DIABETES IN CARE HOMES 14.5.15 Dr J Stephenson Diabetes... · • The body cannot deal with the...
58
DIABETES IN CARE HOMES 14.5.15 Dr J Stephenson NHS England - Yorkshire and the Humber Strategic Clinical Networks
Transcript of DIABETES IN CARE HOMES 14.5.15 Dr J Stephenson Diabetes... · • The body cannot deal with the...

DIABETES IN CARE HOMES 14.5.15
Dr J Stephenson
NHS England - Yorkshire and the Humber Strategic Clinical Networks

• Dr Jenny Stephenson • Diabetes Lead for Primary Care,
Sheffield • GP, Stannington and Walkley Medical
Centres • GP for Hawkhills Residential Home,
Stannington
NHS England - Yorkshire and the Humber Strategic Clinical Networks

WHAT IS DIABETES?
• A condition in which a person’s blood sugar measurements are generally higher than those in non-diabetic people.
• The body cannot deal with the sugar which comes out of the food or drink the person has, allowing levels to rise
• The person then feels thirsty, tired, becomes incontinent & have thrush & other infections
NHS England - Yorkshire and the Humber Strategic Clinical Networks

WHAT CAN HAPPEN?
• Diabetes can cause the person to feel unwell -
and also to cause several other things to go wrong – referred to as ‘diabetic complications’
• Commonest are heart attacks and strokes; blindness and nerve damage in the feet
NHS England - Yorkshire and the Humber Strategic Clinical Networks
…and amputation is a risk
NHS England - Yorkshire and the Humber Strategic Clinical Networks

…and can cause kidney damage
NHS England - Yorkshire and the Humber Strategic Clinical Networks
HOW COMMON IS IT?
• In Sheffield there are 26,000 people with diabetes
• This makes up about 4.7% of adults • Two main sorts – Type 1 and Type 2: • T1 mainly occurs in children & younger adults
and has to be controlled with insulin • T2 may occur in older people and be more
common in the overweight & inactive
NHS England - Yorkshire and the Humber Strategic Clinical Networks

WHY IS IT IMPORTANT TO US?
• Up to 1 in 4 of our patients in Care Homes may have diabetes and be on treatment
• The same number may have it and we don’t know they have it
• Patients on insulin, and on some tablets like gliclazide, run the risk of blood sugar becoming too low (see later)
NHS England - Yorkshire and the Humber Strategic Clinical Networks

..and it can need lots of pills
NHS England - Yorkshire and the Humber Strategic Clinical Networks

DIFFICULTIES WITH DRUGS
• Patients on insulin, and on some tablets like gliclazide, run the risk of blood sugar becoming too low
• This is more likely to happen if they miss a meal or don’t eat much
• Care-givers need to know correct doses and how to give insulin, unless the patient can do this themselves. District Nurses can advise
NHS England - Yorkshire and the Humber Strategic Clinical Networks
HYPOGLYCEMIA
• Can cause sudden confusion, sweating, faintness, aggression, slurring of speech
• Can cause few or no symptoms • More likely on insulin or medication (but
metformin doesn’t cause hypos) • Be aware of early signs or if the patient is at
risk, eg on these meds and not eaten • Act: drink with sugar, followed by meal
NHS England - Yorkshire and the Humber Strategic Clinical Networks

IT’S A BALANCE -
• Between controlling the sugar and at the same time having a nice quality of life
• In the elderly, tight control is not necessary, but quality of life is
• The elderly are more likely to get low blood sugar at times and have falls as a result
NHS England - Yorkshire and the Humber Strategic Clinical Networks

…there is hope…
NHS England - Yorkshire and the Humber Strategic Clinical Networks

THINGS WE CAN DO
• Diagnosing diabetes early – be ‘Diabetes Aware’
• Control the blood sugar using medication – but not too tightly
• Regular Home checks on feet & shoes • Regular checks done by the GP or Nurse, eye
examination every year at certain centres (not by Optician)
NHS England - Yorkshire and the Humber Strategic Clinical Networks

Presentation 2
NHS England - Yorkshire and the Humber Strategic Clinical Networks

Diabetic Foot and the role of the podiatrist
Debora Sanger Maria Haley
Common Cause for hospital bed occupancy Since 1996 the number of diagnosed diabetics has risen from 1.4million to 2.9 million, half of these people will develop some degree of nerve damage. Of those 2.9 million there is a 1 in 4 chance to develop a foot ulcer, half of those who have an ulcer will get an infection & 20% of infections lead to some form of amputation.














