DEVELOPING ANALOGUE/SUBTITUTE FOR THE …bds007.yolasite.com/resources/3-DEVELOPING ANALOGUE...
30
DEVELOPING ANALOGUE/SUBTITUTE FOR THE MANDIBULAR DENTURE BEARING AREA Dr Muhammad Rizwan Memon FCPS Assistant Professor
Transcript of DEVELOPING ANALOGUE/SUBTITUTE FOR THE …bds007.yolasite.com/resources/3-DEVELOPING ANALOGUE...
DEVELOPING ANALOGUE/SUBTITUTE FOR THE MANDIBULAR DENTURE BEARING
AREA
Dr Muhammad Rizwan Memon FCPS
Assistant Professor

Crest of Residual Ridge Buccal Shelf Shape of supporting structure Mylohyoid Ridge Mental foramen Genial tubercles Torus Mandibularis

Mucous membrane covering ridge is similar to that of the upper in healthy mouth.
Underlying bone is cancellous, therefore, the crest of the residual ridge may be not favorable as a primary stress bearing area

It is bounded medially by crest of ridge, laterally by external oblique ridge, anteriorly by buccal frenum and distally by retromolar pad.
Bone of the buccal shelf area is covered by a layer of cortical plate and shelf area lies at right angle to the vertical occlusal forces, makes it the most suitable primary stress bearing area.

The maxilla resorb upward and inward to become smaller b/c of direction & inclination of roots of teeth & alveolar process and opposite is true for mandible which become wider with age and gives patient progenathic appearance

Following the extraction of natural teeth and subsequent resorption, the mylohyoid ridge becomes more prominent. This can result in mucosal soreness beneath the denture bearing area over the mylohyoid ridge, unless relief is provided in denture base

It may become prominent with ridge resorption and produce numbness by compressing nerves & blood vessels unless relief is provided

With resorption of ridge genial tubercles may become prominent

Often found bilaterally below 1st & 2nd Premolar area and require surgical removal to avoid breaking of border seal

Labial Vestibule Buccal Vestibule Distal Extension Lingual Border Mylohyoid Muscle Retromylohyoid fossa Sublingual gland region Alveololingual sulcus

It runs from buccal frenum to buccal frenum on other side
Length & thickness of labial flange very with amount of tissue has lost
If flange is thick in this region, the denture will be displaced by stretching of Orbicularis Oris muscle when mouth is opened wide

Extent of Buccal vestibule is influenced by Buccinator muscle
The External oblique ridge does not govern the extension of the buccal flange because the resistance or lack of encountered in this region varies widely. The buccal flange may extend to the external oblique ridge, up onto it or even over it depending on the location of the mucobuccal fold.

The retro molar pad is a triangular soft pad of
tissue. Its mucosa is composed of thin non keratinized epithelium. Its submucosa contains Glandular tissues Fibers of the buccinator and superior constrictor
muscles Pterygo mandibular raphe Fibers of the temporalis muscle
Action of these muscles limit the extent of denture,& prevents placement of extra pressure on distal part of pad during impression, The anterior section is usually firm and fibrous. It is important for denture support and preventing distal denture displacement therefore the denture base should only extend to one half to two third the retro molar pad

Lingual tissues under the tongue exhibits less direct resistance & distorted easily when impression is being made, that will result in tissue soreness & denture dislodgement by tongue, To avoid this, action of Mylohyoid must be understood
It is a thin sheet of fibers and in a relaxed state will not resist the impression material.
Carrying the border under the mylohyoid cannot be tolerated. The contraction of this muscle will displace the denture.
Lingual Flange must be made parallel to the mylohyoid muscle when it contracts

