Consistent relationship between selenium and apolipoprotein A-II concentrations in the sera of...
10
GCopyright1995by Humana Press Inc. All rights of any nature whatsoeverreserved. 0163-4984/95/5001-0033 $06.00 Consistent Relationship Between Selenium and Apolipoprotein A-II Concentrations in the Sera of Fasting Middle-Aged Male Abstainers and Regular Consumers of Alcohol HIROSHI KOYAMA,* CHIHO WATANABE, 1 HIROSHI SATOH, 1 HIROAKI HOSOKAI, 2 AND SHIZUO TAMURA 2 'Department of Environmental Health Sciences, Tohoku University School of Medicine, Sendai, Japan; and 2NTT Tokyo Health Care Center, Tokyo, Japan Received June 17, 1994; Accepted August 19, 1994 ABSTRACT Several studies have suggested that selenium serum levels may be associated with serum lipids and apolipoproteins. In the present study, 99 clerical workers aged 40-49 yr were selected based on their drinking and smoking habits. The serum concentration of selenium was not affected by these lifestyle factors. The regular drinkers had raised serum high-density lipoprotein cholesterol, apo A-I, and apo A-II concentrations. Correlation analysis showed that serum selenium was positively and consistently associated with apo A-II regardless of alcohol consumption. Factor analysis revealed that serum selenium had no association with factors that represented each lipoprotein frac- tion (LDL, HDL, and VLDL). The present study indicates that serum selenium is positively correlated only with apo A-II levels. Index Entries: Selenium; apolipoprotein A-I; apolipoprotein A-II; lipids; HDL cholesterol; alcohol; smoking. INTRODUCTION Selenium is an essential trace element (1). Its role as an antioxidant and selenium-related diseases have been identified (2). Despite signifi- cant advances in the field of selenium research (3,4), the biological func- tions of selenium are still largely unknown. *Author to whom all correspondence and reprint requests should be addressed. Biological Trace Element Research 33 Vol. 50, 1995
-
Upload
hiroshi-koyama -
Category
Documents
-
view
212 -
download
0
Transcript of Consistent relationship between selenium and apolipoprotein A-II concentrations in the sera of...

GCopyright 1995 by Humana Press Inc. All rights of any nature whatsoever reserved. 0163-4984/95/5001-0033 $06.00
Consistent Relationship Between Selenium and Apolipoprotein A-II
Concentrations in the Sera of Fasting Middle-Aged Male Abstainers
and Regular Consumers of Alcohol HIROSHI KOYAMA,* CHIHO WATANABE, 1 HIROSHI SATOH, 1
HIROAKI HOSOKAI, 2 AND SHIZUO TAMURA 2
'Department of Environmental Health Sciences, Tohoku University School of Medicine, Sendai, Japan; and 2NTT Tokyo
Health Care Center, Tokyo, Japan Received June 17, 1994; Accepted August 19, 1994
ABSTRACT
Several studies have suggested that selenium serum levels may be associated with serum lipids and apolipoproteins. In the present study, 99 clerical workers aged 40-49 yr were selected based on their drinking and smoking habits. The serum concentration of selenium was not affected by these lifestyle factors. The regular drinkers had raised serum high-density lipoprotein cholesterol, apo A-I, and apo A-II concentrations. Correlation analysis showed that serum selenium was positively and consistently associated with apo A-II regardless of alcohol consumption. Factor analysis revealed that serum selenium had no association with factors that represented each lipoprotein frac- tion (LDL, HDL, and VLDL). The present study indicates that serum selenium is positively correlated only with apo A-II levels.
Index Entries: Selenium; apolipoprotein A-I; apolipoprotein A-II; lipids; HDL cholesterol; alcohol; smoking.
INTRODUCTION
Selenium is an essential trace e lement (1). Its role as an antioxidant and selenium-related diseases have been identified (2). Despite signifi- cant advances in the field of se lenium research (3,4), the biological func- tions of se lenium are still largely unknown .
*Author to whom all correspondence and reprint requests should be addressed.
Biological Trace Element Research 33 Vol. 50, 1995

34 Koyama et al.
Previously it was reported that a low concentration of selenium in blood plasma was a risk factor for coronary heart disease (CHD) in east- ern Finland (5). The serum concentration of selenium correlated positively with high-density lipoprotein (HDL) cholesterol (6), which is a well-estab- lished protective factor against CHD (7). This correlation of serum sele- nium with the HDL cholesterol concentration seems to be one plausible mechanism whereby selenium deficiency increases the risk for CHD (6).
