Clinical implications of a molecular genetic classification of monogenic β-cell diabetes
14
www.nature.com/clinicalpractice/endmet SUMMARY Clinical implications of a molecular genetic classification of monogenic β-cell diabetes Rinki Murphy, Sian Ellard and Andrew T Hattersley* Continuing Medical Education online Medscape, LLC is pleased to provide online continuing medical education (CME) for this journal article, allowing clinicians the opportunity to earn CME credit. Medscape, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide CME for physicians. Medscape, LLC designates this educational activity for a maximum of 1.0 AMA PRA Category 1 Credits TM . Physicians should only claim credit commensurate with the extent of their participation in the activity. All other clinicians completing this activity will be issued a certificate of participation. To receive credit, please go to http://www.medscape.com/cme/ncp and complete the post-test. Learning objectives Upon completion of this activity, participants should be able to: 1 List the 4 proposed clinical subtypes of monogenic diabetes. 2 Describe the clinical features of glucokinase hyperglycemia/diabetes. 3 Describe the criteria for testing to distinguish dia- betes caused by hepatocyte nuclear factor-1alpha (HNF-1alpha) mutations from type 1 and 2 diabetes. 4 Describe the clinical features of permanent and transient neonatal diabetes. Competing interests The authors declared no competing interests. Désirée Lie, the CME questions author, declared no relevant financial relationships. INTRODUCTION Since 1992, numerous genetic subtypes of diabetes have been described in which gene mutations result in diabetes primarily through β-cell dysfunc- tion. This knowledge means that patients who were previously categorized clinically as having maturity-onset diabetes of the young (MODY), permanent neonatal diabetes mellitus (PNDM) or transient neonatal diabetes mellitus (TNDM) can now usually be classified by genetic subgroup. Definition of the genetic subgroup can result in appropriate treatment, genetic counseling and prognostic information. In this article we describe the challenge of identifying the minority of patients who have monogenic β-cell diabetes (1–2% of all diabetes cases) amongst the vast majority who have type 1 Monogenic diabetes resulting from mutations that primarily reduce β-cell function accounts for 1–2% of diabetes cases, although it is often misdiagnosed as either type 1 or type 2 diabetes. Knowledge of the genetic etiology of diabetes enables more-appropriate treatment, better prediction of disease progression, screening of family members and genetic counseling. We propose that the old clinical classifications of maturity-onset diabetes of the young and neonatal diabetes are obsolete and that specific genetic etiologies should be sought in four broad clinical situations because of their specific treatment implications. Firstly, diabetes diagnosed before 6 months of age frequently results from mutation of genes that encode Kir6.2 (ATP- sensitive inward rectifier potassium channel) or sulfonylurea receptor 1 subunits of an ATP-sensitive potassium channel, and improved glycemic control can be achieved by treatment with high-dose sulfonylureas rather than insulin. Secondly, patients with stable, mild fasting hyperglycemia detected particularly when they are young could have a glucokinase mutation and might not require specific treatment. Thirdly, individuals with familial, young-onset diabetes that does not fit with either type 1 or type 2 diabetes might have mutations in the transcription factors HNF-1α (hepatocyte nuclear factor 1-α) or HNF-4α, and can be treated with low- dose sulfonylureas. Finally, extrapancreatic features, such as renal disease (caused by mutations in HNF-1β) or deafness (caused by a mitochondrial m.3243A>G mutation), usually require early treatment with insulin. KEYWORDS genetics, glucokinase, maturity onset diabetes of the young, neonatal diabetes, transcription factor R Murphy was a Clinical Research Fellow, S Ellard is Professor of Human Molecular Genetics, and AT Hattersley is Professor of Molecular Medicine at the Peninsula Medical School, Exeter, UK. Correspondence *Peninsula Medical School, Barrack Road, Exeter, Devon EX2 5DW, UK [email protected] Received 29 October 2007 Accepted 14 December 2007 Published online 26 February 2008 www.nature.com/clinicalpractice doi:10.1038/ncpendmet0778 REVIEW CRITERIA For this Review we selected papers and abstracts listed in PubMed that reported on the clinical features, genetics, prevalence, pathophysiology and treatment of β-cell monogenic diabetes. We concentrated on neonatal diabetes and those types of diabetes previously classified as maturity-onset diabetes of the young. SUMMARY CME 200 NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM APRIL 2008 VOL 4 NO 4 REVIEW
Transcript of Clinical implications of a molecular genetic classification of monogenic β-cell diabetes

www.nature.com/clinicalpractice/endmet
SUMMARY
Clinical implications of a molecular genetic classification of monogenic β-cell diabetesRinki Murphy, Sian Ellard and Andrew T Hattersley*
Continuing Medical Education onlineMedscape, LLC is pleased to provide online continuing medical education (CME) for this journal article, allowing clinicians the opportunity to earn CME credit. Medscape, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide CME for physicians. Medscape, LLC designates this educational activity for a maximum of 1.0 AMA PRA Category 1 CreditsTM. Physicians should only claim credit commensurate with the extent of their participation in the activity. All other clinicians completing this activity will be issued a certificate of participation. To receive credit, please go to http://www.medscape.com/cme/ncp and complete the post-test.
Learning objectivesUpon completion of this activity, participants should be able to: 1 List the 4 proposed clinical subtypes of monogenic
diabetes.2 Describe the clinical features of glucokinase
hyperglycemia/diabetes.3 Describe the criteria for testing to distinguish dia-
betes caused by hepatocyte nuclear factor-1alpha (HNF-1alpha) mutations from type 1 and 2 diabetes.
4 Describe the clinical features of permanent and transient neonatal diabetes.
Competing interestsThe authors declared no competing interests. Désirée Lie, the CME questions author, declared no relevant financial relationships.
INTRODUCTIONSince 1992, numerous genetic subtypes of diabetes have been described in which gene mutations result in diabetes primarily through β-cell dysfunc-tion. This knowledge means that patients who were previously categorized clinically as having maturity-onset diabetes of the young (MODY), permanent neonatal diabetes mellitus (PNDM) or transient neonatal diabetes mellitus (TNDM) can now usually be classified by genetic subgroup. Definition of the genetic subgroup can result in appropriate treatment, genetic counseling and prognostic information.
In this article we describe the challenge of identifying the minority of patients who have monogenic β-cell diabetes (1–2% of all diabetes cases) amongst the vast majority who have type 1
Monogenic diabetes resulting from mutations that primarily reduce β-cell function accounts for 1–2% of diabetes cases, although it is often misdiagnosed as either type 1 or type 2 diabetes. Knowledge of the genetic etiology of diabetes enables more-appropriate treatment, better prediction of disease progression, screening of family members and genetic counseling. We propose that the old clinical classifications of maturity-onset diabetes of the young and neonatal diabetes are obsolete and that specific genetic etiologies should be sought in four broad clinical situations because of their specific treatment implications. Firstly, diabetes diagnosed before 6 months of age frequently results from mutation of genes that encode Kir6.2 (ATP-sensitive inward rectifier potassium channel) or sulfonylurea receptor 1 subunits of an ATP-sensitive potassium channel, and improved glycemic control can be achieved by treatment with high-dose sulfonylureas rather than insulin. Secondly, patients with stable, mild fasting hyperglycemia detected particularly when they are young could have a glucokinase mutation and might not require specific treatment. Thirdly, individuals with familial, young-onset diabetes that does not fit with either type 1 or type 2 diabetes might have mutations in the transcription factors HNF-1α (hepatocyte nuclear factor 1-α) or HNF-4α, and can be treated with low-dose sulfonylureas. Finally, extrapancreatic features, such as renal disease (caused by mutations in HNF-1β) or deafness (caused by a mitochondrial m.3243A>G mutation), usually require early treatment with insulin.
KEYWORDS genetics, glucokinase, maturity onset diabetes of the young, neonatal diabetes, transcription factor
R Murphy was a Clinical Research Fellow, S Ellard is Professor of Human Molecular Genetics, and AT Hattersley is Professor of Molecular Medicine at the Peninsula Medical School, Exeter, UK.
Correspondence*Peninsula Medical School, Barrack Road, Exeter, Devon EX2 5DW, [email protected]
Received 29 October 2007 Accepted 14 December 2007 Published online 26 February 2008
www.nature.com/clinicalpracticedoi:10.1038/ncpendmet0778
REVIEW CRITERIAFor this Review we selected papers and abstracts listed in PubMed that reported on the clinical features, genetics, prevalence, pathophysiology and treatment of β-cell monogenic diabetes. We concentrated on neonatal diabetes and those types of diabetes previously classified as maturity-onset diabetes of the young.
