Congenital anomaly of cervical vertebrae is a major complication of Rubinstein–Taybi syndrome
4
American Journal of Medical Genetics 135A:130–133 (2005) Congenital Anomaly of Cervical Vertebrae Is a Major Complication of Rubinstein–Taybi Syndrome Toshiyuki Yamamoto, 1 * Kenji Kurosawa, 1 Mitsuo Masuno, 1,2 Shigeharu Okuzumi, 3 Soichi Kondo, 4 Sahoko Miyama, 5 Nobuhiko Okamoto, 6 Noriko Aida, 7 and Gen Nishimura 8 1 Department of Medical Genetics, Clinical Research Institute, Kanagawa Children’s Medical Center (KCMC), Yokohama, Japan 2 Division of Medical Genetics, Department of Nursing, Kawasaki University of Medical Welfare, Kurashiki, Japan 3 Department of Orthopedic Surgery, Kanagawa Children’s Medical Center (KCMC), Yokohama, Japan 4 Department of Orthopedic Surgery, Yokohama Minami Kyosai Hospital, Yokohama, Japan 5 Department of Pediatrics, Tokyo Metropolitan Kiyose Children’s Hospital, Tokyo, Japan 6 Department of Developmental Medicine, Osaka Medical Center and Research Institute for Maternal and Child Health, Osaka, Japan 7 Department of Radiology, Kanagawa Children’s Medical Center (KCMC), Yokohama, Japan 8 Department of Radiology, Tokyo Metropolitan Kiyose Children’s Hospital, Tokyo, Japan Rubinstein–Taybi syndrome (RTS; MIM# 180849) is a well-known malformation syndrome, cha- racterized by broad thumbs and halluces, a characteristic facies, short stature, and mental retardation. RTS is accompanied by a variety of morbid complications, particularly of the skele- ton. Based on the experience of five RTS patients with malformation of the craniovertebral junc- tion, we draw attention to previously unrecog- nized life-threatening complications of RTS, including instability of C1–C2, os odontoideum, hypoplasia of the dens, and fusion of the cervical vertebrae. One patient developed severe cervical myelopathy. Malformation of the cervical spine may be a common syndromic constituent of RTS, to which special attention should be paid to prevent its neurologic sequelae. ß 2005 Wiley-Liss, Inc. KEY WORDS: Rubinstein–Taybi syndrome; cer- vical instability; os odontoideum; myelopathy; dens INTRODUCTION Rubinstein–Taybi syndrome (RTS; MIM# 180849) is a congenital malformation syndrome, characterized by broad thumbs and halluces, a characteristic facies, short stature, and mental retardation. RTS is commonly associated with a variety of morbid complications particularly in the skeleton, such as an increased risk for fractures [Wiley et al., 2003], slipped capital femoral epiphysis [Bonioli et al., 1993], patellar dislocation [Stevens, 1997], and dislocations of other joints. Dental problems also attract attention [Rubinstein, 1990]. Recently, we encountered an RTS patient with cervical myelopathy as a consequence of stenosis at the craniovertebral junction. We then paid special attention to malformations of the cervical spine in other RTS patients and identified four additional patients with the anomalies. The clinical and radio- logical manifestations of these patients are described here. CLINICAL REPORT Patient 1 A girl was diagnosed as having RTS at birth. Her dysmorphic features included characteristic facial expression with micro- gnathia (Fig. 1A) and broad thumbs and halluces. At age 12 years, her developmental quotient was estimated to be 43. She could not speak any meaningful words or wear clothes independently. At that time, she walked alone, but thereafter she became gradually incapable of ambulating. At age 13 years, recurrent seizures commenced, and increased tendon reflex of extremeties and pathologic reflex including Babinski reflex were confirmed by neurologic examination. Detailed MRI examinations revealed myelopathy due to compression