Antineutro phil Cy to p las mic An ti bod ies (ANCA): Di ...
20
Antineutrophil Cytoplasmic Antibodies (ANCA): Diagnostic Utility and Potential Role in the Pathogenesis of Vasculitis Branko Malenica, Marija Rudolf, Ana Kozmar Division of Immunology, Clinical Institute of Laboratory Diagnosis, Zagreb University Hospital Center, Zagreb, Croatia Corresponding author: Branko Malenica, MD, PhD Division of Immunology Clinical Institute of Laboratory Diagnosis Zagreb University Hospital Center Kišpatiæeva 12 10000 Zagreb, Croatia [email protected] Received: 22.07.2004. Accepted: 18.09.2004. INTRODUCTION Antineutrophil cytoplasmic antibodies (ANCA) are a heterogeneous group of circulating antibodies directed toward the cytoplasmic constituents of neutrophil granules and monocytes. ANCA were first described in 1982 by Davies et al. in a few pa- tients with segmental necrotizing glomerulone- phritis (1,2). The importance of this observation had not been recognized until 1985, when a distinct granular cytoplasmic fluorescence pattern, first called ACPA (anticytoplasmic antibodies) and later termed C-ANCA (cytoplasmic), was shown to be associated with Wegener¢s granulomatosis (WG) (3). Later, a second ANCA fluorescence pattern (later called perinuclear, P-ANCA) was described in patients with microscopic polyangiitis (MPA) (4) and in patients with the idiopathic form of pauci-immune necrotizing crescentic glomerulonephritis (iNCGN) (5). These data have now been confirmed by many groups and support the view that ANCA-associated vasculitis and glomerulonephritis are indeed a dis- tinct disease category (6-11). Subsequently, a third, less clearcut ANCA subtype (later termed ‘atypical’ or very perinuclear, a/P-ANCA) was described in a wide range of connective tissue diseases (CTD), inflammatory bowel (IBD) and autoimmune liver diseases, and infectious diseases (8-13). Today the various ANCA serve as useful seromarkers. They can be used as clinical tools to aid in the diagnosis of WG and to distinguish new entities within the large spectra of vasculitis/glome- 294 Acta Dermatovenerol Croat 2004;12(4):294-313 REVIEW SUMMARY Antineutrophil cytoplasmic antibodies (ANCA) are a heteroge- neous group of circulating antibodies directed toward the cytoplasmic constitu- ents of neutrophils and monocytes. ANCA have been described in various dis- eases including idiopathic systemic vasculitides, connective tissue diseases, inflammatory bowel diseases, autoimmune liver diseases, infectious diseases, and some drugs. ANCA recognize different target antigens such as proteinase 3 (PR3-ANCA), myeloperoxidase (MPO-ANCA), cathepsin G, lactoferrin, bac- tericidal/permeability-increasing protein (BPI), and some others. However, only PR3-ANCA and MPO-ANCA are closely associated with systemic vasculi- tides, in particular Wegener¢s granulomatosis, microscopic polyangiitis and its renal limited manifestation, and Churg-Strauss syndrome. Both in vitro and in vivo experimental data strongly support a pathogenic role for ANCA in vasc- ulitis and glomerulonephritis. KEY WORDS ANCA; PR3-ANCA; MPO-ANCA; vasculitis; pathogenesis
Transcript of Antineutro phil Cy to p las mic An ti bod ies (ANCA): Di ...
Antineutrophil Cy to plas mic An ti bod ies (ANCA): Di ag nos tic
Util ity and Po ten tial Role in the Pathogenesis of Vasculitis
Branko Malenica, Marija Rudolf, Ana Kozmar
Di vi sion of Im mu nol ogy, Clin i cal In sti tute of Lab o ra tory Di ag no sis, Zagreb Uni ver sity Hos pi tal Cen ter, Zagreb, Croatia
Cor re spond ing au thor:
Branko Malenica, MD, PhD
Di vi sion of Im mu nol ogy
Clin i cal In sti tute of Lab o ra tory Di ag no sis
Zagreb Uni ver sity Hos pi tal Cen ter
Kišpatiæeva 12
10000 Zagreb, Croatia
b_malenica@ya hoo.com
Re ceived: 22.07.2004.
Ac cepted: 18.09.2004.
