Chest and Lungs 1

of 11
-
Upload
christine-nazareno -
Category
Documents
-
view
233 -
download
2
Transcript of Chest and Lungs 1
-
8/4/2019 Chest and Lungs 1
1/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 1
PHYSICAL DIAGNOSIS
Chest and Lungs Examination
Lecturer: Dr. Feliciano
References: recording, 2010 ppt, Bates, google Sorry medyo mahaba sya ang dami kasi sinabi ni Dr. Feliciano.. Hi Mico haha! Yung iba jan peechures naman lang
so kering keri! Go!
OUTLINEI. CASE PRESENTATION
II. REVIEW OF ANATOMY
-Anterior
-Posterior
-Landmarks
-Lungs
III. PROPERLY POSITION THE PATIENT
IV. UNDRESS THE PATIENT PROPERLY :>
V. INSPECTION
-rate of breathing
-pattern of breathing
-position of the patient
- antero-posterior and lateral diameter of the chest
-chest and spine deformities
-Lung expansion
-extrapulmonary findings
VI. PALPATION
-lymph node
-trachea
-chest
-palpate for mass and tenderness
-assessing for asymmetry of lung expansion
-tactile fremitus
-unilateral diminished fremitus
-bilateral diminished fremitus
VII. PERCUSSION
-level of diaphragm
-differentiation of notes in percussion
VIII.CERTAIN DISEASES WITH USUAL FINDINGS
Next thing to do: AUSCULTATE, BP, general survey.
Above case is a veryincomplete history. Your physical
examination will depend on the history youll be able to get
from the patient. Remember your title as a clinician when
you are taking the history: You are the HISTORIAN that
means..
Whatever you write down is YOUR story. It is the analysis
of the case with the facts coming from the patient. Do not
just write down what the patient would tell you. You have
to give some of your inputs there and see what is
important/relevant to the assessment you are making.
Going back to the case, you would want to ask more..characterize cough MORE! What aggravates it? What
relieves it? When is the time predilection that the patient
would cough? Is it associated w/ hemoptysis? Fever?
Dyspnea.. How severe? Any medications? In pleuritic chest
pain.. is it localized?
Ask for more information.. sometimes the patient
wouldnt volunteer, then YOU WILL BE THE ONE TO ASK!
Ask forPast Medical History. The case above can manifest
a pulmonary disease as well as systemic disease (cardiac).
Family History. Ask if the patient smokes. Is he a smoker
w/ chronic cough? One of the differentials would be LUNG
CANCER. Ask for history of cancer or other pulmonary
disorder like asthma which can be genetically predisposed
to the patient. Ask Personal/Social History in terms of
occupation history as well.
Review of Anatomy
ANTERIOR
Suprasternal notch- point of reference where trachea
will pass through; where clavicle would attach to the
sternum.. the point where manubrium would start.
Angle of Louis -most prominent area next to
Suprasternal notch; where 2nd
rib would attach. In
tension pneumothorax (air in pleural space), if its too
large causing compression of cardiac
structurebradycarcardia, hypotension, cardiac arrest
Thats a medical emergency so you should
Immediately insert large core needle to release the air
and tension. Insert it at the 2nd INTERCOSTAL SPACE
midclavicular line. Or count 2 intercostals space below..
Case: 57 y/o, 50 pack year smoking
HPI: 1 year PTA- cough intermittent
2 mos PTA- persistent cough, whitish phlegm, anorexia, weight loss
Few days PTA- symptoms progressed, (+) dyspnea, (+) pleuritic chest pain
Transcriber: Peller and Jener
Editor: Cancanoo
Number of pages: 12
-
8/4/2019 Chest and Lungs 1
2/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 2
at the level of 4th
rib/ nipple area(bifurcation of trachea to R and L main bronchus).
the clavicle would block the 1st
intercostals space.2
ndintercostal space-1
stsoft area that you will palpate.
In midclavicular line you could palpate up to 6th
intercostals space. Go obliquely on the lateralfor 7th
, 8th
, 9th
intercostals spaces.
Palpate Xiphoid-where the sternum would end and youll be able to delineate your lung during inhalation.
