STRESS MANAGEMENT Matt Orr, PhD Department of Family and Preventive Medicine.
Rena Buckstein MD Head, Haematology Site GroupAssociate Professor, Department of MedicineOdette Cancer Centre, Sunnybrook Health Sciences Centre

Research funding and honoraria: Celgene Advisory Boards: Celgene, Novartis and Abbvie


Novel insights into MDS and AML diagnosis, pathophysiology and prognosisNew therapies for AML and ALLNew therapies for relapsed Hodgkin’s Improved survival Multiple Myeloma B cell receptor signaling inhibitors


A group of hematopoietic neoplasms characterized by1
Bone marrow failure with resultant cytopenia(s) and related complications High frequency of clonal cytogenetic alterations Dysplastic cytologic morphology Instability and tendency to progress to AML
Overall incidence >3.7-4.8/100,0002
>10,000/yr in US (claims data true estimates ≈37,000-48,000)
AML = acute myeloid leukemia.1. Bennett J, et al. The myelodysplastic syndromes. In: Abeloff MD, et al, eds. Clinical Oncology. New York, NY: Churchill Livingstone; 2004:2849-2881. 2. SEER data. 2000-2009. 3. SEER 18 data. 2000-2009.

Median age at diagnosis: 72
Age at Diagnosis (Yrs)*P for trend < .05Rollison DE, et al. Blood. 2008;112:45-52.
0
10
20
30
40
50
< 40 40-49 50-59 60-69 70-79 ≥ 80
0.1 0.7 2.07.5
20.9
36.4*
FemalesMalesOverall
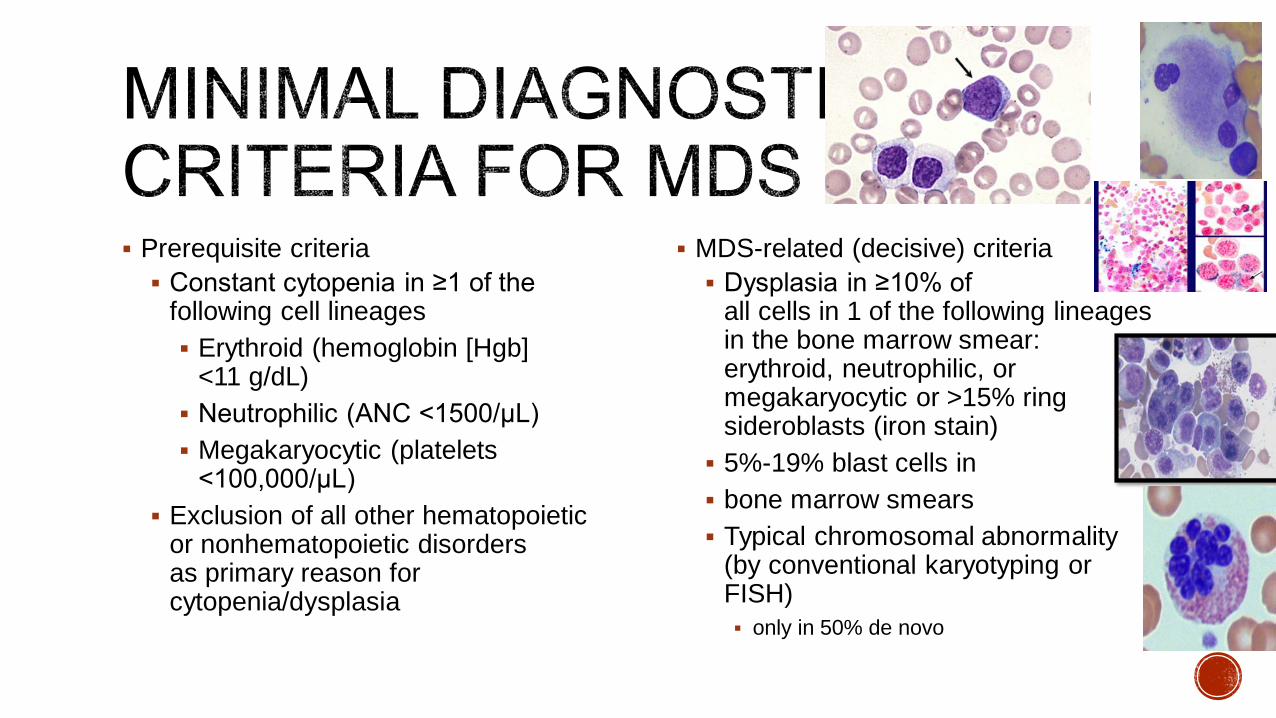
Prerequisite criteria Constant cytopenia in ≥1 of the
following cell lineages Erythroid (hemoglobin [Hgb]
<11 g/dL) Neutrophilic (ANC <1500/μL) Megakaryocytic (platelets
<100,000/μL) Exclusion of all other hematopoietic
or nonhematopoietic disorders as primary reason for cytopenia/dysplasia
MDS-related (decisive) criteria Dysplasia in ≥10% of
all cells in 1 of the following lineages in the bone marrow smear: erythroid, neutrophilic, or megakaryocytic or >15% ring sideroblasts (iron stain) 5%-19% blast cells in bone marrow smears Typical chromosomal abnormality
(by conventional karyotyping or FISH) only in 50% de novo
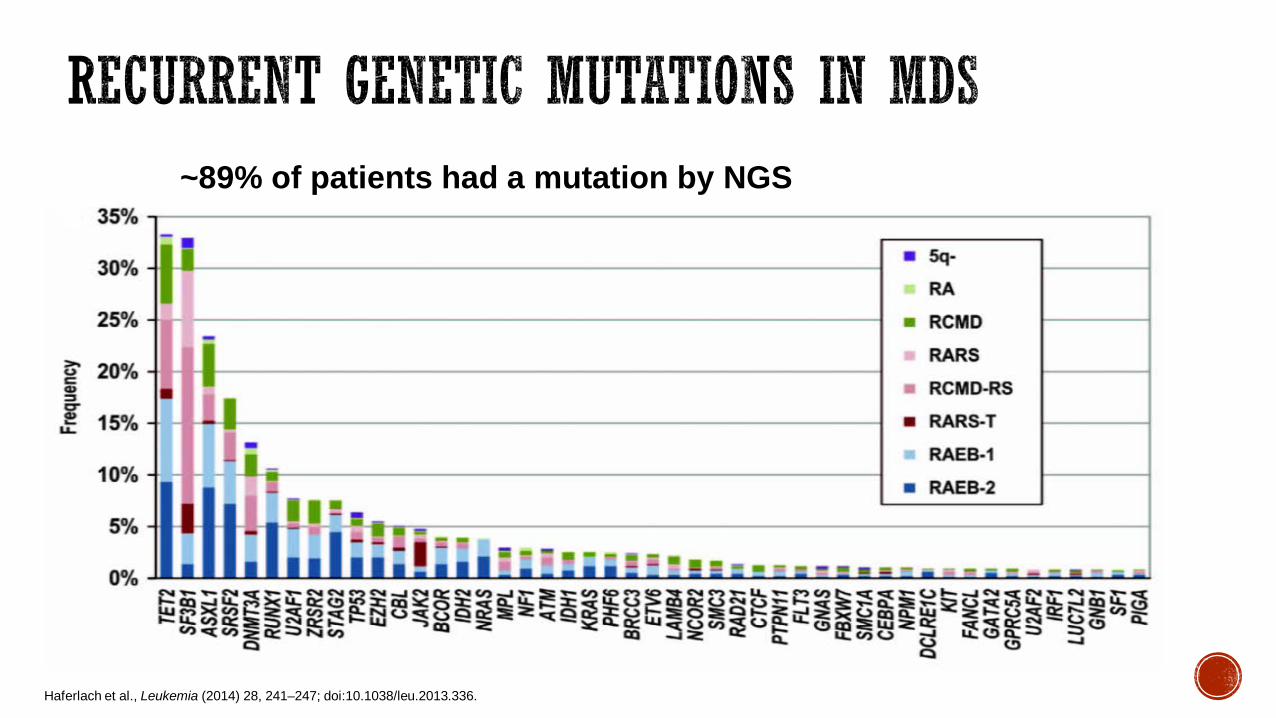
Haferlach et al., Leukemia (2014) 28, 241–247; doi:10.1038/leu.2013.336.
~89% of patients had a mutation by NGS
9

