AXL Inhibition Improves Immunotherapy by …...Agata Rybicka3, Muntequa I. Siraji1,2, Sushil...
1
References: 1 Gubin et al., 2018. 2 Chen and Mellman, 2017. 3 Lemke and Rothlin, 2008. 4 Ye et al., 2010. 5 Chiu et al., 2015. 6 Davidsen K.T et al., 2017. 7 Terry et al., 2017. ICB + bemcentinib targets tumor-immune crosstalk AXL is highly expressed in suppressive myeloid cells AXL + M2φs are reduced by bemcentinib treatment AXL is expressed in distinct DC populations with highly suppressive profiles Conclusions • • • • NK cells NK-S1 NK-S2 NK-S3 NK-S5 CD11b- CD11b+ NK-S4 Ly6G+ MHCII + - iNOS+pDCs DC-S9 DC-S8 CD4+ CD4- DC-S5 CD4+ DC-S4 CD206+ DC-S7 cDC2 DC-S1 CD80+ DC-S6 DC-S3 DC-S2 CD24+ CD8+cDC1 Neutrophils Immature cDC2 PDL1 high DC-T3 DC-T4 Ly6C+(pDCs) CD4+ CD4- DC-T1 Neutrophils CD103+cDC1 CD80 low DC-T8 DC-T9 CD80 int CD11b+MHCII -CD24+ DC-T2 cDC2 DC-T5 DC-T6 DC-T7 Arg-1+ Axl+ NK cells NK-T2 NK-T3 NK-T1 CD11b CD11b- + - Ly6C + - Spleen Tumor Force-directed layout of X-Shift clusters visualizes rare cell populations in spleens and tumors. Lorem ipsum AXL is Expressed in Rare Dendritic Cell Populations T1 Spleen Axl MerTK T2 Spleen Axl MerTK Tumor T1 T2 Tumor Uniform Manifold Approximation and Projection (UMAP ) of single immune cells showing AXL and MerTK expression at timepoint 1 and timepoint 2 in spleens and tumors. Tumors mobilize AXL in Suppressive Myeloid Cells CD4 T cells CD8 T cells gMDSC NK cells B cells Macrophages/ monocytes Macrophages/ monocytes T1 T2 Spleen Tumor BALB/C mice bearing established 4T1 mammary tumors were treated as indicated, n=5 per treatment per timepoint. Spleens and tumors were analyzed by CyTOF using a 34- marker myeloid focused panel. Graphs show single immune cells mapped with UMAP (left; colored by marker expression of CD11b, right;colored by density showing changes over time in immune populations in untreated animals) Day 0 Day 12 Day14 Day 16 Day 18 Day 22 αCTLA4/αPD1 Bemcentinib Randomization T1 T2 ET2 ET1 High Dimensional Single Cell Immune Phenotyping CSF1 mRNA fold change relative to ctr 0 10 20 30 CSF1 α CTLA4/ α PD 1 α CTLA4/ α PD1/Bem Non- responder s Responder s P = 0.0416 Fold change of CSF1 gene expression in 4T1 tumors unresponsive to ICB (n=4) or ICB and bemcentinb (n=5) and responsive tumors treated with ICB/bemcentinib (n=2), compared to vehicle AXL Inhibition Blocks Tumor-Myeloid Crosstalk 0 50 100 150 0 50 100 Days of treatment Percent survival Vehicle n= 1 1 Bemcentinib n=1 2 α CTLA4 / α PD1 n=17 α CTLA4 / α PD1/ Bemcentinib n=2 6 p = 0.0189 Durable tumor clearance in 25.6% of animals with established orthotopic 4T1 mammary tumors treated with bemcentinib + anti-CTLA-4 + anti-PD-1 vs 5.6% of animals treated with anti-CTLA-4 + anti-PD-1 AXL Inhibition Potentiates the Effect on Immune Checkpoint Inhibitors Tumor Single immune cells clustered with PhenoGraph and analyzed with Marker Enrichment Modeling (MEM). Heat map of MEM-scores with changes in individual PhenoGraph clusters over time and between treatments. 