Basics of Mechanicall Ventilationl · PDF fileThe ventilator settings (see advance course for...
63
Basi Basi Mechanical Mechanical Mechanical Mechanical cs of cs of l Ventilation l Ventilation l Ventilation l Ventilation
-
Upload
truongmien -
Category
Documents
-
view
231 -
download
2
Transcript of Basics of Mechanicall Ventilationl · PDF fileThe ventilator settings (see advance course for...

BasiBasiMechanicalMechanicalMechanicalMechanical
cs of cs of l Ventilationl Ventilationl Ventilationl Ventilation

Objec
To understand:How positive pressure ventila
• Reduce the work of breathing
• Restore adequate gas exchange• Restore adequate gas exchange
The basics of • Invasive positive pressure ventilat• Noninvasive positive pressure ven
The principles of bedside mo• Pressure and volume alarmsPressure and volume alarms• Flow and pressure time curves
ctives
ation helps
tion (IPPV) ntilation (NIPPV)
onitoring

Physiopathology of RPhysiopathology of R
ResistanceAW
Δ VA/Δ VA/
Work of Br
Fatig
HypercaHypoxemia AW=Airrway; R=respiratroy system; VE = minute ventilation, VO
Respiratory Failure30Respiratory Failure30
ComplianceR
/Q/Q
VO2
eathing VE2
VCO2
pH
gue Neuromusculardisorders
apnia O2 = Oxygen consumption, VCO2=carbon dioxide production

Indications and RationIndications and RationUnprotected and unstable airways• Intubation and IPPV allows to
- Secure the airwaysy- Reduce the risk of aspiration - Maintain adequate alveolar ventilation
Hypercapnic respiratory acidosis• IPPV and NIPPV
- Reduce the work of breathing and thusrecovery when fatigue is already prese
- Maintain adequate alveolar ventilationMaintain adequate alveolar ventilation
Hypoxic respiratory failure• IPPV and NIPPV help correct hypoxem
- Deliver a high FiO2 (100% if needed dg 2 (- Reduce shunt by maintaining flooded o
Others• Intubation to facilitate procedure (bron
nale for Initiating IPPVnale for Initiating IPPVs (e.g,, coma)
s prevents respiratory muscle fatigue or speeds ent(prevent or limit respiratory acidosis as needed)(prevent or limit respiratory acidosis as needed)
mia as it allows to during IPPV) g )or collapsed alveoli open
nchoscopy), bronchial suctioning

Important Pitfalls and Important Pitfalls and withwithwith with
Potential detrimental effects ass• Heart and circulation
- Reduced venous return and afterload - Hypotension and reduced cardiac outpu
L• Lungs - Barotrauma- Ventilator-induced lung injury- Air trappingpp g
• Gas exchange - May increase dead space (compressio- Shunt (e.g., unilateral lung disease - the
associated with PPV tends to redirectassociated with PPV tends to redirect
Problems Associated Problems Associated PPVPPVPPV PPV
sociated with PPV
ut
n of capillaries) e increase in vascular resistance in the normal lung blood flow in the abnormal lung)blood flow in the abnormal lung)

Important Effects of PImportant Effects of PDecreased preload
• Positive alveolar pressure ↑ lung volumethe intramural pressure of the heart cavippreload is reduced stroke volume dec
drop. This can be minimized with i.v. fluid, wpreload.
P ti t h iti t h i• Patients who are very sensitive to change ihypovolemia, tamponade, PE, severe air twhen PPV is initiated.
Reduced afterloadReduced afterload• Lung expansion increases extramural pres
and thereby reduces LV afterload.
• When the cardiac performance is mainly de• When the cardiac performance is mainly deconditions (e.g., hypervolemic patient with an improved stroke volume. PPV is very heedema, as it helps to reduce preload (lung volume tends to increasevolume tends to increase.
PV on HemodynamicsPV on Hemodynamics
e compression of the heart by the inflated lungs ities rises (e.g., ↑ RAP) venous return decreases ( g , ↑ )creases cardiac output and blood pressure may which helps restore adequate venous return and
i l d diti ( fin preload conditions (e.g., presence of trapping) are particularly prone to hypotension
sure (which helps pump blood out of the thorax)
etermined by changes in afterload than in preloadetermined by changes in afterload than in preload systolic heart failure), PPV may be associated with elpful in patients with cardiogenic pulmonary congestion) and afterload. As a result stroke

Effects of PPV onEffects of PPV on
Generally speaking, the effects oftransmural pressures vary in paratransmural pressures vary in para
• Airway pressure (e.g., ↑ air• Lung compliance (e.g., ↑ co• Chest wall stiffness (e.g., in th
pressure ahemodynaheart is goheart is gocompliant
Marini, Wheeler. Crit Care Med. The E
n Hemodynamicsn Hemodynamics
f PPV on the cardiac chamber allel with:allel with: rway pressure → ↓ venous return)
ompliance → ↓ venous return)he obese patients, a given change in airway and lung volume will have more impact on the amics, given that the pressure rise around the oing to be higher than in patients withoing to be higher than in patients with t chest wall, everything else being equal)
Essentials. 1997.

