
articol Studia
10
1993; 73:447-454. PHYS THER. Stratford and Carolyn Gowland Julie Sanford, Julie Moreland, Laurie R Swanson, Paul W Motor Performance in Patients Following Stroke Reliability of the Fugl-Meyer Assessment for Testing http://ptjournal.apta.org/content/73/7/447 online at: The online version of this article, along with updated information and services, can be found Collections Tests and Measurements Stroke (Neurology ) Stroke (Geriatrics) Motor Control and Motor Learning in the following collection(s): This article, along with others on similar topics, appears e-Letters "Responses" in the online version of this article. "Submit a response" in the right-hand menu under or click on here To submit an e-Letter on this article, click E-mail alerts to receive free e-mail alerts here Sign up by guest on October 3, 2013 http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013 http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013 http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013 http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013 http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013 http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013 http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013 http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013 http://ptjournal.apta.org/ Downloaded from
Transcript of articol Studia

7/27/2019 articol Studia
http://slidepdf.com/reader/full/articol-studia 1/10
1993; 73:447-454.PHYS THER.
Stratford and Carolyn GowlandJulie Sanford, Julie Moreland, Laurie R Swanson, Paul WMotor Performance in Patients Following StrokeReliability of the Fugl-Meyer Assessment for Testing
http://ptjournal.apta.org/content/73/7/447online at:The online version of this article, along with updated information and services, can be found
Collections
Tests and MeasurementsStroke (Neurology)Stroke (Geriatrics)Motor Control and Motor Learning
in the following collection(s):This article, along with others on similar topics, appears
e-Letters"Responses" in the online version of this article."Submit a response" in the right-hand menu underor click onhereTo submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alertshereSign up
by guest on October 3, 2013http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013http://ptjournal.apta.org/ Downloaded from by guest on October 3, 2013http://ptjournal.apta.org/ Downloaded from

7/27/2019 articol Studia
http://slidepdf.com/reader/full/articol-studia 2/10
1993; 73:447-454.PHYS THER.
Stratford and Carolyn GowlandJulie Sanford, Julie Moreland, Laurie R Swanson, Paul WMotor Performance in Patients Following StrokeReliability of the Fugl-Meyer Assessment for Testing
Cited by
http://ptjournal.apta.org/content/73/7/447#otherarticlesarticles:This article has been cited by 54 HighWire-hosted
InformationSubscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
by guest on October 3, 2013http://ptjournal.apta.org/ Downloaded from

7/27/2019 articol Studia
http://slidepdf.com/reader/full/articol-studia 3/10
Research Report
Reliability of the Fugl-Meyer Assessment for Testing
Motor Performance in Patients Following Stroke
Key Words: FuglMeyer assessment, Motor performance, Reliability, Stroke,
Background a nd Purpose . The pulpose of thb study was to establish the inter-
rater reliability of assessments made with the Fugl-Meyer evaluation of physical
per$omzance in a rehabilitation setting. Suwects. Twelve patients (7male,5
female): aged 49 to 86 years @=66), who had sustained a cerebrovascular acci-
Stroke is a major cause of mortality average annual mortality rate for
and disability in many countries. The stroke per 100,000 people is 100.4 in
Julie Sanford
Juiie MoreiandLaurie R SwansonPaul W Stratford
- - - - - - -J Sanford, PT, s Research Coordinator, Rehabilitation Services, St Pcter's Ilospital, 88 Maplewood
Ave. Hamilton, Ontario, Canada L8N 325, and Assistant Clinical Professor, School of Occupational
Therapy and Physiotherapy, Faculty of Health Sciences, McMaster University, 1200 Main St W,
Hamilton, Ontario, Canada L8N 325. Address all correspondence to Ms Sanford at the first address.
dent participated in the study. All patients were admitted consecutively to a reha- Carolyrr Gowiandbilitation center and were between 6 days and 6 months poststroke. Metboa%.Three pbysical therapists, each with more than 10 years of expm'ence, assessed the
patients in a randomized and balanced order using thjs assessment. The therapists
standardized the assessment approach prior to the study but did not discuss the
procedure once the study began. Results. The overall reliability was high (overall
intrac lm correlation coeficient=.96), and the intraclm correlation coeficients
for the subsections of the assessment var iedj km .61 or pain to .97 or the upper
extremity. C d u s i o n and Dtscusston. The relative mm'ts of using the Fugl-
Meyer assessment as a research tool versus a clinical assessment or stroke are
discussed. [SanfordJ MorelandJ Swanson LR, et al. Reliability of the Fugl-Meyer
assessment for testing motor peformance in patients following stroke. Phys Ther.
1993;73:447454.]
J Moreland, PT, s Physical Therapist, Physiotherapy Department, Chedoke-McMaster Hospitals,
Chedoke Division, Hamilton. Ontario, Canada LEN 325, and Clinical Lecturer, School of Occupa-
tional Therapy and Physiotherapy, Faculty of Health Sciences, McMaster University.
LR Swanson, PT,s Doctoral Candidate, Medical Sciences Program, McMaster University
PW Stratford,PT, s Assistant Professor, School of Occupational Therapy and Physiotherapy, Faculty
of Health Sciences, McMaster University.
C Gowland PT, s Associate Professor, School of Occupational Therapy and Physiotherapy, Faculty
of Health Sciences, McMaster University.
This study was approved by the Research Project Advisory Committee of McMaster University and
Chedoke-McMaster Hospitals.
This research was supported by Grant 6606-3771-45, National Health Research and Development
Program, Ottawa, Ontario, Canada.
This article wa s submittedJuly 20, 1992, and wa s accepted March 17, 1993.
the United States, 116.2 in England
and Wales, and 96.6 in Canada.' Data
compiled from a number of surveys
in the United States show that the
annual incidence is approximately 100
to 150 per 100,000 people.' Following
a stroke, patients usually receive in-
tensive therapy to promote motor
recovery and help them cope with
their disability.