Kennedy & Ebert, JCO 2017, PMID: 28297619
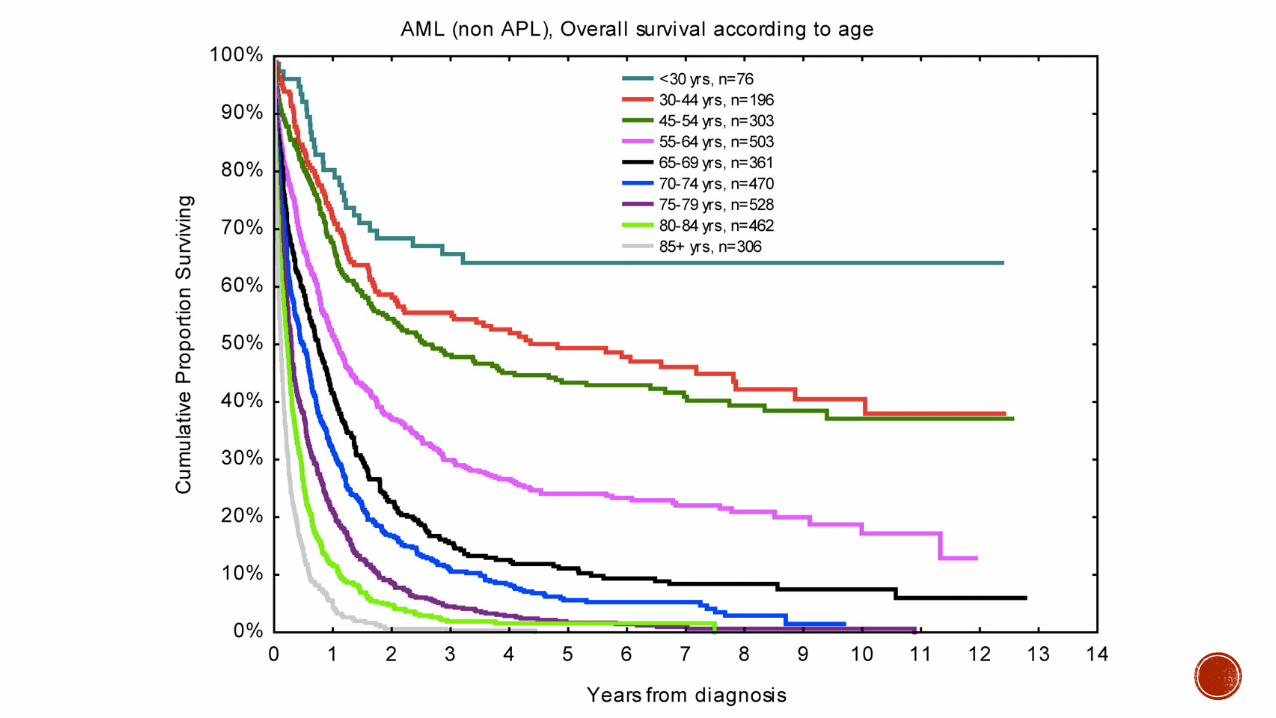
Y e a r s
Ove
rall
Surv
ival
(%)
0 2 4 6 8 1 0 1 2 1 40
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
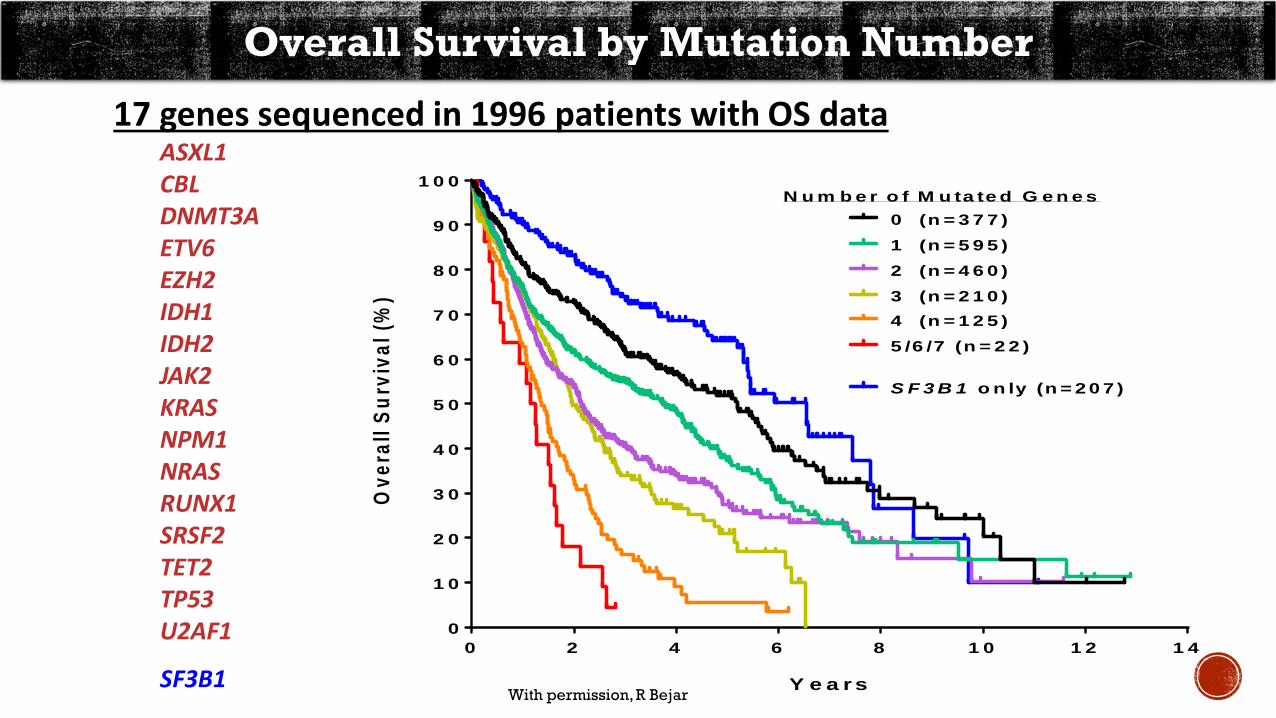
0 (n = 3 7 7 )1 (n = 5 9 5 )2 (n = 4 6 0 )3 (n = 2 1 0 )4 (n = 1 2 5 )5 /6 /7 (n = 2 2 )
S F 3 B 1 o n ly (n = 2 0 7 )
N u m b e r o f M u ta te d G e n e s
Overall Survival by Mutation Number
17 genes sequenced in 1996 patients with OS dataASXL1CBLDNMT3AETV6EZH2IDH1IDH2JAK2KRASNPM1NRASRUNX1SRSF2TET2TP53U2AF1
SF3B1With permission, R Bejar
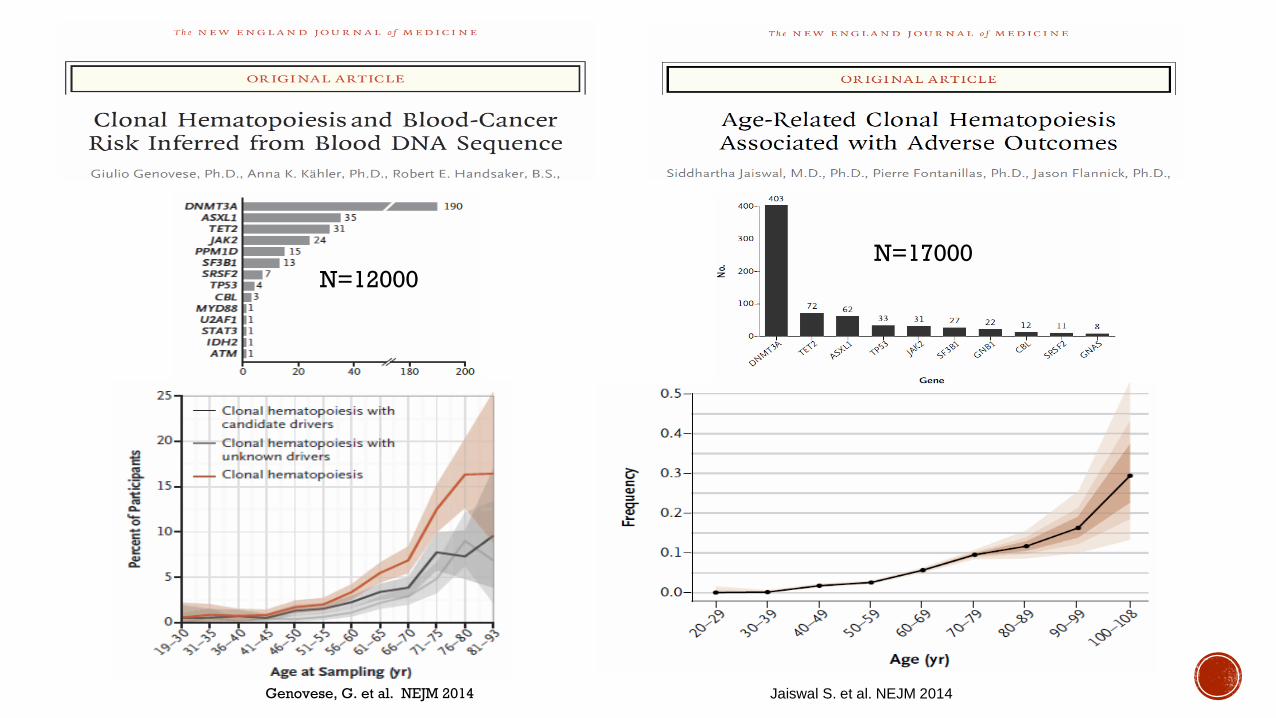
Genovese, G. et al. NEJM 2014 Jaiswal S. et al. NEJM 2014
N=12000N=17000