and stenosis at the craniovertebral junction (Fig. 2C, Table I). Fusion of C2 –C3 is seen on plain X-ray and three-dimensional computed tomography (3D-CT) (Fig. 2A,B). Hypoplasia of the atlas and occipitalization of the posterior arch of the atlas are shown on 3D-CT and MRI (Fig. 2B,C). Decompression surgery restored her gait capability. Patient 2 A girl was diagnosed as having RTS at birth because of broad thumbs with radial deviation, broad second fingers, broad halluces, and a characteristic facial expression with micro- gnathia and downslanting palpebral fissures (Fig. 1B). At age 19 years, she started to show a peculiar posture, presenting as upward tilting of the head and protrusion of the lower jaw. Neurologic examination did not show any specific sign, while radiologic examination revealed atrophy of the cervical cord due to atlanto-axial subluxation (Table I). Hypoplasia of the dens and hyper instability of C1–C2 with an expanded atlas- odontoid process interval were detected on the plain X-ray (Fig. 2D) [Semine et al., 1978]. Narrowing of the cervical spinal canal and atrophy of the cervico-medullary junction are noted on MRI (Fig. 2E). Patient 3 A girl was diagnosed to have RTS at birth, based on her dysmorphic features, including broad thumbs and char- acteristic facial expression. At age 44 months, she underwent *Correspondence to: Toshiyuki Yamamoto, M.D., Ph.D., Department of Medical Genetics, Kanagawa Children’s Medical Center, 2-138-4 Mutsukawa, Minami-ku, Yokohama 232-8555, Japan. E-mail: [email protected] Received 25 August 2004; Accepted 8 March 2005 DOI 10.1002/ajmg.a.30708 ß 2005 Wiley-Liss, Inc.
-
Upload
toshiyuki-yamamoto -
Category
Documents
-
view
221 -
download
4
Transcript of Congenital anomaly of cervical vertebrae is a major complication of Rubinstein–Taybi syndrome

American Journal of Medical Genetics 135A:130–133 (2005)
Congenital Anomaly of Cervical Vertebrae Is a MajorComplication of Rubinstein–Taybi SyndromeToshiyuki Yamamoto,1* Kenji Kurosawa,1 Mitsuo Masuno,1,2 Shigeharu Okuzumi,3 Soichi Kondo,4
Sahoko Miyama,5 Nobuhiko Okamoto,6 Noriko Aida,7 and Gen Nishimura8
1Department of Medical Genetics, Clinical Research Institute, Kanagawa Children’s Medical Center (KCMC), Yokohama, Japan2Division of Medical Genetics, Department of Nursing, Kawasaki University of Medical Welfare, Kurashiki, Japan3Department of Orthopedic Surgery, Kanagawa Children’s Medical Center (KCMC), Yokohama, Japan4Department of Orthopedic Surgery, Yokohama Minami Kyosai Hospital, Yokohama, Japan5Department of Pediatrics, Tokyo Metropolitan Kiyose Children’s Hospital, Tokyo, Japan6Department of Developmental Medicine, Osaka Medical Center and Research Institute for Maternal and Child Health, Osaka, Japan7Department of Radiology, Kanagawa Children’s Medical Center (KCMC), Yokohama, Japan8Department of Radiology, Tokyo Metropolitan Kiyose Children’s Hospital, Tokyo, Japan
Rubinstein–Taybi syndrome (RTS; MIM# 180849)is a well-known malformation syndrome, cha-racterized by broad thumbs and halluces, acharacteristic facies, short stature, and mentalretardation. RTS is accompanied by a variety ofmorbid complications, particularly of the skele-ton. Based on the experience of five RTS patientswith malformation of the craniovertebral junc-tion, we draw attention to previously unrecog-nized life-threatening complications of RTS,including instability of C1–C2, os odontoideum,hypoplasia of the dens, and fusion of the cervicalvertebrae. One patient developed severe cervicalmyelopathy. Malformation of the cervical spinemay be a common syndromic constituent of RTS,to which special attention should be paid toprevent its neurologic sequelae.� 2005 Wiley-Liss, Inc.