Reliable and valid measurements of
sensorimotor status are required for
clinical decision-making and research
purposes. One measure that has been
extensively discussed is the Fugl-
Meyer evaluation of physical perfor-
mance.* The Fugl-Meyer assessment
was developed to assess physical
recovery following stroke. It was pri-
marily developed from the earlier
works of Twitchell3 and Br~nnstrom.~
36 / 447 Physical Therapy/Volume 73, Number 7/July 1993

7/27/2019 articol Studia
http://slidepdf.com/reader/full/articol-studia 4/10
Twitchell examined the ontogeneticconcept of motor recovery, through
the assessment of sequen ced reflexand synergistic patterned movements
seen in patients recovering fromstroke.3 Based o n this reco very se-quence, Brunnstrom identified six
sequences o f temporal, stepwisestages as a method of assessing moto rrecovery in patients with hemiplegia
following stroke.* In addition t o mo-tor performance, balance, sensation,
range of movement, and pain are also
assessed by the Fugl-Meyer items,which examine volitional mo vement
within syne rgies, partially ou t of syn-
ergy, and ind ependen t o f synergies.
The Fugl-Meyer motor assessment
includes items dealing with the sh oul-
de r, elbow, forearm, wrist, and handin the u ppe r extremity and the hip,
knee, and ankle in the lower extrem-
ity. Reflex activity is assessed in the
upper and lower extremities at the
beginning and e nd of the motor as-
sessment. Balance is examined in
sitting and standing . Sensation , evalu-
ated by light touch, is examined o ntwo surfaces in both the upper and
lower extremities, and position se nse
(lunesthesia) and range of motion(ROM) are tested on eig ht joints, four
in each extremity.2
The Fugl-Meyer assessmen t, which
consists of 155 items, is an im pair-ment measure. Impaimzent is definedas any loss or abnormality in psycho-
logical, physiological, o r an atomica lstructure o r function.5 With the Fugl-
Meyer assessment, each item is ratedon a three-point ordinal scale (2points for the detail being performed
completely, 1 point fo r the detail
being p erformed partially, and 0 fo r
the detail not being performed). Themaximum score that can be attainedis 226. The maximu m moto r perfor-
mance score is 66 points for the up-per extremity, 34 points for the low erextremity, 14 points for balance, 24
points for sensation, and 44 pointseach for passive joint motion and
joint pain. Joint pain is assessed bymoving the joint through its availableROM to assess whether pain occurs at
any point in the range. Fugl-Meyerassigned motor function scores to
items that assessed motor function
alone, with a total possible score o f100 points. Scores wer e gro upe daccording to the v arious levels of
impairment, which were as follows:
<50 points =severe moto r impair-
ment, 50-84 points=marked mo torimpairment, 85-95 points=m oderatemotor impairment, and 96-99
points=slight motor impairment."
The properties of this instrument
have been described by various au -
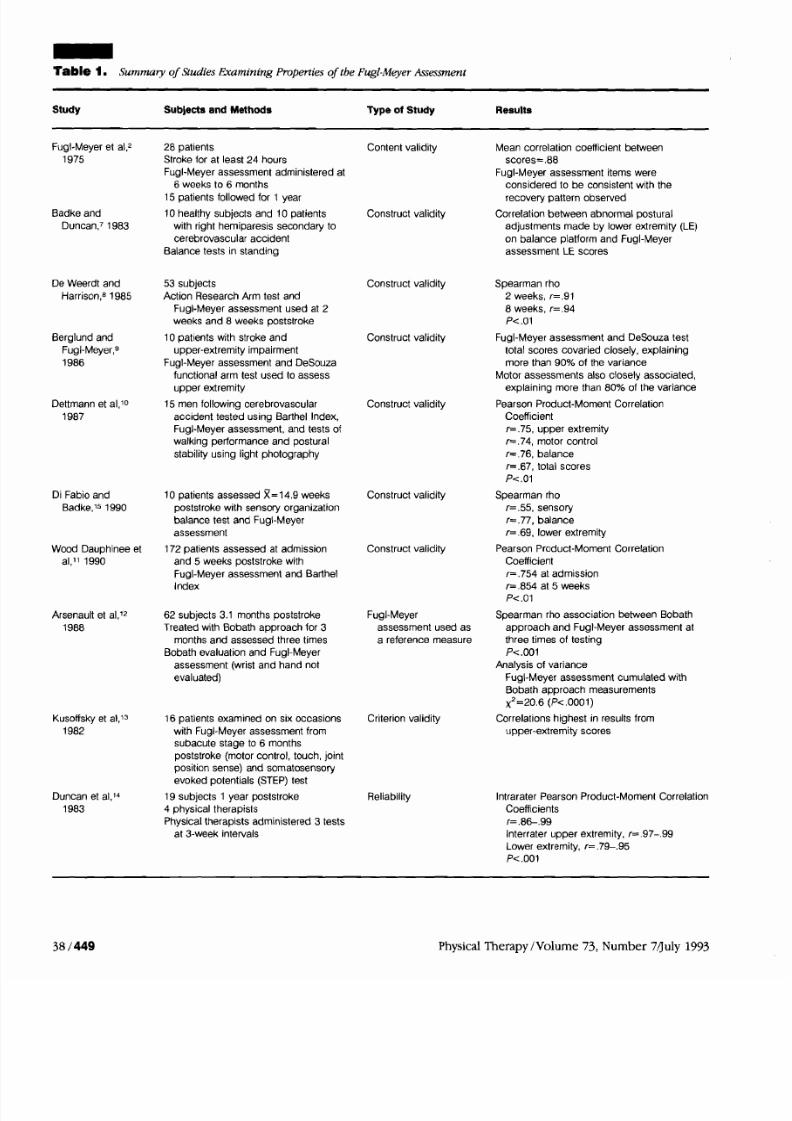
th0rs~,~- l5Tab. 1 ). Most of these
authors exam ined the validity of the
instrument. In the o riginal study byFugl-Meyer et a1,2 28 patients we re
assessed on five occasions during aI-year period following stroke. Themean correlation coefficient between
the u ppe r- and low er-extremity scoreswas .88.2 Oth er researche rs com pared
scores from the Fugl-Meyer assess-ment with data from the B arthel In-
dexloJ1 ; a B obath assessment'z;
upper-extremity function testss; and
tests for balance in standing, walking
perform ance, an d postu ral stability.10
The correlation coefficients reportedfrom these studies varied from .54 for
the total score to .94 for the upperextremity, thus providing evidence ofconstruc t validity.
Studies to date have examined theconstruct validity of the Fugl-Meyer
assessment in samples of chronicallydisabled patients following stroke.