SUMMARY
CME
200 NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM APRIL 2008 VOL 4 NO 4
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

APRIL 2008 VOL 4 NO 4 MURPHY ET AL. NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM 201
www.nature.com/clinicalpractice/endmet
or 2 diabetes. First, we discuss why we think the term MODY might be outdated. Next, we describe how to differentiate monogenic diabetes from other types of diabetes. We then outline the monogenic β-cell forms of diabetes under the following four main phenotypic cate-gories for clearer clinical identification: diabetes diagnosed before 6 months of age (which is usually associated with mutations in Kir6.2 or sulfonyl-urea receptor 1 [SUR1], or with abnormalities in chromosome 6q24); familial, mild fasting hyper-glycemia (asso ciated with glucokinase muta-tion); familial, young-onset diabetes (associated with HNF1 homeobox A gene [HNF1A; previ-ously termed TCF1] or HNF4 homeobox A gene [HNF4A]); and diabetes with extra pancreatic features (associated with HNF1 homeobox B gene [HNF1B; previously termed TCF2] or mitochondrial m.3243A>G mutation).
WHY THE TERM MODY IS DEADThe confusing term maturity-onset diabetes of the young originates from the time when the terms juvenile-onset and maturity-onset were used to distinguish between type 1 (insulin-dependent) and type 2 (noninsulin-dependent) diabetes. MODY was used to describe a subgroup of autosomal-dominantly inherited diabetes that despite having a young age of onset (at least one family member diagnosed before 25 years of age) was noninsulin-dependent (as patients had moderate but insufficient circulating C-peptide levels 5 years after diagnosis).1
At least seven discrete genetic etiologies of diabetes2–4 have been described, and these account for much of the clinical hetero geneity apparent among patients receiving a diagnosis of MODY on the basis of this clinical definition. The different genetic subtypes differ in age of onset, pattern of hyperglycemia, response to treatment and associated extrapancreatic mani-festations, which suggests that it is inappropriate to lump them all into a single category. The ‘maturity-onset’ part of MODY implies a resem-blance to type 2 diabetes, but all the subtypes—as well as differing from each other—are very different from type 2 diabetes. Since the classifi-cation of diabetes was revised in 1998 to reflect etiology,5 we propose that the term MODY is now obsolete and that the correct monogenic names of the different forms of young-onset diabetes should be used when possible.
DIFFERENTIATION OF MONOGENIC FROM OTHER TYPES OF DIABETESDifferentiation from apparent type 1 diabetesPatients with a clinical diagnosis of type 1 diabetes who also have a two-generation or three-generation family history of diabetes with evidence of noninsulin dependence should be suspected of having monogenic diabetes (Table 1). Absence of autoantibodies against pancreatic antigens and detection of measurable C-peptide in the presence of hyperglycemia outside the ‘honeymoon period’ (the period of up to 5 years
Table 1 Differentiation of β-cell monogenic diabetes from type 1 and type 2 diabetes.
Features Type 1 diabetes Young-onsettype 2 diabetes
GCK DM TF DM KATP PNDM 3243 MIDD
Insulin dependence Yes No No No Yes Yes or no
Parent affected 2–4% Yes Yes Yes 15% Mother
Age of onset 6 months to young adulthood
Adolescence and young adulthood
Birth Teens to young adulthood
<6 months Young adulthood
Obesitya Population frequency
Increased frequency
Population frequency
Population frequency
Population frequency
Rare
Acanthosisnigricans
No Yes No No No No
Glycemia High Variable Mild High High Variable
β-Cell autoantibodies Yes No No No No No
C-peptide (nmol/l) <0.33 0.5–>1 0.1–0.7 0.1–0.7 <0.2 0.1–0.7
aThe population frequency is the frequency of obesity that occurs in the general population. Abbreviations: 3243 MIDD, maternally inherited diabetes and deafness associated with mitochondrial m.3243A>G mutation; GCK DM, diabetes mellitus associated with mutations in glucokinase; KATP PNDM, permanent neonatal diabetes associated with mutations in the ATP-sensitive potassium channel; TF DM, diabetes mellitus associated with mutations in transcription factors (e.g. hepatocyte nuclear factor 1-α [HNF1-α], HNF4-α, or HNF-1β).
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

202 NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM MURPHY ET AL. APRIL 2008 VOL 4 NO 4
www.nature.com/clinicalpractice/endmet
after diagnosis when there is some endogenous insulin secretion) are atypical for type 1 diabetes and increase the probability that the patient has monogenic diabetes. We recommend genetic testing for HNF1A mutations (the most common transcription factor mutations that cause mono-genic diabetes) in any young adult with apparent type 1 diabetes and a diabetic parent, and who is antibody-negative at diagnosis, especially if there is preservation of C-peptide levels in both the child and the parent.
Differentiation from apparent young-onset type 2 diabetesMonogenic forms of diabetes should be suspected in cases of young-onset, apparent type 2 diabetes when obesity and features of insulin resistance are absent (Table 1). In patients with young-onset diabetes, lack of obesity, absence of acan-thosis nigricans or polycystic ovarian syndrome, and elevated or normal HDL-cholesterol and reduced or normal triglyceride levels6–8 are all features that make presence of monogenic β-cell forms of diabetes likely.
As mentioned above, when monogenic diabetes is diagnosed it can be classified under four phenotypic categories: diabetes diagnosed before 6 months of age; familial, mild fasting hyperglycemia; familial, young-onset diabetes (Figure 1); or diabetes with extrapancreatic features (Figure 2). We now detail when each of these categories should be considered, and the features of each.
DIABETES DIAGNOSED BEFORE 6 MONTHS OF AGEDiabetes diagnosed before 6 months of age is likely to be one of the monogenic forms of neonatal diabetes and not autoimmune type 1 diabetes.9,10 The diabetes resolves in approxi-mately half of all patients with neonatal diabetes, and the majority of cases of TNDM (~70%) are linked to abnormalities in the chromosome 6q24 region.11 In individuals with PNDM, mutations in KCNJ11 (potassium inwardly rectifying channel, subfamily J, member 11 gene) or ABCC8 (ATP-binding cassette, subfamily C, member 8 gene)—which encode the Kir6.2 and SUR1 subunits, respectively, of the ATP-sensitive potassium channel (KATP channel)—are found in half of the patients.12–17 It is important to identify patients with these mutations because—despite being insulin dependent—oral sulfonylurea provides the most effective therapy.18
Mutations in KCNJ11 or ABCC8 can also cause TNDM.16,19 At the time of diagnosis, it is not known whether the diabetes in an infant will be transient or permanent. We therefore recom-mend testing for 6q24 abnormalities and KCNJ11 mutations first, and for ABCC8 mutations if these tests are negative (Figure 1).
Neonatal diabetes due to mutations in the ATP-sensitive potassium channel Clinical featuresThe majority of patients with Kir6.2 neonatal diabetes (i.e. neonatal diabetes caused by Kir6.2 mutations) have isolated diabetes; most have PNDM rather than TNDM, but 20% have neuro logical features (Table 2). These features occasionally constitute a severe syndrome of developmental delay, epilepsy and neonatal diabetes (DEND) or, more commonly, inter-mediate DEND, which is characterized by diabetes and less-severe develop mental delay without epilepsy.20 The diabetes typically presents from birth to 26 weeks of age (mean 5 weeks), usually with marked hyper glycemia and ketoacidosis.15 Low birth weight (mean 2,500 g) is common because of fetal insulin defi-ciency in utero, because insulin is a major fetal growth factor in the third trimester of preg-nancy.21 SUR1 neonatal diabetes has a similar phenotype, but TNDM is more common than PNDM, and DEND syndrome is rare.
PathophysiologyFour Kir6.2 and four SUR1 subunits make up the pancreatic KATP channel; this channel regulates insulin secretion by linking intracellular ATP production to β-cell membrane potential and insulin secretion. Activating KCNJ11 or ABCC8 mutations mostly reduce the response of the channel to ATP, which prevents channel closure and consequent insulin secretion. The specific mutation determines the phenotype,15,22 and for Kir6.2 mutations there is a striking correlation with the functional severity of the muta-tion (reviewed by Hattersley and Ashcroft20), although there are a few exceptions.23,24
TherapyThe identification of KATP channel mutations in patients with PNDM has had a dramatic impact on their diabetes therapy. These patients have little or no endogenous insulin secretion and C-peptide is usually undetectable,12 so they were previously assumed to require lifelong insulin treatment.