However, studies conducted in other areas showed inconsistent results (8-11). Jossa et al. (11) found serum selenium correlated positively with total cholesterol, but not with HDL cholesterol in southern Italy. Bukkens et al. (10) reported that serum selenium was related with nei- ther total cholesterol nor ~DL cholesterol in the Netherlands. Deguchi and Ogata (9) also failed to find a correlation between selenium and HDL cholesterol, but found a positive correlation between selenium and total cholesterol in Japanese male nondrinkers.
Different blood sampling conditions, fasting, or postprandial may cause conflicting results. The results from casual blood sampling (9,10) failed to demonstrate a positive relationship between serum selenium and HDL cholesterol concentrations. Furthermore, several lifestyle fac- tors, such as habitual alcohol drinking (12-14), smoking (10), physical exercise (15), and subject age (16), are reported to influence the serum concentration of selenium. These factors also modify the concentrations of serum lipids (17-19) and apolipoproteins (20-22).
In the present study, the association of serum selenium with serum lipids and apolipoproteins is assessed among middle-aged clerical male workers. To minimize the conflicting factors mentioned above, blood samples were taken only after overnight fasting. The effects of habitual alcohol drinking and smoking on the concentrations of selenium, lipids, and apolipoproteins and on the associations among them are evaluated, including serum activity of 7-glutamyl transpeptidase (7-GTP), a biologi- cal marker of alcohol consumption (23).
SUBJECTS AND METHODS
Participants in the present study were middle-aged male office work- ers in a telephone company in Tokyo. Blood sampling and a questionnaire survey on the frequency of drinking, number of drinks per time, number of cigarets smoked per day, and frequency of leisure-time physical exercise were completed for 536 persons in autumn 1990. These procedures and measurement of serum lipids were conducted as part of an annual physi- cal examination. Informed consent was obtained from each subject for the additional trace element measurement. This study was approved by the Ethics Committee of Tohoku University School of Medicine.
From 536 candidates, those taking any medications, those performing regular physical exercise, and those who were extremely obese (BMI of 27
Biological Trace Element Research Vol. 50, 1995
Selenium and Apolipoprotein A-II 35
and more) or thin (BMI of 18 or less) were excluded, and 297 middle-aged males (40-49 yr) were selected to minimize possible conflicting influences. Finally 99 persons were selected for the present study considering the combination of two lifestyle factors, i.e., drinking and smoking habits, and four groups were established: Group 1 (n = 25)--those with neither drink- ing or smoking habits; Group 2 (n = 25)--those who only smoked (20 cig- arets/d and more); Group 3 (n = 18)--those who only drank (6 times or more/wk); and Group 4 (n = 31)--those with both smoking (20 cigarets/d and more) and drinking (6 times or more/wk) habits.
After overnight fasting, blood samples were collected at a fixed time of day, approximately at 9-11 AM, to minimize possible diurnal variation. Serum samples were analyzed for 7-GTP activity with an automatic ana- lyzer (Type 736, Hitachi, Tokyo). Total cholesterol and triglycerides were determined enzymatically using Clinimate CHO and TG2 commercial kits (Daiichi Pure Chemicals Co., Tokyo), respectively. Serum HDL cho- lesterol was also determined enzymatically after precipitation of lipopro- teins containing apo B by the phosphotungstic acid magnesium chloride method (Drychem slide, HDL-C-P, Fuji Film Co., Tokyo). Concentrations of serum apolipoproteins A-I, A-II, and B were measured by immuno- turbidimetry using monospecific 7 globulins (Apo Auto-2-Daiichi, Dai- ichi Pure Chemicals Co., Tokyo). The low-density lipoprotein (LDL) cholesterol level was estimated with the formula of Friedewald (24). The ratio of HDL cholesterol to total cholesterol (%HDL-C) was calculated.
Aliquots of serum samples preserved at -70~ were digested with concentrated nitric acid and perchloric acid (metal analysis grade, Wako Pure Chemical Ind., Osaka) on a hot plate at about 140~ for 4 h and finally at 190~ to vaporize nitric acid completely. A fluorometric method with 2,3-diaminonaphthalene (25) was used to analyze selenium with a spectro-fluorometer (Type 821-FP; Japan Spectroscopic Co., Ltd., Tokyo). The accuracy of selenium determination was assured with an NIST stan- dard reference material (No. 1577a, bovine liver; National Institute of Standards and Technology, Gaithersburg, MD) carried through the entire procedure. The recovery of the standard (0.71 ~tg/g) was 101.0%, and the coefficient of variation was 4.4%.