Genovese, G. et al. NEJM 2014 Jaiswal, S. et al. NEJM 2017
HR 12.9
HR 1.4
CHD: HR 2.0 (4 x MI)Ischemic stroke: HR 2.6

Non-clonal ICUSCHIP CCUS LR-MDS HR-MDS
Traditional ICUS MDS by WHO 2008
Clonality
Dysplasia
Cytopenias
Overall Risk
+ – ++ ++ ++
–/+ – – + ++
– + + + ++
Very Low Very Low Low (?) Low High
BM Blast % < 5% < 5% < 5% < 5% 5-19%
Are these two the same?Does morphologic dysplasia matter?
CCUS = clonal cytopenias of undetermined significance; ICUS = idiopathic cytopenias of undetermined significance; CHIP = clonal hematopoiesis of indeterminate potential; LR = lower risk, HR = higher risk

Some Somatic Mutations Matter More:
CCUS
ICUS
• n=154 patients with cytopenia of undetermined significance10-year cumulative probabilities of progression CCUS vs ICUS:
95% vs 9% P < .001
Evolution toheme neoplasm
10-20%/year MDS, <5% blasts
Survival
CCUS with:• SF3B1• ZRSR2• TET2/DNMT3A/ASXL1
+ 1 other
Malcovati L et al. Blood 2017
Somatic mutations are found in virtually all cytogenetically normal MDS patients and can be used for diagnosis and prognosis Insights into pathogenesis and therapeutic targeting
CHIP is found in 10% age > 70 in general population and is a significant risk factor for hematologic cancer (1% risk/year), all cause mortality, CHD, ischemic stroke and premature MICCUS is a risk factor for MDS and specific mutation patterns ……survival tantamount to MDS Longer follow up needed
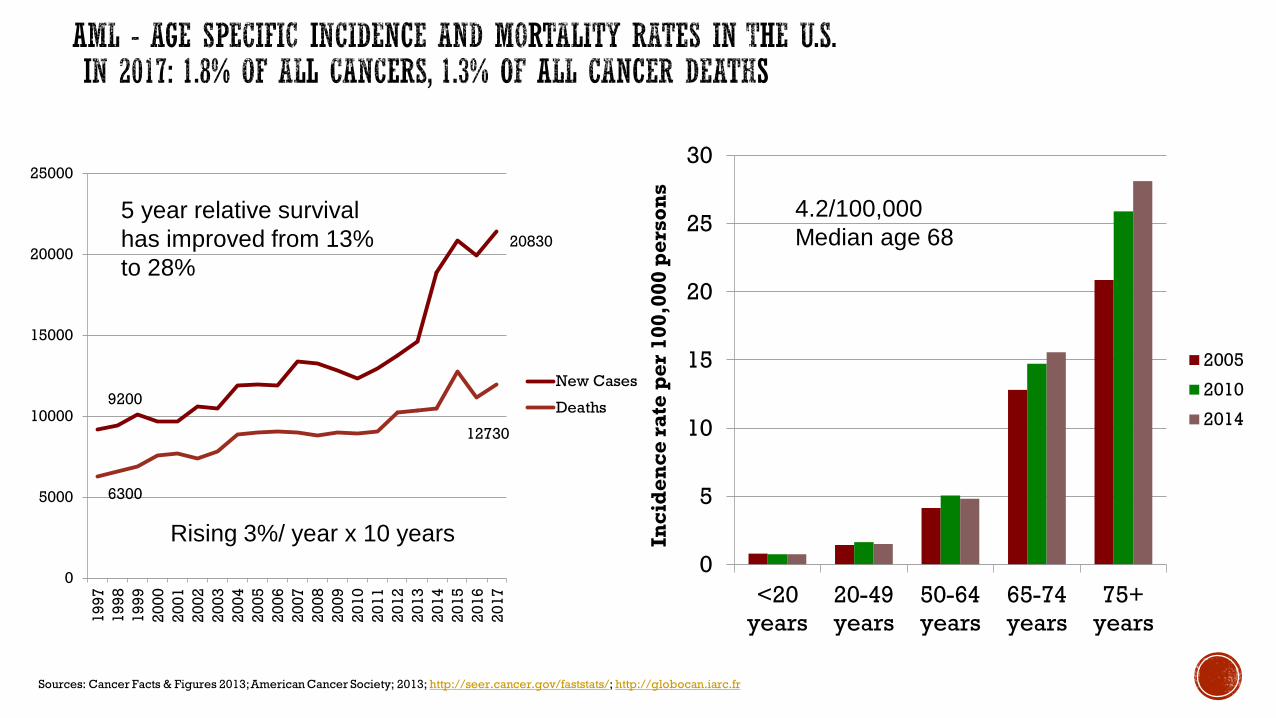
18Sources: Cancer Facts & Figures 2013;American Cancer Society; 2013; http://seer.cancer.gov/faststats/; http://globocan.iarc.fr
0
5
10
15
20
25
30
<20years
20-49years
50-64years
65-74years
75+years
Inci
den
ce r
ate
per
100
,000
per
son
s
2005
2010
20149200
20830
6300
12730
0
5000
10000
15000
20000
25000
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
New Cases
Deaths
5 year relative survival has improved from 13% to 28%
Rising 3%/ year x 10 years
4.2/100,000Median age 68