IN TRO DUC TION
Antineutrophil cy to plas mic an ti bod ies (ANCA)
are a het er o ge neous group of cir cu lat ing an ti bod ies
di rected to ward the cy to plas mic con stit u ents of
neutrophil gran ules and monocytes. ANCA were
first de scribed in 1982 by Davies et al. in a few pa -
tients with seg men tal necrotizing glomerulone -
phritis (1,2). The im por tance of this ob ser va tion had
not been rec og nized un til 1985, when a dis tinct
gran u lar cy to plas mic flu o res cence pat tern, first
called ACPA (anticytoplasmic an ti bod ies) and later
termed C-ANCA (cy to plas mic), was shown to be
as so ci ated with Wegener¢s granulomatosis (WG)
(3). Later, a sec ond ANCA flu o res cence pat tern
(later called perinuclear, P-ANCA) was de scribed in
pa tients with mi cro scopic polyangiitis (MPA) (4) and
in pa tients with the id io pathic form of pauci-im mune
necrotizing cres cen tic glomerulonephritis (iNCGN)
(5). These data have now been con firmed by many
groups and sup port the view that ANCA-as so ci ated
vasculitis and glomerulonephritis are in deed a dis -
tinct dis ease cat e gory (6-11). Sub se quently, a third,
less clearcut ANCA sub type (later termed ‘atyp i cal’
or very perinuclear, a/P-ANCA) was de scribed in a
wide range of con nec tive tis sue dis eases (CTD),
inflammatory bowel (IBD) and autoimmune liver
diseases, and infectious diseases (8-13).
To day the var i ous ANCA serve as use ful
seromarkers. They can be used as clin i cal tools to
aid in the di ag no sis of WG and to dis tin guish new
en ti ties within the large spec tra of vasculitis/glome -
294
Acta Dermatovenerol Croat 2004;12(4):294-313 RE VIEW
SUM MARY Antineutrophil cy to plas mic an ti bod ies (ANCA) are a het er o ge -neous group of cir cu lat ing an ti bod ies di rected to ward the cy to plas mic con stit u -ents of neu tro phils and monocytes. ANCA have been de scribed in var i ous dis -eases in clud ing id io pathic sys temic vasculitides, con nec tive tis sue dis eases,in flam ma tory bowel dis eases, au to im mune liver dis eases, in fec tious dis eases, and some drugs. ANCA rec og nize dif fer ent tar get an ti gens such as proteinase3 (PR3-ANCA), myeloperoxidase (MPO-ANCA), cathepsin G, lactoferrin, bac -te ri cidal/per me abil ity-in creas ing pro tein (BPI), and some oth ers. How ever,only PR3-ANCA and MPO-ANCA are closely as so ci ated with sys temic vascu li -tides, in par tic u lar Wegener¢s granulomatosis, mi cro scopic polyangiitis and itsre nal lim ited man i fes ta tion, and Churg-Strauss syn drome. Both in vi tro and invivo ex per i men tal data strongly sup port a patho genic role for ANCA in vasc -ulitis and glomerulonephritis.
KEY WORDS ANCA; PR3-ANCA; MPO-ANCA; vasculitis; pathogenesis
ru lo nephritis and chronic in flam ma tory bowel and
liver dis eases. Re cent stud ies sup port the hy poth e -
sis that ANCA and their tar get an ti gens may be im -
pli cated in the pathogenesis of these dis eases, at
least in vasculitis (7-11,14-20).
In this re view we will eval u ate back ground in for -
ma tion about the evo lu tion of ANCA meth od ol ogy,
the di ag nos tic ap pli ca tion of ANCA test ing, and the
cur rent un der stand ing of the patho genic role of dif -
fer ent sub types of ANCA. We also dis cuss ANCA in
the con text of cutaneous vasculitis.
ANCA TEST METH OD OL OGY AND
THEIR TAR GET AN TI GENS
Cur rently, three ba sic as say prin ci ples are ap -
plied for the de tec tion of ANCA. The orig i nal me -
thod of ANCA de tec tion is in di rect immunofluores -
cence (IIF) (21). While it re mains the most widely
used method, it does not iden tify the spe cific an ti -
gen re spon si ble for the ANCA immunofluorescen -
ce. En zyme-linked immunosorbent as say (ELISA)
is used for tar get-spe cific ANCA de ter mi na tion (22).