Body mass index (BMI) was calculated using weight in kilograms divided by the square of height in meters. Logarithmic transformation of serum TG and 7-GTP levels and arc sine transformation of %HDL-C were performed for statistical analysis. One-way analysis of variance (ANOVA) was applied to assess the differences of serum concentrations of lipids, apolipoproteins, and selenium among the groups. When ANOVA showed a significant difference, multiple-comparison analysis was carried out by Dunnett's method taking Group 1 as a control. Pear- son's correlation analysis was conducted to assess the relationship of serum selenium with serum lipids and apolipoproteins. Finally, principal factor analysis followed by varimax rotation was performed separately on the abstainers and alcohol consumers. These analyses were performed
Biological Trace Element Research Vol. 50, 1995

36 Koyama et al.
Table 1 Characteristics of the Participants by Smoking Habits and Alcohol Consumption
Group 1 (n=25) Group 2 (n=25) Group 3 (n=l 8) Group 4 (n=31 )
Age (years) 44.2 + 2.7 45.0 + 2.2 43.5 + 2.4 42.8 + 2.7
Body massindex 23.0 + 2.3 22.8 _ 1.9 23.6 _+ 2.0 22.9 + 2.4
Alcohol (drinks#/time) - - 2.2 + 0.9 2.3 + 0.9
Smoking (cigarettes/day) - 27.7 + 13.1 - 25.2 • 11.5
Group 1: those with neither drinking nor smoking habits; Group 2: those with only smoking habits (20 cigares/d and more); Group 3: those with only drinking habits (6 times or more/wk); Group 4: those with both smoking and drinking habits; # One drink, such as a bottle of beer or a cup of sake, contains approx 30 g of alcohol.
with NAP (26), a statistical package for personal computers (PC-9800 series, NEC Co., Tokyo).
RESULTS
Characteristics of the study participants are shown in Table 1. Age and BMI were not significantly different among the groups. The average numbers of drinks per time in Groups 3 and 4 did not significantly dif- fer. The mean numbers of cigarets smoked per day in Groups 2 and 4 were not significantly different.
Serum concentrations of lipids, apolipoproteins, 7-GTP, and selenium are shown in Table 2. Apos A-I, A-II, and also 7-GTP were significantly higher in drinking groups than in abstainers. HDL cholesterol and %HDL- C were also elevated in drinking groups, and a significant increase was observed in %HDL-C of Group 4. Serum concentrations of selenium were not significantly different among the groups. The levels of total cholesterol and apo B showed similar values among the groups. Smoking habits had no effect on the lipids, apolipoproteins, or selenium levels. The following analyses were conducted on combined Groups 1 and 2 vs 3 and 4.
Correlation matrices of the all variables considered in the present study are shown in Table 3. Serum selenium positively correlated with apo A-II and 7-GTP in abstainers. In the regular drinkers, serum sele- nium positively correlated with apo A-II, but not with 7-GTP. The num- ber of alcoholic drinks per time was positively associated with 7-GTP.
