Basics Cervical myelopathy - البروفيسور فريح ابوحسان - استشاري...
39
Cervical Myelopathy Cervical Myelopathy “ “ Always Ignored Always Ignored ” ” !! !! What could Orthopaedic surgeon do? What could Orthopaedic surgeon do?
-
Upload
prof-freih-abu-hassan- -
Category
Health & Medicine
-
view
148 -
download
12
description
• استشاري جراحة العمود الفقري في الاردن / مرضى العمود الفقري بطرق جراحية وغير جراحية / جراحة العمود الفقري بالتداخل المحدود / عمليات الديسك أو الإنزلاق الغضروفي / علاج الديسك / عمليات الديسك / الم الظهر من الديسك / جراحة الد يسك / علاج الديسك في الاردن / اطباء الديسك / اطباء الديسك في الاردن / اسباب الديسك / الام الديسك / الم العمود الفقري / اسباب الانزلاق الغضروفي / اوجاع الديسك / اعراض الديسك / علاج الديسك / افضل اطباء الديسك في الاردن / اسرع علاج للديسك في الاردن / افضل طبيب لعلاج الانزلاق الغضروفي / افضل طبيب لعلاج الانزلاق الغضروفي في الاردن / كسور الفقرات / قوس العمود الفقري عند الكبار / حقائق عن آلام الظهر والديسك / تحرير عصب اليد / عمليات تحرير العصب / ألم الظهر المزمن علاج ألم الظهر المزمن / الانزلاق الغضروفي / هشاشة العظام / علاج هشاشة العظام / نقص فيتامين د / نقص الكالسيوم في الجسم / فائدة الكالسيوم في الجسم / مشاكل نقص الكالسيوم في الجسم / ترقق العظام / عمليات الفقرات / اعراض الديسك / اعراض هشاشة العظام / اعراض نقص الفيتامين د / اعراض نقص الكالسيوم / عندي آلام شديدة في أسفل / خدران في اليد / خدران او تنميل اليد / خدران الرجل / خدران الساق / خدران الاطراف / تنميل الاطراف / تنميل اليد / رجوع الديسك
Transcript of Basics Cervical myelopathy - البروفيسور فريح ابوحسان - استشاري...
Cervical MyelopathyCervical Myelopathy““Always IgnoredAlways Ignored””!!!!
What could Orthopaedic surgeon do?What could Orthopaedic surgeon do?
Cervical Spondylotic Cervical Spondylotic Myelopathy (CSM)Myelopathy (CSM)
Def: Spinal cord dysfunction secondary to:-- Extrinsic compression of the cord.- Blood supply interferance.- Both
(Parke, Spine. 1988)
CSM Syndrome. - Sir Russel Brain : Neurologist. - D. North Field : Neuro Surgeon. - Marcia Wilkinson : Pathologist.
(Brain etal. 1952).
This is one more condition which has been
taken out of the scrap basket into which
we used to put MS or spinal degenerative
disease.
(Gilbert Horrax, 1954).
Cervical Myelopathy : A complication of Cervical
Spondylosis (CSM).
* (Brain etal. 1952). * (Clarke & Robinson 1956).

Pathophysiology of CSMPathophysiology of CSM
* Pre existing cong. or developmental stenosis.
* Degenerative changes in the disc, producing secondary changes on nearby structures
* Osteophyte of facet Joint.
* Ligamentum flavum thickening.
CSMCSM
Most common type of spinal cord
dysfunction above 55y old.
(Simeone etal. 1982)
CSM * frequently under diagnosed, under
treated, often leading to increased disability.
Law etal, (JBJS - A, 1994) Bernhardt etal. (JBJS-A, 1993)* The single most common under
diagnosed spinal disorder. (Dillin etal, 1989).
Clinical EvaluationClinical Evaluation
A- Common Symptoms : Above 55y.
* Loss of dexterity of the U.L.
(Clumsy or weak hands).