In the retro mylohyoid fossa the border of the denture move back toward the body of the mandible producing the S curve of the lingual flange.
Protrusion of tongue causes retromylohyoid curtain to move forward that will determine the posterior extension of denture
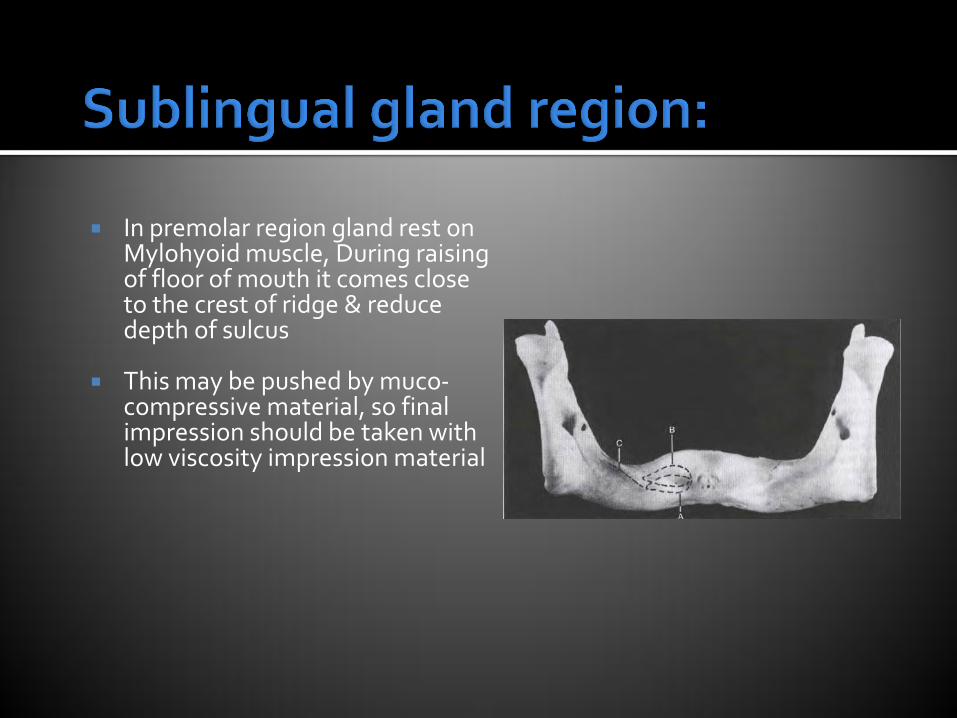
In premolar region gland rest on Mylohyoid muscle, During raising of floor of mouth it comes close to the crest of ridge & reduce depth of sulcus
This may be pushed by muco-compressive material, so final impression should be taken with low viscosity impression material

Examination & conditioning of pt: Selection of impression material Selection of impression tray Seating of pt: Making the preliminary impression Constructing the primary cast Fabrication of primary tray Border molding Diagnostic impression Final impression

Chair position for mandibular impression:
Pt: jaw should be at or above the operator elbow level
Operator should stand in front of the pt:

Objective is to obtain slightly over extended impression around the borders
Tray should be moistened with water before trying it in mouth so as to reduce the friction with lips and oral mucosa
Sides of properly fitted tray should avoid direct contact with the buccal, labial & lingual surfaces of teeth by approximate 5mm
Mandibular tray should extend to include the retromolar pads
Any area of under extension of tray is corrected with boxing wax and entire border of tray is lined with boxing wax to create rim
Tray Selection:

Patient is asked to open mouth halfway
The tray is inserted sideways into the mouth
With a rotary motion it is lined up with the area to be registered, with the tray handle approximately parallel to the occlusal plane and in line with the midline
Patient is instructed to lift the tongue and close his mouth slightly
Tray is seated gently by alternating pressure from an index finger in 1st molar region
When the tray is seated the borders of impression are molded
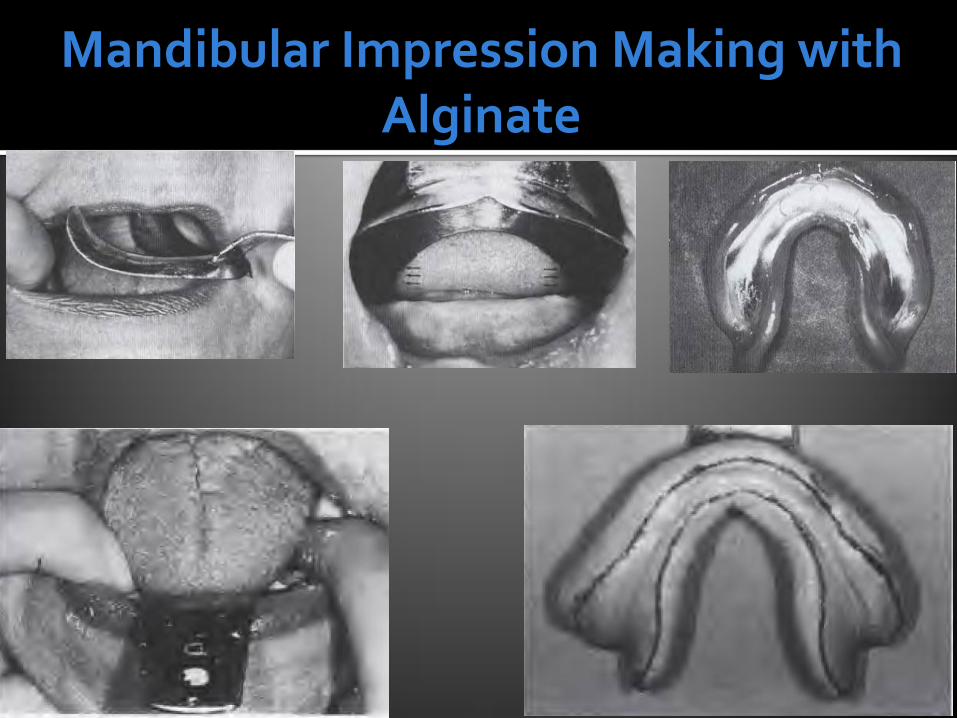
Mandibular Impression Making with Alginate