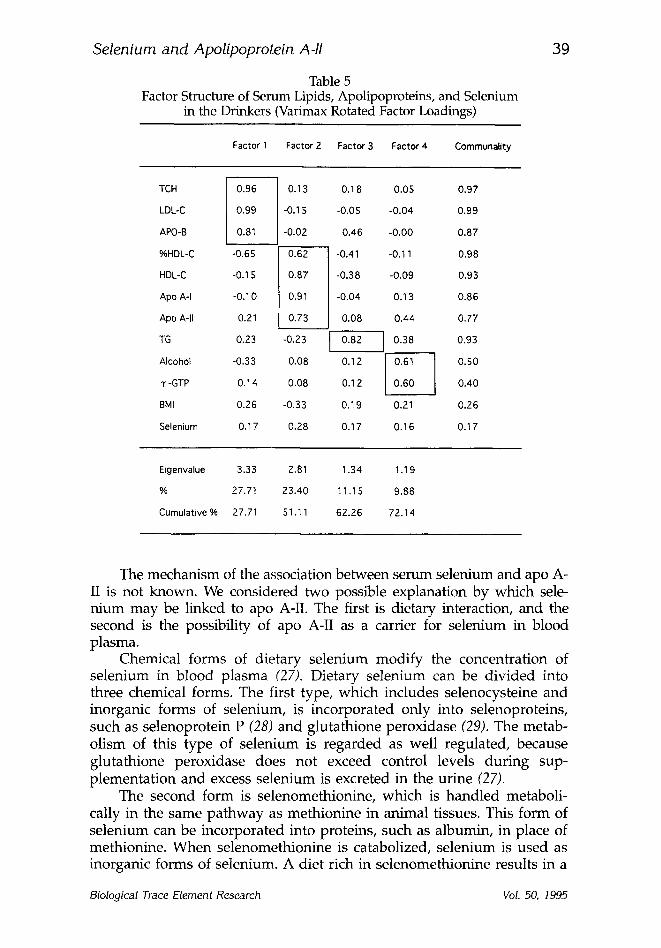
Principal factor analysis using varimax rotation was carried out sep- arately for abstainers and regular alcohol consumers. The results are summarized in Tables 4 and 5. In each group four factors, which had eigen values of > 1.0, were extracted. These four factors accounted for 73 and 72% of the total variance in the observed variables, respectively. For the first to third factors, both groups of abstainers and drinkers exhibited similar factor structures. These factors are considered to represent LDL,
Biological Trace Element Research Vol. 50, 1995

Selenium and Apolipoprotein A-II
Table 2 Serum Concentrations of Lipids, Apolipoproteins, and Selenium of the Participants by Smoking Habits and Alcohol Consumption
37
Group 1 (n=25) Group 2 (n=25) Group 3 (n=l 8) Group 4 (n=31)
TCH(mmol/L) 5.69 + 0.93 5.60 + 0.85 5.70 + 1.15 5.09 + 0.93
LDL-C (mmol/L) 3.92 + 0.80 3.80 + 0.81 3.69 + 1.08 3.00 + 0.92*
HDL-C(mmpl/L) 1.19 + 0,26 1.14 + 0.23 1.28 + 0.31 1.33 + 0.40
%HDL-C(%) 21.1 • 0.3 20.6 • 0.4 23.1 • 0.9 26.6 • 1.1"
TG(mmol/L)@ 1.15 (1.53) 1.32 (1.51) 1,50 (1.43) 1.42(1.73)
ApoA-I(g/L) 1.28 + 0,20 1,26 • 0.16 1.45 • 0.21" 1.46 • 0.24*
ApoA-II(g/L) 0.34 • 0.06 0.33 + 0.06 0.40+0.06* 0 . 3 9 • 0.06"
ApoB(g/L) 1.01 + 0,20 0,98 • 0.17 0.99 + 0.23 0.89 + 0.24
T-GTP (U/L)@ 29.7 (1.73) 32.1 (1.72) 58.2 (2.10)* 55.2 (1.75)*
Selenium(#g/L) 141.3 • 142.2 +18.9 135.3 • 147.0 _+ 7,0
@ geometric means and SDs are shown; *p < 0.05, Dunnett's method.
Table 3 Correlation Matrices of the Observed Variables in Abstainers (Upper Triangle)
and Regular Consumers of Alcohol (Bottom Triangle)
TCH TG T -GTP HDL-C %HDL-C LDL-C Apo A-I Apo A-U Apo B BMI Selenium
TCH 0.399** 0.322* 0.179 -0.541"* 0.935** 0.092 0.493** 0,754"* 0.227 0.212
TG 0.375** 0.248 -0.225 -0.500"* 0.195 -0.053 0 . 2 2 1 0,514"* 0.461"* 0.017
"r-GTP 0.208 0.346** 0.320* 0.002 0.165 0.266 0.376** 0.286* 0.249 0.379**
HDL-C -0.090 -0.583** -0.062 0,714"* -0.036 0.765** O.O1S -0.037 -0.264 0.115
%HDL-C -0.618"* -0.675** -0.160 0.818"* -0.667** 0.578* -0.352* -0,568"* -0,429"* -0.066
LDL-C 0.923** 0.207 0.11 -0.26t -0.701"* -0.118 0.478** 0.690** 0.185 0.201
Apo A-I 0.022 -0.210 0.139 0.819"* 0.625** -0.234 0.231 0.054 -0.063 0.153
ApoA-II 0.313" 0.096 0.386** 0.512"* 0.221 0.079 0.718"* 0.613'* 0,375"* 0.431'*
Apo B 0.866** 0.573** 0.180 -0.297" -0.715"* 0.784** -0.115 0.161 0.365** 0.248
BMI 0.243 0.345* 0.115 -0.406"* *0.491"* 0.279 -0.332" -0.086 0.322* -0.083
Selenium 0.205 0.135 0.097 0.119 -0.014 0.104 0.228 0.405** 0.254 0.070
TCH TG 1" -GTP HDL-C %HDL-C LDL-C Apo A-I Apo A-II Apo B BMI Selenium
*p < 0.05, **p < 0.01.