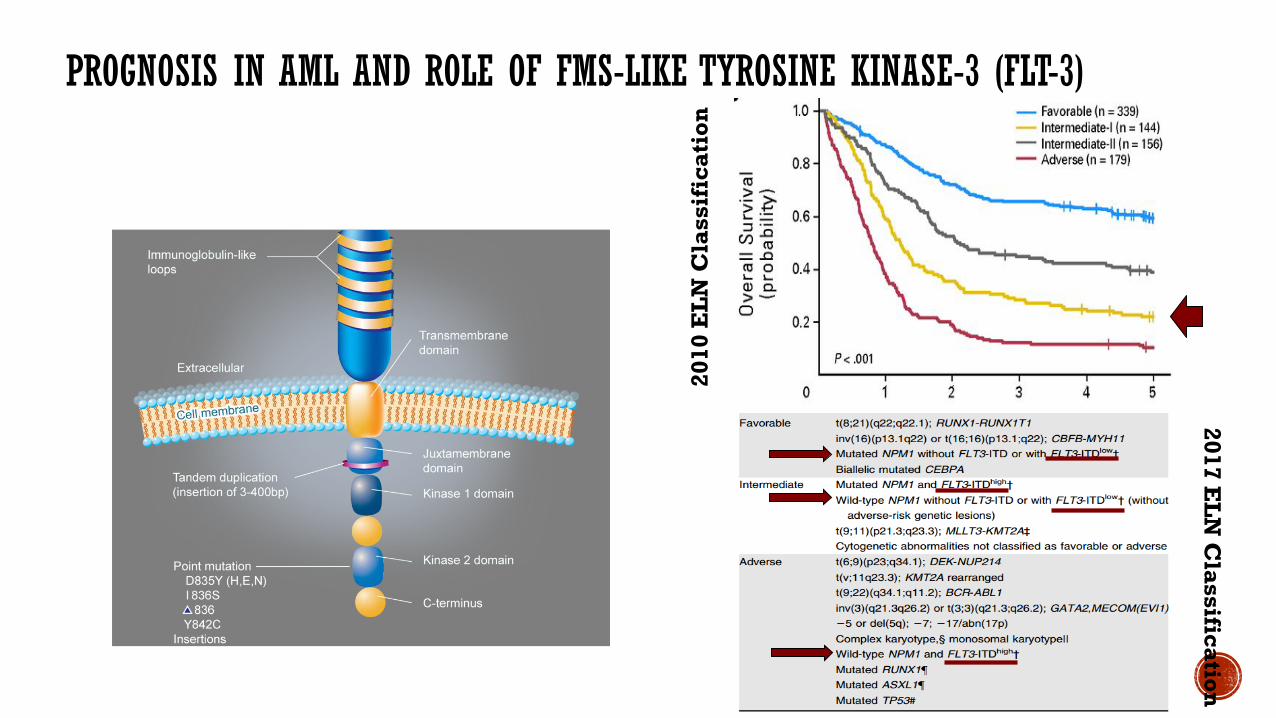
PROGNOSIS IN AML AND ROLE OF FMS-LIKE TYROSINE KINASE-3 (FLT-3)
2010
EL
N C
lass
ific
atio
n
2017 EL
N C
lassification

Potent FLT3 inhibitor but also inhibits other tyrosine kinases Modest single agent activity in relapsed AML RATIFY study evaluated its benefits in FLT3 mutated

PROTOCOL THERAPY Induction: daunorubicin 60 mg/m2 IVP days 1-3, cytarabine 200 mg/m2/d d 1-7 via IVCI, midostaurin 50 mg po bid or placebo days 8-21marrow on day 21. If residual AML, repeat above
Consolidation ( 4 cycles): cytarabine 3 gm/m2 over 3h q 12h days 1, 3, and 5midostaurin 50 mg po bid or placebo days 8-21
Maintenance: midostaurin 50 mg po bid or placebo days 1-28 x 12 cyclesTransplant not specifically mandated

RATIFY: CONSORT DIAGRAM
Stone R. et al. NEJM 2017

CR RATE HIGHER WITH MIDO
MIDO(N=360)
PBO(N=357)
Fisher’s exact p
(2-sided)Initial CR (within 60 days) 212 191Rate 59% 54% 0.15Time to CR, median (range) 35 days (20-60) 35 days (20-60)
Initial CR (at any time) 244 216Rate 68% 61% 0.04Time to CR, median (range) 37 days (20-192) 36 days (20-108)
Stone R. et al. NEJM 2017

OVERALL SURVIVAL - PRIMARY ITT ANALYSIS
• 5 year survival rate: Mido 50.9% vs. PBO 43.3%• Median follow-up time for survivors: 56.7 mo (range: 0.1, 79.2)
Stone R. et al. NEJM 2017

OVERALL SURVIVAL POST-TRANSPLANT: IMPROVED POST MIDO IN CR
All Transplants SCT in/outside of CR1
NE: not estimable
Stone R. et al. NEJM 2017

Many more under evaluation in combination with chemotherapy upfront or relapse, as maintenance post chemotherapy or post allogeneic stem cell transplantNow SOC to use for FLT3 mutated AML which comprises roughly 25% of all AMLSurvival benefit appears to be seen in those that undergo an allogeneic stem cell transplant