Constructing Custom Tray
A wax spacer 1mm thick is placed over crest & slopes of residual ridges except borders and buccal shelf area so tray contacts in this region for selective pressure and positioning of tray One anterior handle is placed to carry tray in mouth and two posterior handles are used as finger rest for placement & stabilization of tray in correct position
Two ways; 1. In one step (Reduce no of insertion of tray and
chances of errors created in one step affect another contour)
2. Segment by segment
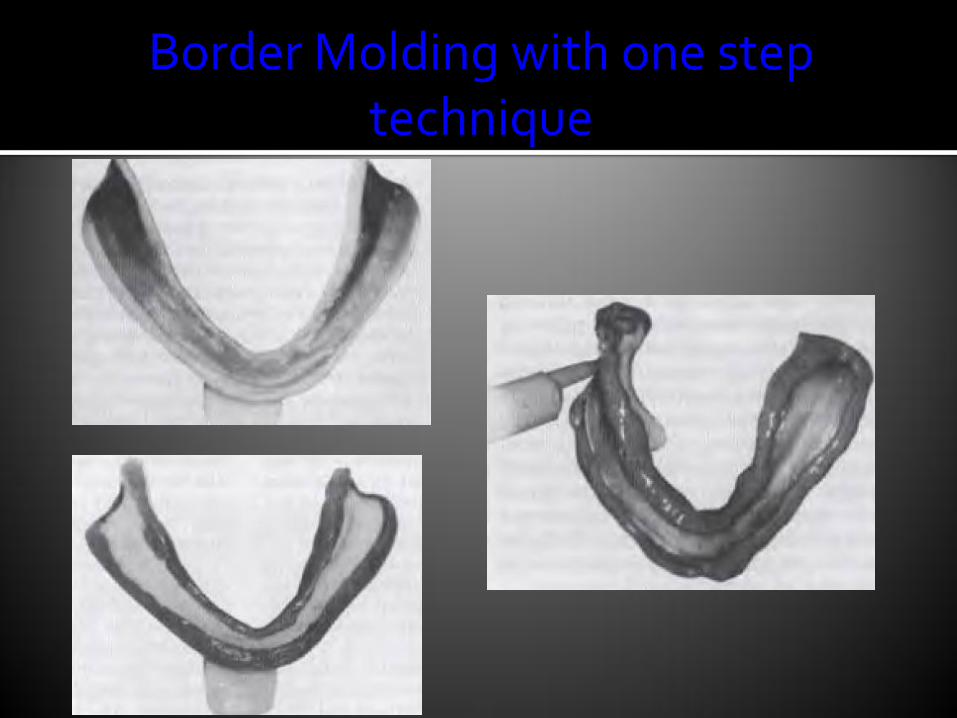
Border Molding with one step technique
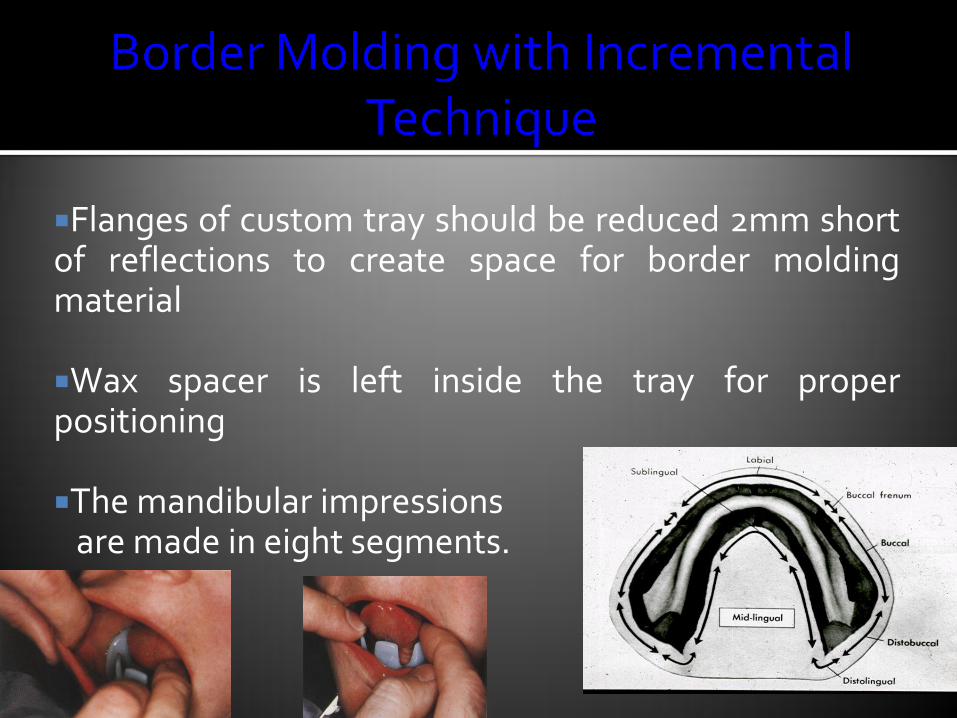
Flanges of custom tray should be reduced 2mm short of reflections to create space for border molding material
Wax spacer is left inside the tray for proper positioning
