Chronic obstructive pulmonary disease Edited by Chien-Da Huang Physician Educator/Associate...
22
Chronic obstructive pulmonary disease Edited by Chien-Da Huang Physician Educator/Associate Professor Department of Thoracic Medicine and Medical Education Chang Gung Memorial Hospital Taipei, Taiwan Case-Based Learning Case-Based Learning Thoracic Medicine Thoracic Medicine
-
Upload
brenda-alexander -
Category
Documents
-
view
214 -
download
1
Transcript of Chronic obstructive pulmonary disease Edited by Chien-Da Huang Physician Educator/Associate...

Chronic obstructive pulmonary disease
Edited by Chien-Da HuangPhysician Educator/Associate Professor
Department of Thoracic Medicine and Medical EducationChang Gung Memorial Hospital
Taipei, Taiwan
Case-Based LearningCase-Based LearningThoracic MedicineThoracic Medicine
胸腔科案例 -- COPD
• 學習目標• To identify the symptoms and signs of COPD.• To understand the pathophysiology and common causes of COPD.• To identify the significant findings of physical examination in
patients with COPD. • To identify the significant findings of Lab examination in patients
with COPD.• To know about newest version of GOLD guideline • To understand the comorbidity of COPD.• To know the optimal treatment to reduce the rate of acute
exacerbation and to improve life of quality for this patients with very severe COPD?

Case presentation
• 66 year-old male • Chief complaints of this admission
– Aggravated shortness of breath on walking for 1 week– Increased amount of yellowish sputum
• Smoking history more than 30 pack per year, but quitting for 10 years
• Diagnosed as chronic obstructive pulmonary disease about 15 years
• He had experienced three episodes of respiratory failure in this year

Questions to be discussed?
• What are the factors aggravating dyspnea ?
• What are the causes of production of sputum?
• How do you define COPD?
• What is acute or chronic respiratory failure?

Physical examination
Physical examination – Body temperature: 36.5; pulse rate: 121
beats/min; respiratory rate: 27 /min; Blood pressure: 172/81 mmHg
– Ill-looking – Accessory muscle used – Decreased breathing sound in bilateral lung field ,
crackles over LUL– Poor lung expansion over BLL – Lower lower limbs: cold, mild pitting edema

Exercise Intolerance/Dyspnea on exertionExercise Intolerance/Dyspnea on exertion

Poor expansion of diaphragmPoor expansion of diaphragm Accessory muscle use Accessory muscle use
Decreased breathing sound in bilateral lung fieldDecreased breathing sound in bilateral lung field

Decreased lower limb muscle power
Peripheral vasoconstrictionPeripheral vasoconstriction
Lower limbs: vasoconstrictionLower limbs: vasoconstriction
Anti-gravity power of lower limb muscle: poorAnti-gravity power of lower limb muscle: poor
Questions to be discussed?
• What do you find in the video clips? Please explain and discuss
• Make comments or share clinical experience from tutors
Laboratory findings
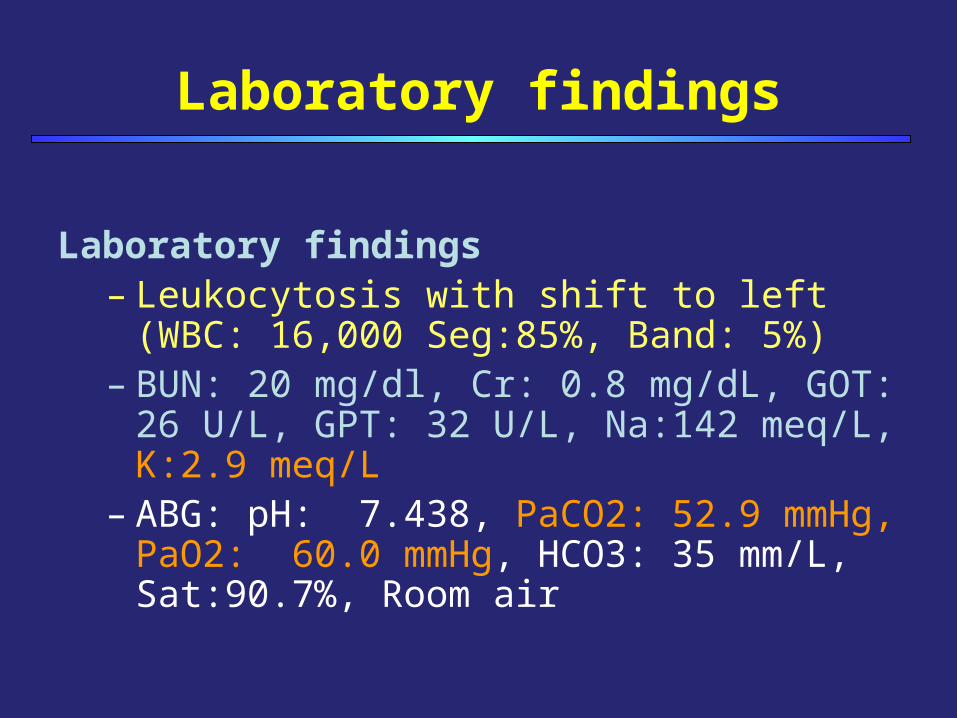
Laboratory findings– Leukocytosis with shift to left (WBC: 16,000
Seg:85%, Band: 5%)– BUN: 20 mg/dl, Cr: 0.8 mg/dL, GOT: 26 U/L, GPT:
32 U/L, Na:142 meq/L, K:2.9 meq/L– ABG: pH: 7.438, PaCO2: 52.9 mmHg, PaO2: 60.0
mmHg, HCO3: 35 mm/L, Sat:90.7%, Room air