Less work has been done to deter-mine the reliability of measurementsobtained w ith this assessment. Dun-
can et all* reported the interraterreliability of motor performance in
the upper and lower extremities and
the intrarater reliability of all sub-
scores and the total Fugl-Meyer scoreusing four physical therapists as evalu-
ators. The 19 patients in their studywere m ore than 1 year poststroke,with a mean time of 51 mon ths sincethe onset of their stroke. lntrarater
Pearson correlations for each su b-score and the total score varied from.86 to .99. he interrater Pearson
correlations for the moto r scores ofthe upper and lower extremities var-ied from .79 to .99. Because Duncan
et a1 studied subjects wh o w erechronically disabled following stroke,
the generalizability of their results
limited to similar patient populati
The study described in this report
examined the overall interrater reability and the reliability of each s
section of the Fugl-Meyer assessmadministered by three raters to patients underg oing active rehabilita
following stroke.
The purposes of our study were (to examin e the interrater reliabilit
measurements obtained with the
Fugl-Meyer assessment and (2) todetermin e the relevance of the as
ment for clinical and research p ur
poses. The specific aims o f the stuwere to determine whether the Fu
Meyer assessment is able to discri
nate amo ng patients when it is us
to evaluate patients' motor recove
following stroke an d to determine
magnitude of the measurement er
for the total score and score of th
subsections of the assessment. Thpriori level of acceptable reliabilit
among raters was set at an intraclacorr elatio n coefficient (ICC [2,1 ])ogreater than .80 for the total score
and subscores.
This study was pan of a larger stu
that examined the measurement p
erties of the Chedoke-McMasterStroke Assessment.16
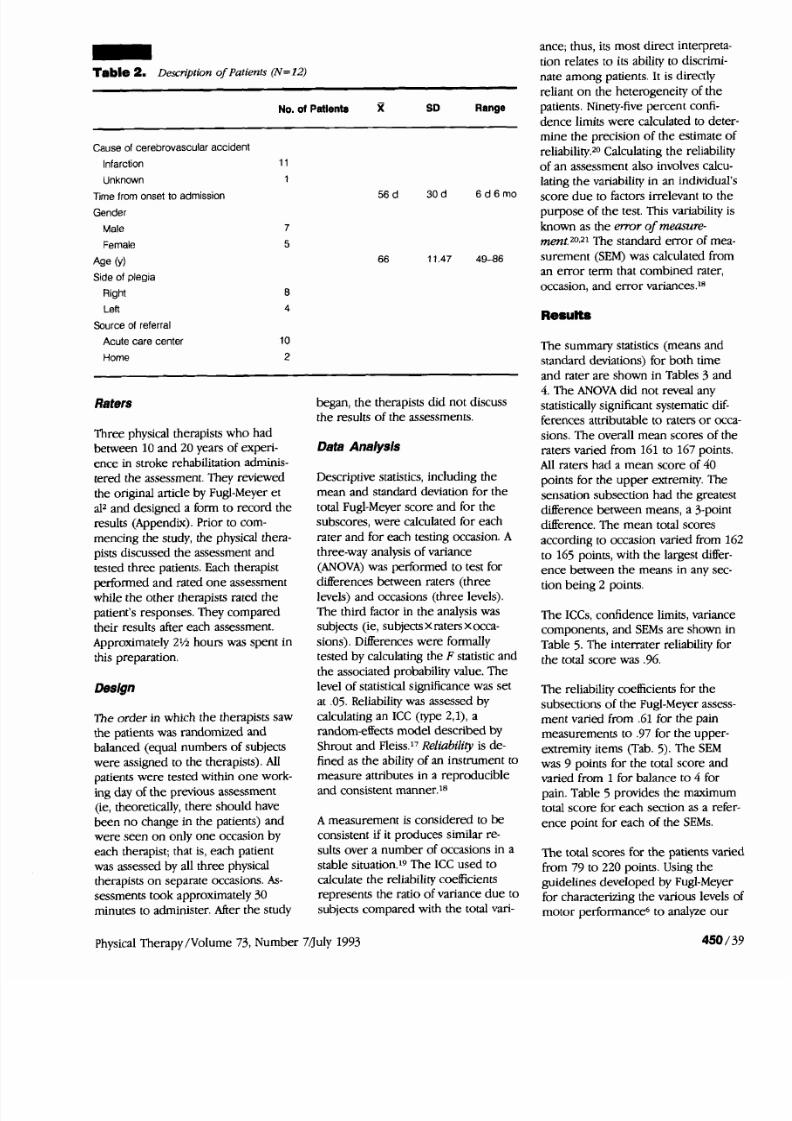
Subjects
Twelve patients consecutively adm
ted to the Chedoke-M cMaster Reh
itation C entre, Hamilton, Ontario,Canada, we re each assessed by thr
therapists (see T ab. 2 for descripti
of the patients) on separate occasiThe Chedoke-McMaster Rehabilita
Centre is a tertiary care setting atwhich patients are treated o n a dabasis by a m ultidisciplinary team.
average length of stay per patient 10 weeks. Patients were included ithey were less than 80 years of ag
were less than 6 months poststrok
and gave their consent to participin the study.