6 19 14 13 3 4 12 23 20 25 2 16 17 10 1 15 9 24 11 21 7 18 5 8 22 CD206 CD11b CD3 CD4 Ly6C MHCII CD80 Ly6G-C CD24 CD40 iNOS CD11c CD19 CD25 Axl MerTK CD49b CD69 CD86 CD45 PD1 CTLA4 CD83 CD8a PDL1 CD335 CD114 Arg-1 CD115 CD64 F4/80 CD103 CD116 CD206 CD11b CD3 CD4 Ly6C MHCII CD80 Ly6G-C CD24 CD40 iNOS CD11c CD19 CD25 Axl MerTK CD49b CD69 CD86 CD45 PD1 CTLA4 CD83 CD8a PDL1 CD335 CD114 Arg-1 CD115 CD64 F4/80 CD103 CD116 T1 T2 Ctr Bem ICB ICB + Bem ICB + Bem Ctr Bem ICB gMDSC NK cells DCs Mφ mMDSC CD4 T cells Axl+MerTK+ Mφ/M2φ gMDSC pDCs Lin- B cells B cells Axl+MerTK+ Mo/Mφ CD8 T cells CD4-CD8- T cells CD116 CD80 CD11c F4/80 CD206 CD64 MHCII CD11b CD24 Ly6G-C Ly6C Axl MerTK iNOS Arg-1 CD115 CD69 PDL1 CD103 CD86 CD3 CTLA4 CD49b CD40 CD45 PD1 CD83 CD335 CD25 CD114 CD19 CD4 CD8 CD116 CD80 CD11c F4/80 CD206 CD64 MHCII CD11b CD24 Ly6G-C Ly6C Axl MerTK iNOS Arg-1 CD115 CD69 PDL1 CD103 CD86 CD3 CTLA4 CD49b CD40 CD45 PD1 CD83 CD335 CD25 CD114 CD19 CD4 CD8 18 19 13 6 20 11 15 16 25 14 10 24 22 8 5 12 3 4 9 7 17 23 Axl+ M2φ int. Mφ iNOS+Arg-1+Mφ MerTK+M2φ M2φ Ly6C high Mo/Mφ CD49b+Axl+MDSC CD24+ Mo/Mφ gMDSC pDC Ly6C+ CD8 T cells DCs Mo/Mφ Lin- CD4-CD8-T cells CD8 T cells CD4 T cells NK cells Lin- T1 T2 Ctr Bem ICB ICB + Bem ICB + Bem Ctr Bem ICB Spleen AXL Inhibition Reshapes the Immune Landscape Background Tumor mobilization of suppressive myeloid cells remains a primary obstacle to immune checkpoint blockade (ICB) efficacy (1) . Tumor microenvironments enriched in suppressive myeloid cells are often T cell infiltrated (2) providing a rationale for ICB combination strategies with myeloid targeting agents. The receptor tyrosine kinase AXL is a key tolerogenic regulator of the innate immune response (3) . Tumor associated macrophages (TAM) express AXL (4) and mediates M2-macrophage polarization (5) . In cancer AXL is associated with epithelial-to-mesenchymal (EMT) -related phenotypic plasticity and therapy resistance (6) . EMT is increasingly recognized as a major contributor to tumor immune evasion (7) . The small molecule AXL inhibitor bemcentinib targets tumor cell intrinsic phenotypic plasticity and myeloid immune suppression. Bemcentinib in combination with ICB is currently in phase II trials for NSCLC (NCT03184571), melanoma (NCT02872259) and mesothelioma (NCT0365483). • • • • • • • • AXL Inhibition Improves Immunotherapy by Targeting Local and Systemic Tumor Myeloid Cross-Talk Kjersti T.Davidsen 1,2 , Katarzyna Wnuk-Lipinska 3 , Sturla M. Grøndal 1,2 , Noelly Madeleine 1,2 , Stacey A. D’mello Peters 1,2 , Magnus Blø 3 , Linn Hodneland 3 , Lavina Ahmed 3 , Agata Rybicka 3 , Muntequa I. Siraji 1,2 , Sushil Dhaka 1,2 , Oddbjørn Straume 2,4 , Michael A. Curran 5 , Rolf A.Brekken 6 , Gro Gausdal 3 , James B. Lorens 1,2 1 Department of Biomedicine, 2 Centre for Cancer Biomarkers, University of Bergen, 3 BerGenBio ASA, 4 Department of Oncology, Haukeland University Hospital, 5 Department of Immunology, The University of Texas MD Anderson Cancer Center, 6 Department of Surgery and Hamon Center for Therapeutic Oncology Research, UT Southwestern Medical Center
Transcript of AXL Inhibition Improves Immunotherapy by …...Agata Rybicka3, Muntequa I. Siraji1,2, Sushil...

References: 1Gubin et al., 2018. 2Chen and Mellman, 2017. 3Lemke and Rothlin, 2008. 4Ye et al., 2010. 5Chiu et al., 2015. 6Davidsen K.T et al., 2017. 7Terry et al., 2017.