There are two pop u lar types of such solid-phase as -
says. The tar get an ti gen can be coated di rectly onto
the plas tic re ac tion well (stan dard ELISA), or it can
be linked to the re ac tion well via tar get an ti gen-spe -
cific mouse monoclonal or rab bit polyclonal an ti -
bod ies (cap ture ELISA or sand wich ELISA) (23).
Other de tec tion meth ods such as radioimmunoas -
say (RIA), immunoblotting (IB) or immunoprecipita -
ti on tech niques are not widely used for routine
ANCA testing (24).
ANCA are rou tinely de tected by IIF on eth a -
nol-fixed neu tro phils (21,25,26). Re cent con sen sus
state ments on test ing and re port ing of ANCA rec og -
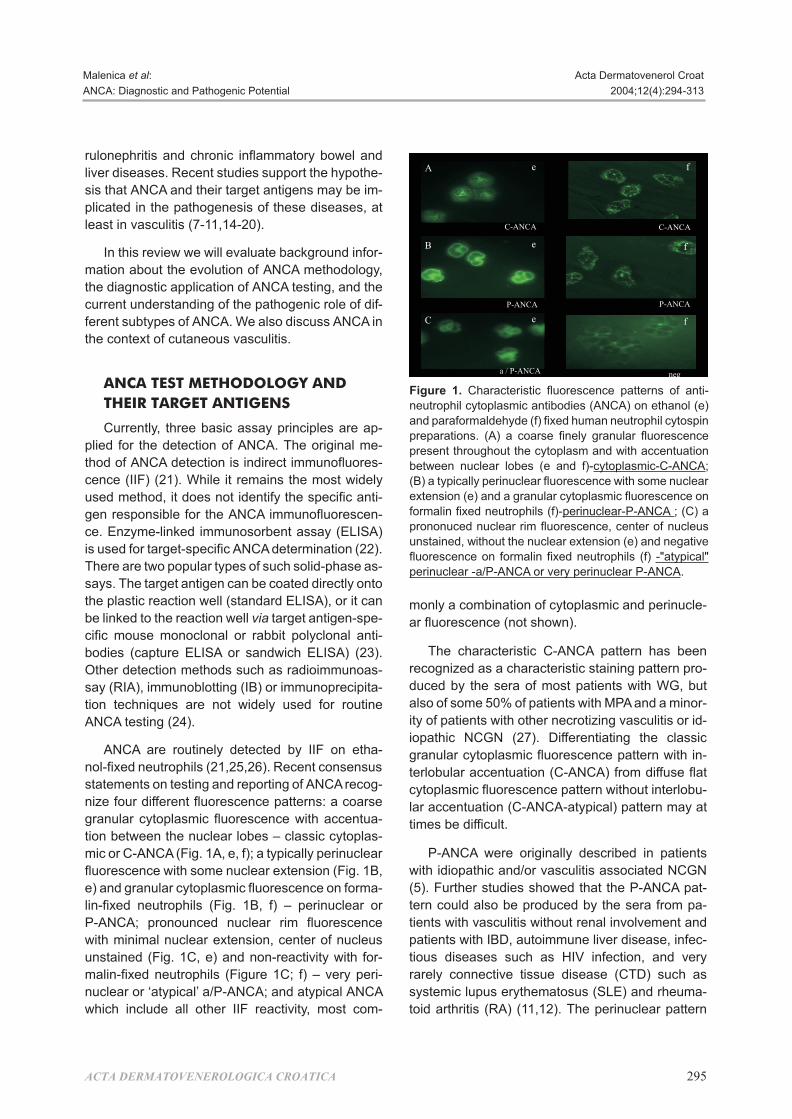
nize four dif fer ent flu o res cence pat terns: a coarse
gran u lar cy to plas mic flu o res cence with ac cen tu a -
tion be tween the nu clear lobes – clas sic cy to plas -
mic or C-ANCA (Fig. 1A, e, f); a typ i cally perinuc lear
flu o res cence with some nu clear ex ten sion (Fig. 1B,
e) and gran u lar cy to plas mic flu o res cence on for ma -
lin-fixed neu tro phils (Fig. 1B, f) – perinuclear or
P-ANCA; pro nounced nu clear rim flu o res cence
with min i mal nu clear ex ten sion, cen ter of nu cleus
un stained (Fig. 1C, e) and non-re ac tiv ity with for -
ma lin-fixed neu tro phils (Fig ure 1C; f) – very peri -
nuclear or ‘atyp i cal’ a/P-ANCA; and atyp i cal ANCA
which in clude all other IIF re ac tiv ity, most com -
monly a com bi na tion of cy to plas mic and perinucle -
ar fluorescence (not shown).