Presentation 3
NHS England - Yorkshire and the Humber Strategic Clinical Networks
Dietary advice for Care Home Residents with Diabetes
Pauline Cowling Specialist Diabetes Dietitian
Aims of care for residents with diabetes in care homes
• To maintain a good quality of life and wellbeing • To provide sufficient support and opportunity to
allow residents to manage their own diabetes where this is feasible
• Achieve an optimum level of blood glucose control which avoids hyperglycaemia and reduces the risk of hypoglycaemia for those residents on insulin or other diabetes medications.
• Provide a well balanced diet which is nutritionally complete and maintains body weight

Nutritional Guidelines for Care Homes
• Under nutrition is a common problem • Dietary recommendations for people with
diabetes may not be appropriate for all people in care homes
• Additional considerations, patients may be underweight and many have low vitamin D levels.
• Calcium, iron and vitamin C can be low.

Practical Guidelines
• Eat 3 meals evenly spaced over the day this will help blood glucose control.
• Have a starchy food at each meal, including some high fibre foods may help with problems such as constipation.
• Include a wide range of fruit and vegetables • Include beans and lentils if possible • Cutting down on fat can help with weight
management only in those patients who are overweight.

Managing Hypoglycaemia
• Timings of meals in relation to timing of medications
• Ensure that carbohydrate foods are eaten at all meals
• Snacks may be needed especially for someone with a poor appetite who struggles to finish a meal
• May need to review diabetes medications

Practical Guidelines
• Limit sugar and sugary foods but you don’t need a sugar free diet. Sugar can be included in foods and baking as part of a healthy diet
• Try and include oily fish where possible • There is no need to use diabetic foods • Watch salt intake • Alcohol is fine in moderation. • Encourage hydration, older adults are at particular risk
of dehydration particularly if they are confused as they forget to drink. Use low sugar squash and fizzy drinks
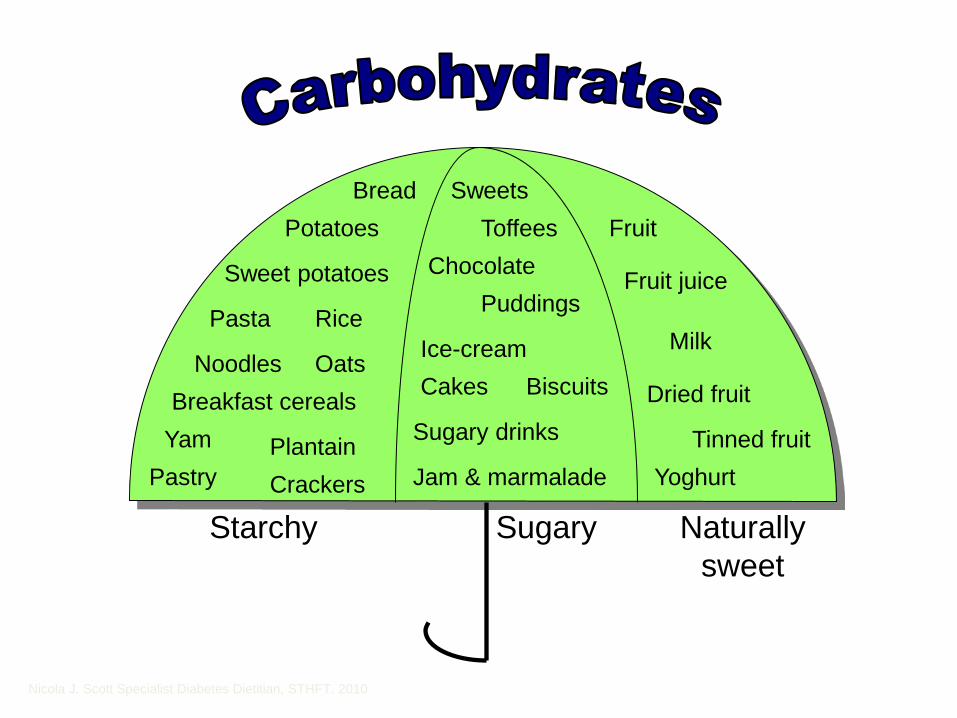
Starchy Sugary Naturally sweet
Bread Potatoes
Rice Pasta
Breakfast cereals Yam Plantain
Pastry Crackers
Sweets
Chocolate
Cakes Biscuits
Sugary drinks
Jam & marmalade
Fruit
Fruit juice
Dried fruit
Milk
Yoghurt
Noodles Oats
Sweet potatoes
Tinned fruit
Toffees
Puddings
Ice-cream
Nicola J. Scott Specialist Diabetes Dietitian, STHFT. 2010
• most vegetables and salads
• diet drinks
• pickles such as pickled onions
• sweeteners
• Meat, fish, cheese, eggs
• Nuts
• Oils, spreading fats
• Cream
• mayonnaise and salad dressings
Foods which do not raise blood glucose levels

What about sugar?
• Generally sugar does not cause a steep rise in blood glucose levels so diabetic products are not needed.
• Sugar is allowed in moderation in the diet of a well controlled non obese diabetic
• Residents can eat foods such as rice pudding, custards and other desserts containing sugar especially if they are under weight and have a small appetite