HDL, and VLDL fractions, respectively. The fourth factor in abstainers had relatively high loads of apo A-II and selenium. In drinkers, the fourth factor was associated with alcohol quantity and 7-GTP. Serum selenium had only a low load in each of the four factors in drinkers.
DISCUSSION
The present study, using sera sampled after overnight fasting, did not reveal any relationship between serum concentrations of selenium
Biological Trace Element Research Vol. 50, 1995

38 Koyama et al.
Table 4 Factor Structure of Serum Lipids, Apolipoproteins, and Selenium
in the Nondrinkers (Varimax Rotated Factor Loadings)
Factor 1 Factor 2 Factor 3 Factor 4 Communality
TCH ] 0.94 l 0.12 0.25 0.19 0.99 LDL-C I ~19662 I -0.1 5 0.02 0.21 0.99 APO-B -0.04 0.43 0.37 0.71 HDLC O.10 I 0.97 I -0.20 0.06 0.99 %HDL-C -0.54 1 0.73 i -0.39 -0.12 0.99 Apo A-I -0.05 0.78 0.02 0.24 0.67
TG 0.19 -0.06 I 0.91 I -0.02 0.86
8MI 0.10 -0.17 I 0.54 I 0.19 0.37
Apo A-II 0.33 0.01 0.24 ~ 0.67
Selenium 0.11 0.08 -0.05 I ~i~77 I 0.35
~, -GTP 0.11 0.29 0.27 0.39
Eigenvalue 2.68 2.25 1.69 1.39
96 24.33 20.46 15.36 12.60
Cumulative % 24.33 44.79 60.14 72.75
and HDL cholesterol. Serum selenium positively correlated only with the serum apo A-II concentration. These results confirm those of a previous study conducted in children (8). The association between selenium and apo A-II was not confined to the abstainers, but was also observed in regular consumers of alcohol who had an increased apo A-II concentra- tion. Principal factor analysis revealed that serum selenium was not asso- ciated with the first to third factors, which represented lipoprotein fractions of LDL, HDL, and VLDL, respectively. The results suggested that serum selenium has no association with either serum lipids or apolipoproteins, except for apo A-II.
A recent s tudy showed that the serum concentration of apo A-II increases with BMI in nondrinkers and drinking frequency in regular consumers of alcohol (22). However, it is not likely that BMI and alcohol consumption control the association between apo A-II and selenium. The present study showed that serum selenium was associated with serum apo A-II independent ly from obesity and habitual consumption of alco- hol. Serum selenium was not related to BMI in either group. The num- ber of drinks per time and serum level of 7-GTP had no association with serum selenium in the drinking group.
Biological Trace Element Research Vol. 50, 1995
Selenium and Apolipoprotein A-II
Table 5 Factor Structure of Serum Lipids, Apolipoproteins, and Selenium
in the Drinkers (Varimax Rotated Factor Loadings)
39
Factor 1 Factor 2 Factor 3 Factor 4 Communality
TCH
LDL-C
APO-B
%HDL-C
HDL-C
Apo A-I
Apo A-II
TG
Alcohol
T -GTP
BMI
Selenium
0.13 0.18 0.05 0.97
-0.15 -0.05 -0.04 0.99
-0.02 0.46 -0.00 0.87
-0,65 ~ -0.41 -0.11 0.98 /
-0.1S I 0.87 -0.38 -0.09 0.93 I
-0.10 I 0.91 -0.04 0.13 0.86 I
0.21 I 0.73 0.08 0.44 0.77 i
0.23 -0.23 0.82 I 0.38 0.93 I
-0.33 0.08 0.12 ~ 0.50
0.14 0.08 0.12 I 0.60 I 0.40
0.26 -0.33 0.19 0.21 0.26
0.17 0.28 0.17 0.16 0.17
Eigenvalue 3.33 2.81 1.34 1.19
% 27.7t 23.40 11.15 9.88
Cumulative % 27.71 51,11 62.26 72.14
The mechanism of the association between serum selenium and apo A- II is not known. We considered two possible explanation by which sele- nium may be linked to apo A-II. The first is dietary interaction, and the second is the possibility of apo A-II as a carrier for selenium in blood plasma.