* Neck stiffness, difficulty in walking,
* Leg weakness or stiffness
* Pain in shoulders or arms
* Radicular nerve roots symptoms.
B - Physical Examination.1. U.M.N.L. : L.L. ( Hyperreflexia)
2. U.M.N.L./L.M.N.L. : U.L. (Atrophy of the hand musculature)
3. Hoffmann`s sign + (Neck extension).
4. Inverted B. Radialis reflex.
5. Neck flexion Electric shock –sensation down the back &L.L. (Lhermitte sign).
6. Changes in deep sensation.
- Position.
- Vibration.
7. Abnormal gait.
8. Early DisdiadochoKinesia
(Uncoordinated alternating movement).
Diagnostic StudiesDiagnostic Studies
1. C. spine x-ray - Routine.
- Instability.
- Pavlov ratio.
2. MRI.
3. Myelogram for dynamic instability.
4. CT myelogram for OPLL.
Differential Dx of CSMDifferential Dx of CSM
1. Multiple sclerosis.
2. Amyotrophic lateral sclerosis.
3. Spinal cord tumor.
4. Subacute combined degeneration.
5. Cervical disc herniation.
6. Cerebral lesion.
7. Syringomyelia

Natural History of CSMNatural History of CSM
* Most becomes worse clinically if untreated.
* > 50% progress to severe disability.
* Surgery best.
= 6-12M symptoms.
= Early myelopathic findings.
Disability Classification of Disability Classification of CSMCSM
(Nurick 1972)(Nurick 1972)* Grade O : Radicular S & S only.
* Grade 1 : Signs of cord involvement.
* Grade 2 : Mild gait involvement.
* Grade 3 : Gait problem affecting work.
* Grade 4 : Ambulation with assistance.
* Grade 5 : Chairbound or bedridden.

Dangerous Conservative Dangerous Conservative treatmenttreatment
1. Cervical traction.
2. Manipulation of C. Spine will cause:
* Narrowing of spinal canal.
* “ “ foramina.
* Irritation to the facet joints &
produce further swelling.
When to consider When to consider conservative treatment?.conservative treatment?.
* Mild symptoms.
* 13 points or more in JOA score.
Conservative treatmentConservative treatment
* How long?.
* Firm orthosis/NSAIDs.
* Isometric muscle strengthening.
* Ice, heat, massage.
* Monthly follow up.
Operative managementOperative management
Absolute indications1. Neurological defecit which are progressive or have already developed.2. Failure of non-operative methods to improve the neurological findings.3. Severe myelopathy.4. 7 points or less in JOA score.

Who will benefit from surgery?Who will benefit from surgery?
1. Severe tingling in the fingers & legs.
2. Poor handling of knife and fork.
3. difficulty in buttoning shirts.
4. Symptoms less than one year.
5. Patients with 8-12 point in JOA score.
Which approach?.Which approach?.
* Anterior decompression!.* Posterior decompression!.* Anterior + Posterior!.
Pre operative Pre operative considerationsconsiderations
* Avoid hyper extension of the neck during positioning.
* Left sided approach to avoid inj. to RLN.
* Pre op 120mg prednisolone to be repeated after 4hrs.
When to do ant. When to do ant. approach?approach?
1. Soft disc herniation 1 to 2 levels.
2. Spondylosis 1 to 4 levels.
3. Developmental narrowing of the canal.
4. Kyphotic deformity.
5. Localized OPLL.
What you should do What you should do anteriorly?anteriorly?
1. ACDF + plates!!!.
2. Corpectomy + graft.
3. Corpectomy + strut graft.
When to do posterior When to do posterior decompression?decompression?
1. Compression of > 4 levels.2. Calcification of lig. flavum.3. Developmental stenosis : (< AP
13mm).4. Extensive OPLL.
Posterior decompression Posterior decompression proceduresprocedures
1. Laminectomy.
2. Bilat. Open door laminectomy (Kirita’s).
3. Expanding laminoplasty.
* Spinous process splitting.