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

APRIL 2008 VOL 4 NO 4 MURPHY ET AL. NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM 203
www.nature.com/clinicalpractice/endmet
Sulfonylureas do, however, bind to the SUR1 subunits of the KATP channel and close the channel in an ATP-independent manner. Approximately 90% of patients with Kir6.2 neonatal diabetes can transfer from insulin to sulfonylurea tablets and achieve improved glycemic control,18,23 and a similar pattern is emerging for patients with SUR1 neonatal diabetes.16,22
Most patients with KATP channel mutations are treated with glibenclamide. The doses used are considerably higher than those used for the treatment of type 2 diabetes,13,18 and these high
doses (typically 0.4–0.8 mg/kg/day) may cause transitory diarrhea.25 Glibenclamide binds nonspecifically to SUR subunits found in KATP channels in nerve, muscle and brain, in addi-tion to β cells, and hence enables some improve-ment of associated neurological symptoms as well as the diabetes. Although many patients with mild developmental delay and diabetes (inter mediate DEND) treated with sulfonylurea therapy have been able to discontinue insulin, and have shown improved motor function, concentration and speech,26 others with the
Diabetes diagnosedbefore 6 months of age
Familial, young-onsetdiabetes
Familial, mild fastinghyperglycemia (>5.5 mmol/l)a
Test for heterozygousGCK mutations
No treatment
Test for HNF1A andif negative HNF4A
Oral sulfonylurea (low dose)
May require insulin in pregnancydepending on fetal growth
Transient Permanent
Test forchromosome
6q24abnormalities
and, if negative, for KCNJ11 and
ABCC8
If negative,consider INS orGCK mutationsor rare causes in
presence ofother features
(Table 2)
Test forKCNJ11 and,
if negative,ABCC8
Transientinsulin
Oralsulfonylurea(high dose)
Observe forrelapse ofdiabetes in
teenage years
Useglibenclamideif neurological
featurespresent
Onset in adolescence oryoung childhoodProgressive hyperglycemiaOGTT: large increment(>4.5 mmol/l) between 0 h and 2 h glucoseComplications frequent
Onset at birthStable hyperglycemiaOGTT: low increment(<4.5 mmol/l) between 0 h and 2 h glucoseComplications rare
Clinical subtypes of β-cellmonogenic diabetes
Diabetes with extrapancreaticfeatures (see Figure 2)
Figure 1 Clinical subtypes and management of monogenic β-cell diabetes that does not have extrapancreatic features. See Figure 2 for diabetes that has extrapancreatic features. To convert plasma glucose measurements to mg/dl, multiply by 18.02. Abbreviations: ABCC8, ATP-binding cassette, subfamily C, member 8 gene; GCK, glucokinase gene; HNF, hepatocyte nuclear factor; HNF1A, HNF1 homeobox A gene; HNF4A, HNF4 homeobox A gene; INS, insulin gene; KCNJ11, potassium inwardly rectifying channel, subfamily J, member 11 gene; OGTT, oral glucose tolerance test.
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am
204 NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM MURPHY ET AL. APRIL 2008 VOL 4 NO 4
www.nature.com/clinicalpractice/endmet
full DEND syndrome have not responded to sulfonylurea therapy. Since a sulfonylurea drug would be used in a situation where it does not have a license, we recommend liaison with centers that have experience in transferring patients from insulin to sulfonylureas to help guide this process.
Genetic counselingFamilies with two or more generations affected are rare (~15% of cases), and most children with KATP channel mutations are born to parents who do not have diabetes. The majority of sporadic cases result from de novo heterozygous muta-tions, but around 40% of patients with PNDM as a result of ABCC8 mutations show recessive inheritance.17 For parents of children with reces-sively inherited ABCC8 mutations the risk of neonatal diabetes for each future child is 25%, but the affected child is at very low risk of having affected offspring. Affected individuals with a heterozygous KATP channel mutation have a 50% chance of passing the mutation to their chil-dren. Unaffected parents of a child with a de novo mutation, however, should be counseled that the recurrence risk of a second child being affected is not negligible because germline mosaicism (in which mutations may be present in the gonads but not detectable in blood) has been reported in several families.27,28
Transient neonatal diabetes due to disordered imprinting Clinical featuresTNDM is usually diagnosed in the first week of life (range 1–81 days). Affected children are typi-cally born with lower birth weight (mean 2,000 g) than those with PNDM, but require less insulin and doses can be tapered so that they are no longer insulin-treated by a median of 12 weeks.29 The relapse rate is 50–60%, at an average age of 14 years; diabetes at this stage results predomi-nantly from moderate β-cell dysfunction. One-third of patients with TNDM have macro-glossia, and occasionally an umbilical hernia is present.
PathophysiologyGene imprinting occurs when only the paternal or maternal allele of a gene is expressed. In 70% of cases of TNDM11 there is an abnormality of a region of chromosome 6q24 that results in the overexpression of the paternally expressed genes PLAGL1 (pleiomorphic adenoma gene-like 1; also termed tumor repressor ZAC) and HYMAI (hydatidiform mole associated and imprinted gene).29 Three types of abnormality have been described: paternal uniparental disomy, which accounts for 50% of sporadic TNDM cases; paternal duplication of 6q24, found in most familial cases; and abnormal methylation of
Renal cystsExocrine pancreatic deficiencyGenitourinary abnormalities
DeafnessShort staturePigmentary retinopathy
Diabetes withextrapancreatic features
Optic atrophyDiabetes insipidusDeafnessRenal tract abnormalitiesNeurological abnormalities
Megaloblastic anemiaDeafnessCardiac abnormalitiesNeurological abnormalities
Test for RCAD syndrome:HNF1B
Test for MIDD: mitochondrial m.3243A>G mutation
Test for Wolfram syndrome:WFS1
Test for TRMA syndrome:SLC19A2
Early insulin Oral sulfonylurea initially,but rapid insulin requirement
Insulin Thiamine and/or sulfonylureaand/or early insulin
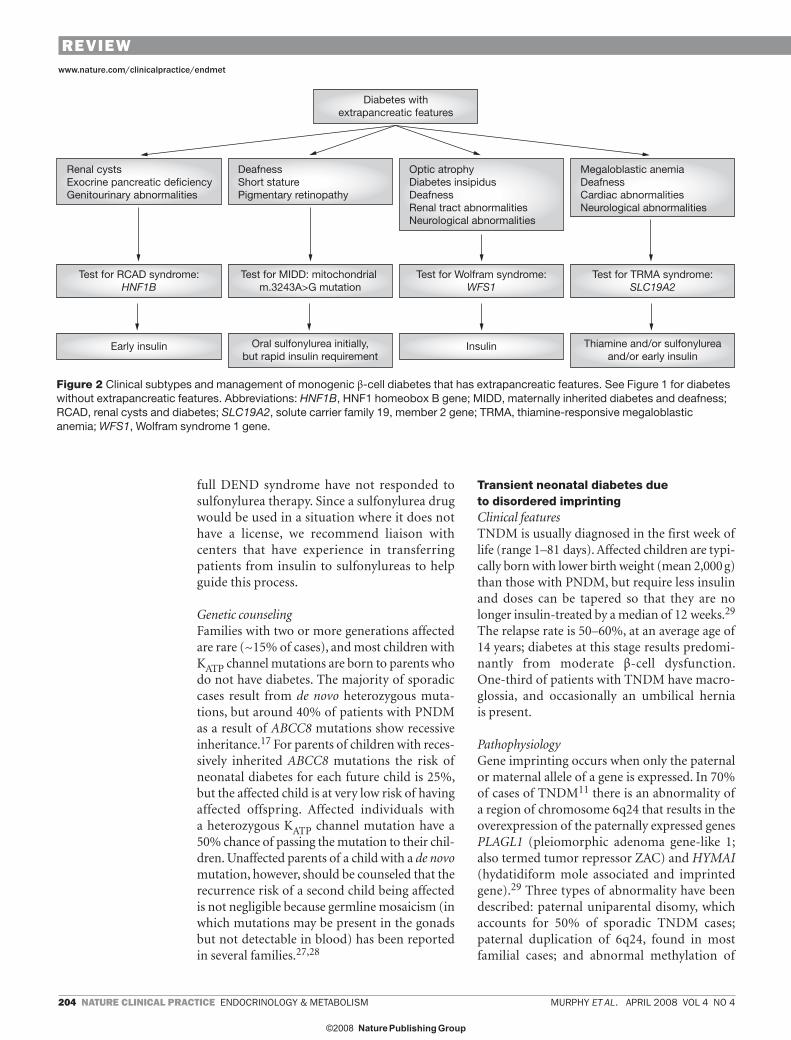
Figure 2 Clinical subtypes and management of monogenic β-cell diabetes that has extrapancreatic features. See Figure 1 for diabetes without extrapancreatic features. Abbreviations: HNF1B, HNF1 homeobox B gene; MIDD, maternally inherited diabetes and deafness; RCAD, renal cysts and diabetes; SLC19A2, solute carrier family 19, member 2 gene; TRMA, thiamine-responsive megaloblastic anemia; WFS1, Wolfram syndrome 1 gene.