Questions to be discussed?
• What are SIRS/sepsis/septic shock?
• Why does the patient get hypokalemia?
• Please discuss the ABG data?

CXR and Sputum culture
• CXR: – LUL alveolar
infiltration– RLL peribronchial
cuffing change• Sputum culture
– Neutrophil 3+– Pseudomonas
aeruoginosa

Questions to be discussed?
• How and what do you read from the CXR?
• How and what do you read the sputum smear and culture from the data?
• What is Pseudomonas aeruoginosa?

FVC: 0.81L (25% pred.) FVC: 0.81L (25% pred.) FEV1: 0.39 L (16% pred.); FEV1: 0.39 L (16% pred.); FEV1/FVC: 48.1%FEV1/FVC: 48.1%FEV1 (BD response <12%)FEV1 (BD response <12%)
2007 GOLD Guideline:2007 GOLD Guideline:
Stage IV:Stage IV:Very severe COPDVery severe COPD
2012 GOLD guideline2012 GOLD guidelineCategory DCategory D
Pulmonary function testPulmonary function test

Questions to be discussed?
• What do you know about newest version of GOLD guideline?
• Try to read the pulmonary function test based on the GOLD guideline?

Medication
• Use of Antibiotics:– Ciprofloxacin 400 mg BID IVF
• Steroids– Oral steroids – Short-term of Hydrocortisone 100 mg iv q6H
• Theophylline 125 mg BID• Procaterol 25 mg/tab1# BID• Nebulization therapy :
– Ipratropium 0.5 mg/UD + Terbutaline 5 mg/UD

MCQ Question 1
The patient complained of aggravated dyspnea during the recovery phase of acute exacerbation in outpatient clinic.
Which factors should be taken into consideration for this patient with very severe COPD?
(A) Mucus retention with 2(A) Mucus retention with 2ndnd infection infection (B) Muscle dysfunction or atrophy(B) Muscle dysfunction or atrophy (C) All of above(C) All of above (D) None of all(D) None of all
Questions to be discussed?
• What are the comorbidities of COPD?

Factor 1: Mucus Retention When there will be mucus retention….
Airway collapse at early expirationAirway collapse at early expiration
Airway inflammation exacerbationAirway inflammation exacerbation
No effective cough functionNo effective cough function due to low inspiratory capacitydue to low inspiratory capacity
New infectionNew infection
Mucus retention is considered for this patient:Mucus retention is considered for this patient:Poor diaphragm movement --- low inspiratory capacityPoor diaphragm movement --- low inspiratory capacityDecreased breathing sound--- mucus plugDecreased breathing sound--- mucus plugPersistent airway inflammationPersistent airway inflammation

