Dasar Dasar Interpretasi Ekg Radityo Prakoso Hary s Muliawan

of 69
-
Upload
achieve-saifulhayat -
Category
Documents
-
view
74 -
download
6
Transcript of Dasar Dasar Interpretasi Ekg Radityo Prakoso Hary s Muliawan
-
DASAR-DASAR
INTERPRETASI EKG
Radityo Prakoso, Hary S Muliawan
Department of Cardiology and Vascular Medicine
Faculty of Medicine University of Indonesia
National Cardiovascular Center Harapan Kita
-
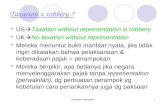
V6V5
V4V3
V2V1
V6RV5R
V4RV3R
Midclavicular line
Anterior axillary line
Midaxillary line
Unipolar Precodial (Chest) Leads
Mervin J. Goldman, MD. 11th edition Principles of clinical Electrocardiography. Clinical Professor of Medicine University of California School of Medicine San Francisco @1995-1982
-
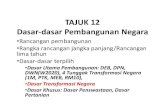
V7 V8 V9 V9RV8RV7R
Horizontal plane of V4-6
Unipolar Precodial (Chest) Leads
Mervin J. Goldman, MD. 11th edition Principles of clinical Electrocardiography. Clinical Professor of Medicine University of California School of Medicine San Francisco @1995-1982
-
ECG INTERPRETATION
1. RATE
2. RHYTHM
3. AXIS
4. HIPERTROPHIC SIGNS
5. MYOCARDIAL INFARCTION
6. ARRHYTHMIA
-
1. RATE
Normal heart rate : 60 100 x/minutes > 100 x/minutes : Sinus Tachycardia < 60 x/minutes : Sinus Bradicardia
Determination heart rate (normal paper speed 25 mm/s):
300
Count number of large square (bold boxes in one R R interval)
1500
Count number of small square in one R R intervals
Number of QRS complex in 6 seconds, multiply by 10
-
2. RHYTHM
Normal cardiac rhythm : SINUS rhythm
Sinus rhythm characteristics :
Rate 60-100 bpm Constant R R interval Negative P wave in aVR and positive di II P wave is always followed by QRS complex
-
12
Gelombang P
-
3. AXIS
-
Determining Axis: An Example
-
4. HYPERTROPHIC SIGNS
-
Atrial Hypertrophy
-
Atrial Hypertrophy
P Pulmonale: Right (RAH)
P Mitrale: Left (LAH)
-
5. MYOCARDIAL INFARCTION
Ischemia
Injury
Necrosis
-
ANTERIOR INFARCTION
-
INFERIOR INFARCTION
-
POSTEROLATERAL INFARCTION
-
ARRHYTHMIA
-
Causes of Cardiac Arrhythmias
Disturbed automaticity : this may involved a speeding up or
slowing down of areas of automaticity such as the sinus
node, the atrioventricular (AV) node, or the myocardium.
Abnormal beats (depolarizations) may arise through this
mechanism from the atria, the AV junction, or the ventricles.
Disturbed conduction : conduction may be either too rapid (as
in Wolff- Parkinson-White syndrome) or too slow (as in AV
block)
Combinations of disturbed automaticity and disturbed
conduction
-
Sinus Rhythm
-
First Degree Heart Block
-
Second Degree Block Type I
*
-
Second Degree Block Type II
-
Third Degree Heart Block
-
Premature Atrial Contraction
*
-
Premature Ventricular
Contraction
-
Atrial Fibrillation
-
Atrial Flutter
-
Supraventricular Tachycardia
-
Ventricular Fibrillation
-
Ventricular Tachycardia
-
Torsade de Pointes
-
Bundle Branch Blocks
Characteristic QRS
pattern in lead I, V1,
and V6
-
Left Bundle Branch Block
*
-
Right Bundle Branch Block
*
-
DISCUSSION
-
Sinus arrhythmia
-
Limb lead reversal
-
Early repolarization
-
Subendocardial ischemia.
Anterolateral ST-segment depression
-
Unstable angina
-
acute anterolateral myocardial infarction
-
High lateral infarction
-
Lateral myocardial infarction
-
Right ventricular infarction
-
Acute inferoposterior myocardial infarction
-
left ventricular aneurysm
-
Mobitz I
-
High-grade atrioventricular block
-
Wolff-Parkinson-White syndrome
-
Wolff-Parkinson-White syndrome
-
Atrial fibrillation
-
Atrial flutter
-
premature ventricular contraction
-
Supraventricular tachycardia
-
Wide complex tachycardia
-
Ventricular flutter
-
Idioventricular rhythm