The char ac ter is tic C-ANCA pat tern has been
rec og nized as a char ac ter is tic stain ing pat tern pro -
duced by the sera of most pa tients with WG, but
also of some 50% of pa tients with MPA and a mi nor -
ity of pa tients with other necrotizing vasculitis or id -
io pathic NCGN (27). Dif fer en ti at ing the clas sic
gran u lar cy to plas mic flu o res cence pat tern with in -
ter lob u lar ac cen tu a tion (C-ANCA) from dif fuse flat
cy to plas mic flu o res cence pat tern with out in ter lob u -
lar ac cen tu a tion (C-ANCA-atypical) pattern may at
times be difficult.
P-ANCA were orig i nally de scribed in pa tients
with id io pathic and/or vasculitis as so ci ated NCGN
(5). Fur ther stud ies showed that the P-ANCA pat -
tern could also be pro duced by the sera from pa -
tients with vasculitis with out re nal in volve ment and
pa tients with IBD, au to im mune liver dis ease, in fec -
tious dis eases such as HIV in fec tion, and very
rarely con nec tive tis sue dis ease (CTD) such as
sys temic lupus erythematosus (SLE) and rheu ma -
toid ar thri tis (RA) (11,12). The perinuclear pat tern
ACTA DERMATOVENEROLOGICA CROATICA 295
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313
A
B
C
f
C-ANCA C-ANCA
P-ANCA P-ANCA
e
e
f
f
a / P-ANCA neg
ee
Fig ure 1. Char ac ter is tic flu o res cence pat terns of anti -
neutrophil cy to plas mic an ti bod ies (ANCA) on eth a nol (e)
and paraformaldehyde (f) fixed hu man neutrophil cytospin
prep a ra tions. (A) a coarse finely gran u lar flu o res cence
pres ent through out the cy to plasm and with ac cen tu a tion
be tween nu clear lobes (e and f)-cy to plas mic-C-ANCA;
(B) a typ i cally perinuclear flu o res cence with some nu clear
ex ten sion (e) and a gran u lar cy to plas mic flu o res cence on
for ma lin fixed neu tro phils (f)-perinuclear-P-ANCA ; (C) a
prononuced nu clear rim flu o res cence, cen ter of nu cleus
un stained, with out the nu clear ex ten sion (e) and neg a tive
flu o res cence on for ma lin fixed neu tro phils (f) -"atyp i cal"
perinuclear -a/P-ANCA or very perinuclear P-ANCA.

can not al ways be dis tin guished from the nu clear
stain ing pat tern. Thus, dis crim i na tion be tween anti -
nuclear an ti bod ies (ANA) and P-ANCA is not pos si -
ble in most sera that are ANA pos i tive when iso lated
eth a nol-fixed neu tro phils are used as a sub strate.
In fact, an ti bod ies re act ing with nu clei of granu lo -
cytes only, and not with those of other sub strates,
have been de tected in pa tients with RA long be fore
ANCA had been de scribed, and were named gra -
nu lo cyte-spe cific antinuclear an ti bod ies (GS-ANA).
Re cent stud ies, how ever, have shown that the
P-ANCA flu o res cence pat tern rep re sents an ar ti fact
of eth a nol fix a tion which al lows for re ar range ment
of pos i tively charged gran ule con stit u ents around
and on the neg a tively charged nu clear mem brane
(28). The use of crosslinking fix a tives, such as pa -
rafo rmaldehyde, dur ing the prep a ra tion of neutro -
phil sub strates pre vents the perinuclear re ar range -
ment of charged an ti gens and thereby al lows for
dis tinc tion of true P-ANCA from ANA with or with out
granulocyte spec i fic ity. On for ma lin-fixed neu tro -
phils, true P-ANCA will dis play dif fuse gran u lar cy -
to plas mic stain ing, whereas an ANA-con tain ing se -
rum sam ple will again dis play nu clear stain ing. The
si mul ta neous test ing for ANA using standard sub -
strates, such as HEp-2 cells, is not sufficient for this
dis tinc tion because P-ANCA and ANA can occur
simultaneously.