ICB + bemcentinib targets tumor-immune crosstalk AXL is highly expressed in suppressive myeloid cells AXL+ M2φs are reduced by bemcentinib treatmentAXL is expressed in distinct DC populations with highly suppressive profiles
Conclusions
••••
NK cells
NK-S1
NK-S2NK-S3
NK-S5
CD11b-
CD11b+
NK-S4 Ly6G
+
MHC
II
+
-
iNOS+pDCs
DC-S9
DC-S8
CD4+
CD4-
DC
-S5
CD4+ DC-S4
CD206+ DC-S7
cDC2
DC-S1
CD80+
DC-S6
DC-S3
DC-S2
CD24+CD8+cDC1
Neutrophils
Immature cDC2
PD
L1high
DC-T3DC-T4
Ly6C+(pDCs)
CD4+
CD4-
DC-T1
Neutrophils
CD103+cDC1
CD80 low
DC-T8
DC-T9
CD80 int
CD11b+MHCII-CD24+
DC-T2
cDC2
DC-T5
DC-T6
DC-T7
Arg
-1+
Axl
+
NK cells
NK-T2
NK-T3
NK-T
1
CD11bCD
11b-
+
-
Ly6C
+
-
Spleen Tumor
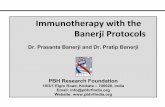
Force-directed layout of X-Shift clusters visualizes rare cell populations in spleens and tumors.
Lorem ipsum
AXL is Expressed in Rare Dendritic Cell Populations
T1Sp
leen
Axl MerTK
T2Sp
leen
Axl MerTK
Tumo
rT1
T2Tu
mor
Uniform Manifold Approximation and Projection (UMAP ) of single immune cells showing AXL and MerTK expression at timepoint 1 and timepoint 2 in spleens and tumors.
Tumors mobilize AXL in Suppressive Myeloid Cells
CD4 T cells
CD8 T cells
gMDSC
NK cells
B cells
Macrophages/monocytes
Macrophages/monocytes
T1
T2
Spleen Tumor
BALB/C mice bearing established 4T1 mammary tumors were treated as indicated, n=5 per treatment per timepoint. Spleens and tumors were analyzed by CyTOF using a 34- marker myeloid focused panel. Graphs show single immune cells mapped with UMAP (left; colored by marker expression of CD11b, right;colored by density showing changes over time in immune populations in untreated animals)
Day 0 Day 12 Day14 Day 16 Day 18 Day 22
αCTLA4/αPD1
Bemcentinib
Rand
omiza
tion
T1T2
ET2ET1
High Dimensional Single Cell Immune Phenotyping
CSF1
mRN
A fol
d cha
nge
relat
ive to
ctr
0
10
20
30
CSF1
αCTLA4/ αPD 1 αCTLA4/ αPD1/Bem
Non- responder s Responder s
P = 0.0416 Fold change of CSF1 gene expression in 4T1 tumors unresponsive to ICB (n=4) or ICB and bemcentinb (n=5) and responsive tumors treated with ICB/bemcentinib (n=2), compared to vehicle
AXL Inhibition Blocks Tumor-Myeloid Crosstalk
0 50 100 1500
50
100
Days of treatment
Perce
ntsu
rviva
l
Vehicle n= 1 1Bemcentinib n=1 2
αCTLA4 /αPD1 n=17αCTLA4 /αPD1/Bemcentinib n=2 6
p = 0.0189
Durable tumor clearance in 25.6% of animalswith established orthotopic 4T1 mammary tumors treated with bemcentinib + anti-CTLA-4 + anti-PD-1 vs 5.6% of animals treated with anti-CTLA-4 + anti-PD-1
AXL Inhibition Potentiates the Effect on Immune Checkpoint Inhibitors
Tumor
Single immune cells clustered with PhenoGraph and analyzed with Marker Enrichment Modeling (MEM). Heat map of MEM-scores with changes in individual PhenoGraph clusters over time and between treatments.