POSTERIOR
-Spine
-Spinous Process(C7-the most prominent)
-Thoracic vertebrae
-Tip of Scapula(7th rib)
LANDMARKS- these are vertical lines used to locate findings around the circumference of the chest. The midsternal
and vertebral lines are precise; the others are estimated.
Anteriorly:Getthe midpoint of your sternum, draw a perpendicular line, to refer to your MIDSTERNAL LINE.
Approximate the midline of clavicle, draw a perpendicular line: MIDCLAVICULAR LINE.
Posteriorly: In your Spinous process, draw perpendicular line to refer to your MIDVERTEBRAL or SPINAL
LINE. In the lateral surface of scapula, you can have your MIDSCAPULAR LINE. In between your scapula, you
have your INTRASCAPULAR AREA. Below the scapula, is INFRASCAPULAR AREA.
Laterally:ANTERIOR AXILLARY LINE, POSTERIOR AXILLARY LINE , MID-AXILLARY LINE
The anterior and posterior axillary lines drop vertically from the anterior and posterior axillary folds, the
muscle masses that border the axilla. The midaxillary line drops from the apex of the axilla.
Posteriorly, the vertebral line overlies the spinous processes of the vertebrae. The scapular line drops
from the inferior angle of the scapula.
From Bates Note special landmarks: 2nd intercostal space for needle insertion for tensionpneumothorax; 4th intercostal space for chest tube insertion; T4 for lower margin of endotracheal tube
on chest x-ra .
From Bates
Note T7-8 interspace as landmark for thoracentesis.
When the neck is flexed forward, the most
protruding process is usually the vertebra ofC7. If
two processes are equally prominent, they are C7
and T1.
-
8/4/2019 Chest and Lungs 1
3/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 3
LUNGS- divided into lobes. Each lobe is divided into segments.
RIGHT LUNG(3 lobes)
Right Upper Lobe: Apical, Anterior, Posterior
Middle Lobe: Medial, Lateral
Posterior Lobe: Superior basal, Antero-lateral
basal, Posterior basal, Medial basal
LEFT LUNG
Upper Lobe: Apicoposterior, Anterior, Superior and
Inferior Lingula
Lower lobe: Superior basal, anteromedial basal, lateral
basal, posterior basal
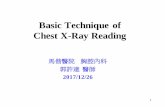
Figure 1. Anterior view
Anteriorly, the apex of each lung rises approximately 2
cm to 4 cm above the inner third of the clavicle. The
lower border of the lung crosses the 6th rib at the
midclavicular line and the 8th rib at the midaxillary line.
Posteriorly, the lower border of the lung lies at about
the level of the T10 spinous process. On inspiration, it
descends farther. See right figure
Each lung is divided roughly in half by an oblique (major)
fissure. This fissure may be approximated by a string that
runs from the T3 spinous process obliquely down and
around the chest to the 6th rib at the midclavicular line.
The right lung is further divided by the horizontal (minor)fissure. Anteriorly, this fissure runs close to the 4th rib
and meets the oblique fissure in the midaxillary line near
the 5th rib. The right lung is thus divided into upper,
middle, and lower lobes. The left lung has only two lobes,
upper and lower. See left figure
-
8/4/2019 Chest and Lungs 1
4/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 4
You can identify problems on RIGHT UPPER LUNG(RUL) and RIGHT MIDDLE LOBE(RML), partly RIGHT LOWER LOBE(RLL) ; LEFT
UPPER LUNG and partly LEFT LOWER LUNG
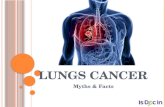
Figure 2. Posterior view:
Partly Left Upper Lung and
Right Upper Lung; Better
appreciation of Left Lower
Lung and Right Lower Lung
Figure 3. Right Lateral view: Right Upper
Lung, Right Middle Lung, Right Lower Lung
divided by OBLIQUE and HORIZONTAL fissure
Figure 4. Left lateral view: LeftUpper lung and Left Lower
lung, divided by OBLIQUE FISSURE
PROPERLY POSITION THE PATIENT: might affect your findings so be cautious about it
Patient: SITTING OR STANDING - so you can examine the anterior and the back(posterior) of the patient
Babies: supine position
Doctors: do not stand in front of your patient! FOR YOUR OWN PROTECTION and HYGIENE PURPOSES. Also if the
patient is female, awkward if guy yung doctor tapos nasa harap dibuh (KINKY!)
