Diagnosing and treating pancreatitis - IDEXX Laboratories · Dr. Roberta Relford: We’ve met here...
16
A roundtable discussion Sponsored by an educational grant from IDEXX Laboratories Prevalence Associated factors Clinical signs Diagnostics Blood tests Imaging Treatment Acute pancreatitis Chronic pancreatitis What’s inside Diagnosing and treating pancreatitis
Transcript of Diagnosing and treating pancreatitis - IDEXX Laboratories · Dr. Roberta Relford: We’ve met here...

A roundtable discussion
Sponsored by an educational grantfrom IDEXX Laboratories
Prevalence
Associated factors
Clinical signs
DiagnosticsBlood testsImaging
TreatmentAcute pancreatitisChronic pancreatitis
What’s inside
Diagnosing andtreating pancreatitis
Dr. Roberta Relford:We’ve met here today to talkabout pancreatitis. Let mestart by asking, “What is pancreatitis?”
Dr. Jörg Steiner: Pancreatitisis an inflammatory disease ofthe pancreas. It can be associ-ated with different types ofinflammatory cells. You couldalso define it as an autodiges-tion of the pancreas followedby inflammation.
Relford: Which comes first—autodigestion or inflammation?
Steiner: If you define auto-digestion as premature en-zyme activation, then auto-digestion would occur first,before cytokines recruitinflammatory cells.
Relford: Is there a bacterialcomponent to pancreatitis?
Steiner: As far as we know, there isn’t a bacterialcomponent in dogs and cats, but there appears to be one in some humanpatients with pancreatitis.However, the bacteria, which usually originate from the intestine and are disseminated in the blood-stream, do not cause clinicalproblems in people until three to four weeks after thepancreatitis begins.
Relford: Are all pancreatitiscases the same?
Dr. David Twedt:Absolutely not. In fact, pan-creatitis can vary from mild to life-threatening—and any-thing in between. That makesit difficult for practitioners todetermine whether patientshave acute gastroenteritis thatwill improve within 24 hoursor acute pancreatitis. In dogs,we see more cases of acutepancreatitis. I don’t thinkwe’re good at recognizingchronic cases.
Dr. David Williams:Classically, the differentiationof acute and chronic pancre-atitis is a histologic one. Butdefining the clinical diseaseitself is much more complicat-ed than that because it’s usu-ally not feasible to obtain pan-creatic biopsy samples. Inaddition, some cases are sub-clinical, and even in clinicalcases, lesions may not beidentified without a thoroughexamination of multiple pan-creas samples at necropsy.
Relford: In acute vs. chronicpancreatitis, where does fibro-sis come into play?
Williams: The difference be-tween acute and chronic pan-creatitis is that chronic casesinvolve irreversible changes tothe structure of the pancreas—most commonly, fibrosis asso-ciated with some loss of func-tion. Acute pancreatitis is afully reversible disease, andrecovery is associated withreturn to normal function.
However, we obviously can’tobtain pancreatic biopsies in most clinical cases, so strict differentiation betweenacute and chronic disease is often impossible.
PrevalenceRelford: How prevalent ispancreatitis?
Steiner: The true prevalence is unknown. The classic studyconducted in Germany about20 years ago showed exocrinepancreatic lesions in 1.7% ofdogs and 1.3% of cats. Two-thirds of those lesions werepancreatitis.1 However, some of the animals had only onesection examined. Today weknow that pancreatitis can behighly localized in any species,so researchers conducting thatstudy 20 years ago may havemissed many of the pancrea-titis lesions.
A recent study conducted atThe Animal Medical Center inNew York2 involved more than200 dogs that were necropsiedfor reasons unrelated to sus-pected pancreatitis. Investiga-tors sampled the pancreasesevery two centimeters andfound lymphocytic infiltrationin 52.5% of all cases and neu-trophilic inflammation in31.7% of all cases. But thequestion is: Which ones wereclinically significant? It’s un-likely that 52% of all dogshave significant pancreatitis.
Williams: Whatever the pre-valence is, pancreatitis has
2
Participants:David A. Williams,MA, VETMB, PhD, MRCVS, DACVIM, DECVIM-CADept. of Veterinary Clinical
MedicineCollege of Veterinary
MedicineUniversity of Illinois at
Urbana-ChampaignUrbana, Ill.
Jörg M. Steiner,MED.VET, DR.MED.VET, PhD,DACVIM, DECVIM-CADept. of Veterinary Small
Animal Clinical SciencesCollege of Veterinary
Medicine & Biomedical Sciences
Texas A&M UniversityCollege Station, Texas
H. Mark Saunders,VMD, MS, DACVRLynks Group PLCShelburne, Vt.
David Twedt,DVM, DACVIMDept. of Clinical SciencesCollege of Veterinary
Medicine & Biomedical Sciences
Colorado State UniversityFort Collins, Colo.
Benita von Dehn,DVM, DACVIMThe Animal Care CenterRohnert Park, Calif.
Moderator:Roberta Relford,DVM, PhD, DACVP, DACVIMIDEXX Reference LaboratoriesDallas, Texas Using the latest diagnostic tests, practitioners are detecting
acute pancreatitis more frequently today than ever before. Early diagnosis is critical for the successful management of this devastating disease.
Cover art by Paul Chason.© 2006 IDEXX Laboratories.
All rights reserved.
Diagnosing and treating pancreatitis
been dramatically under-recognized in the past—especially in cats. I think weare recognizing it more andmore in dogs.
Relford: I agree. The preva-lence of pancreatitis probablyisn’t increasing—we’re justdetecting it more often.
Clinical signsRelford: What are the clinical signs of pancreatitis in animals?
Dr. Benita von Dehn: Theclassic signs in dogs includeanorexia, vomiting, and ab-dominal pain. Vomiting is morecommon in dogs than cats.Additional signs may includeweakness, nausea, drooling,depression, diarrhea, and,occasionally, a fever. In cats,we tend to see more prolongedanorexia, lethargy, and weightloss. The difficulty arises inthe fact that these clinicalsigns are also often associatedwith other diseases.
Williams: Pancreatitis isn’talways an isolated disease.Increasingly, we’re recognizingcases where patients have notonly pancreatic lesions butalso intestinal, gastric, orhepatic lesions. So the signsmay have one or multiplecauses, especially in cats.
Twedt: The abdominal painwe usually associate with pan-creatitis does not occur in allcases. Some studies say ap-proximately 50% exhibitabdominal pain.3
Steiner: In reality, practi-tioners could suspect pancre-atitis with any sick patient.Recently, a friend of mineconsulted with me on hisolder miniature schnauzer.For years, my friend went
to different veterinarians, trying to figure out why the dog wouldn’t play everyday. There were no other clinical signs. We diagnosedchronic pancreatitis andadministered treatment, and the dog plays every daynow. In fact, my friend sayshe has a puppy again.
Practitioners may think that clinical signs in dogs aremore severe and easier to spotthan the more nonspecificclinical signs found in cats.But if you look at the entirespectrum of the disease, I’msure we would find plenty ofdogs with unusual and atypi-cal clinical signs that don’tsuggest pancreatitis.
Relford: Dr. Williams, youmentioned subclinical pancre-atitis cases earlier. Is thereanything practitioners can look for in patients withoutclinical signs?
Williams: Some endocri-nologists recommend that veterinarians screen diabeticanimals for concurrent pan-creatitis because this is apotential aggravating factorthat makes diabetes manage-ment more difficult. That’sone example where it’s rea-sonable to screen patientswithout signs of pancreatitis.
Steiner: It depends on howaggressive veterinarians want to be. Fifty years ago, animalsdiagnosed with renal diseasewere in end-stage renal fail-ure. That’s because creatinineusually elevates before a patient shows clinical signs.By the time the clinical signs appear, about 80% ofthe kidney is gone. Todaypractitioners look for markersof early kidney disease; theydon’t wait for clinical signs to appear before they runtests. Every chemistry profileincludes creatinine and BUN analyses. When I’m on the clinic floor, we run a chemistry profile on everydog with suspected renal disease—whether it’s clinicalor subclinical.