‘Atyp i cal’ P-ANCA with dif fer ent fre quency were
found in pa tients with IBD, au to im mune liver dis -
eases and in fec tious dis eases such as HIV in fec -
tion (11,12). Dis tinc tion be tween these two P-ANCA
sim i lar flu o res cence pat terns is pos si ble on for ma -
lin-fixed neu tro phils where the ‘atyp i cal’ P-ANCA
pat tern dis plays non-re ac tiv ity, whereas true P-
ANCA dis play dif fuse gran u lar cytoplasmic staining
(Fig. 1).
IIF should be per formed on se rum sam ples from
all ‘new’ pa tients, since about 10% of ANCA-pos i -
tive se rum sam ples in pa tients with WG or MPA can
be dem on strated only by IIF.
To cir cum vent the prob lems as so ci ated with IIF,
i.e. the lack of tar get an ti gen spec i fic ity and op er a -
tor de pend ence, tar get an ti gen-spe cific solid-phase
immunoassays have been used. ELISA and IB
tech niques en able iden ti fi ca tion of many tar get an ti -
gens that are as so ci ated with autoantibodies caus -
ing dif fer ent immunofluorescence pat terns (Ta ble
1). The tar get an ti gen rec og nized by most C-ANCA
pos i tive sera has been iden ti fied as proteinase 3
(PR3), a neu tral serine pro te ase pres ent in the
azurophilic gran ules of neu tro phils. Proteinase 3
has been cloned and shown to be a 29 kD glyco -
protein of 228 aminoacids (29-33). Hu man an ti bod -
ies to PR3 ap pear to rec og nize conformational de -
ter mi nants on the mol e cule (34). Very rarely, sera
with PR3-ANCA re ac tiv ity can also cause P-ANCA
flu o res cence pat tern (35). Myeloperoxidase (MPO)
rep re sents the P-ANCA tar get an ti gen with the
great est clin i cal util ity be cause of the fre quent as so -
ci a tion of MPO-ANCA with MPA and iNCGN (36).
All se rum sam ples should be as sayed in PR3-
ANCA and MPO-ANCA ELISAs, since about 5% of
se rum sam ples are pos i tive only by ELISA. How -
ever, many sera that pro duce P-ANCA or a/P-ANCA
stain ing pat tern on eth a nol-fixed neu tro phils do not
con tain autoantibodies to MPO or PR3 as tested by
an ti gen-spe cific as says. It has now been rec og -
nized that a num ber of these sera con tain an ti bod -
ies to other gran u lar con stit u ents of neu tro phils. In
par tic u lar, autoantibodies have been dem on strated
to hu man leu ko cyte elastase (HLE) (37,38), cathe -
psin G (CG) (39-42), lactoferrin (LF) (43-46), lyso -
zyme (47), azurocidin (48), a-enolase (49-51), actin
(52-54), tropomyosin (53, 54), high mo til ity groups
of nonhistone chro mo somal pro teins 1 and 2
(HMG1 and HMG2) (55-57), bac te ri ci dal/ per me a -
296 ACTA DERMATOVENEROLOGICA CROATICA
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313
Ta ble 1. Tar get an ti gens for antineutrophil cy to -plas mic an ti bod ies (ANCA)
ANCA target antigen Immunofluorescence pattern
PR3 C-ANCA, very rarely P-ANCA
MPO P-ANCA, very rarely C-ANCA
Eosinophylic peroxidase a/C-ANCA
HLE P-ANCA
a-Enolase P-ANCA
Azurocidin P-ANCA
Cathepsin G P-ANCA
Lactoferrin P-ANCA
Lysozyme P-ANCA, a/C-ANCA
Actin a/C-ANCA, a/P-ANCA
Tropomyosin a/C-ANCA, a/P-ANCA
HMG1/2 P-ANCA
BPI a/C-ANCA, a/P-ANCA
Lamin B1 a/P-ANCA
Histone H1 a/P-ANCA

bi l ity- in creas ing protein (BPI) (58-61), lamin B1 (13,
47) and histone H1 (13,62).