UNDRESS THE PATIENT PROPERLY (KINKIER!) narinig ko si Rayson at Mico nag-ohhhh
For Male patient, its not a problem
For some who do not want that, allow them to undress themselves and examine the chest directly WITHOUT their
clothes on. (DO NOT AUSCULTATE WITH THE PATIENTS CLOTHES ON.. Remove all obstructions)
In females, ask them to retract their breast (ask permission first) so you can auscultate the chest.
If patient is really that sick, examine them in SUPINE POSITION.
I. INSPECTION
1. Checking Respiratory rate
Dont stare at the patients chest (might be anxious and change his/her manner of breathing).
You can talk to the patient or get the pulse while counting the RR
RR Adults Normal RR - 16-20 breaths/min (Tachypnea-higher; Bradypnea-lower)
RR on Normal Pediatric patients - higher RR
-
8/4/2019 Chest and Lungs 1
5/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 5
2. Pattern of Breathing
While the patient is standing/lying/seated upright at the end of the examing table or bed.
Usual pattern: diaphragm goes down, chest goes anteriorly and upward (inspiratory movement)
Normal Tidal volume(during resting respiration) on average is 500 mL(if patients 50 kg). Depends on the
weight. [TV= 10-15 ml/kg]
If the patient is smaller, smaller tidal volume
Hyperpnea rapid, deeper breathing metabolic acidosis, anxiety, excercise,hypoxia
Hypopnea shallow or less of breathing
Tachypnea Rapid, shallow, > 20/min Fever, pain, exertion, anemia, infection
Bradypnea slow breathing, < 12/min Uremia, diabetic coma, morphine andalcohol abuse
Kussmaul respiration hyperpneic breathing/polypnea; deep,regular, sighing respiration can be fast,normal or slow
Pneumonia, ESRD, Diabetic KETOacidosis,uremia)
Cheyne-Stokes -Regulary irregular: apnea(absence ofbreathing for more than 10 secs),
hypopnea, hyperpnea, hypopnea, apnea in
cycle;
**Trivia: Why Cheyne-Stokes? Best described by
Cheyne a kind of breathing pattern cease of 10
secs, became perceptible though very low, and
became hyperpnea, and gradually ceases
again(apnea)
-UREMIA
-Congestive heart failure(failing heart so
blood flow to brain is slower, then feedback
mechanism is affected and delayed kaya may
hypopnea, hyperpnea, hypopnea, hyperpnea
- brain injuries, metabolic encephalopathy
- common in children
Biots Breathing -Irregularly regular; Not periodic.-Sometimes slow, sometimes rapid.
Sometimes superficial. Sometimes deep;
without any constant relation of
succession between the two types; with
pauses following irregular interval
preceeded and often following by a sigh,
more or less prolonged;
-very irregular: hypopnea, hyperpnea,
hypopnea, hypopnea, hypopnea,
hyperpnea, apnea
-group of quick, shallow inspiration
followed by regular or iregular period of
apnea
MENINGITISCerbro vascular disease
Cranial tumors
generally indicates poor prognosis
Position of the Patient
Patient with COPD(problem with Expiration)- even they prolong the
expiratory phase, it stops because of bronchus closure. So theres incomplete
evacuation of air CO2 retention and hyperinflation; the air can get it but
once the patient exhales, it easily collapses blocking the exit of air
Di makalakad
Arms is resting on his legs: TRIPOD POSITION
Patients Lips: Pursed Lip Breathing(seen with patient w/ Obstructive Lung
Disease) they do not even know that this helps their breathing by creating
POSITIVE PRESSURE that would keep your airway open during expiration
phase; defense mechanism
Depression of supraclavicular fossa-very prominent in chronic lung disease(e.g. Asthma)
Retractions on Intercostal space
The patient is in respiratory distress(general survey), pursed lip breathing, supraclavicular fossa depression,
intercostals retraction, in a patient in Tripod position
3. Measure Antero-Posterior and Lateral Diameter of the Chest
-
8/4/2019 Chest and Lungs 1
6/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 6
Normal ratioAP diameter: Lateral Diameter1:2 to 1:3(adults, bawal ang barrel chest); 1:1(pediatrics, ang
barrel chest okay lang sa baby)
Dont just say the patient is obese!!! Take note of the history! A patient with Bronchitis, AP diameter is 1:1 due to
bronchitis (not just due to obesity).