Physical Therapy /Volu me 73, Number
7/27/2019 articol Studia
http://slidepdf.com/reader/full/articol-studia 5/10
Table 1. Summay of Studies Examin ing Properties of the Fugl-MeyerAssessment
Study Subjects and Methods Type of Study Results
Fugl-Meyer et al,2 28 patients Content validity
1975 Stroke for at least 24 hours
Fugl-Meyer assessment administered at
6 weeks to 6 months
15 patients followed for 1 year
Badke and 10 healthy subjects and 10 patients Construct validity
Duncan,' 1983 with right hemiparesis secondary to
cerebrovascular accident
Balance tests in standing
De Weerdt and
Harrison,B 1985
Berglund and
Fugl-Meyer,g
1986
Dettmann et al,lo
1987
Di Fabio and
Badke,ls 1990
Wood Dauphinee et
al,ll 1990
Arsenault et al,l2
1988
Kusoffsky et al,13
1982
Duncan et al,l4
1983
53 subjects
Action Research Arm test and
Fugl-Meyer assessment used at 2
weeks and 8 weeks poststroke
10 patients with stroke and
upper-extremity mpairment
Fugl-Meyer assessment and DeSouza
functional arm test used to assess
upper extremity
15 men following cerebrovascular
accident tested using Barthel Index,
Fugl-Meyer assessment, and tests of
walking performance and postural
stability using light photography
10 patients assessed R= 14.9 weeks
poststroke with sensory organization
balance test and Fugl-Meyer
assessment
172 patients assessed at admission
and 5 weeks poststroke with
Fugl-Meyer assessment and Barthel
Index
62 subjects 3.1 months poststroke
Treated with Bobath approach for 3
months and assessed three times
Bobath evaluation and Fugl-Meyer
assessment (wrist and hand not
evaluated)
16 patients examined on six occasions
with Fugl-Meyer assessment from
subacute stage to 6 months
poststroke (motor control, touch, joint
position sense) and somatosensory
evoked potentials (STEP) test
19 subjects 1 year poststroke
4 physical therapists
Physical therapists administered 3 tests
at 3-week intervals
Construct validity
Construct validity
Construct validity
Construct validity
Construct validity
Fugl-Meyer
assessment used as
a reference measure
Criterion validity
Reliability
Mean correlation coefficient between
scores=.88
Fugl-Meyer assessment items were
considered to be consistent with the
recovery pattern observed
Correlation between abnormal postural
adjustments made by lower extremity (LE)
on balance platform and Fugl-Meyer
assessment LE scores
Spearman rho
2 weeks, r=.91
8 weeks, r=.94
P< .01
Fugl-Meyer assessment and DeSouza test
total scores covaried closely, explaining
more than 90% of the variance
Motor assessments also closely associated,
explaining more than 80% of the variance
Pearson Product-Moment Correlation
Coefficient
r= .75, upper extremity
r=.74, motor control
r=.76, balance
r=.67, total scores
P<.01
Spearman rho
r=.55, sensory
r= .77, balance
r=.69, lower extremity
Pearson Product-Moment Correlation
Coefficient
r=.754 at admission
r=.854 at 5 weeks
P<.01
Spearman rho association between Bobath
approach and Fugl-Meyer assessment at
three times of testing
P< ,001
Analysis of variance
Fugl-Meyer assessment cumulated with
Bobath approach measurements
X2=20.6 (P<.OOO1)
Correlations highest in results from
upper-extremity scores
lntrarater Pearson Product-Moment Correlation
Coefficients
r= .8&.99
lnterrater upper extremity, r=.97-.99
Lower extremity, r=.79-.95
P<.001
Physical Therapy /Volume 73, Number 71July 1993
7/27/2019 articol Studia
http://slidepdf.com/reader/full/articol-studia 6/10
-able 2. Descrzption ofPatients (N=12)
No. ol Patients % SD Range
Cause of cerebrovascular accident
Infarction
Unknown
Time from onset to admission
Gender
Male
Female
Age (Y)
Side of plegia
Right
Left
Source of referral
Acute care center
Home
Raters
Three physical therapists who had
between 10 an d 20 years of experi-
enc e in stroke rehabilitation adminis-
tered the assessment. They reviewed
the orig inal article by Fugl-Meyer et
alz and de signed a form to rec ord the
results (Appendix). Prior to com -
mencing the study, the physical thera-
pists discussed the assessment and
tested three patients. Each therapist
performed and rated o ne assessmentwhile the other therapists rated the
patient's responses. They comp ared