DI AG NOS TIC UTIL ITY OF ANCA
TEST ING
Since the first de scrip tion of ANCA, the dif fer ent
ANCA flu o res cence pat terns have been de scribed
in var i ous dis eases. In ad di tion to sys temic vascu -
litides, this list now in cludes var i ous CTDs, IBD, au -
to im mune liver dis eases, in fec tions, ma lig nan cies,
myelodysplastic pro cesses and many oth ers, even
di a be tes mellitus. The in ter pre ta tion of many re -
ports is com pro mised by lim ited in for ma tion about
the meth ods uti lized for ANCA de tec tion. Re ports
that in clude data on dif fer ent flu o res cence pat terns
and spe cific tar get an ti gens al low for more mean -
ing ful analysis of clinical as so ci a ti ons and utility.
ANCA in pri mary sys temic vasculitides
The most clear-cut as so ci a tion of a dis ease with
ANCA di rected against a spe cific tar get an ti gen re -
mains the as so ci a tion be tween WG and PR3-
ANCA (Ta ble 2). Be tween 80% to 95% of all ANCA
found in WG are C-ANCA (8,12,63-65). The use of
more sen si tive PR3-ANCA spe cific meth ods (cap -
ture ELISA) of de tec tion has con firmed that the
C-ANCA in WG is al most al ways as so ci ated with
anti-PR3 (23,66). It has been es ti mated that
5%-20% of ANCA in WG may be P-ANCA, which
are mostly di rected against MPO (67,68) and only
rarely against other known tar get an ti gens such as
hu man leu ko cyte elastase (69). The sen si tiv ity of
C-ANCA/PR3-ANCA for WG is re lated to the ex tent,
se ver ity and ac tiv ity of dis ease (64). In a meta-anal -
y sis of C-ANCA in WG, the pooled sen si tiv ity was
91% for the sub set of pa tients with ac tive dis ease
com pared to 63% for those with in ac tive dis ease
(70). Some lon gi tu di nal stud ies have shown that
titers of C-ANCA/PR3-ANCA cor re late with clin i cal
dis ease ac tiv ity (71-74), al though this has been dis -
puted by other au thors (75,76). Ad di tion ally, dis -
ease re lapse can be an tic i pated and pre vented by
in ten si fy ing immunosuppression in re sponse to ris -
ing titers (76,77). Per sis tent or intermittent C-ANCA
positivity is an independent risk factor for relapse
(78-81).
Most pa tients with MPA are ANCA pos i tive, ei -
ther with spec i fic ity for MPO or for PR3 (5,11,12,64,
67). The in ter pre ta tion of data about the as so ci a tion
of ANCA and MPA is com pli cated by the lack of con -
sen sus about the def i ni tion of MPA. Since there
con tin ues to be con tro versy about which fea tures
clearly sep a rate MPA from PAN, it re mains un clear
whether ANCA also oc cur in some pa tients with
clas sic PAN (82). How ever, most data sup port the
per cep tion that MPA, which is fre quently as so ci ated
with GN and/or pul mo nary capillaritis, is of ten as so -
ci ated with MPO-ANCA, whereas clas sic PAN is not
(64,83,84). The re la tion be tween titers of ANCA and
dis ease ac tiv ity has not been studied systematically
in MPA (70,78,80,85).
Other tar get an ti gens for ANCA, such as BPI
and azurocidin, have re cently been de tected in pa -
tients with sys temic vasculitis (48,58,60,86). These
an ti bod ies may also si mul ta neously oc cur with
PR3- or MPO-ANCA.
Most pa tients with iNCGN are pos i tive for
anti-MPO, the re main ing gen er ally be ing pos i tive
for anti-PR3 (5,11,12,68,87). Many of these pa -
tients have con sti tu tional symp toms to gether with
signs of sys temic in volve ment so that the dis tinc tion
be tween WG, MPA and iNCGN is far from absolute.
ANCA have been de tected with vari able fre -
quency in pa tients with CSS (88-90). Both MPO
and PR3 have been de scribed as tar get an ti gens.
Al though Ig-A-ANCA have oc ca sion ally been
noted in Henoch-Schönlein purpura (91-93), most
stud ies have not shown this to be a sig nif i cant as so -
ci a tion with re gard to ei ther fre quency or clin i cal
fea ture of illness (94).