Check for defects or deformities
Pectus Excavatum funnel chest- Depression of lower aspect of the sternum;
common in shoemakers in olden times, they press the shoes in their chest;
abnormal in patients who had Rachitic Rosaryand Marfan Syndrome(congenital)
Rachitic Rosary: manifestaion of Vit D deficiency or problem with
the receptors of Vit D; nutritional in origin; prominence of
costosternal notch; bulging ear like beads thats why it is called
Rachitic rosary); seen in patient 1 to 2 years with Rickets
**Complication: Pectus Excavatum funnel chest
Marfan Syndrome(termed as arachnodactyly but not all patients manifest) long bones, long
skull with Pectus Excavatum; autosomal dominant genetic predisposition
Pectus Carinatum birds chest/pigeons breast/chicken
breast-
softened upper ribs bend inward, forcing the
sternum forward
complication of Rickets, Pagets Disease,
congenital Heart Diseases.
Can develop if epiphysis is still open, up to age
18(females) and 21(males)
Kyphosisexaggeration of the posterior curvature of the back.
Most common: osteoporosis
causes the patient to bend forward
Scoliosis
di pantay ang shoulders at fat fold. Ask the patient to bend
forward to really see (Adams Forward Test)
if you have Chronic Obstructive Lung Disease, this will
cause Restrictive Lung Diseases - lower Tidal Volume,
lower reserve volume, lower total lung capacity, all
inspiratory capacities will be low difficulty of breathingit can also compress cardiac structure cardiac
abnormalities.
Chondrosarcoma
malignancy of the rib or bone
more severe form
describe the lesion, measure the circumference
if it has ulceration(typical of malignancy)
Empyema necessitans - pus draining out of the chest wall;complication of tuberculosis
TB lymphadenitis Scrofula- TB of lymph node
4. Lung Expansion Flail chestdue to multiple rib fracture
common in patient with Atelectasis
when the patient inhales, the chest retracts. When the patient exhales, the chest bulges(opposite of normal)
abnormal pattern of breathing
-
8/4/2019 Chest and Lungs 1
7/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 7
5. Observe Extrapulmonary findingsPuffy face-prominence of superficial vessels(due to obstruction of Superior Vena Cava associated with
lung mass, lymph node enlargement in mediastinal area, COPD patient)
Cyanosis-heart failure(congenital heart disease and patients with hypoxia); Hb level lower than 3 g/dl
Peripheral-most common etiology when you expose your hands to cold (Reynauds
phenomenon); common in patient with Connective Tissue diseases
Central
Clubbing of fingers-decrease in oxygenationneovascularization at the tip of fingertip; sign of chronic
illness due to cardiac or lung diseases, or even tumors.
II. PALPATION
Lymph node
One at a time only! You can kill the patient if
theres a problem in carotid artery and you
compress it
Guide: start with pre-auricular, post-auricular,
submandibular, submental, anterior and
posterior cervical, supraclavicular area or the
other way around.
Trachea
palpate the sides
It should be goind down straight.
If theres deviation, either contralaterally if
theres mass, effussion, or even pneumothorax.
Most common is goiter pushing the trachea on
the other side.
In Atelectasis, the trachea will deviate
ipsilaterally.
Chest
palpate anteriorly and posteriorly.
Check if theres a mass and tenderness.
Palpate the ribs and intercostal space
if you have any pleural involvement like in
pleurisy/pleuritis (inflammation of the pleura),
you can only elicit a pain whenever you try to
palpate the intercostal spaces
If you palpate on the rib and there is a pain on
the rib, then that would be due to a rib problem
and not necessarily a pulmonary problem. Do
this in front or at the back of your patient.
Assessing for Asymmetry of Lung Expansion
by checking respiratory excursion: best done at
the BACK of the patient.
place your hands at 10th
intercostal space
(3 intercostal spaces below the tip of the
scapula as your reference)
your thumb should be positioned in the
paravertebral area
You have to be on fold and ask the
patient to inhale, exhale(This is not the
proper way but a better way of doing it)
Let the patient move your hand. If there
is symmetry, then that is symmetrical
chest expansion.