APL now treated with arsenic and ATRA (NO CHEMO!) Reduced intensity allogeneic stem cell transplants non-inferior to
myeloablative : age not restricted to < 70 Maintenance or vaccines post transplant
Haplo-identical transplants CPX-351 Resurgence of gemtuzumab-ozogamycin (anti-CD33 MoAb + calichymycin) RCT: 7+3 +/- Gem - EFS 9.5 mos versus 17.3 months
Enasidinib- for IDH mutated AML Venetoclax (anti-Bcl2 inhibitor) added to hypomethylating agents or LDAC


Multiple Myeloma: 6.6/100,00010% of all Heme cancers
50% survive 5 years (70% with ASCT)



REVISED ISS STAGING SYSTEM
Palumbo A, et al. J Clin Oncol. 2015;33:2863-2869.
Definition
I
ISS stage I AND Normal LDH No t(4;14), t(14;16), or del(17p)
II Not stage I or III
III
ISS stage IIIAND Serum LDH > ULNOR With t(4;14), t(14;16), or
del(17p)
100
80
60
40
20
00 12 24 36 48 60 72
R-ISS I NRR-ISS II 83R-ISS III 43
Median OS, Mos
MosO
S (%
)
R-ISS Stage

MYELOMA TREATMENT PARADIGM
Induction
Induction followed by continuous therapy
Consolidation MaintenanceSCT
Elig
ible
SCT
Inel
igib
le
Dia
gnos
is a
nd R
isk
Stra
tific
atio
n
Tumor Burden

IFM prospective, randomized trial comparing conventional chemotherapy vs high-dose therapy and ASCT (N = 200)
Attal M, et al. N Engl J Med. 1996;335:91-97.
HIGH-DOSE THERAPY AS CONSOLIDATION IMPROVES OVERALL SURVIVAL BY 1 YEAR
Slide credit: clinicaloptions.com
15 30 45 60
25
50
75
100
OS
(%)
00
High doseConventional dose
Mos15 30 45 60
25
50
75
100
Even
t-Fre
e Su
rviv
al (%
)
00
High doseConventional dose
Mos

META-ANALYSIS OF 3 PHASE III TRIALS: OS IS IMPROVED WITH LENALIDOMIDEMAINT AFTER HIGH-DOSE MELPHALAN AND ASCT
26% reduction in risk of death; estimated 2.5-yr increase in median OS
Attal M, et al. ASCO 2016. Abstract 8001.
Median follow-up: 80 mos
100
80
60
40
20
0
OS
(%)
0 10 20 30 40 50 60 70 80 90 100 110 120Mos
N = 1209
Median OS, mos (95% CI)HR (95% CI)P value
Lenalidomide
NE(NE-NE)
Control
86.0(79.8-96.0)
0.74 (0.62-0.89).001
7-yr OS62%
50%

NON-TRANSPLANT ELIGIBLE: FIRST TRIAL: PFS WITH CONTINUOUS RD BEST, BUT NOT OS
HR:Continuous Rd vs MPT: 0.72 (P < .001)Continuous Rd vs Rd18: 0.70 (P < .001)
PFS OS
Benboubker L, et al. N Engl J Med. 2014;371:906-917.
Pts
(%)
100
80
60
40
20
0
Continuous Rd (n = 535) Rd18 (n = 541)MPT (n = 547)
Median PFS, Mos
25.520.721.2
0 6 12 18 24 30 36 42 48 54 60Mos
Pts
(%)
100
80
60
40
20
0
Continuous Rd (n = 535) Rd18 (n = 541)MPT (n = 547)
4-Yr OS, %595651
0 6 12 18 24 30 36 42 48 54 60
Mos
Survival has increased from 3-6 years…….still incurable Better prognostication guides different therapiesHDT/ASCT offers a 10-15% improvement in overall survival (roughly 1-
1.5 years)Maintenance after stem cell transplant with lenalidomide low dose
improves OS by 2.5 years but at expense of increased rate of secondary primary malignancies, neuropathy, myelosuppression, thrombosisNew oral proteosome inhibitors, monoclonal antibodies, PD-1 inhibitors
are showing promise in the relapsed/refractory patients – toxicities Achieving a deep response to therapy (CR or VGPR) associated with
improved overall survival- doublet versus triplet therapy

The decision followed the FDA’s Oncologic Drugs Advisory Committee’s unanimous vote to
recommend the immunotherapy for approval; in remarks, one panel member called it the “most
exciting thing I’ve seen in my lifetime.”
This approval “marks an important shift in the blood cancer treatment paradigm,” commented Kenneth Anderson, MD, president of the American Society of Hematology (ASH), in a press release. “We now
have proof that it is possible to eradicate cancer by harnessing the power of a patient’s own immune
system.”

AG recognition domain from MoAB
Intracellular T cell signalling and costimulatory domains


Multicenter, open-label, single-arm phase II study
Primary endpoint: ORR (CR + CRi) within 3 mos, assessed by IRC 4-wk maintenance of remission required
Secondary endpoints: MRD status, DoR, OS, cellular kinetics, safety
Pts aged 3-21 yrs* with B-cell ALL; ≥ 5% BM lymphoblasts; no isolated extramedullary disease
relapse, prior CD19-directed therapy, or prior gene therapy
(N = 81)
Single-Dose CTL0192.0-5.0 x 106/kg IV if ≤ 50 kg
1.0-2.5 x 108 IV if > 50 kg(n = 62†)
Grupp SA, et al. ASH 2016. Abstract 221.
Fludarabine30 mg/m² IV QD for 4 doses
Cyclophosphamide500 mg/m² IV QD for 2 doses
*From 3 yrs at screening to 21 yrs at initial diagnosis.
†14 pts discontinued before infusion: deaths (n = 6), manufacturing failures (n = 5), AEs (n = 3).

Grupp SA, et al. ASH 2016. Abstract 221.
*Interim analysis set: first 50 pts infused with CTL019 with 3-mo follow-up. †P < .0001. ‡Full analysis set: all pts infused with CTL019.
Outcome CTL019 (n = 50*)ORR (CR + CRi) within 3 mos (with MRD < 0.01% in BM), % (95% CI) 82 (69-91)†
Best overall response, %CRCRi
6814
OS6 mos, % (95% CI)Median, mos (95% CI)
89 (76-95)‡
NE (8.6-NE)‡
Duration of remission6 mos, % (95% CI)Median, mos (95% CI)
62 (36-78)NE (4.8-NE)

Advantages:Offers cellular immunotherapy in heavily pre-treated hematologic cancers
(ALL, DLBCL……….CLL, HL, MM, solid tumours) High rate and durable CRs ……Cure? Replace allogeneic stem cell transplants?
DisadvantagesOnly specialized centersCost- ½ million dollarsNot off the shelf Cytokine release syndrome- 59% ICU x 8 daysNeuropsychiatric events- serious in 18% Prolonged hypogammaglobulinemiaDurability unknown
Slide credit: clinicaloptions.com