Chemical forms of dietary selenium modify the concentration of selenium in blood plasma (27). Dietary selenium can be divided into three chemical forms. The first type, which includes selenocysteine and inorganic forms of selenium, is incorporated only into selenoproteins, such as selenoprotein P (28) and glutathione peroxidase (29). The metab- olism of this type of selenium is regarded as well regulated, because glutathione peroxidase does not exceed control levels during sup- plementation and excess selenium is excreted in the urine (27).
The second form is selenomethionine, which is handled metaboli- cally in the same pathway as methionine in animal tissues. This form of selenium can be incorporated into proteins, such as albumin, in place of methionine. When selenomethionine is catabolized, selenium is used as inorganic forms of selenium. A diet rich in selenomethionine results in a
Biological Trace Element Research Vol. 50, 1995

40 Koyama et al.
higher serum level of selenium than a diet rich in selenocysteine and/or inorganic forms of selenium, because selenomethionine is deposited not only in selenoproteins, but also in all proteins that contain methionine (30,31). Plants are the ultimate source of selenomethionine. The serum level of selenium may reflect the habitual intake of plant foodstuffs. An epidemiological study supports this hypothesis (32).
The third type of dietary selenium is a form associated with methylmercury contamination in fish (33). Though the bioavailability of selenium in fish has been observed to be low (34), one study shows that the serum concentration of selenium is positively associated with the mercury concentration in erythrocytes (35). Erythrocyte mercury mainly originates from fish in the Japanese diet (36). Thus, serum selenium may be associated with consumption of fish in certain areas where people have an abundant intake of fish.
Consumption of both plant foods and fish may cause an increase in serum selenium concentration. However, it is not clear that these food- stuffs are the key to explaining the association between selenium and apo A-II. Neither plant foods nor fish is likely to raise the serum level of apo A-II. The effects of plant foods and fish, or unsaturated and n-3 polyun- saturated fatty acids, which are rich in plant foods and fish, on the con- centrations of serum total cholesterol and LDL cholesterol (37-41) and serum TG and VLDL-TG (42-44) have been consistent. However, the reported effects on apolipoproteins vary (37-39,41,45-47).
The second possible explanation of the relationship between serum selenium and apo A-II is postulated from the evidence that selenium is likely to bind with lipoproteins. The idea that selenium is associated with lipoproteins in blood during transport has been previously hypothesized (48). Studies show that intravenously injected (49) and in vitro incubated (50) selenium binds to lipoproteins. Approximately 6% of serum sele- nium was found in lipoprotein fractions prepared by an ultracentrifuga- tion method (48).
Selenium is likely to attach to thiol compounds, and apo A-II is a thiol-containing peptide. The reaction of selenium with thiol compounds leads to the formation of selenotrisulfides (51). Such formation seems to be a nonspecific incorporation of selenium into thiol compounds and appears to be largely an in vitro phenomenon (4). Apo A-II was found to be composed of two identical polypeptides linked by a disulfide bridge (52). This arrangement is similar to that of glutathione, which is a com- mon source for selenotrisulfides (51). It is possible that some plasma sele- nium binds to apo A-II forming selenotrisulfides.
Apo A-II is one of the major protein fractions of HDL, like apo A-I. However, the effects of these two apolipoproteins on the cholesterol metab- olism are opposite. A predominant increase in apo A-II may not be benefi- cial for CHD prevention (53-55). The present study shows that serum selenium positively correlates with apo A-II. Dietary interaction is not likely to explain the association, and the formation of selenotrisulfides can be plausibly inferred. Burk and Hill (4) suggested that such formation is not
Biological Trace Element Research Vol. 50, 1995
S e l e n i u m a n d Apol ipoprote in Aq l 41
likely to be of physiological importance. Nevertheless, the possibility that selenium affects the apo A-II metabolism through the formation of selenotrisulfides remains open.
ACKNOWLEDGMENTS
We acknowledge with thanks that the present study was technically supported by B. Satoh and K. Takahashi (NTT Tokyo Health Care Cen- ter). We thank K. Barrymore (Sapporo) for his advice.