their results after each assessment.
Approximately 2% hours was spent in
this preparation.
Design
The order in which the therapists saw
the patients was randomized andbalanced (equal numbers of subjects
we re assigned to the therapists). Allpatients we re tested within on e work-ing day of the previous assessment(ie, theoretically, there should have
been n o change in the patients) andwere see n on only on e occasion by
each therapist; that is, each patient
was assessed by all three physicaltherapists o n separate occasions. As-
sessments took ap proximately 30
minutes to administer. After the study
began , the therapists did n ot discuss
the results of the assessments.
Data Anaiysis
Desc riptive statistics, including the
mean and standard deviation for the
total Fugl-Meyer score and for the
subscores, were calculated for each
rater and for each testing occasion. A
three-w ay analysis of varianc e
(ANOVA) was performed to test for
differences between raters (threelevels) an d occasions ( three levels).
The third factor in th e analysis was
subjects (ie, subjectsX raters x occa-
sions). Differences were formally
tested by calculating the F statistic an d
the associated probability value. Th e
level of statistical significanc e was s et
at .05. Reliability was assessed by
calculatin g an ICC (type 2, I), a
random-effects mod el described by
Shr out an d Fleiss.17Reliability is de -
fined as the ability of an instru men t to
measure attributes in a reproducibleand consistent manner.18
A measurement is considere d to be
consistent if it produces similar re-
sults over a nu mb er of occasions in a
stable situation.'9 The ICC u sed to
calculate the reliability coefficients
represents the ratio of variance du e to
subjects com pared w ith the total vari-
ance; thus, its most direct interpret
tion relates to its ability to discrim
nate am ong patients. It is directly
reliant on the heterogeneity of th e
patients. Ninety-five percent confi-
dence limits were calculated to demine the precision of the estimate
reliability.20 Calculating the reliabil
of a n assessment also involves calc
lating the variability in an individu
score du e to factors irrelevant to tpurpose of the test. This variability
known as the error of measure-met~t.20~21he standard error of m
surement (SEM) was calculated fro
an error term that combined rater
occasion, and er ro r variances.18
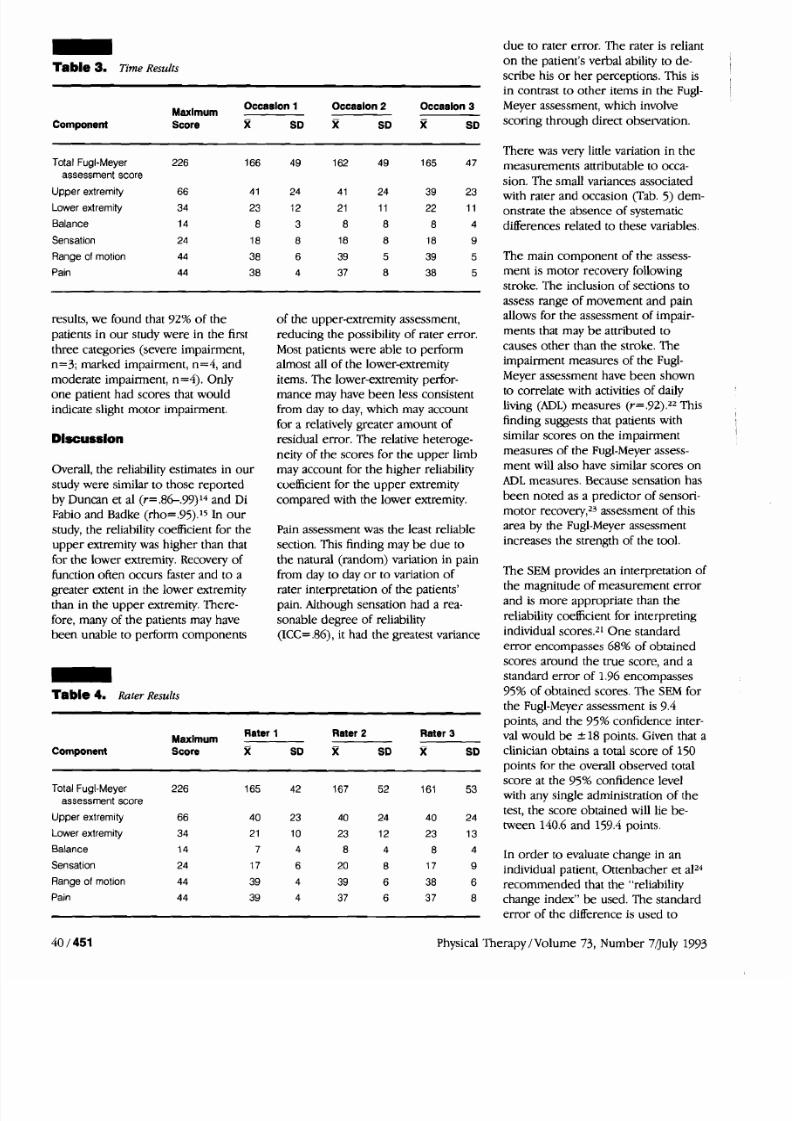
The summary statistics (means andstandard deviations) for both time
and rater are shown in Tables 3 an
4. The ANOVA did not reveal anystatistically significant systematic di
ferences attributable to raters o r o
sions. The overall me an scores of raters varied from 161 to 167 poin
All raters had a mean score of 40
points for the upper extremity. Th
sensation subsection had the great
difference between means, a 3-poi
difference. The m ean total scores
according to occasion varied from
to 165 points, with the largest diff
ence between the means in any se
tion being 2 points.
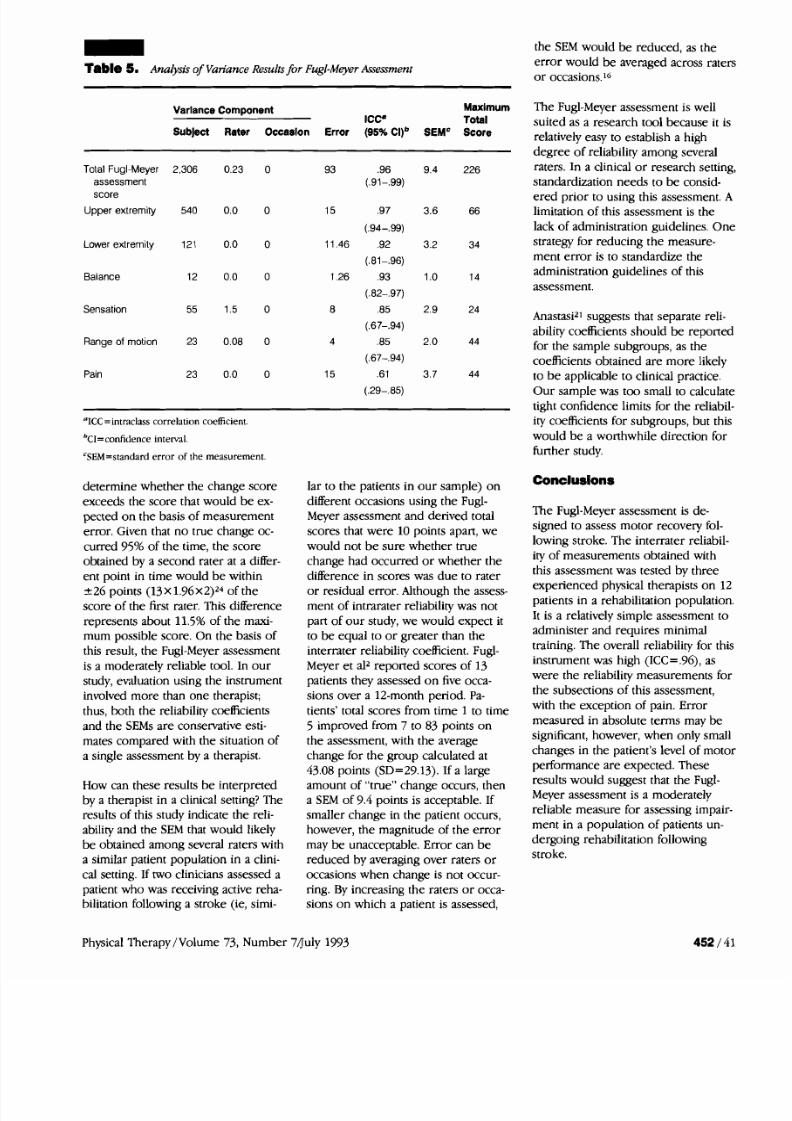
The ICCs, confidence limits, varian
components, and SEMs are shown
Table 5. The inte rrater reliability f
the total score was .96.
The reliability coefficients for the
subsections of the Fugl-Meyer asse
ment varied from .61 for the pain
measurements to .97 for the uppe
extremity items (Tab. 5). The SEM
was 9 points for the total score an
varied from 1 for balance to 4 forpain. Table 5 provides the maxim
total score fo r each section as a re
enc e point fo r each of the SEMs.
Th e total scores for the patients va
from 79 to 220 points. Using the
guidelines developed by Fugl-Mey
fo r characterizing the various leve
motor performance6 to analyze ou
physical Thera py /Volu me 73, Num ber 7/July 1993
7/27/2019 articol Studia
http://slidepdf.com/reader/full/articol-studia 7/10
able 3. Time Results
d u e to rater erro r. The rater is reliant
o n the patient's verbal ability to de-scribe his o r her ~erceo t ions . his isin contrast to other items in the Fugl-
ComponentMaxlmum
Occaslon 1 Occaslon 2 Occaalon 3 Meyer assessment, which involve
Score X SD X SD R SD scoring through direct observation.