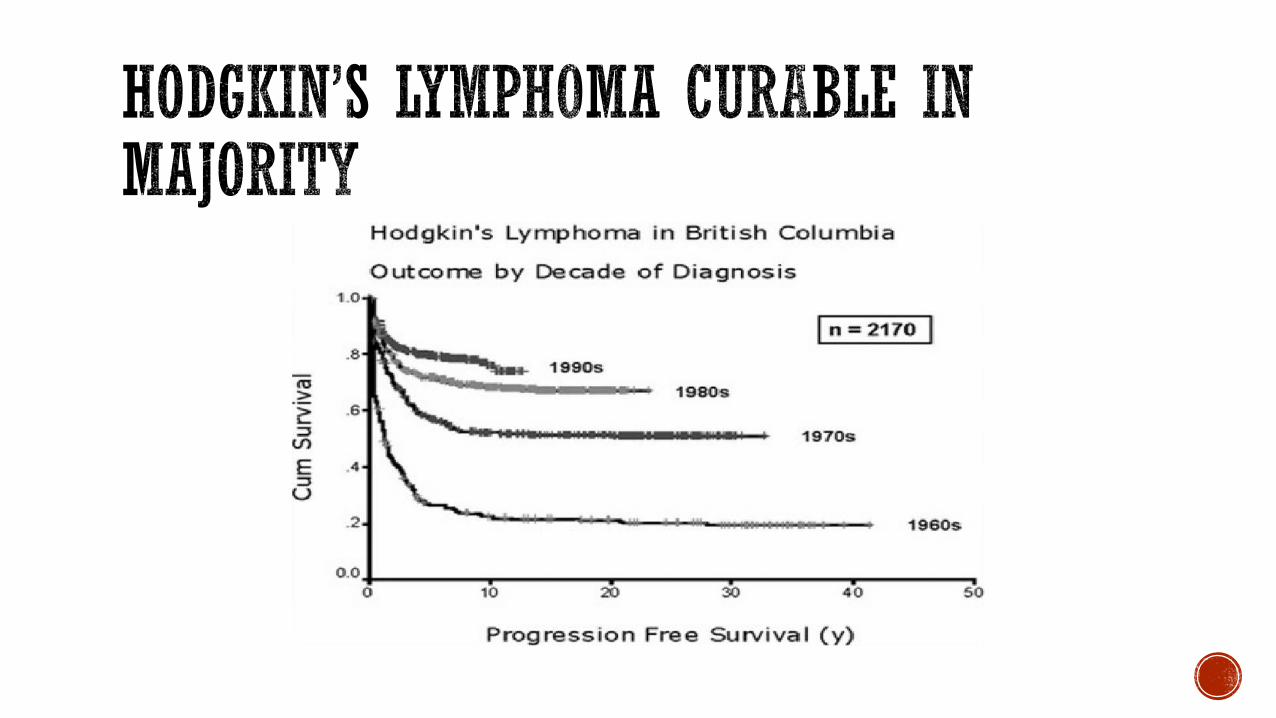

25% will be refractory/relapse Younger patients (39) Salvage chemotherapy + ASCT
curable in 50% Brentuximab-Vedotin if relapse
Older patients: Brentuximab-Vedotin or palliative chemotherapy Brentuximab-Vedotin: monoclonal
antibody-antitubulin agent 75% ORR (CR 34%) 2 year OS 65%



Study Drug N ORR Miscell
Checkmate 2051
Phase 2Nivolumab 3 mg/kg IV q 2 weeks
80 66%CR: 7%
Failed both ASCT and Brentuximab
Keynote-0872
Ongoing Phase 2Pembrolizumab 200 mg IV q 3 weeks x 2 years
210(Results for 60 cohorts 1-2)
70-80%CR 20-27%
1. Failed SCT + BV2. Chemo resistant + Failed BV3. Failed ASCT
Nivolumab: Accelerated approval by FDA May 2016 for relapsed post ASCT + BV
1. Younes, A. Lancet Oncol 20162. Chen R. et al, JCO 2016 34:15_suppl, 7555-7555

Fig 1. Response to treatment. (A) Maximum percentage change from baseline in target lesions. (B) Change from baseline in target lesions. (C) Treatment exposure and response duration. Three patients had a formal response assessment before the protocol-required time point of 12 weeks. One patient only received one dose of pembrolizumab, discontinued treatment because of toxicity at 4 weeks, and had nonprotocol scans to assess response, which showed CR. The other two patients had nonprotocol scans to confirm the clinical impression of progressive disease before the 12-week time point. Abbreviations: CR, complete response; PD, progressive disease; PR, partial response; SD, stable disease.
Published in: Philippe Armand; Margaret A. Shipp; Vincent Ribrag; Jean-Marie Michot; Pier Luigi Zinzani; John Kuruvilla; Ellen S. Snyder; Alejandro D. Ricart; Arun Balakumaran; Shelonitda Rose; Craig H. Moskowitz; JCO 2016, 34, 3733-3739.DOI: 10.1200/JCO.2016.67.3467Copyright © 2016 American Society of Clinical Oncology
Keynote 013- phase 1, n=31, 4+ lines of therapy, 71% post ASCT

Ongoing trials in aggressive and indolent B cell lymphomas, MM, MDS, AML, CLLWell tolerated but immune related adverse events GI, derm, hepatic, endocrine
Duration of treatment unknownDurability of response unknownHD: Being moved up earlier in combination with chemotherapy or other
immune checkpoint inhibitors Expensive


BCR signaling is required for tumor expansion and proliferation BTK is an essential element of the
BCR signaling pathway[28]
Inhibitors of BTK block BCR signaling, diminish proliferation, impair adhesion and migration and induce apoptosis[29]
Targeted inhibition of BTK is a novel approach for the treatment of B-cell malignancies
LYN
SYK
BCR
BTK
PLCγ2
PKC
PI3KDelta
AKT
mTOR
p70s6k elf4E
GSK-3 NF-kβPathway
Herman SEM, et al. Blood. 2011;117:6287-6296. 30. Davis RE, et al. Nature. 2010;463:88-92.

Forms a specific bond with cysteine-481 in BTKHighly potent BTK inhibition[30]
Orally administered with once-daily dosing resulting in 24-hr target inhibition[31]
No cytotoxic effect on T cells or NK cells[32]
In CLL cells, promotes apoptosis and inhibits CLL cell migration and adhesion[33,34]
31. Honigberg LA, et al. Proc Natl Acad Sci U S A. 2010;107:13075-13080. 32. Advani R, et al. J Clin Oncol. 2013;31:88-94. 33. Herman SE, et al, Blood. 2011;117:6287-6296. 34. Ponader S, et al. Blood. 2012;119:1182-21189. 35. de Rooij MF, et al. Blood. 2012;119:2590-2594.
N
N NN
N
O
NH2
O