Pa tients with Kawasaki dis ease may have
ANCA and antiendothelial cell an ti bod ies (AECA)
but these an ti bod ies oc cur in the mi nor ity of pa -
ACTA DERMATOVENEROLOGICA CROATICA 297
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313
Ta ble 2. Dis ease as so ci a tions of C-ANCA (PR3- ANCA) and P-ANCA (MPO-ANCA) in sys temic vas -cu litis
Patients Sensitivity of
with C-ANCA PR3-ANCA P-ANCA MPO-ANCA
WG 80-90 85 5-20 24
MPA 35-45 26 40-50 58
iNCGN 30-40 50 46-65 58
CSS 14-33 33 33-42 50
PAN 3-10 0 5-30 38

tients and do not oc cur more of ten than in other pe -
di at ric fe brile illneses (95,96).
Other forms of vasculitis, par tic u larly gi ant cell
arteritis, Takayasu arteritis and Behcet¢s dis ease,
are not ANCA-as so ci ated (97,98).
ANCA in con nec tive tis sue dis eases(CTD)
ANCA have been de scribed in pa tients with a
va ri ety of CTD, in clud ing RA (99-104), SLE (105-
107), PM/DM (108), ju ve nile chronic ar thri tis (109),
re ac tive ar thri tis (110,111), re laps ing chondritis
(112,113) and anti-phospholipid syn drome (108).
ANCA in scleroderma is un com mon and is of doubt -
ful clin i cal sig nif i cance (114,115). The flu o res cence
pat terns in CTD are mostly P-ANCA. To a lesser ex -
tent, atyp i cal flu o res cence pat terns may be found,
and true C-ANCA pat terns are rare (108,116). A
mul ti tude of tar get an ti gens, in clud ing LF, HLE, LZ,
CG, MPO, HMG1 and HMG2, have been de scribed
in these dis eases (Ta ble 3). How ever, a sig nif i cant
pro por tion of tar get an ti gens for ANCA en coun tered
in this set ting re main to be iden ti fied. PR3-ANCA
occur extremely rarely in these patients (116).
While pa tients with CTD have an in creased fre -
quency of vasculitis, data to sug gest that ANCA
positivity en hances the risk of vasculitis are con tra -
dic tory (108,116). Non-vasculitis as pects of rheu -
matic dis ease ac tiv ity, se ver ity and chronicity also
fail to con sis tently cor re late with ANCA sta tus
(100,102,103,108,116). Con se quently, there is lit tle
clin i cal util ity for ANCA test ing in pa tients with CTD
in whom one of the ANCA-as so ci ated sys temic
vasculitides is not suspected.
ANCA in in flam ma tory bowel dis ease(IBD) and au to im mune liver dis eases
Shortly af ter the dis cov ery of ANCA in WG and
MPA, ANCA were dis cov ered in IBD and au to im -
mune liver dis eases (13,117-125). On IIF these
ANCA pro duce perinuclear and less of ten atyp i cal
cy to plas mic flu o res cence pat terns. MPO is not a
prom i nent tar get an ti gen for these P-ANCA (Ta ble
4). A mul ti tude of other tar get an ti gens, par tic u larly
LF, CG, actin, BPI, catalase and HMG1/2, have
been iden ti fied as tar get an ti gens in IBD (13,39-
41,45,126-128). Data from most se ries sug gest that
the prev a lence of P-ANCA is higher in ul cer ative co -
li tis (40%-80%) than in Crohn¢s dis ease (10%-
40%). Some stud ies have sug gested a higher as so -
ci a tion of ANCA in pa tients with Crohn¢s dis ease
and co lonic in volve ment (129,130), treat ment-re -
sis tant left-sided ul cer ative co li tis (131) or chronic
pouchitis (132,133). The over lap of ANCA find ings
be tween the var i ous clin i cal groups of IBD pa tients
is sig nif i cant. There fore, ANCA test ing does not fa -
cil i tate the dif fer en tial di ag no sis of pa tients with
IBD. Nei ther is the cor re la tion of titers with dis ease
activity sufficiently reliable to be useful for mon i tor -
ing IBD activity (13,123,124,129).