KEY WORDS: Rubinstein–Taybi syndrome; cer-vical instability; os odontoideum;myelopathy; dens
INTRODUCTION
Rubinstein–Taybi syndrome (RTS; MIM# 180849) is acongenital malformation syndrome, characterized by broadthumbs and halluces, a characteristic facies, short stature, andmental retardation. RTS is commonly associated with a varietyof morbid complications particularly in the skeleton, such as anincreased risk for fractures [Wiley et al., 2003], slipped capitalfemoral epiphysis [Bonioli et al., 1993], patellar dislocation[Stevens, 1997], and dislocations of other joints. Dentalproblems also attract attention [Rubinstein, 1990].
Recently, we encountered an RTS patient with cervicalmyelopathy as a consequence of stenosis at the craniovertebral
junction. We then paid special attention to malformations ofthe cervical spine in other RTS patients and identified fouradditional patients with the anomalies. The clinical and radio-logical manifestations of these patients are described here.
CLINICAL REPORT
Patient 1
A girl was diagnosed as having RTS at birth. Her dysmorphicfeatures included characteristic facial expression with micro-gnathia (Fig. 1A) and broad thumbs and halluces. At age12 years, her developmental quotient was estimated to be 43.She could not speak any meaningful words or wear clothesindependently. At that time, she walked alone, but thereaftershe became gradually incapable of ambulating. At age 13 years,recurrent seizures commenced, and increased tendon reflex ofextremeties and pathologic reflex including Babinski reflexwere confirmed by neurologic examination. Detailed MRIexaminations revealed myelopathy due to compression andstenosis at the craniovertebral junction (Fig. 2C, Table I).Fusion of C2–C3 is seen on plain X-ray and three-dimensionalcomputed tomography (3D-CT) (Fig. 2A,B). Hypoplasia of theatlas and occipitalization of the posterior arch of the atlas areshown on 3D-CT and MRI (Fig. 2B,C). Decompression surgeryrestored her gait capability.
Patient 2
A girl was diagnosed as having RTS at birth because of broadthumbs with radial deviation, broad second fingers, broadhalluces, and a characteristic facial expression with micro-gnathia and downslanting palpebral fissures (Fig. 1B). At age19 years, she started to show a peculiar posture, presenting asupward tilting of the head and protrusion of the lower jaw.Neurologic examination did not show any specific sign, whileradiologic examination revealed atrophy of the cervical corddue to atlanto-axial subluxation (Table I). Hypoplasia of thedens and hyper instability of C1–C2 with an expanded atlas-odontoid process interval were detected on the plain X-ray(Fig. 2D) [Semine et al., 1978]. Narrowing of the cervical spinalcanal and atrophy of the cervico-medullary junction are notedon MRI (Fig. 2E).
Patient 3
A girl was diagnosed to have RTS at birth, based on herdysmorphic features, including broad thumbs and char-acteristic facial expression. At age 44 months, she underwent
*Correspondence to: Toshiyuki Yamamoto, M.D., Ph.D.,Department of Medical Genetics, Kanagawa Children’s MedicalCenter, 2-138-4 Mutsukawa, Minami-ku, Yokohama 232-8555,Japan. E-mail: [email protected]
Received 25 August 2004; Accepted 8 March 2005
DOI 10.1002/ajmg.a.30708
� 2005 Wiley-Liss, Inc.

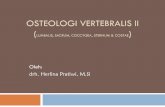
Fig. 1. Facial expression of Patient 1 at age 13 years (A), Patient 2 at 10 years (B), and Patient 4 at 14 years (C).
Fig. 2.

radiologic examination to be screened for cervical malforma-tion. MRI revealed stenosis and compression of the cervicalcord (Fig. 2G). These findings were probably derived fromhypoplasia of the dens and occipitalization of the posterior archof the atlas, identified by X-ray and MRI examinations(Fig. 2F,G, Table I).
Patient 4
A boy was diagnosed as having RTS at birth because of hisbroad thumbs and distinctive facial appearance with micro-gnathia and downslanting palpebral fissures (Fig. 1C). At age23 years, he did not show any neurologic sign, but os odon-toideum with fibrous fusion of the anterior arch of the atlas wasdetected by the 3D and multiplanar reformation (MPR) CTimages (Fig. 2I,J, Table I).