Structural changesStructural changes• Fiber size and compositionFiber size and composition• CapillarityCapillarity• Oxidative stress/enzymesOxidative stress/enzymes
Contributing FactorsContributing Factors• HypoxiaHypoxia• HypercapniaHypercapnia• Systemic inflammationSystemic inflammation• MalnutritionMalnutrition• Drugs (steroids, Drugs (steroids, 2 agonist)2 agonist)• Comorbid statesComorbid states (chronic inactivity)(chronic inactivity)
Functional changesFunctional changes• Muscle weaknessMuscle weakness• Reduced oxygen delivery Reduced oxygen delivery and utilizationand utilization
Factor 2:Muscle dysfunction in chronic obstructive pulmonary disease
Balasubramanian Curr Opin Pulm Med 2006; 12:106.Balasubramanian Curr Opin Pulm Med 2006; 12:106.
Muscle Muscle dysfunctiondysfunction
For this patient:For this patient:
Contributing FactorsContributing Factors• HypoxiaHypoxia• HypercapniaHypercapnia• Systemic inflammationSystemic inflammation• Drugs Drugs
•steroids, steroids, •oral or high dose inhaled oral or high dose inhaled 2 agonist)2 agonist)

MCQ Question 2
What is the optimal treatment to reduce the rate of acute exacerbation and to improve life of quality for this patients with very severe COPD? 1. Tiotropium, 2. Inhaled steroid + long-acting b-2
agonist, 3. inhaled long-acting b2 agonist, 4. pulmonary rehabilitation, 5. vaccination, 6. oxygen supplement
(A)(A) 1 + 2 + 5 1 + 2 + 5 (B)(B) 1 + 3 + 5 + 61 + 3 + 5 + 6(C)(C) 1 + 4 + 5 + 61 + 4 + 5 + 6(D)(D) 1 + 2 + 4 + 5 + 61 + 2 + 4 + 5 + 6
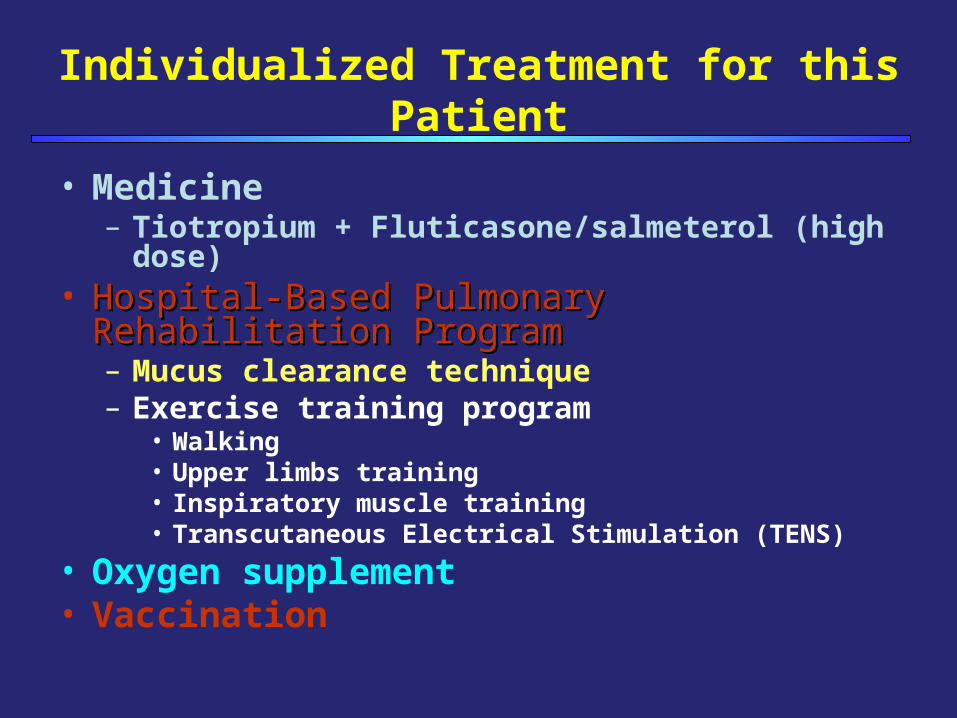
Individualized Treatment for this Patient
• Medicine– Tiotropium + Fluticasone/salmeterol (high dose)
• Hospital-Based Pulmonary Rehabilitation ProgramHospital-Based Pulmonary Rehabilitation Program – Mucus clearance technique– Exercise training program
• Walking• Upper limbs training• Inspiratory muscle training• Transcutaneous Electrical Stimulation (TENS)
• Oxygen supplement• Vaccination