Total Fugl-Meyer 226 166 49 162 49 165 47
assessment score
Upper extremity 66 4 1 24 4 1 24 39 23
Lower extremity 34 23 12 21 11 22 11
Balance 14 8 3 8 8 8 4
Sensation 24 18 8 18 8 18 9
Range of motion 44 38 6 39 5 39 5
Pain 44 38 4 37 8 38 5
results, we found that 92% of the
patients in o ur study were in the firstthree categories (severe impairment,
n= 3; marked impairment, n= 4, and
moderate impairment, n=4). Only
one patient had scores that wouldindicate slight m otor impairment.
Dlscusslon
Overall, the reliability estimates in our
study were similar to those repo rted
by Duncan et a1 (r=.8&.99)l4 and DiFabio and Badke (rho=.95).'5 In ou r
study, the reliability coefficient for the
upp er extremity was higher than that
for the lower extremity. Recovery of
function often occurs faster and to agreater extent in the lo wer extremitythan in the up per extremity. There-
fore, many of the patients may have
been unable to perform com ponents-able 4. Rater Results
of the upper-extremity assessment,reducing the possibility of rater erro r.
Most patients were able to performalmost all of the lower-extremity
items. The lower-extremity perfor-
mance may have been less consistentfrom day to day, which m ay account
for a relatively greater amoun t ofresidual erro r. The relative heteroge-
neity of the scores for the upp er limbmay account for the hig her reliability
coefficient for the up pe r extremity
compared with the lower extremity.
Pain assessment was the least reliable
section. This finding may b e d ue tothe natural (rando m) variation in pain
from day to day o r to variation of
rater interpretation of the patients'pain. Although sensation had a rea-
sonable d egre e of reliability
(KC= .86), it had the greatest variance
There was very little variation in the
measurements attributable to occa-
sion . The small v ariances associated
with rater and o ccasion (Tab. 5) dem-onstrate the absence of systematic
differences related to these variables.
The main component of the assess-ment is motor recovery following
stroke. The inclusion of sections to
assess range of movement and painallows for the assessment of impair-
ments that may b e attributed to
causes oth er than the stroke. Theimpairment measures of the Fugl-
Meyer assessment have been shown
to corr elate with activities of dailyliving (ADL) measures (r= 92).22 This
finding suggests that patients withsimilar scores on the impairment
measures of the Fugl-Meyer assess-
men t will also have similar scores onADL measures. Because sensation has
been noted as a predictor of sensori-
mo tor recovery,23 assessmen t of thisarea by the Fugl-Meyer assessment
increases the strength of the tool.
The SEM provides an interpretation of
the magnitude of measurement erro rand is more appropriate than the
reliability coefficient for interpretingindividual scores.21 On e standard
erro r encompasses 68% of obtained
scores around the true score, and astandard error of 1.96 encompasses
95% of obtained scores. The SEM fo rthe Fugl-Meyer assessmen t is 9.4points, and the 95% confidence inter-
MaximumRater 1 Rater 2 Rater 3 ;a1 wo uld b e +- I8 points. Given that a
Component Score X SD X SD X SD clinician obtains a total score of 150points for the overall observed total
score at the 95% confidence levelTotal Fugl-Meyer 226 165 42 167 52 161
assessment score
53with any single administration of the
Upper extremity 66 40 23 40 24 40 24test, the sco re obtaine d will lie be-
tween 140.6 and 159.4 points.Lower extremity 34 21 10 23 12 23 13
Balance 14 7 4 8 4 8 In order to evaluate change in anSensation 24 17 6 20 8 17 individ ual patient, Otte nba cher et a124Range of motion 44 39 4 39 6 38 6 recommended that the "reliabilityPain 44 39 4 37 6 37 8 change index" be used. The standard
erro r of the difference is used to
40 / 451 Physical Therapy /Vo lum e 73, Num ber 7/July 1993
7/27/2019 articol Studia
http://slidepdf.com/reader/full/articol-studia 8/10
able 5. Analysis of Variance Resultsfor Fugl-MeyerAsessment
the SEM would be reduced, as the
error would be averaged across rat
or occasions.16
Varlance Component MaxlmumICC* Total
Subject Rater Occaslon Error (95%Cl)b SEMC Score
Total Fugl-Meyer 2,306 0.23 0
assessment
score
Upper extremity 540 0.0 0
Lower extremity 121 0.0 0
Balance 12 0.0 0
Sensation 55 1.5 0
Range of motion 23 0.08 0
Pain 23 0.0 0
OICC= ntraclass correlation coefficient.
b~~=confitiencenterval
'SEM=standard error of the measurement.
determine whether the change score
exceeds the score that would b e ex-
pected on the basis of measurement
error. Given that no true change oc-
curred 95% of the time, the score
obtained by a second rater at a differ-
ent point in time would be within-+26 points (13X 1 . 9 6 ~ 2 ) ~ ~f the
score of the first rater. This difference
represents about 11.5% of the maxi-
mum possible score. On the basis of
this result, the Fugl-Meyer assessment
is a moderately reliable tool. In our
study, evaluation using the instrument
involved more than one therapist;
thus, both the reliability coefficients
and the SEMs are conservative esti-
mates compared with the situation of
a single assessment by a therapist.
How can these results be interpreted
by a therapist in a clinical setting? The
results of this study indicate the reli-
ability and the SEM that would likely
be obtained among several raters with
a similar patient population in a clini-
cal setting. If two clinicians assessed a
patient who was receiving active reha-
bilitation following a stroke (ie, simi-
lar to the patients in our sample) on
different occasions using the Fugl-
Meyer assessment and derived total
scores that were 10 points apart, we
would not b e sure whether true
change had occurred or whether the
difference in scores was due to rateror residual error. Although the assess-
ment of intrarater reliability was not
part of our study, we would expect it
to be equal to or greater than the
interrater reliability coefficient. Fugl-
Meyer et a12 reported scores of 13
patients they assessed on five occa-
sions over a 12-month period. Pa-
tients' total scores from time 1 to time
5 improved from 7 to 83 points on
the assessment, with the average
change for the group calculated at
43.08 points (SD=29.13). If a largeamount of "true" change occurs, then
a SEM of 9.4 points is acceptable. If
smaller change in the patient occurs,
however, the magnitude of the erro r
may be unacceptable. Error can b e
reduced by averaging over raters or
occasions when change is not occur-
ring. By increasing the raters or occa-
sions on which a patient is assessed,
The Fugl-Meyer assessment is well
suited as a research tool because it
relatively easy to establish a high
degree of reliability among several
raters. In a clinical or research setti
standardization needs to be consid-
ered prior to using this assessment
limitation of this assessment is the
lack of administration guidelines. O
strategy for reducing the measure-
ment error is to standardize the
administration guidelines of this
assessment.