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

APRIL 2008 VOL 4 NO 4 MURPHY ET AL. NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM 205
www.nature.com/clinicalpractice/endmet
the maternal copy of chromosome 6, found in sporadic cases.29 Most of the remainder of patients with TNDM have KATP channel muta-tions,11,19 but there is virtually no overlap with the mutations observed in PNDM cases.
TherapyTreatment during the neonatal phase is with insulin; however, on relapse treatment may include dietary modification, oral hypoglycemic agents and/or insulin.30
Genetic counselingGenetic counseling of TNDM cases depends on the genetic etiology. Cases with uni parental disomy of chromosome 6 are sporadic and, therefore, have low recurrence risk in siblings and offspring. In cases of familial paternal duplications of the 6q24 region, males have a 50% chance of transmitting TNDM to their children. If females pass on this duplica-tion, their children will not be affected but the sons may pass on the risk of TNDM to their children.
Other subtypes of neonatal diabetesHeterozygous mutations in the insulin gene (INS) have been identified and could account for 15–20% of cases of PNDM.31 Patients with PNDM and an INS mutation have permanent diabetes without extrapancreatic features except a low birth weight, which is a feature of all subtypes of neonatal diabetes. The other known genetic causes of neonatal diabetes are rare (Table 2). Clinical features, such as pancreatic aplasia or extrapancreatic features, and knowledge of consanguinity can be very helpful when deciding whether to test for other genetic subtypes.
FAMILIAL, MILD FASTING HYPERGLYCEMIAPatients who have mild fasting hyperglycemia (5.5–8.0 mmol/l; to convert to mg/dl, multiply by 18.02) that shows little deterioration with age might have heterozygous glucokinase gene (GCK) mutations that do not require any specific treat-ment. Although the mild hyperglycemia can be present from birth, patients are asymptomatic and most remain undiagnosed until later in life. The age at testing will determine the clinical
Table 2 Causes of neonatal diabetes mellitus.
Pancreatic pathophysiology
Protein, chromosome or gene affected
Reported prevalence Inheritance Features in addition to neonatal diabetes and low birth weight
Reduced β-cell function
KATP channel 50% of PNDM and 25% of TNDM
Autosomal dominant or recessive
Developmental delay and epilepsy
Chromosome 6q24 70% of TNDM Variable Macroglossia and umbilical hernia
GCK (recessive mutation)
6 cases of PNDM77–79 (6 families)
Autosomal recessive Both parents have heterozygous GCK-associated hyperglycemia
SLC2A2 1 case of PNDM80 (1 family)
Autosomal dominant Hypergalactosemia, hepatic failure
GLIS3 6 cases of PNDM81,82 (3 families)
Autosomal recessive Congenital hypothyroidism, glaucoma, liver fibrosis and cystic kidney disease
Reduced pancreas mass
PTF1A 5 cases of PNDM83 (2 families)
Autosomal recessive Pancreatic and cerebellar agenesis
PDX1 2 cases of PNDM56,84 (2 families)
Autosomal recessive Pancreatic agenesis
HNF1B 1 case of PNDM, 1 case of TNDM10,65 (2 families)
Autosomal dominant Exocrine pancreas insufficiency and renal cysts
Increased β-cell destruction
EIF2AK3 25 cases of PNDM85–87 (15 families)
Autosomal recessive Spondyloepiphyseal dysplasia, renal failure, recurrent hepatitis and mental retardation
FOXP3 17 cases of PNDM88–92 (13 families)
X-linked Immune dysregulation, intractable diarrhea, eczematous skin rash and elevated IgE
INS 21 cases of PNDM31 (16 families)
Autosomal dominant None
Abbreviations: EIF2AK3, eukaryotic translation initiation factor 2-α kinase 3 gene; FOXP3, forkhead box P3 gene; GCK, glucokinase gene; GLIS3, GLIS family zinc finger 3 gene; HNF1B, HNF1 homeobox B gene; INS, insulin gene; KATP channel, ATP-sensitive potassium channel; PDX1, pancreatic and duodenal homeobox 1 gene (previously termed IPF1); PNDM, permanent neonatal diabetes mellitus; PTF1A, pancreas specific transcription factor, 1a gene; SLC2A2, solute carrier family 2, member 2 gene (previously termed GLUT2); TNDM, transient neonatal diabetes mellitus.
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

206 NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM MURPHY ET AL. APRIL 2008 VOL 4 NO 4
www.nature.com/clinicalpractice/endmet
classification given to patients; individuals can be diagnosed as having incidental hyperglycemia or even type 1 diabetes (if detected during child-hood), gestational diabetes (if detected during pregnancy) or well-controlled type 2 diabetes (if detected in adulthood). A diagnosis of incidental hyperglycemia in a young child might trigger intensive monitoring for incipient type 1 diabetes and in some cases unnecessary treatment with insulin.32 Making a genetic diagnosis of gluco-kinase hyperglycemia is, therefore, worthwhile.33 Fasting hyperglycemia in a child is strongly sugges-tive of a GCK mutation and apparently una ffected parents should be tested for asympto matic fasting hyperglycemia (Figure 1).
PrevalenceNo large-scale population studies to assess the prevalence of GCK mutations have been performed. Approximately 2% of pregnant women are diagnosed as having gestational diabetes, and of these approximately 2–5% have a GCK mutation,34 which would suggest a population prevalence of 0.04–0.10%.
PathophysiologyThe glucokinase enzyme catalyzes the rate-limiting step of glucose phosphorylation and, therefore, enables the β cell and hepatocyte to respond appropriately to the degree of glycemia.35 The kinetics of the glucokinase enzyme mean that heterozygous mutations cause an increased fasting glucose set point but that glucose meta bolism is regulated to this new level. As a result, most indivi-duals with heterozygous GCK mutations have fasting plasma glucose levels between 5.5 and 8.0 mmol/l. Patients with mutated GCK produce adequate insulin responses, and most have a small increment in plasma glucose (<3 mmol/l in 70% of patients) 2 h after an oral glucose load.36 This feature also explains why hemoglobin A1c levels rarely exceed 7.5% and why microvascular complications are rare.37 Approximately half of all patients with a GCK mutation are diagnosed as diabetic based on an oral glucose tolerance test (OGTT), with the majority being diagnosed according to fasting values rather than 2 h values. Most of those without diabetes have impaired fasting glucose levels.36,38
ManagementHypoglycemic medication is not appropriate for most patients with heterozygous gluco kinase diabetes, as they have mild hyperglycemia;
furthermore, because of the preserved regula-tion of glycemia, such medication has minimal effect. In 28 patients we observed identical hemo-globin A1c values (6.3%) before and after treat ment with insulin or other medication was dis continued (O Gill-Carey et al., unpublished data).
Pregnancy is the one exception in which hypo-glycemic medication might be appropriate, but insulin is required only in cases in which there is excess fetal growth.39 The fetus has a 50% chance of inheriting the GCK mutation from its mother, and the presence of the GCK mutation in the fetus influences its sensing of maternal glycemia. If the fetus does not inherit the GCK mutation it will respond to maternal hyperglycemia by excess insulin production and, therefore, excess growth; however, if the fetus does inherit the GCK mutation it will produce normal amounts of insulin and grow normally.40,41 If increased fetal growth is detected it will be hard to lower the mother’s glucose level (which is regulated at the raised level); thus, greater-than-replacement doses of insulin will be required.39 Early delivery is often the most helpful intervention.
Even though microvascular complications are rare in glucokinase diabetes, it is prudent to maintain regular retinopathy screening in patients over 40 years of age. The inheritance of a GCK mutation does not protect against the concurrent development of type 2 diabetes, which occurs at a similar prevalence in those with GCK mutations as in the general population.