Alveolar Pressure Alveolar Pressure
ffec
tssi
ty o
f the
ef
Inte
ns
Alveolar PreAlveolar Pre
Note that as airway pressure increasesPEEP [positive end-expiratory pressurPEEP [positive end expiratory pressur
• Oxygen transport start to decline despite th• Dead space also tends to increase due to
pressure, creating ventilated but poorly pe
Adapted from: Marini, et al. Crit C
and Gas Exchangeand Gas Exchange
PaO2
Dead space
Oxygen transport
essureessure
s above a certain level (e.g., high re]):re]):he rising PaO2 as cardiac output starts falling.compression of alveolar capillaries by high alveolar
rfused alveolar units.
Care Med. 1992.

Other Potentially AdversOther Potentially AdversVentiVentiVentiVenti
Excessive airway pressure and tid(ventilatorinduced lung injury) an(ventilatorinduced lung injury) an
Lungs of dogs ventilated for a few hours with large tidal volume demonstrate extensive hemorrhagic
injury.
se Effects of Mechanical se Effects of Mechanical lationlationlation lation
dal volume can lead to lung injury nd contribute to increased mortalitynd contribute to increased mortality.
The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301-1308.

Other Potentially AdversOther Potentially AdversVentiVentiVentiVenti
In the setting of obstructive physioadjustment of the tidal volume andnormal pH and PaCO2 can lead to
severe hy
Up
Th
1.22.
3.
Tuxen et al. Am Rev Resp Dis 198
se Effects of Mechanical se Effects of Mechanical lationlationlation lation ology (e.g., asthma and COPD), d rate minute ventilation to restore a o air trapping, pneumothoraces, and ypotension.
pper Panel: When airway resistances are high, there is for a few breath more air going in than coming out of the lungs (dynamic hyperinflation). Subsequently, a new equilibrium is reached. The amount of air trapped can be estimated in a passive patient by discontinuing ventilation and collecting the expired volume (lower
l)panel).
he volume of trapped gas is largely determined by:
The severity of airway obstructionThe ventilator settings (see advance course for details) Of all theThe ventilator settings (see advance course for details). Of all the settings, the imposed minutes ventilation (set rate x VT) and the most important one. The time left between tidal breath for exhalation is less important if a low VT and VE are targeted.
87;136:872.

Positive PressuPositive PressuThe EquatioThe EquatioThe EquatioThe Equatio
In a passive subject, airway pressure racross the respiratory system. p y yThe work required to deliver a tidal brepressureThe pressure (P) associated with the dp ( )simplified equation of motion of the res
P = VT/CR+ VT/Ti xT R T
P elastic P res
Where CR = compliance of the respiratory system, Ti = inspiratory tiPEEP total = the alveolar pressure at the end of expiration = externaextrinsic (PEEP dialed in the ventilator) adds to the inspiratory pressure
P elastic P res
ure Ventilation: ure Ventilation: on of Motionon of Motionon of Motionon of Motionrepresents the entire pressure (P) applied
eath (Wb) = tidal volume (VT) x airway
delivery of a tidal breath is defined by the y yspiratory system (lungs & chest wall):
x RR + PEEP totalR total
istive P elastic
me and VT/Ti = Flow, RR = resistance of the respiratory system and al PEEP + auto (or intrinsic) PEEP, if any. Auto PEEP = PEEP total – P e one needs to generate a tidal breath.
istive P elastic

Work of BWork of B
Work per breath is depicted as a presWork per breath (Wbreath) = P x tidal voWork per breath (Wbreath) P x tidal voWmin = wbreath x respiratory rate
e e
Volu
me
Volu
me
V T
Pressure Press
The total work of breathing can be partitioned between an elastic and rethrough a straw varies; one needs to overcome the resistance of the str
BreathingBreathing
sure-volume areaolume (VT)olume (VT)
e W i ti k
WEL = elastic work
Volu
me WR = resistive work
sure Pressure
esistive work. By analogy, the pressure needed to inflate a balloon raw and the elasticity of the balloon.