Anastasi2' suggests that separate reli
ability coefficients should be report
for the sample subgroups, as the
coefficients obtained are more likel
to b e applicable to clinical practice.
Our sample was too small to calcul
tight confidence limits for the reliab
ity coefficients for subgroups, but th
would be a worthwhile direction fo
further study.
The Fugl-Meyer assessment is de-
signed to assess motor recovery fol
lowing stroke. The interrater reliabi
ity of measurements obtained with
this assessment was tested by three
experienced physical therapists on
patients in a rehabilitation populatio
It is a relatively simple assessment t
administer and requires minimal
training. The overall reliability for th
instrument was high (ICC= 96), as
were the reliability measurements f
the subsections of this assessment,
with the exception of pain. Error
measured in absolute terms may be
significant, however, when only sma
changes in the patient's level of mo
performance are expected. These
results would suggest that the Fugl-
Meyer assessment is a moderately
reliable measure for assessing impa
ment in a population of patients un-
dergoing rehabilitation following
stroke.
Physical Therapy /Volume 73, Number 7duly 1993

7/27/2019 articol Studia
http://slidepdf.com/reader/full/articol-studia 9/10
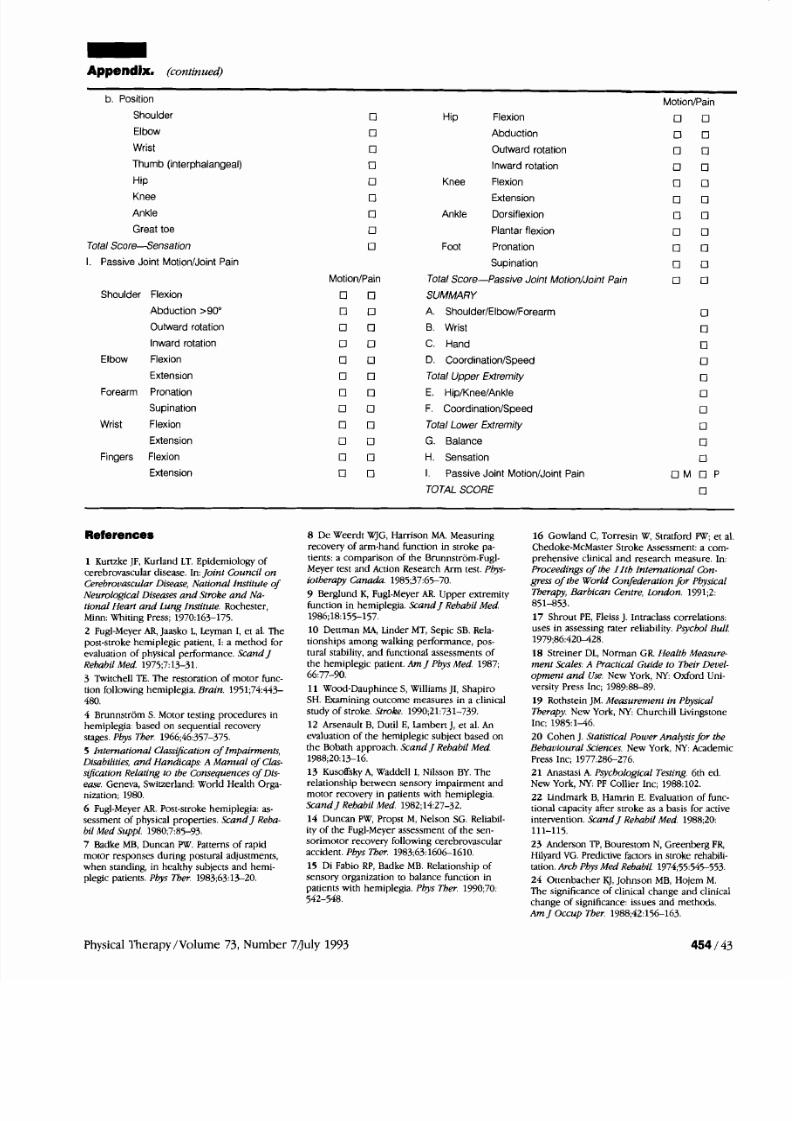
-ppendb. Fugl-MeyerAssessment Score Sheet
Patient's Name Patient No.