Why should it be differentfor pancreatitis? Like renal disease, pancreatitis may startlong before the clinical signsappear. In 20 or 30 years, Ithink we’ll be screening forpancreatitis the same way we screen for renal or hepaticdisease today.
Twedt: Fortunately, we havefound ways to prolong survivalin patients with renal disease.If practitioners can anticipatecomplications with pancreati-tis, they can try to slow downthe disease’s progression.
Relford: Is it fair to say that the earlier a clinicianidentifies pancreatitis, thebetter the likelihood for thepatient’s survival?
Steiner: That’s a fair statement.
3
Pancreatitis isn’t always an isolated disease. Increasingly,
we’re recognizing patients withintestinal, gastric, or hepaticlesions—not just pancreatic.
So the signs may have one or multiple causes, especially in cats. David Williams
In dogs, the classicclinical signs of pancreatitis are:
• anorexia• vomiting• abdominal pain.
Other signs mayinclude:
• nausea• drooling• depression• diarrhea• fever.
Cats usually exhibitsigns of anorexia,lethargy, and weightloss.
Diagnosing pancre-atitis can be difficultbecause these signsare often associatedwith other diseases.
Clinical signs of pancreatitis
Williams: I think it dependson the group of animals you’reevaluating. There are dogswith chronic pancreatitis thatare not going to die from it,but heightened awareness canhelp practitioners preventacute flare-ups. If practition-ers recognize severe acutepancreatitis early, they caninstitute aggressive supportivetherapy for this potentiallyfatal disease sooner.
Twedt: Absolutely. Pancreati-tis mimics so many other diseases. If practitioners canidentify pancreatitis, they candirect their efforts to managingit and not looking for a liverproblem, gastroenteritis, orinflammatory bowel disease.
von Dehn: I would add thatpatients might have a betterprognosis if practitioners canidentify and remove an incit-ing or incriminating agent.
Williams: That’s a goodpoint. Specific causes
may not be identified fre-quently, but when they arerecognized, practitioners canmanage them.
Steiner: But it’s also impor-tant to step back and take a more general look. One could make the statementthat if a specific cause cannotbe identified, then outcome is really dependent on thepresence of systemic compli-cations (e.g., hypoperfusion,disseminated intravascularcoagulation [DIC], pulmonaryfailure, renal failure) and pan-creatic complications (e.g.,pancreatic necrosis and ab-scesses) and not so much oninciting causes.
Associated factorsBreed, age, sexRelford: Which breed, age, or sex characteristics are asso-ciated with pancreatitis?
von Dehn: In general, pan-creatitis tends to occur inmiddle-aged, neutered dogs
with no gender preference.Dogs with pancreatitis areoften overweight. Terrier andnonsporting breeds tend to beoverrepresented. Cats diag-nosed with pancreatitis tendto be older, neutered, domes-tic shorthaired breeds with noobvious gender predilection.
Steiner: I generally find thesame tendencies. But I nowbelieve that cats of any agecan develop pancreatitis.When we studied a group of 20 cats with exocrine pan-creatic insufficiency, whichwe assumed was caused bychronic pancreatitis, three of them were less than 6months old. The cats musthave experienced enough pancreatitis in those first sixmonths of their lives to de-stroy their pancreases. Thatchanged my mind.
Relford: So is it fair to saythat pancreatitis can occur inanimals of any age, breed, orsex, even though there’s a
higher incidence in the populations Dr. von Dehndescribed?
Williams: Yes, although there is little evidence to sup-port that statement. There iscertainly anecdotal evidenceof a predisposition in minia-ture schnauzers, and there is published evidence of agenetic component predispos-ing German shepherds tochronic lymphocytic pancre-atitis, which can lead to pan-creatic insufficiency.4
DrugsRelford: Are any predisposingfactors drug-related?
Williams: Yes. Potassium bro-mide and many chemotherapyagents are implicated.
Steiner: I would say potassi-um bromide is the biggest factor. We’ve seen pancreatitisin 6.4% of patients treated with potassium bromide. That is probably higher thanwith L-asparaginase or vinca alkaloids—the big cancerdrugs that can cause pancre-atitis. I suspect the second-highest drug-related factor forpancreatitis is L-asparaginase.
Our studies with potassiumbromide show that the associ-ation with pancreatitis is notdose-dependent. That alsosuggests that the pancreatitisis probably an idiosyncraticreaction.
Twedt: We occasionally seeanimals that we believe havepancreatitis associated withazathioprine.
Steiner: In human medicine,doctors follow a more system-atic reporting method. The listnow contains 54 drugs anddrug classes suspected ofcausing pancreatitis. Virtually
4
Diagnosing and treating pancreatitis
DrugsAlthough any drug can potentiallycause pancreatitis, the most com-mon associations involve:
• potassium bromide• chemotherapy drugs,
especially L-asparaginase• antibiotics, especially tetracy-
cline and sulfonamides• organophosphates.
Diseases and medical conditionsA cause-and-effect relationship has been found between pancre-atitis and the following:
• feline viral diseases (e.g., calicivirus infection),
toxoplasmosis, and a hepaticfluke infection
• immune-mediated disorders• hypercalcemia.
Other factorsAnimals may also develop pancre-atitis from:
• high-fat and, possibly, low-protein diets
• a genetic predisposition• surgical interference secondary
to hypovolemic, hypotensive, or ischemic insults to the pancreas
• trauma.
Associated factors
any drug you can imagine is on that list. I would go asfar as saying that any drug canpotentially cause pancreatitis,just like any drug can poten-tially cause acute hepaticnecrosis through an idiosyn-cratic reaction.
Williams: Years ago, we sawquite a few cats develop pan-creatitis after being treatedwith tetracyclines.
Steiner: That association has been reported in people,too. A whole range of antibi-otics is associated with pan-creatitis, but tetracycline and the sulfonamides are the most common.5
There have also been re-ports linking organophos-phates to pancreatitis in cats.6
Relford: Just in cats?
Steiner: It hasn’t been re-ported in dogs, but I wouldassume that treating a dogwith organophosphates wouldpose the same risk. In additionto cats, children in third worldcountries have developed pan-creatitis from organophos-phates. I can’t see why dogswouldn’t be affected.
Twedt: What about cortico-steroids? The literature oftenreferences them as potentialcauses of pancreatitis. But ifyou think about all the ani-mals treated with cortico-steroids, the connection withpancreatitis is minimal.
Williams: There is certainlyevidence that corticosteroidsin dogs cause serum lipaseactivity to increase, and while veterinarians used tothink there was a pancreaticassociation, there are no pan-creatic lesions in treated ani-mals.7 The lipase must be
another type of lipase, possi-bly hepatic.
Steiner: In human medicine,corticosteroids have been re-moved from the list of drugscausing pancreatitis; however,a lot of patients on steroidshave diseases that predisposethem to pancreatitis, so theprimary disease process may be at fault, not thesteroids administered to treat those diseases.
DiseasesRelford: Are there any dis-eases in dogs that predisposethem to pancreatitis?
Williams: In the literature,pancreatitis is often listed as a complication of hyper-adrenocorticism,8 but, over the years, I have not seen that association.
von Dehn: Infectious etiolo-gies have been described moreoften in cats, unlike dogs.9
Steiner: One may think thatbacterial infections can causepancreatitis in cats, but, actu-ally, the two have never beenassociated. Instead, felinepancreatitis is associated with certain viral diseases(including calicivirus infec-tion), toxoplasmosis, and
infection with a hepatic fluke called Amphimeruspseudofelineus. Feline infec-tious peritonitis, feline im-munodeficiency virus infec-tion, feline leukemia virusinfection, and panleukopeniahave also been reported tocause pancreatitis, but acause-and-effect relationshiphas not been demonstrated.
Williams: In many of those cases, however, pan-creatitis is only part of thepicture because there areoften concurrent diseases,especially in cats.
Steiner: I also think weshould mention immune-mediated pancreatitis. Twentyyears ago, the disease wasunknown in people, and nowit’s considered fairly common.If you look at the progressionin people, you can almost pre-dict the same progression inanimals. I would bet that 20years from now, veterinarianswill be saying, “Yes, a lot ofthese idiopathic cases—pastand present—are actuallyimmune-mediated disorders.”However, it will take a lot ofstudies to define the diseasein dogs and cats.