Patient 5
At age 6 years, a boy was diagnosed as having RTS on thebasis of his dysmorphic features, including his characteristicfacies with micrognathia, and bilateral broad thumbs. Psycho-motor development was moderately retarded with IQ of 45.Although there was no pyramidal sign, radiologic examinationat age 20 years showed os odontoideum and a fusion of posteriorelement of C2–C3 (Fig. 2K, Table I).
DISCUSSION
The neurologic and radiologic manifestations in the fivepatients we described are summarized in Table I. The spec-trum of skeletal abnormalities comprised occipitalization andhypoplasia of the atlas, hypoplasia of the dens, os odontoideum,and fusion of C2 and C3. Three patients (Patients 1, 2, and 3)showed compression or atrophy of the cervical cord as a
consequence of stenosis at the craniovertebral junction: thestenosis was attributed to congenital malsegmentation of theatlanto-occipital region in two patients (Patients 1 and 3),while it was caused by atlanto-axial instability with hypoplasiaof the dens in the other (Patient 2). Os odontoideum withoutatlanto-axial instability was found in other two patients(Patients 4 and 5).
Most anomalies of the craniovertebral junction above areapparently congenital. However, it remains to be definitivelydetermined whether os odontoideum in Patients 4 and 5 iscongenital or acquired. Os odontoideum is defined as a smallcorticated ossicle separated from the base of the axis, which iscommonly associated with atlanto-axial instability [Hadley,2002; Fukuda et al., 2003]. The etiology remains controversial.It is postulated that dense fracture is occasionally responsiblefor the development of os odontoideum [Sakaida et al., 2001;Hadley, 2002]. In the context of increased risk for fracture inRTS, the role of dense fracture should be considered in ourpatients. In our series of RTS patients, however, os odontoi-deum was always accompanied by other congenital anomaliesof the cervical spine, implying its congenital origin.
Transcriptional coactivators, CREB-binding protein (CBP)and EP300, are key regulators of RNA polymerase II-mediatedtranscription [Kalkhoven, 2004]. Both of them are known asthe family of mammalian HATs and share structural homologyeach other. Haploinsufficiency of theCBPgene (CBP) is a likelycause of RTS in humans, since no clear phenotypic differenceswere observed between patients in whom microdeletions ortruncating mutations were found [Kalkhoven et al., 2003]. Justrecently, mutations in the EP300 gene have also been reportedto cause RTS, and genetic heterogeneity has been confirmed inthis entity [Roelfsema et al., 2004]. No deletion was detected inthree (Patients 1, 2, and 4) of our five patients [Masuno et al.,1994] by FISH analysis using RT1 cosmid probe (provided byLyden University) including CBP, but molecular studies to
TABLE I. Summary of Neurologic and Radiologic Findings in Five Patients
No. ofpatients
Gender/age
(years)Neurologic
findings
Radiologic findings
C1 Dens
Relationshipbetween
C1 and C2
Othervertebral
fusion
Spinalcanal
stenosisSpinalcord
1 F/13 Mild Hypoplasia — — C2–C3 þ Compressionquadriplegia Occipitalization High signal
on T2WI2 F/19 Abnormal
posture— Hypoplasia Atlanto-axial
dislocation— þ Atrophy
3 F/3 — Occipitalization Hypoplasia — — þ Compression4 M/23 — — Os odontoideum Fusion of atlas
and osodontoideum
— — n.e.
5 M/20 — — Os odontoideum — Posteriorelementof C2–C3
n.e. n.e.
F, female; M, male; T2WI, T2-weighted image; n.e., not evaluated.
Fig. 2. Lateral view of the cervical spine in flexion position of Patients 1(A), 2 (D), and 3 (F). Three-dimensional computed tomography (3D-CT) ofPatients 1 (B) and 4 (I). Sagittal T2-weighted MRI of Patients 1 (C), 2 (E),and 3 (G). Lateral view of the cervical spine in normal position of Patients 4(H) and 5 (K). Mid-sagittal multiplanar reformation (MPR) CT image ofPatient 5 (J). A and B: Vertebral fusion (arrowhead) and occipitalization ofC1 (arrow). C: Abnormal compression and high signal of the cervico-
medullary junction (arrow). D: Distance (arrow) between posterior portion ofthe anterior arch of the atlas and adjacent border of the odontoid process ofthe axis is expanded to 8 mm. E: Narrowing of the cervical spinal canal andatrophy of the cervico-medullary junction (arrow). F: Occipitalization of C1(arrow). G: Stenosis of the cervical canal and compression of the cervical cord(arrow). I and J: Os odontoideum (arrow). K: Os odontoideum (arrow) andvertebral fusion (arrowhead).