You can also do that in the anterior chest
usually at the level of 6th
intercostal
space. You do the same technique.
You can also do that on your upper chest
but do not press too much on your
brachial.
For the patient who cannot sit up, you
can also do that while your patient is on
supine position.
Asymmetrical Lung expansion
Problems on the side borders pathology
There would be a lag if there is a pleural
effusion, pneumothorax or large mass in
that area
If theres no mass, effusion nor
pneumothorax, possible cause is
In summarry for INSPECTION
Respiratory rate
Breathing pattern
(+)/(-)intercostal retractions/ use of accessory muscles
(+)/(-)Deformities or defects
(+)/(-)Mass or lesions
Symmetry in inhalation/expiration
Extra pulmonary findings- cyanosis, clubbing, increase vascularity of superficial veins, puffy face
Cyanosis is of two kinds, depending on the oxygen level in the arterial blood. If this level is low,
cyanosis is central. If it is normal, cyanosis is peripheral. Peripheral Cyanosis occurs when
cutaneous blood flow decreases and slows, and tissues extract more oxygen than usual from the
blood. Peripheral Cyanosis may be a normal response to anxiety or a cold environment.
-
8/4/2019 Chest and Lungs 1
8/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 8
diaphragmatic paralysis (since diaphragm
is the major muscle in respiration).
Tactile Fremitus
The last you have to do with palpation
Ask the patient to say ninety-nine, tres, tres,
for as long as that the frequency of what you
would ask the patient to say is the same
frequency as the chest wall and the lungs.
For females with high frequency or high pitches,
expect that the fremitus might be decreased or
not appreciable at all. Ask the female to lower
down the pitch or voice to appreciate the lung
fremitus.
Certain points to consider:
Usually the first point of examination is your
supraclavicular area then down to your
intercostal space and then obliquely downward
to these points (zigzag pattern).
You can do it one at a time or at the same time
depending on your preference.
When examining the back, ask the patient to
place the hands on the shoulder to retract the
scapula so you would have more space to palpate,
percuss or auscultate. You have to place the baller
surface of palm or ulnar surface of your hands.
Best sensed by using the palmar bases of the
fingers applied on the chest wall
The intensity is dependent on tissue densityFeel for vibration. When you ask the patient to say
tres tres or ninety-nine, your vocal cords will
vibrate and will send vibrations towards your
bronchus, to your parenchyma and your chest
wall.
Remember your hand should be placed in the
intercostal space.
Normal is equal vocal fremitus.
Abnormality in fremitus can be seen in
consolidation that can be appreciated in patient
with Pneumonia because of increase in secretion
in alveoli due to the inflammatory mucus and cells
that would increase density of the lungs allowing a
better transmission of that vibration from your
lung parenchyma toward the chest wall. This is the
only one that can increase the fremitus.
The rest of the abnormality will diminish the
fremitus.
o Unilateral diminished fremitus
Pleural effusion of one side.
Fluid will block the transmission of
vibration from your lung parenchyma
towards your chest wall.
Same is true if there is a pleural
thickening or a big tumor with
obstruction. If you have only tumor and
the tumor is located 5-6cm away from
the chest wall, it might not manifest
with anything at all. it might notmanifest any physical findings.
Atelectasis (collapse of lung) will also
decrease the fremitus, as well as
pneumothorax.
o Bilateral diminished fremitus
You can probably appreciate among
the patient with excess fat tissues
(it is quite difficult to appreciate
fremitus) thats acceptable, report that
the fremitus cannot be appreciated or
diminished but be sure that this is dueto obesity or excessive fat tissues.
Air trapping which is common among
patients with COPD, asthma or any
obstructive lung disease, because of
that, there would be bilateral decrease
in fremitus as well.
III. PERCUSSION
use the dominant hand as a plexor if right
handed, use the right hand as a plexor
the other hand would be your pleximeter.
So your pleximeter is usually your non-
dmoninant hand, you have to press it in the
intercostal space, and then you have to tap
it with your plexor.
the force should come from the wrist and
not from you elbow. You should do a 1-3strikes to appreciate the sounds created by
percussion.