Williams: At this point, it has been shown that immune-
mediated lymphocytic pancreatitis predisposes German shepherds to pan-creatic atrophy.4
Steiner: One may think thisdifferentiation of idiopathicand immune-mediated pan-creatitis is merely academic;however, it is really huge: Idio-pathic pancreatitis can’t betreated, but immune-mediatedpancreatitis can be treated with corticosteroids.
Medical conditionsRelford: Are any other med-ical conditions considered tobe predisposing factors?
Steiner: Hypercalcemia caus-es pancreatitis. I see thisquite frequently in the clinic.Dogs that present with aserum calcium concentrationof 14 mg/dl or higher mayhave concurrent pancreatitis.Of course, lymphoma or ananal sac adenocarcinoma isusually the underlying causeof the hypercalcemia.
Williams: We test numerousblood samples from diabeticanimals, and some of themshow evidence of chronic pan-creatitis or acute pancreatitisflare-ups, which may predis-pose the animals to periods of insulin resistance.
5
I would go as far as saying that any drug can potentially
cause pancreatitis, just like any drug can
potentially cause acute hepatic necrosis through an idiosyncratic reaction. Jörg Steiner
von Dehn: Wouldn’t every-one agree that evidence suggests that obese dogs onlow-protein, high-fat diets are potentially predisposed to pancreatitis?10,11
Williams: Some animals withnormal body weights developpancreatitis, but there is evi-dence from experimentalstudies that obese dogs willget more severe pancreatitisthan underweight dogs, andobesity is certainly a potentialrisk factor for complicationsof pancreatitis.
Relford: So does diet play a role?
Williams: Hyperlipidemia,which clients and veterinarianscan modify with diet, almostcertainly does. We believe thatit’s associated with pancreatitisin schnauzers, but I don’tknow if it’s been proved thathyperlipidemia predisposesanimals to pancreatitis.
Relford: So what about thoseanimals that are fed bacon inthe morning and presented tothe veterinarian in the after-noon with pancreatitis?
Williams: Some of them have pancreatitis, but many of them probably have non-specific gastroenteritis.
Steiner: There are two sidesto the fat issue. Of coursethere is a clinical impressionthat most veterinarians share:High-fat meals cause pancre-atitis. However, there is littlescientific evidence for a cause-and-effect relationship. Onlyone study has been done thatevaluates the relationshipbetween a high-fat diet andpancreatitis.11 In this study, agroup of healthy dogs were fedpork lard exclusively for sixweeks. These dogs developedpancreatitis, but they died ofhepatic necrosis. Unfortunately,I don’t think the study is clini-cally relevant to the patientspractitioners see every day.
However, I do believe that dietplays a role because dietarymanagement in many of thesedogs is quite successful,whether it’s for acute or chronic pancreatitis.
Williams: Diets extremelylow in protein have beenshown to predispose animalsto pancreatitis, although it’srare.11 Dr. Steiner hit on thebigger point: Patients withchronic pancreatitis oftenrespond to low-fat diets.
Relford: So I’m hearing thatdiet plays an important role inmanaging pancreatitis, but itrarely causes pancreatitis. If a happy, healthy dog runsaround wagging its tail one dayand the next day gets pancre-atitis, what flipped the switch?
Williams: Those cases aremostly idiopathic. There’s onestudy that says obesity is apredisposing factor,12 but thecontrol group might have beenunderweight. The pancreatitispopulation was heavier thanthe nonpancreatitis popula-tion, but I’m not sure theywere really obese. That’s whyI’m hesitant to agree with thestudy’s assertion. However,there are many other reasonsto try to control obesity.
Other factorsRelford: Are there any otherpredisposing factors wehaven’t mentioned?
von Dehn: In addition tohigh-fat diets and maybe low-protein diets, practition-ers should consider heredi-tary causes in dogs, as theyhave been implicated in thehuman literature.10
Pancreatitis may also be induced by surgical interfer-ence secondary to hypovole-mic, hypotensive, or ischemic
6
Diagnosing and treating pancreatitis
In chronic cases,serum chemistry profilescan be totally normal.Practitioners need to watchfor occasional vomiting,loss of appetite, weight loss,or unusual behaviors. Roberta Relford
• Variable changes in amylase andlipase activity (elevated lipase maybe present in about 50% of activepancreatitis cases)
• Liver enzyme elevation (mayreflect underlying endotoxemia,dehydration, or both)
• Elevated BUN and creatinine levels (most often secondary tohypovolemia, dehydration, oracute renal failure)
• Hypocalcemia (usually secondaryto concurrent hypoalbuminemia)
• Hyperglycemia (may be due tohyperglucagonemia, stress, ordestruction of islet cells by ongoing pancreatitis)
• Hyperbilirubinemia (secondary to severe hepatocellular damage,intrahepatic or extrahepaticobstruction of bile flow, or both)
• Hypoalbuminemia (usually due to vascular and peritoneal leakage)
• Hypercholesterolemia• Hypertriglyceridemia
Serum chemistry findings associated with pancreatitis
insults to the pancreas. Even a trauma, like getting hit by a car, could predispose an ani-mal to pancreatitis by causingpancreatic hypoxia.
Williams: That’s true. Catsthat have fallen out of highbuildings have developed pan-creatitis, which is probablyrelated to subsequent shockand hypovolemia.
Twedt: It’s also a widespreadmisconception that touchingthe pancreas causes pancre-atitis. In fact, it’s unusual to see pancreatitis developfrom either a laparoscopic orsurgical biopsy of the pan-creas. If it happens, it’s pro-bably because of vascularchanges, hypovolemia, orcytokine release.
Steiner: Doctors in humanmedicine used to believe the same thing. Now theyknow they’re seeing hypoper-fusion of the pancreas duringanesthesia. As it turns out,there is an increased rate of pancreatitis in humanpatients who have undergoneabdominal surgery, open-heart surgery, and leg amputa-tion. Of course, animals candevelop pancreatitis if the surgeon traumatizes the pan-creas, but gentle handling ofthe pancreas is unlikely tocause pancreatitis.
DiagnosticsBlood testsRelford: If an animal presents with anorexia, ab-dominal pain, vomiting, orother gastrointestinal signs,what tests should practition-ers perform first?
von Dehn: I don’t assume it’s pancreatitis, but it’s defi-nitely on the differential list.Every dog receives a complete
physical examination and aminimum database evaluation,including a complete bloodcount (CBC), serum chem-istry profile, and urinalysis. A pancreatic lipase immuno-reactivity (PLI) test may beincluded. I use the CBC andserum chemistry profile tocheck for systemic complica-tions that might indicate moresevere underlying problems,such as thrombocytopenia orhypocalcemia. I also recom-mend radiographs of the chestand abdomen to rule outother causes of anorexia andvomiting, such as foreign bod-ies, and to check for pleural
effusion or other thoracic ab-normalities. After reviewingthe radiographs, I usually pursue ultrasonography, if indicated.
Relford: What should practi-tioners look for in a CBC andserum chemistry panel?
von Dehn: Inflammatory orinfectious leukograms are acommon laboratory change in patients with severe acutepancreatitis. Mild elevations in the packed cell volume arelikely a result of dehydrationand will often decrease withfluid therapy.
In addition, numerous
serum chemistry findings areassociated with pancreatitis(see the sidebar on page 6).
Steiner: But pancreatitis isn’tlike kidney failure, where youcan rule it out just by findinga normal serum creatinineconcentration. With pancreati-tis, it’s more complicated; thefindings aren’t always cut anddried. If practitioners don’tfind the signs Dr. von Dehnjust mentioned, it only makespancreatitis less likely.
Relford: So if the results of a minimum database arenot consistent with acute
pancreatitis, that doesn’t meanpancreatitis isn’t present.
Twedt: Absolutely. I getfooled all the time by caseswhere the bilirubin is high,the liver enzymes are abnor-mal, and the animal is vomit-ing. I assume it’s liver disease.But additional diagnosticsreveal pancreatitis as the pri-mary cause; the liver prob-lems are secondary to thepancreatitis. Practitionershave to rule out the other dis-eases first because a mini-mum database or radiographwon’t necessarily indicatepancreatitis, and pancreatitismimics many other diseases.