Genetic counselingEach child of a parent with glucokinase diabetes has a 50% chance of inheriting the GCK muta-tion. Predictive genetic testing of children is not advocated since measurement of fasting blood glucose provides a simple diagnostic test—GCK mutation carriers have mild hyperglycemia from birth. Molecular genetic analysis can then be used as a confirmatory test. In the rare circumstance in which both parents have glucokinase diabetes (more likely in consanguineous couples), each child has a 25% chance of having PNDM caused by inheriting two GCK mutations.
FAMILIAL, YOUNG-ONSET DIABETESThose patients in whom diabetes is diagnosed before age 25 years and does not fit the phenotypes of either type 1 or type 2 diabetes, and who also have a strong family history of diabetes, need to be evaluated for mutations in transcription factors, most commonly hepatocyte nuclear factor 1-α
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

APRIL 2008 VOL 4 NO 4 MURPHY ET AL. NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM 207
www.nature.com/clinicalpractice/endmet
(HNF-1α; encoded by HNF1A). An important reason for making this genetic diagnosis is that, in many cases, treatment with low-dose oral sulfonylurea is highly effective (Figure 1).
Heterozygous mutations in the trans cription factor genes HNF1A, HNF4A, or HNF1B (effects of mutations in this gene are detailed in the later section on diabetes with extrapancreatic features), and more rarely in PDX1 (pancre-atic and duodenal homeobox 1 gene; previ-ously termed IPF1) or NEUROD1 (neurogenic differentiation 1 gene), result in similar diabetes phenotypes. Patients with these mutations differ from those with glucokinase diabetes by having normal glucose levels at birth and progressive deterioration in glucose tolerance. As a conse-quence of their increasing hyperglycemia they are at high risk of diabetic complications. In the early stages of diabetes, fasting glucose remains relatively normal initially, but increases greatly following meals or a glucose load.36
HNF1A mutation carriers Clinical featuresPatients with HNF1A mutations typically present in their teens or early adult life with symptomatic diabetes and have progressive β-cell failure that results in increasing hyperglycemia throughout life. HNF1A mutation carriers often have fasting plasma glucose levels that remain normal initially, despite diabetes being indicated by elevated 2 h plasma glucose concentrations during OGTT,36 with a large increment value (typically >4.5 mmol/l). This test result occurs because initially the insulin secretion rate in HNF1A mutation carriers is appropriate to their insulin sensitivity at glucose values below 8 mmol/l.42
The frequency of microvascular complications in patients with HNF1A diabetes is similar to that in patients with type 1 and type 2 diabetes, and is related to poor glycemic control.43 Although the frequency of hypertension in patients with HNF1A diabetes is similar to that in patients with type 1 diabetes, the frequency of coronary heart disease seems to be greater in patients with HNF1A diabetes.43 Raised HDL-cholesterol levels are observed in patients with HNF1A diabetes, in contrast to the reduced levels seen in patients with type 2 diabetes and the normal levels seen in patients with type 1 diabetes.7 The elevated HDL-cholesterol level does not, however, seem to be cardioprotective.
Glycosuria is a key feature of HNF1A mutation carriers before they develop diabetes.44 A
positive urine test for glycosuria after a large unrefined carbohydrate meal could, therefore, suggest the need for a formal OGTT and genetic testing in young children from families with an HNF1A mutation.
PrevalenceMutations in the HNF1A gene are the commonest monogenic form of transcription factor diabetes, with 193 different mutations reported; the most common mutation is the insertion of a C nucleotide (Pro291fsinsC) in a polyC-tract mutation hotspot.45 We estimate that patients with mutations in HNF1A account for approximately 1–2% of patients with diabetes, although most cases are not diagnosed. This prevalence level would result in a population frequency of approximately 0.02–0.04%.
PathophysiologyPatients with HNF1A mutations have a progres-sive β-cell defect. HNF-1α is one of several tran-scription factors within a complex regulatory network that includes HNF-4α, PDX1 and HNF-1β. This network is crucial for pancreatic β-cell development and functioning.
PenetranceHNF1A mutations have a high penetrance, with 63% of carriers developing diabetes by 25 years of age, 79% by 35 years and 96% by 55 years.46 The age at diagnosis is determined in part by the loca-tion of the mutation: patients with mutations in the terminal exons (8–10) diagnosed on average 8 years later than those with mutations in exons 1–6.47 Intrauterine exposure to maternal diabetes reduces the age of onset of this type of diabetes in the offspring by approximately 12 years.48
ManagementThe importance of diagnosing patients who have HNF1A diabetes is that this type of diabetes is very sensitive to sulfonylurea therapy.49 The therapy is highly effective because the β-cell defects that result from reduced transcription factor function are in glucose metabolism and are, therefore, bypassed by sulfonylureas, which act on the KATP channel to stimulate insulin release.49 We recommend sulfonylurea therapy initially in very low doses (e.g. 20–40 mg glicla-zide daily) as the first-line pharmacological treat-ment in HNF1A diabetes, and that patients on other oral agents or insulin should have a trial of sulfonylureas. Currently, insulin remains the most common treatment during pregnancy for this
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

208 NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM MURPHY ET AL. APRIL 2008 VOL 4 NO 4
www.nature.com/clinicalpractice/endmet
patient group, but further studies are required to validate the safety and efficacy of sulfonylureas such as glibenclamide (also known as glyburide) that have least permeability through the placenta and have been used in gestational diabetes.50
Genetic counselingA parent with HNF1A diabetes has a 50% chance of passing on the mutation to each child. Predictive genetic testing in unaffected family members may be helpful but should be preceded by counseling to enable relatives to make an informed decision. The main advantages of knowing this genetic informa-tion include reduction in uncertainty over the risk of diabetes and increased efficiency in monitoring for early signs of diabetes.51
HNF4A mutation carriers Clinical featuresThe diabetes of HNF4A mutation carriers presents in a very similar way to that of HNF1A mutation carriers. Unlike HNF1A mutation carriers, however, these carriers have reduced levels of lipoprotein A1, lipoprotein A2 and HDL cholesterol, whereas LDL-cholesterol levels tend to be increased; thus, the lipid patterns of HNF4A mutation carriers resemble those commonly seen in patients with type 2 diabetes.8 Increased birth weight (by ~800 g) and macrosomia are common features of HNF4A mutation carriers, and transient neonatal hypo glycemia may precede the diabetes.52
PrevalenceThe prevalence of HNF4A diabetes is 20–30% in patients thought to have transcription factor diabetes who do not have a mutation in HNF1A.8
PathophysiologySimilar to patients with HNF1A diabetes, patients with HNF4A mutations have a progressive β-cell dysfunction. The mechanism that underlies the biphasic pattern of hyperinsulinism in utero followed by diabetes in later life is unknown.52
PenetranceGenerally, HNF4A has a high penetrance, with the majority of carriers developing diabetes by the age of 25 years; however, in some families the age of diagnosis is older.52
ManagementLong-term treatment with low-dose sulfonyl-ureas seems effective for HNF4A diabetes.8 The clinical significance of reduced HDL-cholesterol
and increased LDL-cholesterol levels in these patients remains to be determined; at present the cholesterol levels of patients with HNF4A mutations should be managed in light of other cardiovascular risk factors, as for other patients with diabetes. Genetic counseling is similar to that for individuals with HNF1A mutations.
Other etiologiesMutations in the transcription factor genes PDX1 and NEUROD1 are extremely rare,53–56 but from the limited data it seems that the diabetes pheno-type, penetrance and pathophysiology resemble those in patients with mutations in the tran-scription factor HNF-1α. Two different mutations in the transcription factor gene PAX4 (paired box 4 gene) have been identified in Thai fami-lies with MODY.57 Two families with diabetes and exocrine pancreatic dysfunction have been found who have mutations in the gene encoding the enzyme carboxyl ester lipase (CEL).3
In at least 11% of families with autosomal-dominant β-cell disease a genetic diagnosis cannot be made, presumably because of the presence of as-yet-undetermined gene mutations.4
DIABETES WITH EXTRAPANCREATIC FEATURESVery rare diabetes-related disorders (Figure 2), such as Wolfram syndrome and thiamine-responsive megaloblastic anemia, are fairly easy to recog-nize because of the presence of co morbidities; Wolfram syndrome (also known as DIDMOAD because of the occurrence of diabetes insipi dus, diabetes mellitus, optic atrophy and deaf-ness) is also characterized by progressive neuro-degeneration. Patients with thiamine-responsive megaloblastic anemia in addition to hemato-logical manifestations might also have deafness, cardiac abnormalities and neurological abnormal-ities. Two diabetes subtypes with extra pancreatic features that are frequently under diagnosed at present, however, are the renal cysts and diabetes syndrome resulting from mutations or dele-tions of the transcription factor gene HNF1B, and maternally inherited diabetes and deafness (MIDD) resulting from the mito chondrial point mutation m.3243A>G.