Therapist's Name
UPPER EXTREMITY
A. Shoulder/Elbow/Forearm
I. Reflex activity
Flexors -Biceps
-Finger flexorsExtensors--Triceps
II. a. Flexor synergy
Shoulder-Retraction-Elevation-Abduction-Outward rotation
Elbow -Flexion
Forearm -Supination
b. Extensor synergy
Shoulder-Adductionlinward rotation
Elbow -Extension
Forearm -Pronation
Ill. Hand to lumbar spine
Hand -Move to lumbar spine
Shoulder -Flexion 0"-90"
Elbow 90"-Pronationlsupination
IV. Shoulder -Abduction 0"-90"-Flexion 90"-180"
Elbow 0" -Pronation/supination
V. Normal reflex activity
Total-Shoulder/Elbow/Forearm
B. Wrist
Elbow 90"-Wrist stability
Elbow 90"-Wrist flexionlextension
Elbow 0" -Wrist stabilityElbow 0" -Wrist flexionlextension
Circumduction
TotaC Wrist
C. Hand
Fingers mass llexion
Date
LOWER EXTREMITY
E. HipIKneelAnkle
I. Reflex activity
Flexors -Hamstrings
-Achilles
Extensors-Patellar
11. a. Flexor synergy
Hip -Flexion
Knee-Flexion
Ankle-Dorsiflexion
b. Extensor synergy
Hip -Extension
-Adduction
Knee-Extension
Ankle--Plantar flexion
Ill. Knee-Flexion
Ankle-DorsiflexionIV. Knee-Flexion
Ankle-Dorsiflexion
V. Normal reflex activity
Flexors -Hamstrings
-Achilles
Extensors--Patellar
Total-Hip/Knee/Ankle 0
F. CoordinationISpeed
Tremor
Dysmetria 0
Speed
TotaCCoordination/SpeedTotal Motor Score for the Lower Extremity
G. Balance
Sit without support 0
Parachute reaction, nonaffected side 0
Parachute reaction, affected side
Fingers mass extension Supported standing 0
Grasp a
Grasp b
Grasp c
Grasp d
Grasp e
Total--HandD. CoordinationISpeed
Tremor
Dysmetria
Speed
Total-Coordination/Speed
Total Motor Score for the Upper Extremity
Standing without support
Stand on nonaffected leg
Stand on affected leg
Total Score-Balance
H. Sensation
a. Light touchArm
Palm
Leg
Plantar
(continued)
Physical Therapy /Vo lum e 73, Numb er 7fluly 1993
7/27/2019 articol Studia
http://slidepdf.com/reader/full/articol-studia 10/10
ppendix. (continued)
b. Position
Shoulder
Elbow
Wrist
Thumb (interphalangeal)
Hip
Knee
Ankle
Great toe
Total Score--Sensation
I. Passive Joint MotionIJoint Pain
Shoulder Flexion
Abduction >90°
Outward rotation
Inward rotation
Elbow Flexion
Extension
Forearm Pronation
Supination
Wrist Flexion
Extension
Fingers Flexion
Extension
Hip Flexion
Abduction
Outward rotation
Inward rotation
Knee Flexion
Extension
Ankle Dorsiflexion
Plantar flexion
Foot Pronation
Supination
Total Score-Passive Joint Motion/Joint Pain
SUMMARY
A. Shoulder/Elbow/Forearm
B. Wrist
C. Hand
D. CoordinationISpeed
Total Upper Extremity
E. HipIKneelAnkle
F. CoordinationlSpeed
Total Lower Extremity
G. Balance
H. Sensation
I. Pass ive Joint MotionIJ oint Pain
TOTAL SCORE
References
1 Kunzke JF, Kurland LT. Epidemiology of
cerebrovascular disease. In:Joint Council on
Cerebrouascular Disease, National Institute ofNeurological Diseases and Stroke and Nu-
tional tieari and Lung Imitute. Rochester,
Minn: Whiting Press; 1970:163-175.
2 Fugl-Meyer AR, Jaasko L Leyman I, et al. The
post-stroke hemiplegic patient, I: a method for
evaluation of physical performance. Scand J
Rehabil Med. 1975;7:13-31.
3 Twitchell TE. he restoration of motor func-
tion following hemiplegia. Brain. 1951;74:443-
480.
4 Brunnstrom S. Motor testing procedures in
hemiplegia: based on sequential recovery
stages.Pbys Ther. 1966;46:357-375.
5 International C l ~ ~ c a t i o nf Impainnats,
Disabilities, and Handicaps: A Manual of C h -
stfication Relating to the Consequences of Dis-
ease. Geneva, Switzerland: World Health Orga-
nization; 1980.
6 Fugl-MeyerAR. Post-stroke hemiplegia: as-
sessment of physical properties. Scand J Reba-
bil Med Suppl. 1980;7:85-93.
7 Badke MB, Duncan PW. atterns of rapid
motor responses during postural adjustments,
when standing, in healthy subjects and hemi-
plegic patients. Pbys Thm 1983;63:1520.
8 De Weerdt WJG, Harrison MA. Measuring
recovery of arm-hand function in stroke pa-
tients: a comparison of the Brunnstrom-Fugl-
Meyer test and Action Research Arm test. Pbs-
iotherapy Canada. 1985;37:65-70.9 Berglund K, Fugl-Meyer AR. Upper extremity
function in hemiplegia. Scand J Rehabil Med.
1986;18:155-157.
10 Dettman MA, Linder MT, Sepic SB. Rela-
tionships among walking performance, pos-
tural stability, and functional assessments of
the hemiplegic patient. Am J Phys Med. 1987;
66:77-90.
11 Wood-Dauphinee S, Williams JI, Shapiro
SH. Examining outcome measures in a clinical
study of stroke. Stroke. 1990;21:731-739.
12 Arsenault B, Dutil E, Iamben J, et al. An
evaluation of the hemiplegic subject based on
the Bobath approach. Scand J Rebabil Med.
1988;20:13-16.
13 Kusoffsky A, Waddell I, Nilsson BY. The
relationship between sensory impairment and
motor recovery in patients with hemiplegia.
ScandJ Rehabil Med. 1982;14:27-32.
14 Duncan PW, Propst M, Nelson SG. Reliabil-
ity of the Fugl-Meyer assessment of the sen-
sorimotor recovery following cerebrovascular
accident. Pbys Tber. 1983;63:16061610.
15 Di Fabio RP,Badke MB. Relationship of
sensory organization to balance function in
patients with hemiplegia. Phys Ther. 1990;70:
542-548.
16 Gowland C, Torresin W, Stratford PW; et
Chedoke-McMaster Stroke &sessment: a com
prehensive clinical and research measure. In
Proceedings of the 22th Intmtional Con-
gress of the World Confederation or PhysicaTherapy, Barbican Centre, London. 1991;2:
851-853.
17 Shrout PE, Fleiss J. Intraclass correlations
uses in assessing rater reliability. Psycho1 Bu
1979;86:420428.
18 Streiner DL, Norman GR. IIealth Measur
ment Scales: A Practical Guide to Their Deue
opma t and Use. New York, NY: Oxford Uni
versity Press Inc; 198988439,
19 Rothstein JM.Measurement in Pbysical
Therapy. New York, NY: Churchill Livingston
Inc; 1985:146 .
20 Cohen J. Statistical Power Ana&is for th
Behauioural Sciences. New York, NY: Academ
Press Inc; 1977:286276.
21 Anastasi A. Psychological Testing.6th ed.
New York, NY: PF Collier Inc; 1988:102.
22 Lindmark B, Hamrin E. Evaluation of fun
tional capacity after stroke as a basis for acti
intervention. Scand J Rehabil Med. 1988;20:
111-115.
23 Anderson TP,Bourestom N, Greenberg FR
Hilyard VG. Predictive factors in stroke rehabi
tation.Arch Pbys Med Rebabil. 1974;55:54555
24 Ottenbacher KJ, Johnson MB, Hojem M.
The significance of clinical change and clinic
change of significance: issues and methods.
Am J Occup Tber. 1988;42:156163.
Physical I'herapy /Volume 73, Number 7/July 1993


