STEP 1 Similar Carbohydrate Portions What is a portion?
• One third of plate as carbohydrate:
Ways of increasing calories in underweight residents
• Use full fat milk for puddings and custards, drinks etc
• Add butter or margarine to potatoes, consider adding grated cheese
• Add cream to soups or on tinned fruit • Consider peanut butter on toast • Crumpets, fruit loaf, cheese and biscuits, full
fat yoghurt are all suitable snacks
Ways of increasing calories in underweight residents
• Milky drinks such as Horlicks, Ovaltine or drinking chocolate are suitable or a glass of milk instead of tea or coffee
• Consider the use of supplements such as Build up or Complan
• Supplements prescribed by the GP may also be appropriate such as Fortisip for example
• Medications may need to be reviewed.
Summary
• Weigh clients regularly to ensure they are gaining weight if they need to.
• Encourage snacks if someone has a small appetite.
• General diabetes guidelines for diet may not be appropriate with this group of clients.
• For overweight clients weight maintenance may be the most appropriate goal.
• Don’t forget the fluid!
Presentation 4
NHS England - Yorkshire and the Humber Strategic Clinical Networks
Medicines associated with the control of Diabetes mellitus
Ian Hutchison, Medicines Management Pharmacist Joy Smith, Medicines Standards Officer, Care Homes
http://www.youtube.com/watch?v=8NPzLBSBzPI
Sheffield CCG
Presenter
Presentation Notes
http://www.youtube.com/watch?v=8NPzLBSBzPI

• Glycaemic control e.g. orals, insulin • Blood pressure control • Lipid management • Neuropathic pain • Vascular disease • Depression
Common types of medication in diabetic patients

Oral Hypoglycaemic Agents I • Metformin
• Reduces glucose production and increases peripheral utilisation of glucose (only effective in type-2 diabetes)
• Often first choice oral, particularly in obese patients • Start with low doses and build up gradually • Common side effects are mainly GI e.g. initial diarrhoea • Monitor renal and liver function
• Sulfonylureas (SFU)
• Act mainly by augmenting insulin secretion • Useful in non-obese patients and/or in addition or instead of
metformin • Associated with hypoglycaemia, particularly with high doses
and/or missed meals
Oral Hypoglycaemic Agents II
• Pioglitazone • Reduces peripheral insulin resistance • Used alone or with metformin and/or a SFU or with insulin • Issues with heart failure, fractures and bladder pathology, etc
• DDP-4 Inhibitors (Gliptins)
• Moderate efficacy and reasonably well tolerated
• GLP-1 Agonists (Exenatide, etc) • Given by s/cut injection and benefits around weight loss
• SGLT2s (Gliflozins) • Reduce glucose reabsorption but genito-urinary side effects
Insulins
• Required in all type-1s and type-2s where other methods have failed to achieve good control
• Types include short-acting, intermediate and long-acting • Short-acting insulins include soluble and rapid-acting
insulin • Intermediate insulins include isophane insulin • Long-acting insulins include insulin detemir and glargine • Insulin therapy needs to be individualised and can be
given via a number of regimes e.g. basal insulin, mixed insulin or basal-bolus combinations
• Many insulins come in convenient pen devices

Complications
• Most important acute complication is hypoglycaemia • Most closely associated with insulin and SFU treatment • Use glucose to reverse symptoms e.g. sugar, drinks,
snacks and/or prescribable gels such as GlucoGel • In an emergency, use glucagon injection
Do you and the patient (if appropriate) know how to recognise and treat a ‘hypo’??

Monitoring
• Main measure of chronic control of blood glucose is via the HbA1c test
• This should be measured around 3-6 monthly • Each patient should have a documented long term
target • Some patients may benefit from the use of a blood
glucose monitoring device (meter and strip) but this should be clearly recorded in the patient’s care plan
• Consideration should be given to whether type-1 diabetics need to have the ability to measure blood ketones

• Printed times/ time of day on MAR charts • Use of the reverse of the MAR chart • Advice labels
MAR charts – meeting the need

• Ordinary release tablets • Modified release tablets • Sachets • Liquids
• Combination products
Formulations of oral antidiabetic drugs
Presenter
Presentation Notes
• What is the drug for? • Reason for dose being
missed • Consequence of missed
dose
• Individual care plan to manage what to do in the event of a missed dose
Missed doses
Summary • Aim of medication to treat diabetes (glucose) is to
achieve the optimum level of metabolic control i.e. prevent hyperglycaemia and avoid hypos (watch in patients prescribed insulin and/or SFU)
• Care should be reviewed regularly and individualised allowing easy access to specialist care
• Does your home have a policy/guidance on the care of patients with diabetes?
• The importance of effective recording and reporting • Do you need to improve your knowledge of diabetes
and how to contribute to better care?
Presenter
Presentation Notes

• Mary - type 2 diabetic - on oral hypoglycaemic agents and insulin
• Mrs Patel – type 2 diabetic – on oral hypoglycaemic agents, also had a stroke
Scenarios