The lung percussion note is resonance.
Heartand liveris dull. Stomach is tympanic.
Thigh is flat. Again, you have to do
percussion same as earlier (zigzag pattern).
Do not forget to percuss the lateral chest.
Be sure to cut your nails (long nails can be
painful in percussion).You can do it in supine position. But the
vibration might be dumped when doing in
supine. It is more audible when you do it in
a sitting position and there is a better
resonance on your apex rather than on the
base and it is highly appreciated on the
right intercostal area.
-
8/4/2019 Chest and Lungs 1
9/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 9
At the back, you have to do that on your
vertebra and scapula, again, ask the patient
to retract the scapula (by putting his hands
on his shoulders).
To check the level of the diaphragm
o You can check it during the resting
expiration.
o Ask the patient to exhale, tap it quickly, and
note for resonance, and if there is dullness
you can appreciate, then that is the level of
your lung.
o And then ask the patient to inhale then tap
it again and you will expect it to go down.
o The difference should be around 4-6cm
thats the normal excursion of your lung.
You would also expect your right side to be
more elevated than your leftbecause of the
presence of the liver (they call this the Alley
of percussion)
Differentiation of notes in percussion (Technically)
The definitions of notes are arbitrary. But it can be
differentiated in terms ofpitch, intensity and quality
FLATNESS is usually high-pitched with soft intensity
and it is really dull (normally in thigh, sternum)
You can also appreciate if there is atelectasis or
pleural effusion.
DULLNESS has medium pitch and intensity and tad-
like quality. Normal in liver, cardiac and diaphragm.
Abnormal if you have pneumonia, tumor, Atelectasis
and even pleural effusion.
RESONANCE is the normal sound of your lung, it is
low, moderate to loud intensity and hallow in
quality. But you can also have hyperresonance as
normal sound among children or infants.
HYPERRESONANCE has lower pitch than resonance
sound, very loud intensity, booming in quality. In
abnormal diseases like pneumothorax, asthma,
chronic bronchitis and emphysema.
TYMPANIC SOUND is a high-pitched, loud intensity,
with drum-like or musical quality, well appreciated in
the asthma but it is also suggest a presence of
pneumothorax.
If you have difficulty in hearing the sound of
percussion, it is not the force of your plexor that
matters. You can actually apply more pressure with
your pleximeter before you try to percuss.
Certain Diseases with usual findings
Asthma
Reversible obstructive lung disease that is usually
caused by atopy or allergy or triggered by certain
allergens. And just like any obstructive lung disease, you would
expect to have air trapping thats why if you have
air-trapping, you have hyperinflation, you would
expect to have hyperresonance upon percussion.
In inspection, you would see the patient is dyspneic,
using of accessory muscles upon breathing, and
cyanosis.
On palpation, it is often normal but it might cause a
decrease in fremitus as well. Aside from being
hyperresonance, you will have a low lying diaphragm
as well.
Emphysema
Another obstructive lung disease.
You would expect to have increase in AP diameter,
use of accessory muscles, and the patient would
appear relatively thin. (LIKE ME :p)
Emphysema in chronic bronchitis is part of your
COPD (Chronic Obstructive Pulmonary Disease).
oThe only thing that we try to do is to probably
say that the COPD is predominantly emphysema
or predominantly bronchitic.
oMore often, both these things happen in a
patient with COPD.
The patient with emphysema would have decreased
fremitus, increase resonance, and decreased
excursion of the diaphragm.
Chronic Bronchitis
Present with cyanosis, they are short and stacky
Often with normal palpation and percussion.
Pneumothorax
Air in the pleural space.
Often normal or may have a lack on the affected
side.
It is normal if there is only minimal pneumothorax.
In summary, in percussion, you will report
the normal findings as resonance on all lungfield except on the area of cardiac dullness.
If you report otherwise, then it indicates
some other diseases.
-
8/4/2019 Chest and Lungs 1
10/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 10
On palpation, there might be absent fremitus and if
there is tension pneumothorax, you will appreciate
deviation of your trachea to your contralateral side.
On percussion, it is hyperresonant.