Relford: In chronic cases,serum chemistry profile re-sults can be totally normal.Practitioners need to watchfor clinical signs, which wementioned earlier, includingloss of appetite, occasionalvomiting, weight loss, or unusual behaviors.
Williams: In patients withsuspected chronic pancreatitisor chronic small intestinal dis-ease, I would combine anevaluation of the pancreaswith serum cobalamin andfolate tests, which are goodscreening tests for chronicsmall intestinal disease.
Steiner: Let’s face it, most ofthe abnormalities in a serumchemistry profile are notcaused by pancreatitis; theyare changes associated withthe complications from pan-creatitis. Practitioners won’tfind those changes unless thepancreatitis is severe enoughto cause those complications.
Relford: What about lipaseand amylase activities? Ani-mals with pancreatitis may ormay not have elevated levels.
Twedt: We still run amylaseand lipase at our hospital. If all other clinical parametersand laboratory findings suggest
7
I get fooled all the time bypatients with high bilirubin,abnormal liver enzymes, andvomiting. I assume it’s liver
disease, but additional diagnostics reveal pancreatitis
as the primary cause. David Twedt
pancreatitis, it may help sup-port that diagnosis. It’s justanother piece of the puzzle.
Williams: Elevated amylaseand lipase activities meansomething is wrong with the animal, but it’s most likely gastrointestinal, hepatic,or renal disease. Unless activi-ties are severely increased,pancreatitis is possible butnot probable.
Steiner: I wouldn’t limit it tothose three diseases. The list of conditions that could triggerfalse elevations of serum lip-ase activity in small animals is endless—hepatic disease,renal disease, sepsis, cancers,pulmonary failure, and muscleactivity are just a few. Never-theless, veterinarians can useit as a guideline, but in mymind, it isn’t acceptable for a definitive diagnosis.
von Dehn: If the CBC and serum chemistry profiledon’t help with the diagnosisof pancreatitis and I amunsure about serum amylaseand lipase activity, I may run a serum PLI test. Thistest is more sensitive and specific than any other test,including trypsin-likeimmunoreactivity (TLI).
Relford: Dr. Williams, couldyou comment on using TLI todiagnose pancreatitis?
Williams: We’ve been usingTLI for more than 20 years todiagnose pancreatic insuffi-ciency, and it remains anexcellent test. When the testbecame available, I was hop-ing we could use it to diagnoseacute pancreatitis. It didn’ttake long for us to realize itslimitations. Currently, it iden-tifies pancreatitis in 33% to66% of affected animals. In
cats, it’s much better thantesting for amylase and lipaseactivities, but it falls far shortof what practitioners wouldlike to see. But it’s excellentfor diagnosing pancreatic in-sufficiency in dogs and cats.
Relford: Amylase and lipasetests can produce false posi-tives and negatives. Are TLIelevations usually consistentwith pancreatitis?
Williams: TLI elevations canoccur in animals with severerenal failure because trypsino-gen is filtered by the kidneys.Before increases in serum TLIbecome apparent in patientswith renal failure, creatininemust increase to at least 3.5mg/dl in cats and 4.5 mg/dl indogs. In most patients, TLIvalues remain normal in theface of renal failure. If practi-tioners obtain high TLI levels,they need to look at renalfunction and follow up with aPLI test to confirm or elimi-nate possible pancreatitis.Perhaps most importantly,normal TLI levels do not ruleout pancreatitis.
There are certain things wedon’t know about PLI either.But if practitioners find a highPLI, there’s a good chance the animal has pancreatitisbecause concentrations do notincrease with renal failure.
Steiner: Veterinarians mustremember that there’s a differ-ence between lipases meas-ured by a PLI test and thosemeasured by a serum chem-istry profile. There are manydifferent lipases in the body.The PLI test is based on animmunoassay and evaluatesthe molecular concentration;it is not based on enzymaticfunction. A serum chemistryprofile may pick up any lipasecirculating in the blood,
whether it’s from the liver,stomach, or pancreas.
Twedt: I use PLI tests in caseswhere I suspect pancreatitisand want to confirm it. Forexample, I use it in acute pan-creatitis cases that I’m treatingsymptomatically, subtle chroniccases where I’m not surewhat’s going on (especially incats), chronic gastrointestinaldisease patients, diabeticpatients that aren’t doing wellor don’t respond to therapy,patients that may have under-lying pancreatitis, or patientswith acute ketoacidosis.
Relford: Should we be testingfor pancreatitis more often torule it out or to see if it’s oc-curring with other diseases?
Steiner: It’s sort of a standingjoke at Texas A&M that,whenever I see a nontypicalpatient, I run a PLI on it.When those patients with sus-pected pancreatitis have nor-mal PLI tests, we look furtherand often find a different dis-ease process. One time, wedid a feeding trial using veteri-nary students’ pets. To be surethe six normal control dogswere healthy, we ran a CBC,serum chemistry profile, andthe newly released PLI. Twoof the PLI tests were abnor-mal, and one showed amarked elevation. We askedthe student if the dog wasexhibiting any clinical signs ofpancreatitis. She said the dogwas happy and healthy. Anultrasound confirmed pancre-atitis without a doubt. Aftertwo weeks on a new diet, thestudent realized that her doghadn’t always eaten breakfastbefore but was now eating itevery day. If a veterinary stu-dent can’t detect clinical signs,how do we think our clientscan? I truly believe that practi-
tioners will find many cases ofsubclinical pancreatitis. Andany case of subclinical pancre-atitis can lead to diabetes,pancreatic insufficiency, or apotentially fatal acute episode.
Relford: So the PLI test ishelpful for diagnosing clinicalor subclinical pancreatitis that may or may not produceultrasonographic findings.This could help practitionersimprove the outcome for pancreatitis patients or ruleout pancreatitis and look forother diseases.
Twedt: Absolutely. If youdon’t look for the disease, youcan’t diagnose it. A practition-er might identify low-gradepancreatitis in an animal withnonspecific gastrointestinalsigns. It may not change theoverall management of thecase, but it alerts the practi-tioner about what to expectlong-term.
Williams: Yes. It may notrequire immediate action, butit makes the practitioner andowner aware that more severesigns of pancreatitis may sur-face sooner or later.
Relford: Dr. Williams, you’veworked closely with IDEXXLaboratories during the lastfew years on the Spec cPL(canine pancreas-specificlipase) test, a modification ofthe canine PLI assay. Will theincreased availability of thisassay alter the way practition-ers handle pancreatitis cases?
Williams: I’m sure that it will.It’s a new test using a relativelynew technology, but the evi-dence to date clearly showsthat it surpasses the otheravailable options (data on file,IDEXX Laboratories). It will bea useful tool for expanding our
8
Diagnosing and treating pancreatitis
knowledge of pancreatitis andrefining patient management inthe future (Table 1).
Relford: So practitioners usingthis new test shouldn’t be star-tled if they start finding more
animals with elevations in pan-creatic lipase concentration.
Williams: I’m sure the testwill help practitioners findmore pancreatitis cases andgain an increasing apprecia-
tion for those patients thathave atypical clinical signs.
Relford: Can the PLI test beused for cats, and is it available?
Steiner: The PLI test for
cats is available only throughthe gastrointestinal laboratoryat Texas A&M University(www.cvm.tamu.edu/gilab;979-862-2861). The test forcats is completely differentfrom the test for dogs.