Intrinsic PEEP andIntrinsic PEEP and
When present, intrinsic PEEP contribbe offset by applyi
Volu
me
V T
FRCPressur
PEEPi = intrinsic or auto PEEP; green triangle = tidal elastic work; redoffsetting intrinsic PEEP (an expiratory driver) during inflation
d Work of Breathing d Work of Breathing
butes to the work of breaking and can ing external PEEP.
V T
rePEEPi
Dynamic Hyperinflation
d loop = flow resistive work; blue rectangle = work expended in

The Pressure and Work ofThe Pressure and Work ofProvided by the VentiProvided by the VentiProvided by the VentiProvided by the Venti
++₊₊
f Breathing can be Entirely f Breathing can be Entirely lator (Passive Patient)lator (Passive Patient)lator (Passive Patient)lator (Passive Patient)
VentilatorVentilator
++₊

Work of Breathing UndWork of Breathing Und
When the lung is inflated by constant flow timeWhen the lung is inflated by constant flow, timethe monitored airway pressure tracing (Paw) reinspiration. A pressure-sensing esophageal balthe pleural space and therefore the work of che
der Passive Conditionsder Passive Conditions
e and volume are linearly related Thereforee and volume are linearly related. Therefore, eflects the pressure-volume work area during loon reflects the average pressure change in
est wall expansion.

The Work of Breathing caThe Work of Breathing caVentilator anVentilator anVentilator anVentilator an
The ventilator generates positive pressinspiratory muscles generate negainspiratory muscles generate nega
Paw = Airway pressure, Pes= eso
an be Shared Between the an be Shared Between the nd the Patientnd the Patientnd the Patient nd the Patient
sure within the airway and the patient’s ative pressure in the pleural space
PAC mode
ative pressure in the pleural space.
PAW
i hipatient machine
PES time
ophageal pressure

Relationship Between thRelationship Between thLevel and the PatienLevel and the PatienLevel and the PatienLevel and the Patien
Carrey et al. Chest. 1990;97
he Set Pressure Support he Set Pressure Support nt’s Breathing Effortnt’s Breathing Effortnt s Breathing Effortnt s Breathing Effort
The changes in Pes (esophageal pressure) and in the diaphragmatic activity (EMG) i t d(EMG) associated with the increase in the level of mask pressure (Pmask =pressure (Pmask = pressure support) indicate transfer of the work of breathingthe work of breathing from the patient to the ventilator.
7:150.

Partitioning of the WorkloPartitioning of the Workloand theand theand theand the
How the work of breathing partitions betwdepends on:depends on:
• Mode of ventilation (e.g., in assist control mo• Patient effort and synchrony with the mode o• Specific settings of a given mode (e.g., level p g g ( g
oad Between the Ventilator oad Between the Ventilator e Patiente Patiente Patiente Patient
ween the patient and the ventilator
ost of the work is usually done by the ventilator)of ventilation
of pressure in PS and set rate in SIMV)p )

Common ModeCommon Mode
Volume targeted ventilation (flowVolume targeted ventilation (flow• AC
Pressure targeted ventilationPressure targeted ventilation• PCV (pressure controlled, time cycled• PS
Combination modes• SIMV with PS and either volume or pr
es of Ventilationes of Ventilation
w controlled volume cycled)w controlled, volume cycled)
)
essure-targeted mandatory cycles

Pressure and VolumePressure and Volume
In pressure-targeted ventilation: aninspiratory time are set, while flow ap y ,dependent variables.
I l t t d til ti (flIn volume targeted ventilation (flowvolume and flow (or inspiratory timepressure and inspiratory time (or flo
)time is preset) become the depend
The tidal volume is the integral of thThe tidal volume is the integral of thunder the curve of the flow time cu
e Targeted Ventilation e Targeted Ventilation
n airway pressure target and and tidal volume become the
t ll d l l d) t tw-controlled, volume cycled), a target e in certain ventilator) are preset and ow in the ventilator where inspiratory ent variables.
he flow during inspiration = areahe flow during inspiration area rve during inspiration (see next slide).

Pressure and VolumePressure and Volume
Marini, Wheeler. Crit Care Med. The
e Targeted Ventilation e Targeted Ventilation
VT
e Essentials. 1997.

AssistAssist--
Set variables • Volume, TI or flow rate, frequency, flow• PEEP and FIO2
Mandatory breaths• Ventilator delivers preset volume and
Spontaneous breaths• Additional cycles can be triggered by t
mandatory breath.mandatory breath.
--controlcontrol
w profile (constant or decel)
preset flow rate at a set back-up rate
the patient but otherwise are identical to the

SIMSIMKey set variables
• Targeted volume (or pressure target), flow • PEEP FIO pressure support• PEEP, FIO2, pressure support
Mandatory breaths• Ventilator delivers a fixed number of cycle
fAlternatively, a preset pressure is applied f
Spontaneous breaths • Unrestricted number, aided by the selected, y
MVMV
rate (or inspiratory time, Ti), mandated frequency
s with a preset volume at preset flow rate. f ffor a specified Ti
d level of pressure supportp pp

Peak Alveolar and TranPeak Alveolar and TranP(t) = VT/CR+ Flow
+_ _
_ _ _++ +
+ Palveolar
Ppleural
Ptranspulmonary = Palveolar - PpleuralTranspulmonary pressure is a key dTranspulmonary pressure is a key d
nspulmonary Pressuresnspulmonary Pressuresw x RR + PEEP tot
Plateau pressure
Peak Airway Pressure
Alveolar Pressure
meanPaw
Plateau pressure
meanPaw
External PEEPIntrinsic PEEP
Pplat = Maximum Palveolardeterminant of alveolar distensiondeterminant of alveolar distension.