Renal cysts and diabetes syndrome Clinical featuresThe predominant phenotype of patients with HNF1B mutations is developmental renal disease, which is characterized by renal cysts
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

APRIL 2008 VOL 4 NO 4 MURPHY ET AL. NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM 209
www.nature.com/clinicalpractice/endmet
(the most common phenotype), renal dysplasia, renal-tract malformations and/or familial hypo-plastic glomerulocystic kidney disease.10 Female genital-tract malformations, gout and hyper-uricemia can also occur (Figure 3A).58,59 Birth weight is reduced by around 800 g as a result of reduced insulin secretion in utero.60 Half of all HNF1B mutation carriers have early-onset diabetes that presents in a similar fashion to HNF1A diabetes, but HNF1B mutation carriers are more insulin resistant.61 Common vari-ants in the HNF1B gene are associated with an increased risk for prostate cancer but protect against type 2 diabetes.62
PrevalenceHNF1B mutations are less frequent than HNF1A or HNF4A mutations in patients with diabetes, but they are common in patients with develop-mental renal disease.63 A family history of renal disease (or diabetes) is not essential to prompt a screen for this disorder, as spontaneous muta-tions and deletions of this gene are common (one-third to two-thirds of cases).63,64
PathophysiologyHNF-1β is a transcription factor that is expressed in early embryonic development of the kidney,
pancreas, liver and genital tract, which explains the multiple organ involvement seen (Figure 3A).
PenetranceThere is wide variation in phenotypes even within a single pedigree, such that different combinations and severities of organ involve-ment are manifest among affected individuals who have identical mutations.58,59,63,65
ManagementThe coexisting pancreatic atrophy and associ-ated insulin resistance means that the diabetes of HNF1B carriers is not sensitive to sulfonylurea medication, and early insulin therapy is required.
Maternally inherited diabetes and deafness Clinical featuresMaternally inherited diabetes associated with young-onset, bilateral sensorineural deafness should prompt genetic testing for the most common mito-chondrial point mutation—m.3243A>G. This mutation results in dysfunction of mitochondria (organelles whose main purpose is to generate energy by producing ATP); as a result, the manifes-tations in patients with MIDD are within the organs that are most metabolically active (Figure 3B). At the most severe end of the spectrum, the
Developmentalkidney disease
Gout
Urogenitalabnormalities
DiabetesPancreaticatrophy
AbnormalLFTs
Focalsegmentalglomerulosclerosis
Constipation
Deafness
Myopathy
Diabetes
Cardiomyopathy
Pigmentary retinopathy
A B
Figure 3 Phenotypes seen in diabetes with extra-pancreatic features. (A) Renal cysts and diabetes syndrome caused by mutation in HNF1 homeobox B gene (HNF1B). (B) Maternally inherited diabetes and deafness caused by mitochondrial m.3243A>G mutation. Kidney manifestations of HNF1B mutations include hypoplastic glomerulocystic kidney disease, cystic renal dysplasia, solitary functioning kidney, horseshoe kidney and oligomeganephronia. Urogenital manifestations of HNF1B mutations include bicornuate uterus, bilateral agenesis of vas deferens, large epididymal cysts and asthenospermia. Abbreviation: LFTs, liver function tests.
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

210 NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM MURPHY ET AL. APRIL 2008 VOL 4 NO 4
www.nature.com/clinicalpractice/endmet
m.3243A>G mutation can manifest in mito-chondrial myopathy, encephalopathy, lactic acidosis and stroke-like episodes syndrome.66
Diabetes in MIDD usually presents insidiously in a similar way to type 2 diabetes, but approxi-mately 20% of patients have an acute presenta-tion that resembles that of type 1 diabetes, with ketoacidosis occurring in 8%.67–69 The mean age at diagnosis of diabetes is 37 years, and ranges from 11 to 68 years.67
PrevalenceThe prevalence of MIDD due to the m.3243A>G mutation in Japanese patients with diabetes is 1.5%, which seems to be higher than that in Europeans and other ethnic groups (0.4%).70
PathophysiologyThe pathophysiology of diabetes in MIDD is related to the mitochondrial dysfunction in the highly metabolically active pancreatic islets. This dysfunction causes abnormal β-cell function, reduction in β-cell mass71,72 and insulin deficiency.73,74
PenetranceThe penetrance of diabetes in offspring with the m.3243A>G mutation is age dependent, but is estimated to be more than 85% by the age of 70 years.69,75
ManagementThe majority of patients with MIDD are initially treated with dietary modification or oral hypo-glycemic agents, but insulin is usually required by 2 years after diagnosis.67–69 Metformin should probably be avoided because of the theoretical risk of exacer bating lactic acidosis, as metformin is known to interfere with mitochondrial function (although no cases have been reported to date).
Genetic counselingAffected fathers should be reassured that they will not transmit the disorder to their children. An affected mother transmits the m.3243A>G mutation to all her children, even though some children may remain clinically unaffected.
CONCLUSIONSWith the advances in defining the monogenic etiology of diabetes, which accounts for approxi-mately 1–2% of all diabetes cases, we have learned that these genetic subtypes of diabetes require different treatments. Patients with Kir6.2 or SUR1
PNDM require high-dose sulfonylurea therapy, most cases of transcription factor diabetes require low-dose sulfonylurea therapy, and glucokinase diabetes requires no hypo glycemic treatment.
These therapies are different to those used to treat type 1 or type 2 diabetes, so it is impor-tant that we identify individuals with a probable monogenic cause for their diabetes. Molecular genetic testing for a mutation in the KCNJ11 or ABCC8 genes that encode the KATP channel subunits should be considered in all patients with diabetes diagnosed before 6 months of age. Individuals with familial, young-onset diabetes (diagnosed before 25 years of age) that does not fit with type 1 or type 2 diabetes should be screened for mutations in the tran-scription factor gene HNF1A, and then for those in HNF4A. Patients with familial, mild fasting hyperglycemia that does not deteriorate with age should be tested for GCK mutations. Diagnostic molecular genetic testing is now available in many countries.76 This testing can improve the management of these monogenic forms of diabetes, which are often underdiagnosed.