REFERENCES
1. K. Schwarz and C. M. Foltz, J. Am. Chem. Sci. 79, 3292 (1957). 2. G. Lockitch, Crit. Rev. Clin. Lab. Sci. 27, 483 (1989). 3. O. A. Levander, Annu. Rev. Nutr. 7, 227 (1987). 4. R. E Burk and K. E. Hill, Annu. Rev. Nutr. 13, 65 (1993). 5. J. T. Salonen, G. Alfthan, J. K. Huttunen, J. Pikkarainen, and P. Puska, Lancet
175 (1982). 6. J. T. Salonen, R. Salonen, K. Seppanen, M. Kantola, M. Parviainen, G.
Alfthan, P. H. Maenpaa, E. Taskinen, and R. Rauramaa, Atherosclerosis, 70, 155 (1988).
7. T. Gordon, W. P. Castelli, M. C. Hjortland, W. B. Kannel, and T. R. Dawber, Am. J. Med. 62, 707 (1977).
8. M. Gebre-Medhin, U. Ewald, and T. Tuvemo, Upsala J. Med. Sci. 93, 57 (1988). 9. Y. Deguchi and A. Ogata, Igaku To Seibutsugaku 121, 229 (1990) (in Japanese).
10. S. G. E Bukkens, N. de Vos, E J. Kok, E. G. Schouten, A. M. de Bruijn, and A. Hofman, J. Am. Coll. Nutr. 9, 128 (1990).
11. E Jossa, M. Trevisan, V. Krogh, E. Farinaro, D. Giumetti, G. Fusco, R. Galasso, S. Panico, S. Frascatore, C. Mellone, and M. Mancini, Atherosclerosis 87, 129 (1991).
12. P. Houze, H. Rouach, M. Gentil, M. T. Orfanelli, and R. Nordmann, Free Rad. Res. Comms. 12-13, 663 (1991).
13. J. T. Snook, Alcohol 8, 13 (1991). 14. H.-K. Cho, E L. Yang, and J. T. Snook, Alcohol 8, 91 (1991). 15. A. Singh, B. L. Smoak, K. Y. Patterson, L. G. LeMay, C. Veillon, and P. A.
Deuster, Am. J. Clin. Nutr. 53, 126 (1991). 16. H. Imai, T. Suzuki, H. Kashiwazaki, T. Takemoto, T. Izumi, and K. Moji,
Nutr. Res. 10, 1205 (1990). 17. W. P. Castelli, J. T. Doyle, T. Gordon, C. G. Hames, M. C. Hjortland, S. B.
Hulley, A. Kagan, and W. J. Zukel, Lancet 2, 153 (1977). 18. J. K. Hutunen, E. Lansimies, E. Voutilainen, C. Ehnholm, E. Hietanen, I.
Penttila, O. Siitonen, and R. Rauramaa, Circulation, 60, 1220 (1979). 19. C. C. Patterson, E. McCrum, D. McMaster, M. Kerr, D. Sykes, and A. E.
Evans, Acta Med. Scand. Suppl. 728, 150 (1988). 20. M.-R. Taskinen, E. A. Nikkila, M. Valimaki, T. Sane, T. Kuusi, Y. A.
Kesaniemi, and R. Ylikahri, Am. Heart J. 113, 458 (1987). 21. E. N. Meilahn, L. H. Kuller, E. A. Stein, A. W. Caggiula, and K. A. Matthews,
Arteriosclerosis 8, 515 (1988). 22. H. Hosokai, S. Tamura, H. Koyama, and H. Satoh, J. Nutr. Sci. Vitaminol. 39,
235 (1993).
Biological Trace Element Research Vol. 50, 1995
42 K o y a m a et al.
23. Y. Yamada, M. Ishizaki, T. Kido, R. Honda, I. Tsuritani, E. Ikai, and H. Yamaya, Hypertension 18, 819 (1991).
24. W. T. Friedewald, R. I. Levy, and D. S. Fredrickson, Clin. Chem. 18, 499 (1972). 25. J. H. Watkinson, Anal. Chem. 38, 92 (1966). 26. S. Aoki, IGAKU TOKEI KAISEKI: Reference Manual. Igaku Shoin, Tokyo
(1989) (in Japanese). 27. R. F. Burk, J. Am. Med. Assoc., 262, 775 (1989). 28. R. Read, T. Bellew, J.-G. Yang, K. E. Hill, I. S. Palmer, and R. E Burk, J. Biol.