9
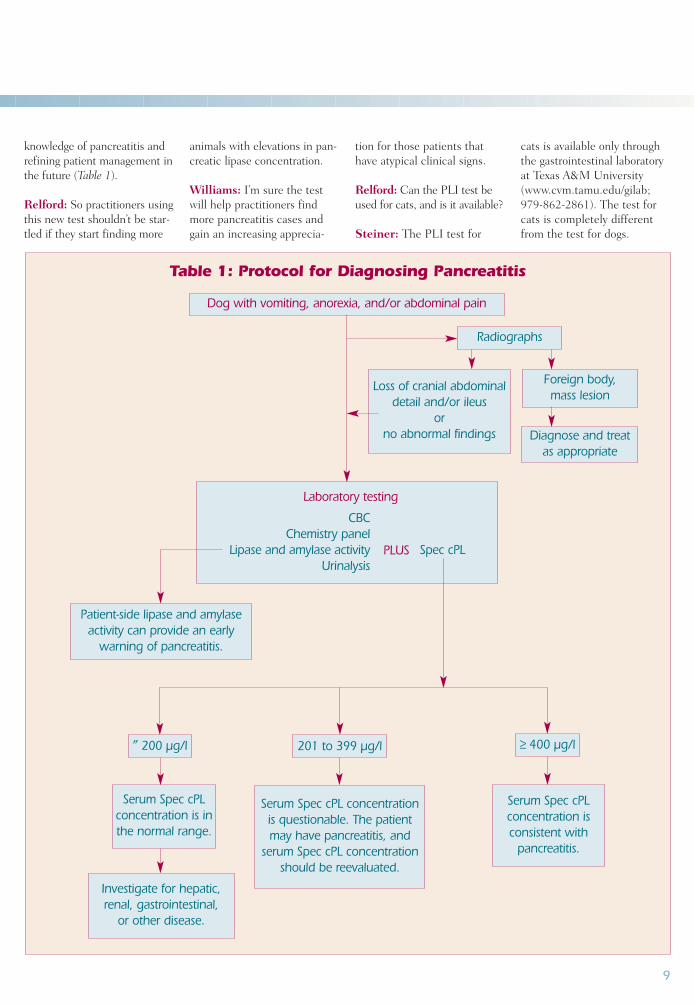
Table 1: Protocol for Diagnosing Pancreatitis
Dog with vomiting, anorexia, and/or abdominal pain
Radiographs
″ 200 µg/l
Foreign body, mass lesion
Loss of cranial abdominaldetail and/or ileus
or no abnormal findings
Patient-side lipase and amylaseactivity can provide an early
warning of pancreatitis.
Investigate for hepatic, renal, gastrointestinal,
or other disease.
Laboratory testing
CBCChemistry panel
Lipase and amylase activity Spec cPLUrinalysis
Diagnose and treat as appropriate
Serum Spec cPL concentration is in the normal range.
201 to 399 µg/l
Serum Spec cPL concentration is questionable. The patientmay have pancreatitis, and
serum Spec cPL concentrationshould be reevaluated.
≥ 400 µg/l
Serum Spec cPL concentration is consistent with
pancreatitis.
PLUS
Relford: What about theSpec cPL test?
von Dehn: Currently, theSpec cPL test is availablethrough IDEXX ReferenceLaboratories. The turnaroundtime is 12 to 24 hours.
ImagingRelford: When practitionersturn to radiographs and ul-trasound for diagnosing pan-creatitis, what should theylook for?
Saunders: Practitionersshould take abdominal andthoracic radiographs to rule out a radiopaque foreign body,signs of gastrointestinal ob-struction, peritonitis, othercauses of an acute abdomen,or a pleural effusion secondaryto pancreatitis.
However, I rarely rely onabdominal radiographs todiagnose pancreatitis. I justdon’t find the classic radio-graphic signs of pancreatitis:widening of the gastroduode-nal angle, loss of right cranialquadrant abdominal detail,loss of peritoneal contrast anddetail, lateral displacement ofthe descending duodenum,gas in the descending duode-num, and gas in the trans-verse colon at the hepaticflexure. I use radiographs
mainly to rule out other possi-ble disease processes.
On the other hand, ultra-sound works well on dogs withsevere acute pancreatitis thatincludes hemorrhage andnecrosis. In those cases, theultrasound will show a severelyhypoechoic, almost mass-likelesion in the right cranialquadrant. The pancreas will beirregular and no longer visibleas a distinct structure. There is substantial peripancreaticinflammation demonstrated by hyperechoic mesentery.There may or may not be asmall volume of peritonealeffusion, either around thepancreas or throughout theperitoneal cavity. Finally, the duodenum may appear plicated and irritated, or it may appear static, withoutactive contractions.
I also think it’s important to look for extrahepatic biliaryobstruction and portal veinthrombosis. This can be difficult—especially in ani-mals that have a lot of painfrom mesenteric inflamma-tion. I have a hard time finding the portal vein anddoing color flow Doppler onpainful patients.
The cases without acutepancreatic hemorrhage andnecrosis are less severe-looking. There may be duo-
denal motility and an absenceof effusion. The pancreas is a hypoechoic structure sur-rounded by hyperechoicmesentery; it doesn’t have thatmass effect in the right cranialquadrant. Beyond that, I havefound that ultrasound isn’tuseful for detecting low-grade,chronic, fibrosing pancreatitis.
Ultrasonographers are re-ported to detect pancreatitis(confirmed histologically) inabout 30% of cats13 and 68%of dogs.3
Steiner: Do you think the68% figure would be highertoday because we’re usingmore modern equipment?
Saunders: Yes. I think the cur-rent sensitivity in severe acutecases is much higher. Thatstudy was conducted 10 yearsago using some relatively inex-perienced ultrasonographers—including me. Our knowledgeand equipment have improvedsince then.
Relford: Does sensitivity relyon individual ultrasonographers?
Saunders: Very much so.There’s a saying about ultra-sound: “You find what you look for, and you only look forwhat you know.” So unlessyou’re clued in to the possibili-
ty of pancreatitis, you may notattach much significance toyour findings. The more pan-creases practitioners visualizeand follow up on, the better they’ll become.
The size of the pancreasand its location also make pan-creatic ultrasounds difficult toperform. Unlike the liver, thepancreas is a small organ, andit’s difficult to detect the pan-creas on a normal abdominalscan. Second, the pancreas is shielded by several gas-containing structures—thestomach, duodenum, andcolon. The right lobe is easierto visualize in a dog, and that’swhy practitioners typicallydetect pancreatitis in the rightlobe. Practitioners don’t seethe normal pancreas in 100%of the animals; this can skewtheir reference point of what isa normal pancreas. I typicallydon’t see the normal pancreason all the dogs I scan, but I do scan the pancreatic regionfor abnormalities.
von Dehn: In my experience,the pancreas of normal dogsand cats is often difficult torecognize as a discrete struc-ture on abdominal ultrasoundbecause the echogenicity issimilar to the adjacent mesen-teric fat.
Steiner: As an internist, Icannot stress enough howimportant it is for practition-ers to rely on experiencedultrasonographers. Buying amachine and completing atwo-day course is not enough.Ultrasonography isn’t thesame as endoscopy or a bonemarrow aspiration, where youknow you’ve been successful.It doesn’t matter if you diag-nose pancreatitis unless youfind out if you’re right.
With that said, my currentconcern with ultrasound re-
10
Diagnosing and treating pancreatitis
When performing ultrasounds, practitioners
don’t see the normal pancreas in 100% of theanimals. This can skew
their reference point of a normal pancreas. Mark SaundersMark Saunders
volves around specificity. Inthe UC-Davis study, threecats that had been suspectedof having pancreatitis had noevidence of it.14 But in two ofthose cats, the ultrasonogra-pher had diagnosed pancreati-tis, so if you just look at thoseanimals, the specificity wouldhave been 33%. That numberwould concern me greatly.
Saunders: Cats are totallydifferent because pancreatitisis much more subtle. Few cats have the blatant-looking,necrotic, hemorrhagic pan-creatitis that I see in dogs.Unfortunately, many of theultrasonographic criteria forpancreatitis in dogs have been applied to cats. In otherwords, practitioners want tosee a hypoechoic, irregularpancreas surrounded by hyper-echoic mesentery. In my expe-rience, that finding is rare incats, and practitioners willmiss many cases of pancreati-tis if they use dog criteria.
I also find that cats withpancreatitis demonstrate lesspain than dogs during ultra-sounds. Cats just lie there andlet you press on the pancreas.
As for statistics, two retro-spective studies reported a 25%to 30% sensitivity in cats forultrasonographic detection ofpancreatitis.13,15 The low sensi-tivity is probably clinically ac-curate. These were real-worldcases that presented with non-specific clinical signs, and pan-creatitis may not have evenbeen on the differential list.
von Dehn: Is pancreatic ductmeasurement of any relevancewhen performing ultrasoundsin cats?