* Hemilat. open.
* Z-Plasty.
Combined approaches!!!!Combined approaches!!!!
* Cervical instability.
* Dominant, localized ventral lesion.
e.g cervical disc, OPLL with canal stenosis.
* Dominant, localized vental lesion with extensive CS or OPLL.
Poor prognosis after Poor prognosis after decompressiondecompression
1. Atrophy of the spinal cord on MRI
(Severe cord malacia).2. Weakness of peroneal muscles (Kozo etal. 1991).3. Worse pre op. neurological function (Emery etal 1998).4. Loss of vibration & propriocepition (Montgomery 1992).
Complications of surgery for Complications of surgery for CSMCSM
1. Graft problems.
a. Dislodgment.
b. Non union.
c. Graft site morbidity.
2. Spinal instability.
3. Spinal cord injury.
4. Injury to nearby structures.
5. Technical.
108 patient CSM ,1974 - 108 patient CSM ,1974 - 19931993
(Emery etal. JBJS-A 1998)(Emery etal. JBJS-A 1998)
Procedure : Ant. decompression + graft.
2 Patients died (MI, Pneumonia).
Follow up (2-17 years).
87 pt. had motor defecit pre 87 pt. had motor defecit pre op.op.
54 pt. Complete recovery post op.26 pt. Partial recovery post op.06 pt. No change.01 pt. Worse deficit.
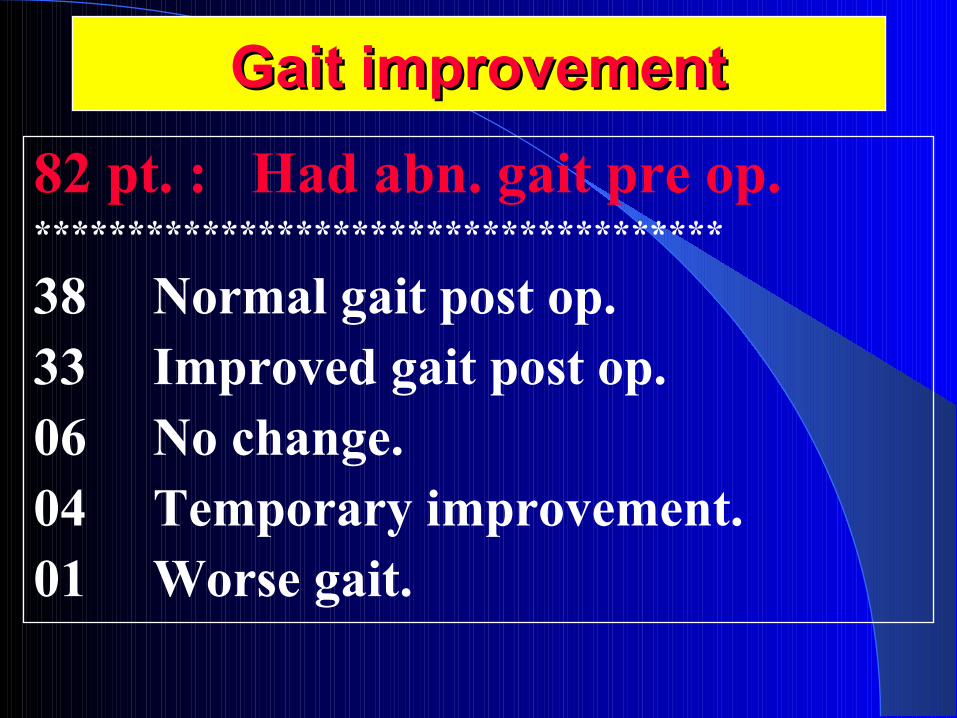
Gait improvementGait improvement
82 pt. : Had abn. gait pre op.*************************************
38 Normal gait post op.33 Improved gait post op.06 No change.04 Temporary improvement.01 Worse gait.
Pre op. Nurick score : 2.4
Post op. = = = = = : 1.2 (Average 0.0 to 5.0).