Chem. 265, 17899 (1990). 29. N. Avissar, J. C. Whitin, P. Z. Allen, D. D. Wagner, P. Liegey, and H. J. Cohen,
]. Biol. Chem. 264, 15850 (1989). 30. J. T. Deagen, J. A. Butler, M. A. Beilstein, and P. D. Whanger, J. Nutr. 117, 91
(1987). 31. J. T. Deagen, J. A. Butler, B. A. Zachara, and P. D. Whanger, Anal. Biochem.
208, 176 (1993). 32. T. Suzuki, T. Hongo, T. Ohba, K. Kobayashi, H. lmai, H. Ishida, and H.
Suzuki, Nutr. Res. 9, 839 (1989). 33. T. Suzuki, H. Satoh, R. Yamamoto, and H. Kashiwazaki, Bull. Environ. Con-
tam. Toxicol. 24, 805 (1980). 34. J. S. Douglass, V. C. Morris, J. H. Soares Jr., and O. A. Levander, ]. Nutr. 111,
2180 (1981). 35. T. Hongo, C. Watanabe, S. Himeno, and T. Suzuki, Nutr. Res. 5, 1285 (1985). 36. S. Shishido and T. Suzuki, Tohoku J. Exp. Med. 114, 369 (1974). 37. J. M. Iacono and R. M. Dougherty, Am. J. Clin. Nutr. 53, 660 (1991). 38. F. Fumeron, L. Brigant, H.-J. Parra, J.-M. Bard, J.-C. Fruchart, and M. Apfel-
baum, Am. J. Clin. Nutr. 53, 655 (1991). 39. G. M. Wardlaw, J. T. Snook, M.-C. Lin, M. A. Puangco, and J. S. Kwon, Am.
J. Clin. Nutr. 54, 104 (1991). 40. P. Wolmarans, A. J. S. Benade, T. J. Kotze, A. K. Daubizer, M. P. Marais, and
R. Laubscher, Am. J. Clin. Nutr. 53, 1171 (1991). 41. P. Mata, J. A. Garrido, J. M. Ordovas, E. Blazquez, L. A. Alvarez-Sala, M. J.
Rubio, R. Alonso, and M. de Oya, Am. J. Clin. Nutr. 5, 77 (1992). 42. H. O. Bang, J. Dyerberg, and A. H. Nielsen, Lancet, B>I, 1143 (1971). 43. L. Cobiac, P. M. Clifton, M. Abbey, G. B. Belling, and P. J. Nestel, Am. ]. Clin.
Nutr. 53, 1210 (1991). 44. F. Fumeron, L. Brigant, V. Ollivier, D. de Prost, F. Driss, P. Darcet, J.-M. Bard,
H.-J. Parra, J.-C. Fruchart, and M. Apfelbaum, Am. J. Clin. Nutr. 54, 118 (1991). 45. C. M. Smuts, M. Kruger, P. J. van Jaarsveld, J. E. Fincham, R. Schall, K. J. van
der Merwe, and A. J. S. Benade, Prostaglandins, Leukotriene, Essential Fatty Acids 47, 129 (1992).
46. K. H. Bonaa, K. S. Bjerve, and A. Nordoy, Am. J. Clin. Nutr. 55, 1126 (1992). 47. E. B. Schmidt, S. D. Kristensen, R. D. Caterina, and D. R. Illingworth, Ath-
erosclerosis 103, 107 (1993). 48. S. G. Morss, H. R. Ralston, and H. S. Olcptt, Anal. Biochem, 49, 598 (1972). 49. R. H. Burk, Biochim. Biophys. Acta 372, 255 (1974). 50. M. Sandholm, Acta Pharmacol. et Toxicol. 36, 321 (1975). 51. H. E. Ganther, Biochemistry 10, 4089 (1971). 52. H. B. Brewer, Jr., S. E. Lux, R. Roman, and K. M. Hohn, Proc. Natl. Acad. Sci.
USA 69, 1304 (1972). 53. C. J. Fielding and P. E. Fielding, Proc. Natl. Acad. Sci. USA., 78, 3911 (1981). 54. R. Barbaras, P. Puchois, J.-C. Fruchart, and G. Ailhaud, Biochem. Biophys. Res.
Commun. 142, 63 (1987). 55. G. Franceschini, P. Maderna, and C. R. Sirtori, Atherosclerosis, 88, 99 (1977).
Biological Trace Element Research Vol. 50, 1995