Treatment Naive ≥ 65 yrsIbrutinib
420 mg/day or 840 mg/day (n = 31)
Relapsed/Refractory Ibrutinib
420 mg/day or 840 mg/day (n = 61)
Patients with CLL/SLL treated with ibrutinib
monotherapy* and ECOG PS ≤ 2
(N = 116)
Enrolled May 2010 - July 2011
36. Byrd JC, et al. ASH 2012. Abstract 189.
A multicohort phase Ib/II trial
High-risk† Relapsed/RefractoryIbrutinib
420 mg/day (n = 24)
20.3 mosmedian follow-up
22.1 mosmedian follow-up
14.7 mosmedian follow-up
*Patients with SLL not included in current analysis†Defined as progression of disease < 24 mos after initiation of a chemoimmunotherapy regimen or failure to respond.
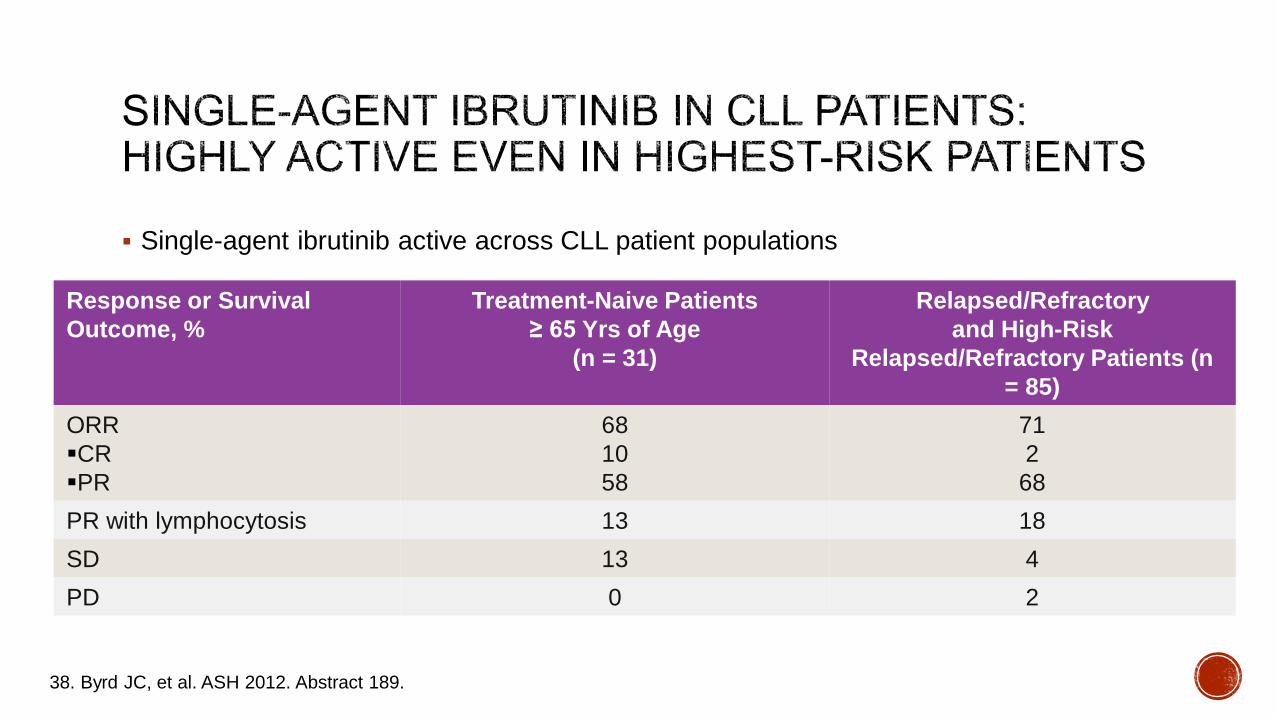
Single-agent ibrutinib active across CLL patient populations
38. Byrd JC, et al. ASH 2012. Abstract 189.
Response or Survival Outcome, %
Treatment-Naive Patients ≥ 65 Yrs of Age
(n = 31)
Relapsed/Refractory and High-Risk
Relapsed/Refractory Patients (n = 85)
ORRCRPR
681058
712
68PR with lymphocytosis 13 18SD 13 4PD 0 2

Ibrutinib monotherapy superior to chlorambucil for ORR, EFS, PFS, and OS Risk of death reduced by 84% with favorable AE profile
Burger JA, et al. N Engl J Med. 2015;373:2425-2437. Slide credit: clinicaloptions.com
100
80
60
40
20
00 6 12 18 273 9 15 21 24
PFS According to Investigator Assessment
Mos
Pts
With
PFS
(%)
HR: 0.09 (95% CI: 0.04-0.17; P < .001)
Chlorambucil15.0
IbrutinibNR
Median, mos
100
80
60
40
20
0
Pts
Who
Sur
vive
d (%
)
0 6 12 18 273 9 15 21 24Mos
HR: 0.16 (95% CI: 0.05-0.56; P = .001 by log-rank test)
ChlorambucilIbrutinib
OS

PFS benefit in all subgroups analyzed, including bulky disease, IgVH mutation status, no. prior therapies, presence of del(11q)
OS results confounded by crossover of 90 (31%) pts in placebo arm to ibrutinib arm after PD
Chanan-Khan AAA, et al. Lancet Oncol. 2015;[Epub ahead of print].
100
80
60
40
20
0
PFS
(%)
320 4 8 16 20 24 2812Mos
Placebo + BR(median PFS: 13.3 mos)
Ibrutinib + BR(median PFS: NR)
100
80
60
40
20
0
OS
(%)
320 4 8 16 20 24 2812Mos
Placebo + BR
Ibrutinib + BR
PFS OS
HR: 0.203 (95% CI: 0.150-0.276;P < .0001)
Median OS NR in either armHR: 0.628 (95% CI: 0.385-1.024;P = .0598)
Slide credit: clinicaloptions.com

IbrutininibCLLMantle Cell LymphomaWaldenstromsMacroglobulinemiaMarginal Zone Lymphoma
IdelalisibPreviously treated CLL + RituximabFollicular and SLL who have received 2 prior therapies

Practical recommendations for the clinic
Ibrutinib• Grade 1 bruising is frequent but harmless• Antiplatelet or anticoagulation (DOAC or
LMWH) therapy appears safe• Avoid combined antiplatelet and
anticoagulation therapy• Withhold ibrutinib 3-7 days before and after
invasive procedures• Check for atrial fibrillation regularly• Hypertension may occur even later during
therapy• Check blood counts regularly during first
months
Idelalisib• PJP prophylaxis and regular CMV
monitoring are mandatory• Take diarrhea seriously and handle
according to Figure 3• Be aware of the low but potentially life
threatening risk of pneumonitis• Check liver enzymes in the first 3
months and handle elevations according to Figure 5
• Check blood counts regularly during first months
De Weerdt, I. et al. Haematologica 2017


OUTCOMES WITH SECONDARY OR THERAPY RELATED AML ARE INFERIOR
67Granfeldt-Osgard, et al. J Clin Oncol. 2015;33:3641
Time Since AML Diagnosis (years)
0
0.2
0.4
0.6
0.8
1.0
Surv
ival
(pro
babi
lity)
1 3 5 7 9 11 13
De novo AMLsAML, MDSsAML, non-MDStAML