Saunders: It looks like pan-creatic duct size increaseswith normal aging, but itappears unlikely that we will
be able to use duct dilation asan indicator of pancreatitis.16
Twedt: What do you thinkabout the role of ultrasound-guided aspiration in suspectedcases of pancreatitis?
Saunders: Many people feelthat we need to start aspiratingmore pancreases, especially in cats. If aspirations andbiopsies are truly warranted, I think they should be per-formed by specialists, not general practitioners.
von Dehn: How would youproceed if a pancreatic mass orcystic lesion was identified?
Saunders: I will aspirate amass or cyst. A cystic structurecould be either an abscess orpseudocyst—they look similaron ultrasound. You need anaspiration to tell the differ-ence. I sometimes see cysts inthe pancreas of cats, and whenI do, I suspect pancreatitis.
Williams: Have you ever hada complication from a needleaspiration of the pancreas?
Saunders: No.
Williams: The complicationrate in human medicine isincredibly low, less than 3%,and those are nearly all minor.
Saunders: Right. I haven’tperformed that many, butwhen I have performed aspi-rations, they definitely bene-fited the outcome of the case. It’s similar to aspirating a gallbladder—everyone is re-luctant to do it, but I think it’san excellent diagnostic test.
Twedt: I think an aspirationis definitely warranted ifthere’s a small amount of effu-sion. Fine-needle aspiration is
also helpful in determining ifthere’s a tumor or just inflam-mation. If you aspirate carci-noma cells, it’s neoplasia.
Relford: Is there anythingelse on the ultrasound thatwould help practitioners deter-mine if it’s worth performingan aspiration?
Saunders: I don’t think anaspiration or biopsy is neededin pancreatitis cases with a lotof hemorrhage and necrosis.If you stick a needle into that,you’ll probably just get hemor-rhage and necrosis, and it maybe hard to find a more viablesection of the pancreas.
I would contemplate aspi-ration with the cases thatdon’t look quite normal butare not obviously acute andsevere. Maybe they don’t haveeffusion. Maybe they haveslight peripancreatic inflam-mation, and you’re undecidedabout the diagnosis.
Relford: Should veterinariansperform fine-needle or corebiopsies?
Saunders: A core biopsywould be more diagnostic.But it’s a bit more invasive toperform a core biopsy becausewe generally use 14- or 16-ganeedles. With fine-needleaspirations, 22-ga needles can be used.
Relford: What about com-puted tomography (CT)?
Steiner: Two studies havebeen done on CT scans incats. They both found that CTis not very useful.14,15
TreatmentAcute pancreatitisRelford: How should practi-tioners manage patients withacute pancreatitis?
von Dehn: One of the mostimportant treatments for dogsand cats is intravenous crystal-loid support, which helpsrestore pancreatic perfusion,corrects dehydration and electrolyte imbalances, andcompensates for ongoing losses caused by vomiting ordiarrhea. Another commontreatment is colloid support,
11
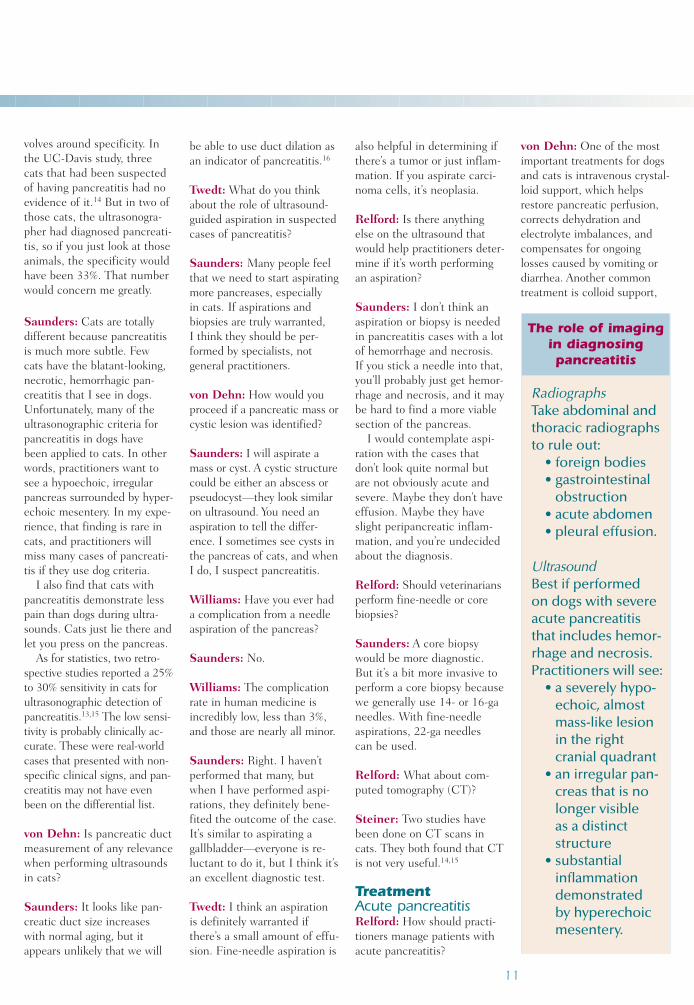
RadiographsTake abdominal and thoracic radiographs to rule out:
• foreign bodies • gastrointestinal
obstruction• acute abdomen• pleural effusion.
UltrasoundBest if performed on dogs with severeacute pancreatitisthat includes hemor-rhage and necrosis.Practitioners will see:
• a severely hypo-echoic, almostmass-like lesionin the right cranial quadrant
• an irregular pan-creas that is nolonger visible as a distinctstructure
• substantialinflammationdemonstrated by hyperechoicmesentery.
The role of imagingin diagnosing pancreatitis

usually in the form of fresh frozen plasma. We suspect that replacing α2-macroglobulins may helpwith pancreatic edema andhypoalbuminemia. Obviously,removal of a possible incitingagent is also instituted.
Instituting antibiotic thera-py is controversial. I initiateantibiotic therapy if a poten-tial for bacterial translocationfrom the gut exists. I also include analgesics in mytreatment plan (e.g., butor-phanol, fentanyl, or meperi-dine) because most of thesedogs have discomfort andpain. If vomiting persistsdespite nothing per os, I ad-minister antiemetics, such asmetoclopramide continuousrate infusion.
Relford: Should practitionersfeed animals with pancreatitis?
von Dehn: We used to with-hold food and water for longperiods—often longer thanfive days. We now realize thatthis may lead to gastrointesti-nal villus atrophy and ileus.Therefore, I now attemptenteral feeding (either bymouth, with an esophagosto-my tube, or with trickle feed-ing through a nasogastrictube) as soon as the vomitinghas subsided, which is usuallyby the third day.
If enteral feeding is tolerat-ed, it has advantages overintravenous total or partialparenteral nutrition and jejunostomy tube placement,which are more costly proce-dures that require an experi-enced staff. Enteral feeding is thought to stabilize the gut barrier and improve intes-tinal motility, decreasing theneed for antibiotics and, pos-
sibly, decreasing the length of hospitalization.
Twedt: I agree that withhold-ing food is an outdated theory.We don’t do it either. Thepancreases in animals with severe or acute pancreatitisprobably don’t produce addi-tional enzymes that make the pancreatitis worse. Withholding food can lead to substantial catabolicdeficits, a higher suscepti-bility to bacterial intestinaltranslocation, decreased pro-tein levels, and decreasedimmune function and neu-trophil function. I think nutri-tion is extremely important.
Steiner: I agree as well.There is no evidence whatso-ever that withholding food hasany beneficial effect. Humandoctors believed that prema-
ture enzyme activation causedpancreatitis, which led to thetheory about inhibiting pan-creatic function and restingthe pancreas.
Twedt: In severe pancreatitispatients, I insert a feedingtube, usually a nasogastric, gastrostomy, or esophagealtube. If you’re performing asurgical procedure, you cansometimes bypass the vomit-ing problem by inserting ajejunostomy feeding tube.