KEY POINTS■ The old clinical classifications of maturity-
onset diabetes of the young (MODY) and neonatal diabetes should now be replaced with a molecular genetic diagnosis, as this offers a more useful guide to clinical management
■ Monogenic β-cell diabetes is often misdiagnosed as type 1 or type 2 diabetes and a correct diagnosis can improve treatment
■ Diabetes diagnosed before 6 months of age will be monogenic diabetes and the underlying gene mutations can be identified in 75% of cases
■ Most neonatal patients with mutations in the potassium-sensitive ATP channel subunits Kir6.2 and sulfonylurea receptor 1 will be best treated with high-dose sulfonylureas rather than insulin injections, despite seeming insulin dependent
■ Patients with glucokinase mutations have stable, mild, regulated hyperglycemia throughout life and do not need pharmacological treatment except possibly during pregnancy
■ Patients with mutations in HNF1A have hyperglycemia that deteriorates with age and that can be severe; these patients, like patients with mutations in HNF4A, are sensitive to the hypoglycemic effects of sulfonylureas
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

APRIL 2008 VOL 4 NO 4 MURPHY ET AL. NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM 211
www.nature.com/clinicalpractice/endmet
References1 Tattersall RB (1974) Mild familial diabetes with
dominant inheritance. Q J Med 43: 339–3572 Raeder H et al. (2007) Pancreatic lipomatosis is a
structural marker in nondiabetic children with mutations in carboxyl-ester lipase. Diabetes 56: 444–449
3 Raeder H et al. (2006) Mutations in the CEL VNTR cause a syndrome of diabetes and pancreatic exocrine dysfunction. Nat Genet 38: 54–62
4 Stride A and Hattersley AT (2002) Different genes, different diabetes: lessons from maturity-onset diabetes of the young. Ann Med 34: 207–216
5 Alberti KG and Zimmet PZ (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 15: 539–553
6 Lehto M et al. (1999) Mutation in the HNF-4α gene affects insulin secretion and triglyceride metabolism. Diabetes 48: 423–425
7 Pearson E et al. (2003) HDL-cholesterol: differentiating between HNF-1α MODY and type 2 diabetes [abstract]. Diabet Med 20 (Suppl 2): S1–S33
8 Pearson ER et al. (2005) Molecular genetics and phenotypic characteristics of MODY caused by hepatocyte nuclear factor 4α mutations in a large European collection. Diabetologia 48: 878–885
9 Iafusco D et al. (2002) Permanent diabetes mellitus in the first year of life. Diabetologia 45: 798–804
10 Edghill EL et al. (2006) Mutations in hepatocyte nuclear factor-1β and their related phenotypes. J Med Genet 43: 84–90
11 Flanagan SE et al. (2007) Mutations in ATP-sensitive K+ channel genes cause transient neonatal diabetes and permanent diabetes in childhood or adulthood. Diabetes 56: 1930–1937
12 Gloyn AL et al. (2004) Activating mutations in the gene encoding the ATP-sensitive potassium-channel subunit Kir6.2 and permanent neonatal diabetes. N Engl J Med 350: 1838–1849
13 Sagen J et al. (2004) Permanent neonatal diabetes due to mutations in KCNJ11 encoding Kir6.2: patient characteristics and initial response to sulfonylurea therapy. Diabetes 53: 2713–2718
14 Vaxillaire M et al. (2004) Kir6.2 mutations are a common cause of permanent neonatal diabetes in a large cohort of French patients. Diabetes 53: 2719–2722
15 Flanagan SE et al. (2006) Mutations in KCNJ11, which encodes Kir6.2, are a common cause of diabetes diagnosed in the first 6 months of life, with the phenotype determined by genotype. Diabetologia 49: 1190–1197
16 Babenko AP et al. (2006) Activating mutations in the ABCC8 gene in neonatal diabetes mellitus. N Engl J Med 355: 456–466
17 Ellard S et al. (2007) Permanent neonatal diabetes caused by dominant, recessive, or compound heterozygous SUR1 mutations with opposite functional effects. Am J Hum Genet 81: 375–382
18 Pearson ER et al. (2006) Switching from insulin to oral sulfonylureas in patients with diabetes due to Kir6.2 mutations. N Engl J Med 355: 467–477
19 Vaxillaire M et al. (2007) New ABCC8 mutations in relapsing neonatal diabetes and clinical features. Diabetes 56: 1737–1741
20 Hattersley AT and Ashcroft FM (2005) Activating mutations in Kir6.2 and neonatal diabetes: new clinical syndromes, new scientific insights, and new therapy. Diabetes 54: 2503–2513
21 Slingerland AS and Hattersley AT (2005) Mutations in the Kir6.2 subunit of the KATP channel and permanent neonatal diabetes: new insights and new treatment. Ann Med 37: 186–195
22 Patch AM et al. (2007) Mutations in the ABCC8 gene encoding the SUR1 subunit of the KATP channel cause transient neonatal diabetes, permanent neonatal diabetes or permanent diabetes diagnosed outside the neonatal period. Diabetes Obes Metab 9 (Suppl 2): S28–S39
23 Masia R et al. (2007) An ATP-binding mutation (G334D) in KCNJ11 is associated with a sulfonylurea-insensitive form of developmental delay, epilepsy, and neonatal diabetes. Diabetes 56: 328–336
24 Shimomura K et al. (2006) Mutations at the same residue (R50) of Kir6.2 (KCNJ11) that cause neonatal diabetes produce different functional effects. Diabetes 55: 1705–1712
25 Codner E et al. (2005) High-dose glibenclamide can replace insulin therapy despite transitory diarrhea in early-onset diabetes caused by a novel R201L Kir6.2 mutation. Diabetes Care 28: 758–759
26 Slingerland AS et al. (2006) Improved motor development and good long-term glycaemic control with sulfonylurea treatment in a patient with the syndrome of intermediate developmental delay, early-onset generalised epilepsy and neonatal diabetes associated with the V59M mutation in the KCNJ11 gene. Diabetologia 49: 2559–2563
27 Edghill EL et al. (2007) Origin of de novo KCNJ11 mutations and risk of neonatal diabetes for subsequent siblings. J Clin Endocrinol Metab 92: 1773–1777
28 Gloyn AL et al. (2004) Permanent neonatal diabetes due to paternal germline mosaicism for an activating mutation of the KCNJ11 gene encoding the Kir6.2 subunit of the β-cell potassium adenosine triphosphate channel. J Clin Endocrinol Metab 89: 3932–3935
29 Temple IK et al. (2000) Transient neonatal diabetes mellitus: widening our understanding of the aetiopathogenesis of diabetes. Diabetes 49: 1359–1366
30 Temple IK and Shield JP (2002) Transient neonatal diabetes, a disorder of imprinting. J Med Genet 39: 872–875
31 Stoy J et al. (2007) Insulin gene mutations as a cause of permanent neonatal diabetes. Proc Natl Acad Sci U S A 104: 15040–15044
32 Schnyder S et al. (2005) Genetic testing for glucokinase mutations in clinically selected patients with MODY: a worthwhile investment. Swiss Med Wkly 135: 352–356
33 Matyka KA et al. (1998) Genetic testing for maturity onset diabetes of the young in childhood hyperglycaemia. Arch Dis Child 78: 552–554
34 Ellard S et al. (2000) A high prevalence of glucokinase mutations in gestational diabetic subjects selected by clinical criteria. Diabetologia 43: 250–253
35 Matschinsky FM (1993) Evolution of the glucokinase glucose sensor paradigm for pancreatic β cells. Diabetologia 36: 1215–1217
36 Stride A et al. (2002) The genetic abnormality in the β cell determines the response to an oral glucose load. Diabetologia 45: 427–435
37 Velho G et al. (1997) Identification of 14 new glucokinase mutations and description of the clinical profile of 42 MODY-2 families. Diabetologia 40: 217–224
38 Froguel P et al. (1993) Familial hyperglycemia due to mutations in glucokinase. Definition of a subtype of diabetes mellitus. N Engl J Med 328: 697–702
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

212 NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM MURPHY ET AL. APRIL 2008 VOL 4 NO 4
www.nature.com/clinicalpractice/endmet
39 Spyer G et al. (2001) Influence of maternal and fetal glucokinase mutations in gestational diabetes. Am J Obstet Gynecol 185: 240–241
40 Hattersley AT et al. (1998) Mutations in the glucokinase gene of the fetus result in reduced birth weight. Nat Genet 19: 268–270
41 Velho G et al. (2000) Maternal diabetes alters birth weight in glucokinase-deficient (MODY2) kindred but has no influence on adult weight, height, insulin secretion or insulin sensitivity. Diabetologia 43: 1060–1063
42 Byrne MM et al. (1996) Altered insulin secretory responses to glucose in diabetic and nondiabetic subjects with mutations in the diabetes susceptibility gene MODY3 on chromosome 12. Diabetes 45: 1503–1510
43 Isomaa B et al. (1998) Chronic diabetic complications in patients with MODY3 diabetes. Diabetologia 41: 467–473
44 Stride A et al. (2005) β-Cell dysfunction, insulin sensitivity, and glycosuria precede diabetes in hepatocyte nuclear factor-1α mutation carriers. Diabetes Care 28: 1751–1756
45 Ellard S and Colclough K (2006) Mutations in the genes encoding the transcription factors hepatocyte nuclear factor 1 α (HNF1A) and 4 α (HNF4A) in maturity-onset diabetes of the young. Hum Mutat 27: 854–869