Monitoring PressureMonitoring PressureVentiVentiVentiVenti
Plateau pressure tracks the highesdeterminant of alveolar distensiondeterminant of alveolar distension.
Plateau pressure (Pplat) is, howevedistending pressure (transpulmonag p ( ppressure).• e.g., in a patient with a low chest wall c
associated with a higher pleural pressug p ptranspulmonary pressure) than in a pat
The difference between the Ppeak pressure as dictated by the equatiopressure, as dictated by the equatiopause, flow becomes zero, the resiairway pressure drops from its pea
e in Volume Targeted e in Volume Targeted lationlationlationlation
st tidal alveolar pressure, a key
er, only a surrogate of peak alveolar ary pressure = Pplat – pleural y p p p
compliance, a given Pplat is typically ure but less alveolar distension (smaller (tient with a compliant chest wall.
and Pplat tracks the resistive on of motion During an inspiratoryon of motion. During an inspiratory istive pressure is eliminated and the k to the plateau pressure.

Airway Resistance anAirway Resistance anCompCompCompComp
Under conditions of constabetween peak and plateau end-inspiratory flow. When airflow is stopped inWhen airflow is stopped inpatient by occlusion of theend inspiration (plateau pre(t t l PEEP) th(total PEEP), the pressure elastic recoil of the lungs aof the tidal volume is given
l Di idi th d livalues. Dividing the deliverdifference quantifies the recompliance. p
nd Respiratory System nd Respiratory System pliancepliancepliancepliance
ant flow, the difference airway pressures drives
a passively ventilated a passively ventilated e expiratory circuit valve at essure) and end expiration
d d t thneeded to overcome the nd chest wall during delivery as the difference in these
d tid l l b thired tidal volume by this spiratory system

Mean AirwaMean Airwa
Although measured in the connpressure is a valid measure of tplung and chest wall, averaged aventilatory cycle - but only undeChanges in mean airway pressuChanges in mean airway pressuminute ventilation, PEEP, and IMean airway pressures affect py p pdistention. Therefore, changes in mean airinflation may influence:inflation may influence:• Arterial oxygenation• Cardiac output
ay Pressureay Pressure
ecting circuit, mean airway the pressure applied across the p ppacross both phases of the er passive conditions.ure are produced by changes inure are produced by changes in :E ratio.
pleural pressure and lung p p g
rway pressure during passive

Pressure ControPressure ControKey set variables:
• Pressure, TI, and frequency • PEEP and FIO2PEEP and FIO2
Mandatory breaths• Ventilator generates a predetermined press
Spontaneous breaths• PCV-AC mode: same as mandatory breaths• PCV-SIMV mode: unsupported or PS
Important caveat• It is important to understand that in pressure
rate and minute ventilation is complex. Abovpcreated due to a reduced expiratory time), tdelivered tidal volume.
• A pneumothorax or other adverse change intrigger a high alarm pressure but a low tidaltrigger a high alarm pressure but a low tidal
olled Ventilationolled Ventilation
sure for a preset time
s
e-controlled ventilation the relation between the set ve a certain frequency (e.g., when intrinsic PEEP is q y ( g ,he driving pressure starts to drop--and so does the
n the mechanics of the respiratory system will not volume alarm instead volume alarm instead.

PressurePressure
Pressure = set variable. Mandatory breaths: noneMandatory breaths: none.Spontaneous breaths• Ventilator provides a preset pressure ap p p
specified fraction (typically 25%) of its • Patient effort determines size of breath
e Supporte Support
assist, which terminates when flow drops to a , pmaximum.
h and flow rate.

PCV: Key ParametPCV: Key Paramet
AA
ter to Monitor is Vter to Monitor is VTT
What Causes a Decreased VT During PCV?
Change in mechanics• ↑ airway resistance:
b h
T g
. e.g., bronchospasm• ↓ respiratory system compliance .
.e.g, pulmonary edema, pneumothorax
AutoPEEP ↑AutoPEEP ↑• ↑ expiratory resistance• ↓ expiratory time
e.g., ↑ rateg ,
Inspiratory time ↓• e.g., ↑ rate if I:E ratio constant

AutoAuto--PEEP (IntrinPEEP (Intrin
Note that AutoPEEP is not equivalent to air trapping. Active expira(left panel) to positive press
Marini, Wheeler. Crit Care Med. Th
nsic PEEP, PEEPi)nsic PEEP, PEEPi)
atory muscle contraction is an often under appreciated contributor sure at the end of expiration
he Essentials. 1997.