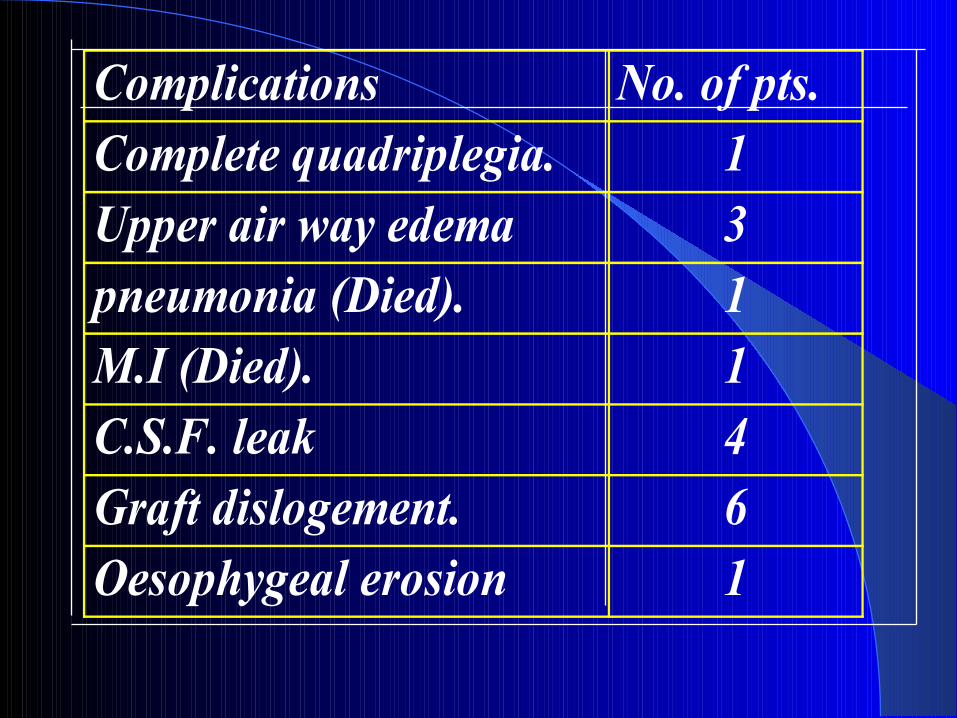
Complications No. of pts.Complete quadriplegia. 1Upper air way edema 3pneumonia (Died). 1M.I (Died). 1C.S.F. leak 4Graft dislogement. 6Oesophygeal erosion 1
ConclusionConclusion
1. CSM is under diagnosed and under treated.
2. Surgery will improve the gait and neurology.
3. Surgical approach depends on the site of
the pathology and surgeon experience.
ConclusionConclusion
4. Atrophy of the spinal cord is a poor
prognostic indicator.
5. Complications of surgery is minimal in
comparison with the functional
improvement of disability.
Spinal Tracts Syndromes in Spinal Tracts Syndromes in CSMCSM
1. Transverse lesion : Most common.
* AHC.
* Spino. Th. Tract.
* Cortico spinal tract.
* Lately : Post column.
2. Motor system synd.
* Cortico spinal tract.
* Weak U.L. + L.L.
* Spasticity.
3. Central cord syndrome.
* U.L. weaker than L.L.
* Prominant hand weakness.
* Rarely post column.
4. Brown-Sequard Syn:Early form of CSM..
* Cortico spinal tract (Unilat.)
- Hemi paresis.
- Pain & Temp. analgesia.
* Best prognosis for recovery.
5. Brachialgia cord syndrome.
* U.L. root compression : Radicular
symptoms with paraesthesia &
hyporeflexia.
* Long tract signs, weakness.
* Gait disturbance.