The mandibular impressions are made in eight segments.
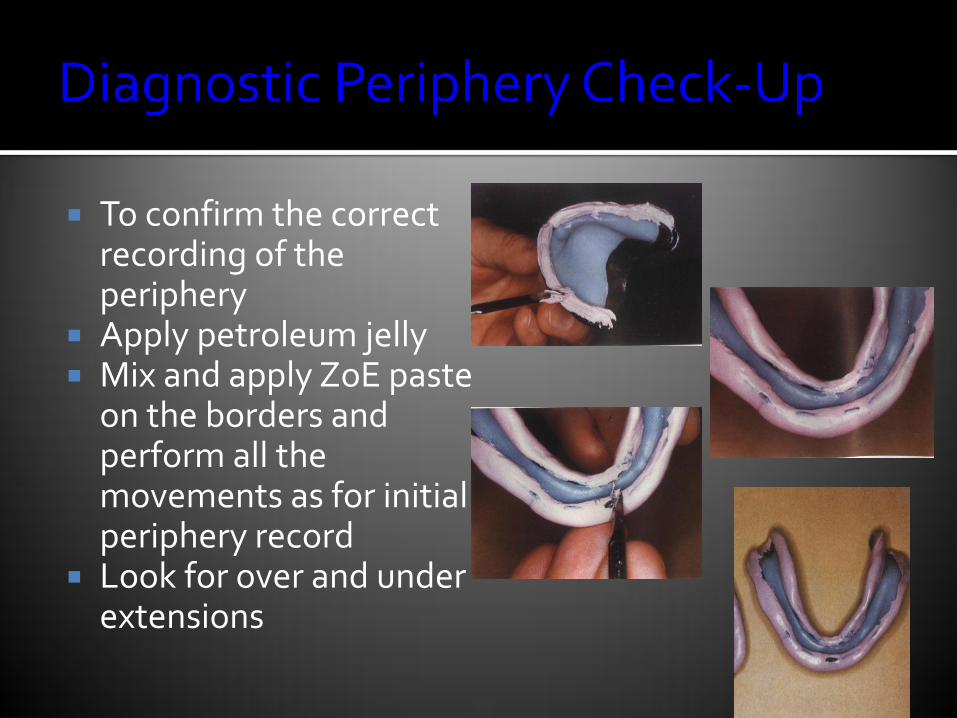
To confirm the correct recording of the periphery
Apply petroleum jelly Mix and apply ZoE paste
on the borders and perform all the movements as for initial periphery record
Look for over and under extensions
0.5 mm of border molding material is removed to create space for final impression material
Spacer wax if present is removed from inside the tray

Mix material in proper ratio and paint a thin layer on whole surface of tray including the periphery
Seat first anterior then posterior After one minute border mold (first anterior
then posterior) Ask the patient to perform the tongue movements Remove after 3-4 minutes

Boxing impression and Making Cast