Suspecting and MeSuspecting and Me
sure
End expirat
Ti
Pres
s
PEE
Pe
Time
AutoPEEP is commonly measured by performing a pause at the end of expiequilibration through the entire system. In such conditions, proximal airway phyperinflation.
easuring AutoPEEP easuring AutoPEEP
Suspect AutoPEEP if flow at the end of expiration does not return to theof expiration does not return to the
zero baseline.
Total PEEP
tory pause
PEEPi
ration. In a passive patient, flow interruption is associated with pressure pressure tracks the mean alveolar pressure caused by dynamic

Interim SummaryInterim Summary
Mechanical ventilation helps to exchange and can provide comexchange and can provide comassistance.Safe and effective implementatiprequires understanding the equsystem.Monitoring dynamic and static aMonitoring dynamic and static avital information for interpreting system and for adjusting machiperformanceperformance.
y and Key Pointsy and Key Points
improve respiratory gas mplete or partial work of breathingmplete or partial work of breathing
ion of mechanical ventilation ation of motion for the respiratory
airway pressures and flows yieldsairway pressures and flows yields the mechanics of the respiratory ne settings for optimal

Mechanical VenMechanical VenExchExchExchExch
RespiratoryHypox
ntilation and Gas ntilation and Gas hangehangehangehange
y acidosisxemia

HypercapnHypercapn
Determinants of PaCODeterminants of PaCO2• PACO2 = 0.863 x VCO2/VA • VA = VE (1-VD/VT)
C f h iCauses of hypercapnia • Inadequate minute ventilation (VE)• Dead space ventilation ↑ (VD/VT)• CO2 production ↑ (VCO2 )CO2 production ↑ (VCO2 )
Corrective measures for respira• When appropriate, increase the minut
volume )o u e )
ic Acidosisic Acidosis
VD = dead spaceVA = alveolar ventilationVE = minute ventilationVT = tidal volumeVCO2 = CO2 productionVCO2 = CO2 production
atory acidosise ventilation (e.g., the rate or the tidal

Mechanism for AMechanism for A
Reduced FiO (e g toxic fumeReduced FiO2 (e.g., toxic fumeHypoventilationImpaired diffusionImpaired diffusionVentilation/perfusion (VA/Q) mis• High VA/Q (∞ = Shunt)• Low V /Q (0 = Dead Space)• Low VA/Q (0 = Dead-Space)
Shunting• If significant shunting is present, the F
Arterial HypoxemiaArterial Hypoxemia
es altitude)es, altitude)
smatching
FIO2 requirement is typically > 60%

Minute Ventilation Minute Ventilation
The relationship between PaCO2 and minuwith hypoventilation, small changes in minthe PaCO2.
and Gas Exchange and Gas Exchange
ute ventilation is not linear. In patients nute ventilation may have large effect on

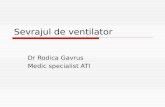
Shunting: EffectsShunting: Effectss of FiOs of FiO22 on PaOon PaO22
Note that as the % of shunt rises, increasing the FIO h l d l i t P OFIO2 has less and less impact on PaO2.
Under such conditions, reducing the shunt fraction is key to the ability to improve gas exchange, and this typically requires PPV and PEEPPEEP.

Key Factors DeterminingKey Factors Determiningon Arterial Oon Arterial Oon Arterial Oon Arterial O
450 0 mmHgmmHg mmHg
70%100%
85%50% 50%
g the Effects of Shunting g the Effects of Shunting OO SaturationSaturationOO22 SaturationSaturation
Note that inpatients with shunt physiology a reduction in arterial Ophysiology a reduction in arterial O2saturation may be due to a change in:
• the intraparenchymal shunt fraction (e.g., atelectasis)
oror• the SvO2 (e.g., drop in cardiac
output).A sudden drop in O2 saturation in patients with ARDS warrants a
SvO2
patients with ARDS warrants athorough assessment of the respiratory and cardiovascular system.
Shunt fraction

Mean Airway and A
In normal lungs, the inspiratory resistive pressure is similar to the expressure-time curve) so that mean airway pressure (Paw) can be us
Adapted from: Ravenscraft et al. Crit Ca
Alveolar Pressures
xpiratory resistive pressure (light shaded area under the airway sed to track mean alveolar pressure (Palv).
are Med. 1992.

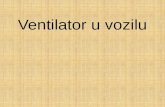
PEEP, Regional Lung VPEEP, Regional Lung V
Lung regions with shunt tend to distribute preferentially in the depenPEEP helps to maintain those regions open throughout expiration anvaries along the gravitational axis.
Volume, and ShuntingVolume, and Shunting
ZEEP
CPAP
dent regions. Tidal ventilation helps open collapsed regions, and nd to reduce shunt. Note that level of PEEP required to achieve such

Effect of PEEPEffect of PEEP--ininRecruitmenRecruitmenRecruitmenRecruitmen
Malbuisson et al. AJRCCM. 2001:
nduced Alveolar nduced Alveolar nt on PaOnt on PaOnt on PaOnt on PaO22
163:1444-1450.