Steiner: The advent of theantiemetic drug dolasetron (0.3 to 0.6 mg/kg IV, SC, ororally once or twice daily) hasdramatically changed the wayI approach these patients.Before, I was always afraid of using metoclopramidebecause anything that antago-nizes dopamine may causesplanchnic hypoperfusion.Dolasetron is an effectiveantiemetic, and it’s affordable.Now I can stop the vomitingin a lot of these animals andfeed them orally or through astomach tube. I couldn’t havedone that before.
von Dehn: Is dolasetron with-in the same drug classification(5-HT3 receptor antagonist) asondansetron (Zofran)?
Steiner: Yes, but it’s far lessexpensive. I don’t know theexact price, but practitionerscan treat a large dog for about$10 a day vs. $50 a day withondansetron. That makes itinexpensive for cats.
Relford: Animals that present with acute vomitingoften have gastritis. Maybethey got into a garbage can,but practitioners don’t know if the animals have pancreati-tis, and they won’t get PLItest results for 12 or 24 hours.
12
Diagnosing and treating pancreatitis
Acute pancreatitis• Provide intravenous crystalloid
support. • Provide colloid support
(usually in the form of freshfrozen plasma).
• Administer analgesics for pain.• Remove inciting agent, if
identified.• Administer antiemetics if vomit-
ing persists despite nothing peros (dolasetron recommended).
• Administer antibiotics if there’s apotential for bacterial translocation.
• Insert feeding tube (in severecases) and begin enteral feeding.
Chronic pancreatitis• Prescribe a low-fat diet with
adequate protein content.• Find drug alternatives for animals
taking drugs known to cause pan-creatitis (see pages 4, 5, and 14).
• Check serum calcium and triglyc-eride concentrations routinely(prescribe gemfibrozil if dietdoes not help lower triglycerides).
• In cats, routinely measure serumcobalamin and correct subnor-mal levels.
Acute gastritis After ruling out a gastrointestinalobstruction or other diseases:• Follow a nothing per os
approach for the first 24 hours.In gastritis cases, the vomitingshould subside fairly quickly.
• Administer intravenous fluidtherapy, if indicated.
• Administer antacids or an H2blocker for nonspecific gastritis.
Treatment of pancreatitis and gastritis
How should practitionersmanage that? When shouldthey start therapy?
Williams: Patients with pan-creatitis probably won’t getbetter immediately. Practi-tioners should begin enteralfeeding after a few days if theanimals haven’t started to eaton their own. Patients withgastritis will likely improvequickly, although they mayneed some fairly aggressiveantiemetic therapy.
Practitioners’ initial treat-ments also depend on theowner’s resources. I think it’s best to evaluate for pan-creatitis initially, but if aclient has limited resources, it may make more sense totreat the pet for 24 hours andthen, if the patient is notrecovering, look for morecomplicated diseases.
Twedt: Could some of theseso-called nonspecific gastritiscases be pancreatitis flare-ups?
Williams: Yes, they could be.
Steiner: But the time frameis important, just as it is forpeople. If two people comeinto a hospital and both pre-sent with similar signs, it’s difficult to determine whichone needs more aggressivecare. Approximately 50% of people who die from pan-creatitis die within the first 72 hours.
I think dogs and cats aresimilar—they come in anddon’t appear that sick, but 24to 72 hours later, they’re dead.I recommend treating bothtypes of cases more aggres-sively at the onset. If practi-tioners begin therapy 24 to 48 hours later, they’re behindthe eight ball. By then, thepatients may have started todevelop systemic complica-
tions of pancreatitis that maybe difficult or impossible tocounteract. Treatment in-cludes pain medication andplasma with evaluation ofpotassium and sodium con-centrations several times aday. You don’t want to missthe point of no return. That’swhy it’s so critical to diagnosepancreatitis early.
Twedt: I think practitionersare usually presented with pa-tients that have some sort of“garbage gut” or acute, self-limiting gastroenteritis. Withsymptomatic therapy, thosepatients usually get betterwithin 24 to 36 hours. Again,you have to consider theseverity of the disease: Is itmild? If they don’t get betterin a short period of time, thenthere’s something else goingon. Those are the cases Iinvestigate further with diag-nostic laboratory tests andradiography.
On the other hand, casesdeemed more severe (i.e.,with protracted vomiting,dehydration, or abdominalpain) require immediate diag-nostics and aggressive therapy.
Relford: So what does symp-tomatic therapy include? You have an animal withsevere acute gastritis, but
it doesn’t look that bad. Youdon’t know if the animal haspancreatitis, and you definite-ly don’t want it to get past thepoint of no return.
von Dehn: I would use anothing per os approach for the first 24 hours. If indicated,I would institute intravenousfluid therapy immediately
and administer antiemetics,provided no gastrointestinalobstruction is present. I mayalso administer antacids or an H2 blocker, such as famoti-dine or cimetidine, for non-specific gastritis. Colloidalsupport is usually not neces-sary in most gastritis cases,unlike pancreatitis.
An example of a gastritiscase that would warrant moreaggressive therapy would behemorrhagic gastroenteritis.
Williams: I would probablyadd radiographs to rule outother diseases.
Steiner: I wouldn’t use anti-emetics in these acute gastri-tis cases. I actually use vomit-ing as a monitoring tool to seehow aggressive I need to be.But in the pancreatitis cases,my goal is to feed them early,so I want to stop the vomitingas quickly as possible.
Twedt: I usually find that ifyou withhold food and waterfrom those patients, the vomit-ing subsides.
Relford: So if it’s just a die-tary indiscretion or mild gas-tritis, the patient should onlyvomit a few times and thenbegin to improve. If it contin-ues to vomit, then practition-
ers need to start institutingmore aggressive therapy andperform other diagnostic tests.
Williams: Practitionersshould also remember painmanagement. We know thatpeople with acute and chronicpancreatitis suffer from ex-treme abdominal pain. I recommend potent analgesictherapy for all dogs and catswith pancreatitis—but not in cases of nonspecific gastri-tis. Classical fears regardingthe use of opiate analgesics(e.g., morphine) in patientswith pancreatitis have nowbeen discounted.
Steiner: I agree. Analgesia isimportant—even for patientsthat go home.
Twedt: Some patients maywag their tails and don’t seemto be in pain. But when youput them on pain management
13
Acute pancreatitis patientswill initially require more
frequent evaluations and PLImonitoring. Chronic cases
may only need rechecksevery few weeks or months
or with acute flare-ups. Benita von Dehn
for pancreatitis, their wholedemeanor changes.
Steiner: Practitioners cansend patients home with fen-tanyl patches, tramadol, ororal butorphanol.
Relford: Once practitionershave diagnosed pancreatitis, isthere anything else they mightconsider a potential problem?
Williams: Fortunately, it’s rel-atively rare, but sometimespancreatic adenocarcinomacauses pancreatitis. In thosecases, a tumor may be causinglocal ischemia, which predis-poses the patient to pancreati-tis development.
Twedt: Pancreatic adeno-carcinoma is a horrible anddevastating disease. I thinkthe prognosis becomes poorer for older animals oranimals that develop pancre-atitis from a concurrentunderlying disease.
Chronic pancreatitisRelford: What are the bestways for practitioners to han-dle chronic pancreatitis cases?
Twedt: I certainly look atdiet, and I look for underlyingdisease as well. I think it’simportant to keep patients’lipid and triglyceride concen-trations down.
Relford: What does evaluat-ing the diet entail?
Twedt: I want to make surethey’re on relatively low-fatdiets with adequate proteincontent.
Steiner: I also routinelycheck the serum calcium andtriglyceride (18-hour fasting)concentrations. If the triglyc-eride concentration is more
than 500 mg/dl, I would mon-itor it to make sure a low-fatdiet decreases it. If not, I putthe patient on gemfibrozil tohelp lower the triglycerides.
Twedt: Those same precau-tions should be taken withhigh-risk dogs, includingschnauzers and shelties thatare prone to hyperlipidemia.