46 Shepherd M et al. (2001) Genetic testing in maturity onset diabetes of the young (MODY): a new challenge for the diabetic clinic. Pract Diab Int 18: 16–21
47 Harries LW et al. (2006) Isomers of the TCF1 gene encoding hepatocyte nuclear factor-1 α show differential expression in the pancreas and define the relationship between mutation position and clinical phenotype in monogenic diabetes. Hum Mol Genet 15: 2216–2224
48 Stride A et al. (2002) Intrauterine hyperglycemia is associated with an earlier diagnosis of diabetes in HNF-1a gene mutation carriers. Diabetes Care 25: 2287–2291
49 Pearson ER et al. (2003) Genetic cause of hyperglycaemia and response to treatment in diabetes. Lancet 362: 1275–1281
50 Langer O et al. (2000) A comparison of glyburide and insulin in women with gestational diabetes mellitus. N Engl J Med 343: 1134–1138
51 Liljestrom B et al. (2005) Genetic testing for maturity onset diabetes of the young: uptake, attitudes and comparison with hereditary non-polyposis colorectal cancer. Diabetologia 48: 242–250
52 Pearson ER et al. (2007) Macrosomia and hyperinsulinaemic hypoglycaemia in patients with heterozygous mutations in the HNF4A gene. PLoS Med 4: e118
53 Kristinsson SY et al. (2001) MODY in Iceland is associated with mutations in HNF-1α and a novel mutation in NeuroD1. Diabetologia 44: 2098–2103
54 Liu L et al. (2007) A novel mutation, Ser159Pro in the NeuroD1/BETA2 gene contributes to the development of diabetes in a Chinese potential MODY family. Mol Cell Biochem 303: 115–120
55 Malecki MT et al. (1999) Mutations in NEUROD1 are associated with the development of type 2 diabetes mellitus. Nat Genet 23: 323–328
56 Stoffers D et al. (1997) Early-onset diabetes mellitus (MODY4) linked to IPF1. Nat Genet 17: 138–139
57 Plengvidhya N et al. (2007) PAX4 mutations in Thais with maturity onset diabetes of the young. J Clin Endocrinol Metab 92: 2821–2826
58 Bingham C and Hattersley AT (2004) Renal cysts and diabetes syndrome resulting from mutations in hepatocyte nuclear factor-1β. Nephrol Dial Transplant 19: 2703–2708
59 Lindner TH et al. (1999) A novel syndrome of diabetes mellitus, renal dysfunction and genital malformation associated with a partial deletion of the pseudo-POU domain of hepatocyte nuclear factor-1β. Hum Mol Genet 8: 2001–2008
60 Edghill EL et al. (2006) Hepatocyte nuclear factor-1 β mutations cause neonatal diabetes and intrauterine growth retardation: support for a critical role of HNF-1β in human pancreatic development. Diabet Med 23: 1301–1306
61 Pearson ER et al. (2004) Contrasting diabetes phenotypes associated with hepatocyte nuclear factor-1α and –1β mutations. Diabetes Care 27: 1102–1107
62 Gudmundsson J et al. (2007) Two variants on chromosome 17 confer prostate cancer risk, and the one in TCF2 protects against type 2 diabetes. Nat Genet 39: 977–983
63 Ulinski T et al. (2005) Renal phenotypes related to hepatocyte nuclear factor-1β (TCF2) mutations in a pediatric cohort. J Am Soc Nephrol 17: 497–503
64 Bellanne-Chantelot C et al. (2005) Large genomic rearrangements in the hepatocyte nuclear factor-1β (TCF2) gene are the most frequent cause of maturity-onset diabetes of the young type 5. Diabetes 54: 3126–3132
65 Yorifuji T et al. (2004) Neonatal diabetes mellitus and neonatal polycystic, dysplastic kidneys: phenotypically discordant recurrence of a mutation in the hepatocyte nuclear factor-1β gene due to germline mosaicism. J Clin Endocrinol Metab 89: 2905–2908
66 Goto Y-i et al. (1990) A mutation in the tRNA Leu(UUR) gene associated with the MELAS subgroup of mitochondrial encephalomyopathies. Nature 348: 651–653
67 Guillausseau PJ et al. (2004) Heterogeneity of diabetes phenotype in patients with 3243 bp mutation of mitochondrial DNA (maternally inherited diabetes and deafness or MIDD). Diabetes Metab 30: 181–186
68 Guillausseau PJ et al. (2001) Maternally inherited diabetes and deafness: a multicenter study. Ann Intern Med 134: 721–728
69 Maassen JA et al. (2004) Mitochondrial diabetes: molecular mechanisms and clinical presentation. Diabetes 53 (Suppl 1): S103–S109
70 Murphy R et al. (2007) Clinical features, diagnosis and management of maternally inherited diabetes and deafness (MIDD) associated with the 3243A>G mitochondrial point mutation. Diabet Med [doi:10.1111/j.1464-5491.2007.02359.x]
71 Kobayashi T et al. (1997) In situ characterization of islets in diabetes with a mitochondrial DNA mutation at nucleotide position 3243. Diabetes 46: 1567–1571
72 Lynn S et al. (2003) Heteroplasmic ratio of the A3243G mitochondrial DNA mutation in single pancreatic β cells. Diabetologia 46: 296–299
73 Kadowaki T (1994) Mutations in the mitochondrial gene in patients with NIDDM [Japanese]. Nippon Rinsho 52: 2708–2714
74 Walker M et al. (1995) Insulin and proinsulin secretion in subjects with abnormal glucose tolerance and a mitochondrial tRNA Leu(UUR) mutation. Diabetes Care 18: 1507–1509
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am

APRIL 2008 VOL 4 NO 4 MURPHY ET AL. NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM 213
www.nature.com/clinicalpractice/endmet
75 Maassen JA (2002) Mitochondrial diabetes: pathophysiology, clinical presentation, and genetic analysis. Am J Med Genet 115: 66–70
76 Diabetes Genes [www.diabetesgenes.org]77 Njolstad PR et al. (2003) Permanent neonatal diabetes
caused by glucokinase deficiency: inborn error of the glucose-insulin signaling pathway. Diabetes 52: 2854–2860
78 Njolstad PR et al. (2001) Neonatal diabetes mellitus due to complete glucokinase deficiency. N Engl J Med 344: 1588–1592
79 Porter JR et al. (2005) Permanent neonatal diabetes in an Asian infant. J Pediatr 146: 131–133
80 Yoo HW et al. (2002) Identification of a novel mutation in the GLUT2 gene in a patient with Fanconi–Bickel syndrome presenting with neonatal diabetes mellitus and galactosaemia. Eur J Pediatr 161: 351–353
81 Senee V et al. (2006) Mutations in GLIS3 are responsible for a rare syndrome with neonatal diabetes mellitus and congenital hypothyroidism. Nat Genet 38: 682–687
82 Taha D et al. (2003) Neonatal diabetes mellitus, congenital hypothyroidism, hepatic fibrosis, polycystic kidneys, and congenital glaucoma: a new autosomal recessive syndrome? Am J Med Genet A 122: 269–273
83 Sellick GS et al. (2004) Mutations in PTF1A cause pancreatic and cerebellar agenesis. Nat Genet 36: 1301–1305
84 Schwitzgebel VM et al. (2003) Agenesis of human pancreas due to decreased half-life of insulin promoter factor 1. J Clin Endocrinol Metab 88: 4398–4406
85 Delepine M et al. (2000) EIF2AK3, encoding translation initiation factor 2-α kinase 3, is mutated in patients with Wolcott-Rallison syndrome. Nat Genet 25: 406–409
86 Iyer S et al. (2004) Wolcott-Rallison syndrome: a clinical and genetic study of three children, novel mutation in EIF2AK3 and a review of the literature. Acta Paediatr 93: 1195–1201
87 Senee V et al. (2004) Wolcott-Rallison syndrome: clinical, genetic, and functional study of EIF2AK3 mutations and suggestion of genetic heterogeneity. Diabetes 53: 1876–1883
88 Baud O et al. (2001) Treatment of the immune dysregulation, polyendocrinopathy, enteropathy, X-linked syndrome (IPEX) by allogeneic bone marrow transplantation. N Engl J Med 344: 1758–1762
89 Bennett CL et al. (2001) The immune dysregulation, polyendocrinopathy, enteropathy, X-linked syndrome (IPEX) is caused by mutations of FOXP3. Nat Genet 27: 20–21
90 Chatila TA et al. (2000) JM2, encoding a fork head-related protein, is mutated in X-linked autoimmunity-allergic disregulation syndrome. J Clin Invest 106: R75–R81
91 Wildin R et al. (2001) X-linked neonatal diabetes mellitus, enteropathy and endocrinopathy syndrome is the human equivalent of mouse scurfy. Nat Genet 27: 18–20
92 Wildin RS et al. (2002) Clinical and molecular features of the immunodysregulation, polyendocrinopathy, enteropathy, X linked (IPEX) syndrome. J Med Genet 39: 537–545
AcknowledgmentsWe thank all our colleagues in Exeter (past and present) for their contributions to the literature reviewed here. The assistance of K Colclough during the preparation of the manuscript is appreciated. Our research is supported by the Wellcome Trust (AT Hattersley is a Wellcome Trust Clinical Research Leave Fellow) and the Research and Development Directorate at the Royal Devon and Exeter NHS Foundation Trust (S Ellard). Désirée Lie, University of California, Irvine, CA, is the author of and is solely responsible for the content of the learning objectives, questions and answers of the Medscape-accredited continuing medical education activity associated with this article.
Competing interestsThe authors declared no competing interests.
REVIEW
Nature.indt 1Nature.indt 1 28/11/07 9:46:50 am28/11/07 9:46:50 am