ApproacApproac
Is MV i
Y
ContraindicaNO
NIPPV Y
YES
Success ? InvasNO
ch to MVch to MV
ndicated ? NO
Conservative
YES
treatment and periodic
reassessment
ation to NIPPV ?
YES
sive MV

NoninvasiveNoninvasive
Ventilatory support provided with• No tracheostomy• No ETT
e Ventilatione Ventilation
hout invasive airway control

Key Differences BetwKey Differences Betw
Advantages of NIPPVAdvantages of NIPPVAllows the patients to maintain normal functions• Speech• Eating
Helps avoid the risks and complications related to:p• Intubation• Sedation
Less ventilator-associated pneumoniapneumonia
ween NIPPV and IPPV ween NIPPV and IPPV
Disadvantages of NIPPVDisadvantages of NIPPVLess airway pressure is tolerated
Does not protect against aspiration
No access to airway forNo access to airway for suctioning

Clinical Use of NIPPClinical Use of NIPP
Decompensated COPD (Hypercp ( yp
Cardiogenic pulmonary edema
Hypoxic respiratory failureHypoxic respiratory failure
Other possible indications• Weaning (post-extubation) g (p )• Obesity hypoventilation syndrome• Patients deemed not to be intubated• Post-surgeryg y• Asthma
Adapted from: Am J Respir Crit Care Med. 20
PV in Intensive CarePV in Intensive Care
capnic Respiratory Failure)p p y )
001;163:283-291.

ContraindicatiContraindicatiCardiac or respiratory arrest
Nonrespiratory organ failure
Severe encephalopathy (e.g., G
Severe upper gastrointestinal b
Hemodynamic instability or uns
Facial surgery, trauma, or defog y
Upper airway obstruction
Inability to cooperate/protect thInability to cooperate/protect th
Inability to clear respiratory sec
High risk for aspirationHigh risk for aspirationAdapted from: Am J Respir Crit Care Me
ions to NIPPVions to NIPPV
GCS < 10)
bleeding
stable cardiac arrhythmia
ormityy
he airwayhe airway
cretions
d. 2001;163:283-291.

InitiatingInitiating
Initial settings:• Spontaneous trigger mode with backu• Start with low pressures
- IPAP 8 - 12 cmH2O PEEP 3 5 H O- PEEP 3 - 5 cmH2O
• Adjust inspired O2 to keep O2 sat > 90• Increase IPAP gradually up to 20 cm H
alleviate dyspnea- alleviate dyspnea- decrease respiratory rate- increase tidal volume- establish patient-ventilator synchronyp y y
g NIPPVg NIPPV
up rate
0%H2O (as tolerated) to:

Success and FailurSuccess and Failur
Improvements in pH and PCO2 othe eventual success of NPPVthe eventual success of NPPV.
If stabilization or improvement hthi ti i d th ti t hthis time period, the patient shoufailure and intubation must be st
Other criteria for a failed NPPV tencephalopathy or agitation, inainability to tolerate any availableinability to tolerate any availableinstability, worsened oxygenatio
e Criteria for NPPV e Criteria for NPPV
occurring within 2 hours predict
as not been achieved during ld b id d NPPVuld be considered an NPPV
trongly considered.
trial include: worsened ability to clear secretions, e mask hemodynamice mask, hemodynamic on.

ConcluConclu
A good understanding of respirthe judicious mechanical ventila
Unless contraindicated, NIPPVtry in many settings.
Monitoring key variables such ad t t f d ff timandatory to safe and effective
usionsusions
ratory physiology is required for ation.
V is becoming the first modality to
as Pplateau and auto-PEEP is tie practice.

Post Module TPost Module T
29-year-old patient (weight 120
ARDS secondary to bilateral pn
Ventilator settings: AC with VT 8PEEP 5 cmH2O, FIO2 80 %
Measured variables: rate 25, VEP l t 35 H OPplat 35 cm H2O
ABG: pH 7.40, PaO2 55 mmHg,85%85%
Testing: Case 1Testing: Case 1
kg, height 170 cm)
eumonia
800 ml and back-up rate 10/min,
E = 20 l/min, Ppeak 40 cm H2O,
PaCO2 38 mmHg, O2 saturation

QuestQuest
Wh t h i b t l i thWhat mechanism best explains th
1. V/Q mismatch1. V/Q mismatch2. Shunt3. Abnormal diffusion4 Inadequate oxygen delivery and high4. Inadequate oxygen delivery and high
tion 1tion 1
ti t’ h i ?e patient’s hypoxemia?
h tissue extractionh tissue extraction