132 Yamamoto et al.

scan mutations in theCBP and the EP300 genes have not beenperformed in our patients. It remains to be investigatedwhether cervical abnormalities are associated with specificmutation(s) in the CBP or EP300 gene.
Wiley et al. [2003] recently proposed medical guidelines forRTS, but never mentioned malformations of the cervical spine.We would like to recommend medical geneticists to pay muchattention to the alignment of the cervical structure of RTSpatients for the prevention of its neurologic sequelae.
REFERENCES
Bonioli E, Bellini C, Senes FM, Palmieri A, Di Stadio M, Pinelli G. 1993.Slipped capital femoral epiphysis associated with Rubinstein–Taybisyndrome. Clin Genet 44:79–81.
Fukuda M, Aiba T, Akiyama K, Nishiyama K, Ozawa T. 2003. Cerebellarinfarction secondary to os odontoideum. J Clin Neurosci 10:625–626.
Hadley MN. 2002. Os odontoideum. Neurosurgery 50:S148–S155.
Kalkhoven E. 2004. CBP and p300: HATs for different occasions. BiochemPharmacol 68:1145–1155.
Kalkhoven E, Roelfsema JH, Teunissen H, den Boer A, Ariyurek Y, ZantemaA, Breuning MH, Hennekam RC, Peters DJ. 2003. Loss of CBP
acetyltransferase activity by PHD finger mutations in Rubinstein–Taybi syndrome. Hum Mol Genet 12:441–450.
Masuno M, Imaizumi K, Kurosawa K, Makita Y, Petrij F, Dauwerse HG,Breuning MH, Kuroki Y. 1994. Submicroscopic deletion of chromosomeregion 16p13.3 in a Japanese patient with Rubinstein–Taybi syndrome.Am J Med Genet 53:352–354.
Roelfsema JH, White S, Ariyrek Y, Bartholdi D, Niedrist D, Carnavale F, denDunnen JT, van Ommen G-JB, Hennekam RC, Peters DJM. 2004.Mutations in the EP300 gene cause Rubinstein–Taybi syndrome. Am JHum Genet Suppl 75:S27.
Rubinstein JH. 1990. Broad thumb-hallux (Rubinstein–Taybi) syndrome1957–1988. Am J Med Genet 6:S3–S16.
Sakaida H, Waga S, Kojima T, Kubo Y, Niwa S, Matsubara T. 2001. Osodontoideum associated with hypertrophic ossiculum terminale. Casereport. J Neurosurg 94(1 Suppl):S140–S144.
Semine AA, Ertel AN, Goldberg MJ, Bull MJ. 1978. Cervical-spineinstability in children with Down syndrome (trosomy 21). J Bone JointSurg Am 60:649–652.
Stevens CA. 1997. Patellar dislocation in Rubinstein–Taybi syndrome. Am JMed Genet 72:188–190.
Wiley S, Swayne S, Rubinstein JH, Lanphear NE, Stevens CA. 2003.Rubinstein–Taybi syndrome medical guidelines. Am J Med Genet 119:101–110.
Vertebral Anomalies of Rubinstein–Taybi Syndrome 133
![KEY CHART FOR MODEL Circulatory System with ......33. Tibia 33.脛骨 34. Fibula 34.腓骨 2 24. Cervical vertebrae[C1-C7] 25. Thoracic vertebrae[T1-T12] 26. Lumbar vertebrae[L1-L5]](https://static.fdocument.pub/doc/165x107/6094bfd05d03d21fc74cac1e/key-chart-for-model-circulatory-system-with-33-tibia-33ee-34-fibula.jpg)