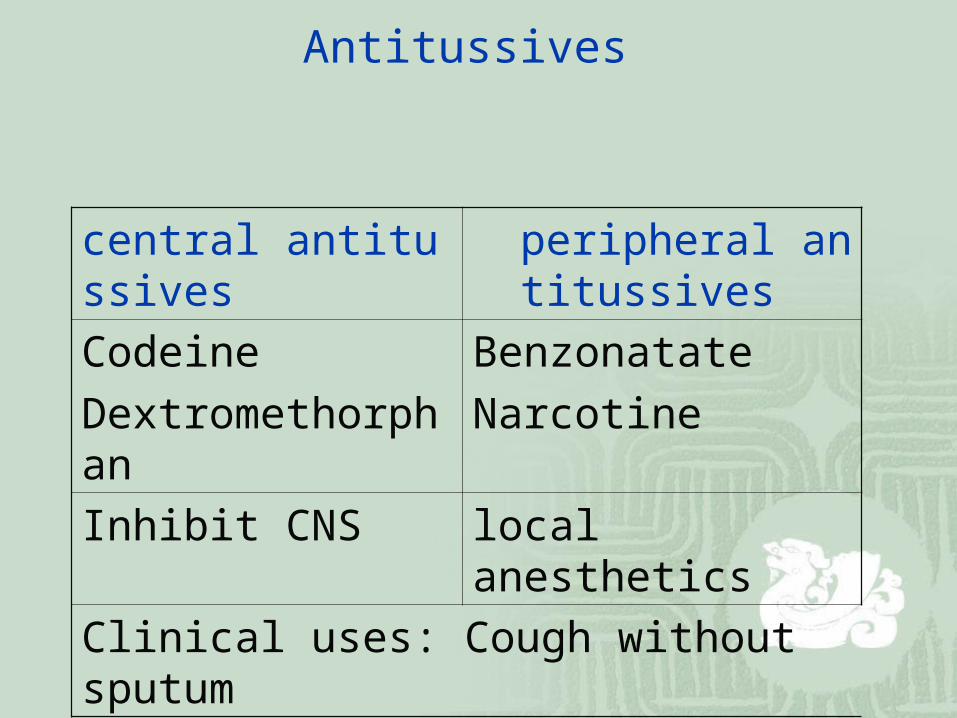
Antitussives
central antitussives peripheral antitussives
Codeine
Dextromethorphan
Benzonatate
Narcotine
Inhibit CNS local anesthetics
Clinical uses: Cough without sputum
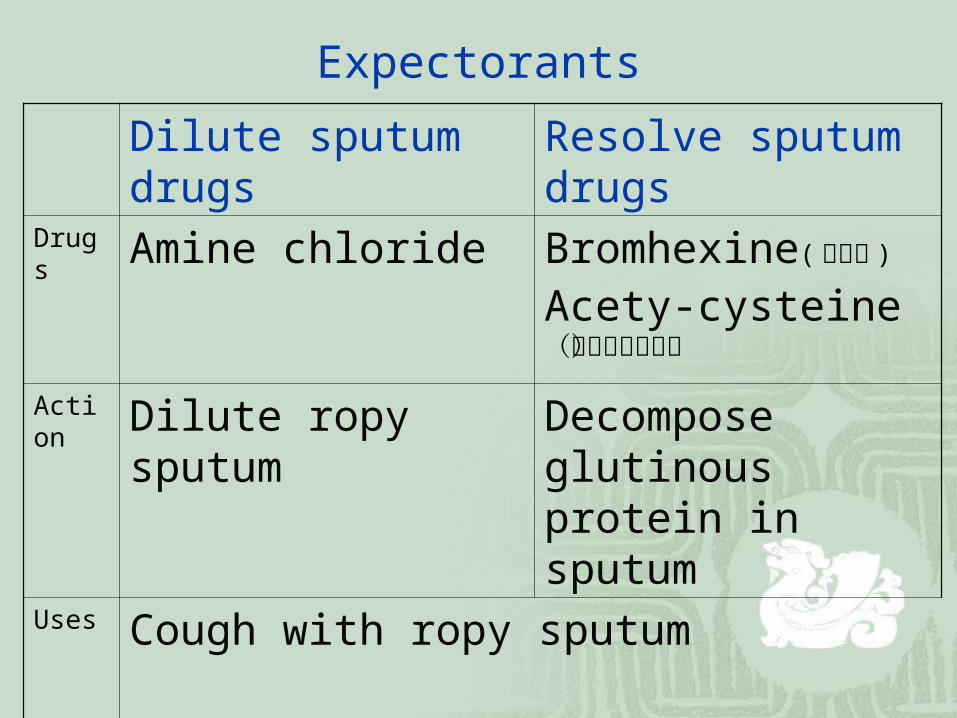
Expectorants
Dilute sputum drugs Resolve sputum drugs
Drugs Amine chloride Bromhexine( 必消痰 )
Acety-cysteine (乙酰半胱氨酸)
Action Dilute ropy sputum Decompose glutinous protein in sputum
Uses Cough with ropy sputum