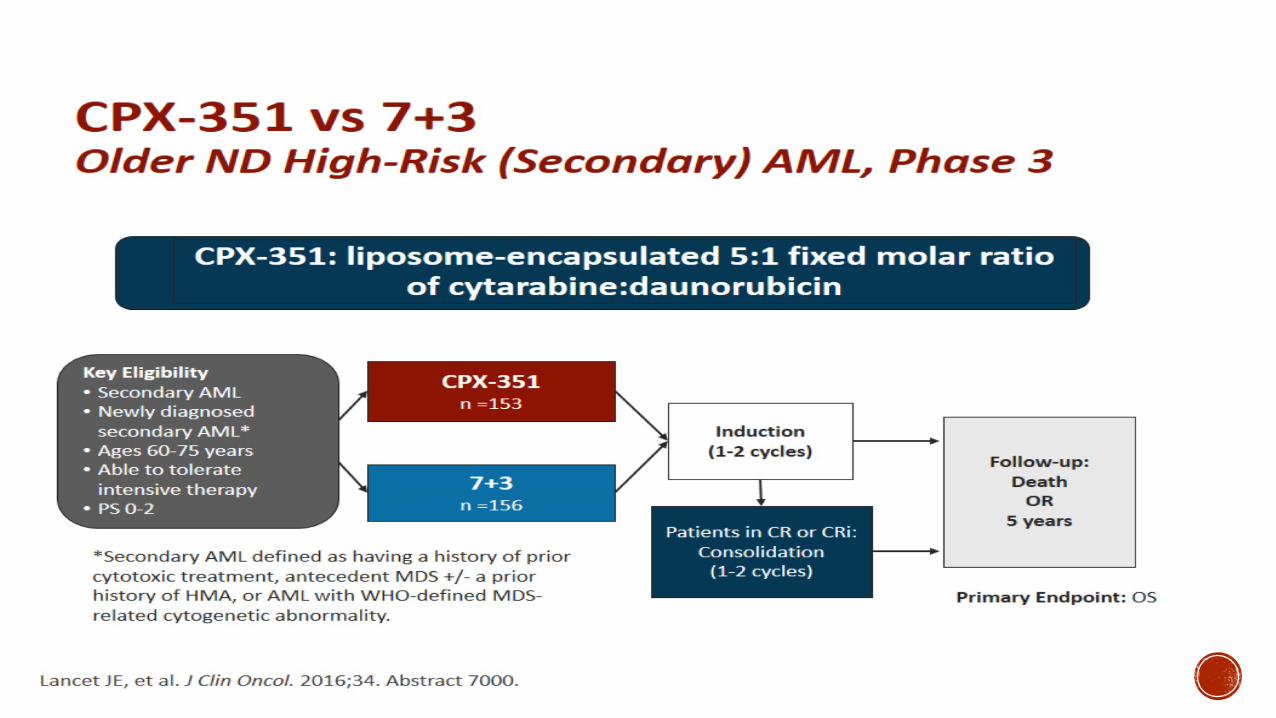

70Lancet J et al. ASCO, 2016

71
KAPLAN-MEIER CURVE FOR OVERALL SURVIVAL LANDMARKED AT STEM CELL TRANSPLANT ITT ANALYSIS POPULATION
100
80
60
40
20
03 6 9 12 15 18 21 24 27 30 33 36
Months from Randomization
Surv
ival
(%)
Events/NCPX-351
7+318/5226/39
Not Reached10.25 (6.21, 16.69)
Median Surv. (95% CI)
4631
4027
3420
2715
207
154
91
61
30
00
00
CPX-3517+3
5239
Hazard Ratio = 0.46p-value = 0.0046
0
Lancet J et al. ASCO, 2016
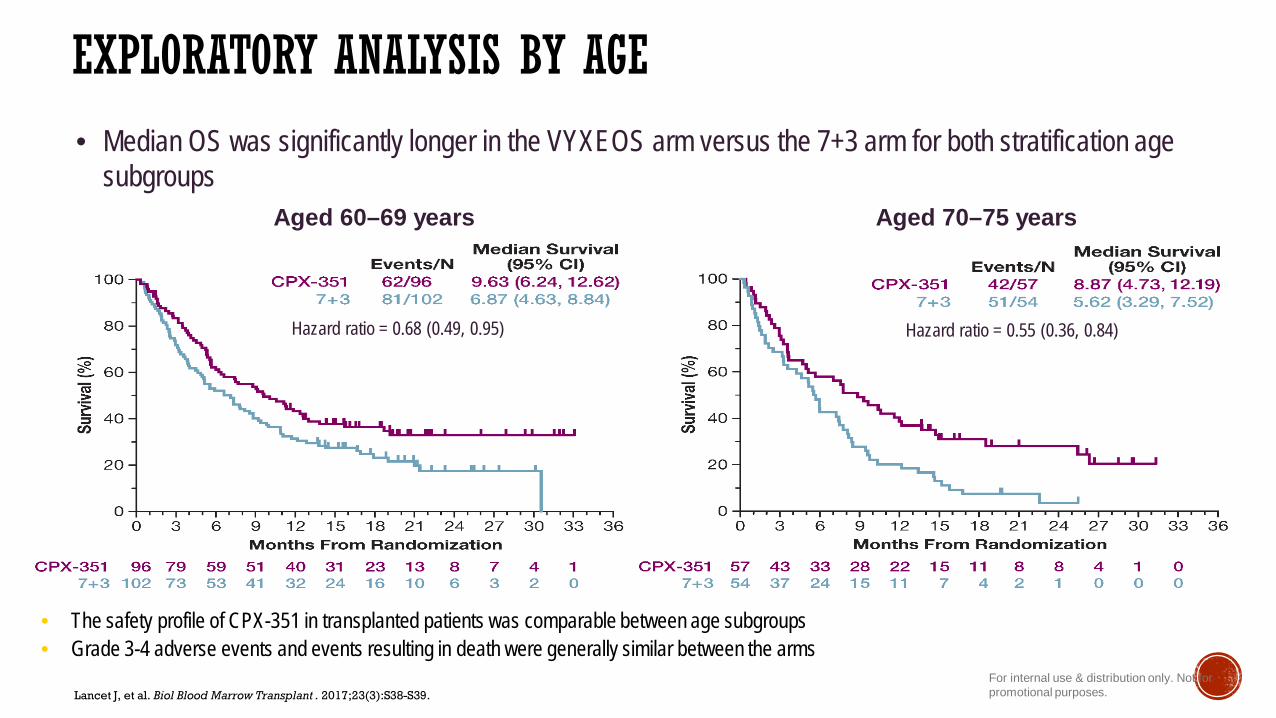
EXPLORATORY ANALYSIS BY AGE
Aged 60–69 years Aged 70–75 years
Hazard ratio = 0.55 (0.36, 0.84)Hazard ratio = 0.68 (0.49, 0.95)
• Median OS was significantly longer in the VYXEOS arm versus the 7+3 arm for both stratification age subgroups
Lancet J, et al. Biol Blood Marrow Transplant . 2017;23(3):S38-S39.For internal use & distribution only. Not for promotional purposes.
• The safety profile of CPX-351 in transplanted patients was comparable between age subgroups• Grade 3-4 adverse events and events resulting in death were generally similar between the arms


![[*] Chairman, History of Medicine Department,ِ](https://static.fdocument.pub/doc/165x107/5891ad0e1a28abfa4d8b6ca2/-chairman-history-of-medicine-department.jpg)