619141334
122320252
1617101
159
2411217
1858
22
CD
206
CD
11b
CD
3
CD
4
Ly6C
MH
CII
CD
80Ly
6G-C
CD
24
CD
40iN
OS
CD
11c
CD
19
CD
25A
xl
Mer
TK
CD
49b
CD
69
CD
86
CD
45P
D1
CTL
A4
CD
83
CD
8a
PD
L1
CD
335
CD
114
Arg
-1
CD
115
CD
64
F4/8
0
CD
103
CD
116
CD
206
CD
11b
CD
3
CD
4
Ly6C
MH
CII
CD
80Ly
6G-C
CD
24
CD
40iN
OS
CD
11c
CD
19
CD
25 Axl
Mer
TK
CD
49b
CD
69
CD
86
CD
45P
D1
CTL
A4
CD
83
CD
8a
PD
L1
CD
335
CD
114
Arg
-1
CD
115
CD
64
F4/8
0
CD
103
CD
116
T1 T2
Ctr
Bem
ICB
ICB
+ B
em
ICB
+ B
emCtr
Bem
ICB
gMDSC
NK cells
DCs
Mφ
mMDSC
CD4 T cells
Axl+MerTK+Mφ/M2φ
gMDSC
pDCs
Lin-
B cells
B cells
Axl+MerTK+Mo/Mφ
CD8 T cellsCD4-CD8-T cells
CD
116
CD
80C
D11
cF4
/80
CD
206
CD
64M
HC
IIC
D11
bC
D24
Ly6G
-CLy
6C Axl
Mer
TKiN
OS
Arg
-1C
D11
5C
D69
PD
L1C
D10
3C
D86
CD
3C
TLA
4C
D49
bC
D40
CD
45P
D1
CD
83C
D33
5C
D25
CD
114
CD
19C
D4
CD
8
CD
116
CD
80C
D11
cF4
/80
CD
206
CD
64M
HC
IIC
D11
bC
D24
Ly6G
-CLy
6CA
xlM
erTK
iNO
SA
rg-1
CD
115
CD
69P
DL1
CD
103
CD
86C
D3
CTL
A4
CD
49b
CD
40C
D45
PD
1C
D83
CD
335
CD
25C
D11
4C
D19
CD
4C
D8
1819
136
20
1115
16251410
2422
85
12
34
97
1723
Axl+ M2φint. Mφ
iNOS+Arg-1+MφMerTK+M2φ
M2φ
Ly6C high Mo/MφCD49b+Axl+MDSC
CD24+ Mo/Mφ
gMDSC
pDCLy6C+ CD8 T cells
DCsMo/Mφ
Lin-
CD4-CD8-T cells
CD8 T cells
CD4 T cells
NK cellsLin-
T1 T2
Ctr
Bem
ICB
ICB
+ B
em
ICB
+ B
emCtr
Bem
ICB
Spleen
AXL Inhibition Reshapes the Immune LandscapeBackground
Tumor mobilization of suppressive myeloid cells remains a primary obstacle to immune checkpoint blockade (ICB) efficacy(1).
Tumor microenvironments enriched in suppressive myeloid cells are often T cell infiltrated(2) providing a rationale for ICB combination strategies with myeloid targeting agents.
The receptor tyrosine kinase AXL is a key tolerogenic regulator of the innate immune response(3).
Tumor associated macrophages (TAM) express AXL(4) and mediates M2-macrophage polarization(5).
In cancer AXL is associated with epithelial-to-mesenchymal (EMT) -related phenotypic plasticity and therapy resistance (6).
EMT is increasingly recognized as a major contributor to tumor immune evasion(7).
The small molecule AXL inhibitor bemcentinib targets tumor cell intrinsic phenotypic plasticity and myeloid immune suppression.
Bemcentinib in combination with ICB is currently in phase II trials for NSCLC (NCT03184571), melanoma (NCT02872259) and mesothelioma (NCT0365483).
•
•
•
•
•
•
•
•
AXL Inhibition Improves Immunotherapy by Targeting Local and Systemic Tumor Myeloid Cross-Talk Kjersti T.Davidsen1,2, Katarzyna Wnuk-Lipinska3, Sturla M. Grøndal1,2, Noelly Madeleine1,2, Stacey A. D’mello Peters1,2, Magnus Blø3, Linn Hodneland3, Lavina Ahmed3, Agata Rybicka3, Muntequa I. Siraji1,2, Sushil Dhaka1,2, Oddbjørn Straume2,4, Michael A. Curran5, Rolf A.Brekken6, Gro Gausdal3, James B. Lorens1,2
1 Department of Biomedicine, 2 Centre for Cancer Biomarkers, University of Bergen, 3 BerGenBio ASA, 4 Department of Oncology, Haukeland University Hospital, 5 Department of Immunology, The University of Texas MD Anderson Cancer Center, 6 Department of Surgery and Hamon Center for Therapeutic Oncology Research, UT Southwestern Medical Center