AnswAnsw
If in a ventilated patient, FIO2 > the main cause for the hypoxem
As a rule, increasing the FIO2 wi t hi b t t f h t Wmismatching but not for shunt. W
present, hypoxemia typically co
Altered diffusion is rarely a cliniAltered diffusion is rarely a clini
Increasing the ventilation rate woxygenation unless it contributeoxygenation unless it contribute
wer 1wer 1
60% is needed, shunt is certainly mia (correct response: 2).
will compensate for VA/Q Wh V /Q i t hi iWhen VA/Q mismatching is
orrects with an FIO2 < 60%.
cally relevant issuecally relevant issue.
will not exert a significant impact on es to air trapping and auto-PEEP.es to air trapping and auto PEEP.

QuestQuest
Which of the following ventilatory sWhich of the following ventilatory sstep to reduce shunt and increbedside index of oxygen exch
1. Increase PEEP to 10 cmH202. Increase the FIO2 to 100%2
3. Add an inspiratory pause of 1 secon4. Increase respiratory rate to 30/min
tion 2tion 2
setting changes is the next bestsetting changes is the next best ease the PaO2/FIO2 ratio (a ange)
d

AnswAnsw
Interventions that target mean airwThey help recruit flooded or collapalveoli open for gas exchange (red
Increasing PEEP is the first interveinspiratory time and I:E ratio is a sinspiratory time and I:E ratio is a spressure.
In the presence of shunt, increasinp
Although increasing rate may affecminor. Rate adjustment is mainly uits consequences on:its consequences on: • air trapping • PaCO2 and pH
wer 2wer 2
way pressure are the most helpful. sed alveoli and maintain the recruited
duced shunt).
ention to consider; extending the econdary option to raise mean airwayecondary option to raise mean airway
ng the FIO2 would reduce the ratio. g 2
ct mean Paw, its impact is overall used to control minute ventilation and

QuestQuest
PEEP is increased to 10 cmH
P O i 85 H P l tPaO2 is now 85 mmHg, Pplat
The high pressure alarm is no
Your next step is:1. Reset the alarm pressure to 55 cmH2. Disconnect the patient from the venp3. Order a stat chest x-ray to assess fo4. Reduce the tidal volume slowly unti5. None of the above
tion 3tion 3
H20
i 45 d P k 50 H Ois 45, and Ppeak 50 cmH2O
ow triggered.
H20.ntilator and start manual ventilation (bagging). ( gg g)or a pneumothorax.l the alarm turns off.

AnswAnswThe correct answer is 5. Option 1 does not adairway pressure.
The rise in airway pressure that triggered the aPEEP l l Th i th d f 2 d 3PEEP level. There is thus no need for 2 and 3
Tidal volume is never titrated to an arbitrary se
Pplat, which tracks alveolar pressure and the (VILI) is an easy and accessible bedside para(VILI), is an easy and accessible bedside paraoverdistension. In this patient, it is the high Ppvolume that puts the patient at risk of VILI.
Patients with ARDS have reduced aerated lunsmall tidal volumes: e.g., 6 ml/kg predicted idean excessive tidal volume for his size (ideal orreduced. A tidal volume and PEEP combinatiogenerally considered safe. Concerns regardinwhen Pplat is > 30 cmH2O.
Remember, however, that the actual distendin(Pplat- Ppleural). Higher Pplat can be accepteless alveolar distension will be present for theless alveolar distension will be present for the
wer 3wer 3ddress the issue of the excessive tidal volume and
alarm was predictable following the increase in 33.
et alarm pressure.
risk of developing ventilator-induced lung injury ameter used to assess the risk of alveolarameter used to assess the risk of alveolar plat associated with the choice of an excessive tidal
ng volume (“baby lungs”) and need to ventilated with eal body weight. This patient is clearly ventilated with r predicted body weight). The tidal volume must be on associated with a Pplat of less than 25 cmH2O is g the risk of overdistension and VILI is significant
ng alveolar pressure is the transpulmonary pressure ed in a patient with low chest wall compliance, as
same Pplat everything else being equalsame Pplat, everything else being equal.