Steiner: It’s also important tolook at drugs in chronic pan-creatitis cases. Veterinariansneed to find drug alternatives,if absolutely needed, forpotassium bromide, L-asparaginase, azathioprine,estrogen, calcium—drugsknown to cause pancreatitis.
von Dehn: Oral pancreaticenzyme supplementation isoccasionally implemented for chronic or recurrent pan-creatitis. Anecdotal evidencehas shown that supplementa-tion may be beneficial in pro-viding negative feedback tothe pancreas by inhibitingpancreatic secretion.
Twedt: It’s thought that pan-creatic enzyme supplementa-tion may decrease pancreaticpain or secretions. In veterinarymedicine, we just don’t know.
Williams: That’s true. Wedon’t know. If practitionershave done everything else, I recommend trying it for amonth or two. It’s a fairlybenign therapy, and the cli-ents can decide if it’s helping.I often tell people to call meif they think it works, but noone has ever called me back.
Steiner: Physicians disagreeon whether it’s beneficial forpeople. For one thing, the pa-tients were given high doses—not doses veterinarians wouldnormally use.17 I tell practition-
ers to try it and see what hap-pens, but they shouldn’t expecta miracle. It’s not going tochange the course of pancre-atitis. It will only change thepain because of the feedbackmechanism in the pancreas.
von Dehn: In patients withchronic pancreatitis, primarilycats, measuring serum cobal-amin levels may be useful, as a fair number of cats haveconcurrent inflammatorybowel disease and hepatic lipi-dosis. Replacing subnormalcobalamin levels allows a moreoptimal therapeutic response.
Relford: When should practi-tioners expect to see sometype of improvement in thesechronic cases? When shouldpatients come back?
von Dehn: Obviously, acutepancreatitis patients will ini-tially require more frequentevaluations and PLI monitor-ing. In cases of chronic smol-dering pancreatitis, practition-ers may only need to schedulerechecks every few weeks ormonths or when acute flare-ups occur.
Steiner: Every case is differ-ent because the disease cov-ers a wide spectrum. In severeacute cases, I run serum PLIsevery two to three days to seeif the patient is improving. I examine the patient, too, but a PLI test mirrors the dis-ease’s clinical progressionquite well. For patients inintensive care for three to four weeks, it might be once a week. For the dog that occa-sionally doesn’t eat his break-fast or receives potassium bro-mide, I may run it every sixmonths. These decisions alsodepend on the clients andhow closely they want tomonitor the disease.
Relford: When should practi-tioners expect to see a changein the PLI result?
Steiner: If I start treating catswith chronic pancreatitis withprednisone, I check the PLIbefore I start the prednisone,and I check it again in 10 to14 days because I want to seea drop in the serum PLI con-centration. If I’m changing thediet, I wait three to four weeks.
von Dehn: How quickly willthe PLI adjust?
Steiner: It will adjust veryquickly. If veterinarians wereable to stop pancreatitis onthe spot, the half-life wouldprobably be no longer than 12 hours. The problem is thatpancreatitis doesn’t just stop, it ebbs and flows.
Relford: What if practitionerswant to start potassium bro-mide treatment or check ananimal that got into thegarbage? How quickly wouldthey see the PLI increase?
Williams: In serum samplesfrom dogs with mild to severeexperimental pancreatitis,which were available for us toevaluate, PLI increased withinhours, and concentrationswere extremely high within sixhours. In samples from catswith experimental mild tran-sient pancreatitis, the increaseswere sustained for more than aweek in all the cats.
Steiner: In that experimentalstudy in dogs, PLIs were ele-vated in severe cases withinone hour after pancreatitis was induced and within threehours for the less severe cases.
Relford: Is there anythingpractitioners or clients can doto prevent pancreatitis?
14
Diagnosing and treating pancreatitis

Twedt: Identify the risk fac-tors (e.g., obesity, hypertriglyc-eridemia, drug therapy) andtry to address them.
If practitioners can identifyflare-ups and confirm previouspancreatitis in chronic cases,they can manage those pa-tients much more aggressively.
Steiner: Perhaps it’s better to ask how practitioners canprevent serious pancreatitis.Asking if we can prevent pan-creatitis as a whole is toobroad. It’s more feasible tofocus on serious pancreatitis.Practitioners can increasetheir awareness with miniatureschnauzers, dogs on potassiumbromide or L-asparaginase,and all the other predisposingfactors we discussed.
Relford: Thank you all forparticipating in today’s round-table. We’ve come full circle,ending our discussion almostwhere it began—at predispos-ing factors. With the latestdiagnostic tools and ongoingdiscussions, practitioners willcontinue to expand theirknowledge of pancreatitis,learning how to better diag-nose and manage this devas-tating, costly disease.
References1. Hänichen T, Minkus G. Retro-
spektive studie zur pathologie dererkrankungen des exokrinen pankreasbei hund und katze. TierärztlicheUmschau 1990;45:363-368.
2. Newman S, Steiner J, Woosley K,et al. Localization of pancreatic inflam-mation and necrosis in dogs. J VetIntern Med 2004;18:488-493.
3. Hess RS, Saunders HM,VanWinkle TJ, et al. Clinical, clinico-pathologic, radiographic, and ultrasono-graphic abnormalities in dogs with fatalacute pancreatitis: 70 cases (1986-1995). J Am Vet Med Assoc 1998;213:665-670.
4. Wiberg ME. Pancreatic acinaratrophy in German shepherd dogs andrough-coated collies: Etiopathogenesis,diagnosis, and treatment. Vet Q 2004;26:61-75.
5. Frick TW, Speiser DE, BimmlerD, et al. Drug-induced acute pancreati-tis: further criticism. Dig Dis 1993;11:113-132.
6. Hill RC, Van Winkle TJ. Acutenecrotizing pancreatitis and acute suppurative pancreatitis in the cat. A retrospective study of 40 cases(1976-1989). J Vet Intern Med1993;7:25-33.
7. Parent J. Effects of dexametha-sone on pancreatic tissue and on serumamylase and lipase activities in dogs. JAm Vet Med Assoc 1982;180:743-746.
8. Williams DA, Steiner JM. Canineexocrine pancreatic disease. In:Ettinger SJ, Feldman EC, eds. Textbookof veterinary internal medicine (Vol. 2).6th ed. St. Louis: Elsevier SaundersCo, 2005;1482-1488.
9. Steiner JM, William DA. Felineexocrine pancreatic disease. In:Ettinger SJ, Feldman EC, eds. Textbookof veterinary internal medicine (Vol. 2).
6th ed. St. Louis: Elsevier SaundersCo, 2005;1489-1492.
10. Williams DA, Steiner JM. Canine exocrine pancreatic disease. In:Ettinger SJ, Feldman EC, eds. Textbookof veterinary internal medicine (Vol. 2).6th ed. St. Louis: Elsevier SaundersCo, 2005;1482-1488.
11. Lindsay S, Entenmann C,Chaikoff IL. Pancreatitis accompanyinghepatic disease in dogs fed a high fat,low protein diet. Arch Path 1948;45:635-638.
12. Hess RS, Kass PH, Shofer FS, et al. Evaluation of risk factors for fatalacute pancreatitis in dogs. J Am VetMed Assoc 1999;214:46-51.
13. Saunders HM, VanWinkle TJ,Drobatz K, et al. Ultrasonographic find-ings in cats with clinical, gross patho-logic, and histologic evidence of acutepancreatic necrosis: 20 cases (1994-2001). J Am Vet Med Assoc 2002;221:1724-1730.
14. Forman MA, Marks SL, DeCock HE, et al. Evaluation of serumfeline pancreatic lipase immunoreactiv-ity and helical computed tomographyversus conventional testing for thediagnosis of feline pancreatitis. J VetIntern Med 2004;18:807-815.
15. Gerhardt A, Steiner JM,Williams DA, et al. Comparison of thesensitivity of different diagnostic testsfor pancreatitis in cats. J Vet Intern Med2001;15:329-333.
16. Larson MM, Panciera DL, WardDL, et al. Age-related changes in theultrasound appearance of the normalfeline pancreas. Vet Radiol Ultrasound2005;46:238-242.
17. Czako L, Takacs T, Hegyi P, etal. Quality of life assessment after pan-creatic enzyme replacement therapy in chronic pancreatitis. Can J Gastro-enterol 2003;17:597-603.
15

09-65647-00