Pneumonia
Common infection of the lung parenchyma.
The patient may present with possible cyanosis, and
splinting on the affected side, increased fremitus,
dullness on percussion.
Theres a special resonance that can be appreciated
(also in patient with pneumohydrothorax) skodaic
resonance or tympany.
o you would have dullness in the area and
have consolidation but just above it you
would appreciate hyperresonance or almost
tympany.
o It can also appreciated inpneumohydrothorax where you have both
air and fluid in the pleura.
In the area where you have fluid,
you have dullness. The area where
you have air in the pleura, you will
have hyperresonance or tympany
upon percussion.
Pleural Effusion
Usually present with lag on affected side or if it is
minimal it can have normal lung expansion.
On palpation, you would have a decrease infremitus, and the trachea is shifted to the
contralateral side.
On percussion, it would be dull.
Atelectasis
It can be normal if there is only a segmental
atelectasis but if it is a lobar atelectasis or atelectasis
of the whole lung then you would expect lag on the
affected side, decrease in fremitus and shifting of
the trachea to the affected side or ipsilaterally.
There is dullness on percussion.
Acute Respiratory Distress Syndrome (ARDS)
Upon inspection, the patient is using accessory
muscles upon breathing and cyanosis, but the
percussion and palpation may be normal.
Pulmonary Embolism
normal physical examination. You would need to
have a good clinical eye. Probably look for risk
factors. And have a high index of suspicion before
you make a diagnosis of pulmonary embolism.
Pulmonary edema or congestion
It might also have inspection but in severe
congestion you might have dyspnea.
Upon palpation and percussion it would be normal.
There might have fine crackles when you have
congestion.
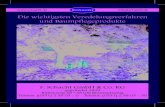
On the left, anterior sequence of percussing the chest while on
the right picture shows posterior examination of the chest
Relativeintensity
Relativepitch
Relativeduration
location Examples
Flatness Soft high Short Thigh Pleural effusion
Dullness Medium Medium Medium Liver Lobar
pneumonia
Resonance Loud Low Long Normal lung Chronic
bronchitis
Hyperresonance Very loud Lower longer None Emphysema,
pneumothorax
tympany loud High Gastric air
bubble
Large
pneumothorax
-
8/4/2019 Chest and Lungs 1
11/11
PHYSICAL DIAGNOSIS : Chest and Lungs | 11
Differentiation of Common Pulmonary Conditions
Condition Inspection Palpation Percussion Auscultation
Asthma Dyspnea; use of
accessory muscles;
poss. Cyanosis;
hyperinflation
Often normal,
decreased fremitus
Often normal;
hyperresonant; low
diaphragm.
Prolonged
expiration; wheezes;
decreased lung
sounds
Emphysema Increased AP
diameter; use of
accessory muscles;
thin
Decreased fremitus Increased
resonance;
decreased excursion
of diaphragm
Decreased lung
sounds and vocal
fremitus
Chronic Bronchitis Poss. Cyanosis;short, stocky
Often normal Often normal Early crackles;rhonchi
Pneumothorax Often normal; lag on
affected side
Absent fremitus;
trachea shifted to
contralateral
Hyperresonant Absent breath
sounds
Pneumonia Poss. Cyanosis and
splinting on affected
side
Increased fremitus Dull Late crackles;
bronchial breath
sounds
Pleural Effusion Often normal; lag on
affected side
Decreased fremitus;
trachea shifted to
contralateral
Dull Absent breath
sounds
Atelectasis Often normal; lag on
affected side
Decreased fremitus;
trachea shifted to
ipsilateral
Dull Absent breath
sounds
ARDS Use of accessory
muscles; cyanosis
Usually normal Often normal Normal initially;
crackles and
decreased lung
sounds
Pulmonary
Embolism
Often normal Usually normal Usually normal Usually normal
Pulmonary Edema Often normal Often normal Often normal Early crackles;
wheezes
-END-
Hi batchmates! Galingan natin!
Thank you Jener sa pagtulong sakin sa last 20 mins of recording.. Nakakapagod tranx na to hmp!
Pag may tanong kayo guys, or tingin nyo na mali sabihin nyo lang.. or dedma haha! Goodluck satin!
Number of noh?: 133