CasCas
67-year-old female (weight 50 kg) withCOPD decompensation. She failed Nand intubation.
Soon after intubation and initiation of mhypotensive (BP dropped from 170/95hypotensive (BP dropped from 170/95distended neck veins, midline tracheabreath sounds with prolonged expirato
Ventilatory settings are: assist controlVentilatory settings are: assist controlcmH2O, FIO2 1.0 (100%)
ABG: pH 7.20, PaO2 250 mmHg, PaC
Measured variables: rate 15/min, VE =cmH2O
se 2se 2
h severe emphysema is admitted for IPPV and required sedation, paralysis,
mechanical ventilation, she became 5 to 80/60). She has cold extremities,5 to 80/60). She has cold extremities, a, distant heart sounds, and symmetrical ory phase.
tidal volume 500ml rate 15/min PEEP 5, tidal volume 500ml, rate 15/min, PEEP 5
CO2 77 mmHg
= 7.5 l/min, Ppeak 45 cmH2O, Pplat 30

QuesQues
The next step in this patient’s manp p
1. Order a stat echocardiogram to ass2 Order a stat AngioCT to assess for2. Order a stat AngioCT to assess for 3. Measure AutoPEEP, disconnect the
resume ventilation with a lower tidafluid.fluid.
4. Start the patient on intravenous dopthe PaCO2.
stion 1stion 1
nagement should be:g
sess for tamponade.p lmonar embolismpulmonary embolism.
e patient briefly from the ventilator, then l volume and rate and administer intravenous
pamine and adjust the ventilator to normalize

AnswAnsw
The correct answer is 3. Remember thatventilated patient with obstructive physio
A i k l k t th i t fl t iA quick look at the expiratory flow tracinmaneuver demonstrated that the patientand intrinsic PEEP (15 cmH2O).
B i f di ti (1 2 i t ) fBrief disconnection (1 - 2 minutes) from oxygen saturation is safe in this conditioPEEP to decrease--thus restoring venourestoration of BP following ventilator discgTherefore, intrinsic PEEP needs to be m
It is also important to consider the possiThe symmetrical chest and midline trachy
Also notice that Pplat was elevated (duewith stiff lungs (ARDS), there is a large dairway resistance is markedly elevated iy y
wer 1wer 1
t gas trapping is your key concern in the ology.
d f i i tg and performing an expiratory pause t has developed severe dynamic hyperinflation
th til t hil ti l it ithe ventilator while continuously monitoring on and allows for the lung to empty, intrinsic us return, preload, stroke volume, and BP. The connection is not specific for air trapping. p pp g
measured to confirm the diagnosis.
bility of a tension pneumothorax in this patient. hea did not suggest this possibility here.gg p y
e to gas trapping), but in contrast to a patient difference between Ppeak and Pplat because n patients with COPD.p

QuesQues
You change the ventilator’s tidal 15/min. After 1 liter of physiologip y g100/70 mmHg and heart rate is mmHg, PaCO2 60 mmHg. Measl/min, Ppeak 37 cmH2O, Pplat 25l/min, Ppeak 37 cmH2O, Pplat 257cmH2O (total PEEP=12 cmH2O
The best next step is to:1. Continue with bronchodilators and t2. Increase the rate to normalize PaCO3. Increase the tidal volume but only to4. Ask for another ABG since you do n
ventilation declined.
tion 2tion 2
volume to 300 ml and the rate to ic saline is infused, the BP is now ,120/min. ABG: pH 7.30, PaO2 250
sured variables: rate 20/min, VE = 6.0 5 cmH2O, Intrinsic PEEP is now5 cmH2O, Intrinsic PEEP is now
O).
tolerate the current mild respiratory acidosis.O2.o normalize the pH.not believe the drop in PaCO2--minute

AnswAnsw
The best next step is continueth t ild i tthe current mild respiratory ac
• The patient has no contraindicationscentral nervous system problem, thaintracranial pressure associated witintracranial pressure associated witarrhythmia.
• Although less than present initially, Pplat and relatively low BP). Thus, iPplat and relatively low BP). Thus, ithe pH or PaCO2 will make this wors
• The reduction in PaCO2 is due to leand reduced dead space ventilationand thus promote ventilation of unp
wer 2wer 2
e with bronchodilator and tolerate id i (RA)cidosis (RA).
s to mild RA (history of an acute or chronic at may be worsened by the increase in th RA heart failure cardiac ischemia orth RA, heart failure, cardiac ischemia, or
dynamic hyperinflation is still an issue (high increasing the minute ventilation to normalizeincreasing the minute ventilation to normalize se.
ess air trapping, with improved venous return n. Hyperinflation tends to compress capillaries erfused alveolar units (dead space).

References and SuReferences and Su
Hubmayr RD, Abel MD, Rehder K.ventilation Crit Care Med 1990;18ventilation. Crit Care Med. 1990;18Tobin MJ. Mechanical ventilation. Marini JJ. Monitoring during mechaMarini JJ. Monitoring during mecha1988;9:73-100.Brochard L. Noninvasive ventilatio2002;288:932-9352002;288:932-935. Calfee CS, Matthay MA. Recent adAm J Med. 2005;118:584-91.
uggested Readingsuggested Readings
. Physiologic approach to mechanical 8:103-138:103-13. N Engl J Med. 1994;330;1056-61. anical ventilation. Clin Chest Med.anical ventilation. Clin Chest Med.
on for acute respiratory failure. JAMA.
dvances in mechanical ventilation.