ANCA are also fre quently found in pa tients with
pri mary sclerosing cholangitis (PSC) and au to im -
mune hep a ti tis type 1 (50%-90%). ANCA are gen er -
ally not as so ci ated with pri mary biliary cir rho sis
298 ACTA DERMATOVENEROLOGICA CROATICA
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313
Ta ble 3. Tar get an ti gens of ANCA in con nec tive tis -sue dis eases (CTD)
Patients Target antigens in ELISA (%)
with PR3 MPO LF CG HMG1/2
SLE 0 1 11 37 37/18
RA 0 1 35 33 40/25
SS 0 0 0 22 44/11
SSc 0 18 5 5 36/18
PM/DM 0 0 27 9 18/18
SLE=systemic lupus erythematosus; RA=rheumatoid arthritis;SS=Sjögren’s syndrome; SSc=systemic sclerosis;PM/DM=polymyositis/dermatomyositis; PR3=proteinase 3;MPO=myeloperoxidase; LF=lactoferrin; CG=cathepsin G;HMG1/2=high mobility group (HMG) nonhistone chromosomalproteins 1 and 2
Ta ble 4. Tar get an ti gens of ANCA in pa tients within flam ma tory bowel and au to im mune liver dis e -ases
Patients Target antigen in ELISA (%)
with MPO LF CG Actin BPI Catalase HMG1/2
UC 2-29 5-50 0-1 NT 43 38 32
CD 0-6 1-21 0-2 NT 26 26 26
PBC NT NT NT NT 25 NT NT
PSC 0-33 0/50 NT NT 35 NT NT
AIH type 1 NT 8 0 47-52 29 NT NT
UC=ulcerative colitis; CD=Crohn’s disease; PBC=primary biliarycirrhosis; PSC=primary sclerosing cholangitis; AIH=autoimmunehepatitis; BPI=bactericidal/permeability increasing protein;HMG1/2=high mobility group (HMG) nonhistone chromosomalproteins 1 and 2; NT=not tested

(13,121,122,134-136). ANCA re ac tiv ity in au to im -
mune hep a ti tis type 1 most of ten ap pears to be di -
rected to actin (13,54,136).
ANCA in in fec tious dis eases
ANCA, mainly with ‘atyp i cal’ cy to plas mic or P-
ANCA immunofluorescence pat terns, have been
de scribed in hu man im mu no de fi ciency vi rus (HIV)
in fec tion (137,138), cys tic fi bro sis with bac te rial air -
way in fec tions (139,140), chromomycosis (141),
acute ma laria (42,142), in va sive amebiasis (143),
and in pa tients with some other in fec tions (144,
145). These ANCA are not caused by an ti bod ies
against PR3 and MPO. A re cent re port has de -
scribed the oc cur rence of BPI-IgG-ANCA and BPI-
IgA-ANCA in the ma jor ity of pa tients with cys tic fi -
bro sis (146). Anti-BPI titers were di rectly re lated to
the se ver ity of air way de struc tion. Cathepsin G has
been iden ti fied as the most sig nif i cant tar get an ti -
gen for ANCA, caus ing an atyp i cal cy to plas mic flu o -
res cence pat tern in pa tients with acute ma laria
(42,142). In va sive amebiasis is the only in fec tion
that has been re ported to be as so ci ated with PR3-
ANCA (143). The pres ence of autoantibodies caus -
ing cy to plas mic flu o res cence on eth a nol-fixed neu -
tro phils from pa tients with in fec tion shows the im -
por tance of ex clud ing in fec tious pro cesses be fore
ini ti at ing immunosuppressive ther apy. These ob -
ser va tions may sug gest that ANCA, which oc cur
tran siently in the set ting of in fec tion, and the per sis -
tent ANCA in pa tients with vasculitis may be the re -
sults of mo lec u lar mim icry in sus cep ti ble hosts
(147). Sub se quent di ver si fi ca tion of T- and B-cell
re sponses (‘epitope spread ing’) may lead to re -
sponse against dif fer ent epitopes on the same
target molecule (intramolecular spreading) or may
extend to other molecules (intermolecular spread -
ing) (148,149).
ANCA as so ci ated with drugs
In creas ing num bers of case re ports and re ports
of small se ries have iden ti fied as so ci ated dis eases
that are pre sumed to be in duced by cer tain drugs
with ANCA re ac tiv ity. The fol low ing drugs have
been con nected to au to im mune clin i cal se quels
and ANCA: hydralazine-in duced lupus with anti-
MPO and elastase an ti bod ies, hydralazine-as so ci -
ated vasculitis with anti-MPO and anti-LF an ti bod -
ies and minocycline-in duced ar thri tis, fe ver, and li -
ve do reticularis with anti-MPO an ti bod ies (150-
156). Vasculitis oc cur ring af ter propylthiouracil ther -
apy has been as so ci ated with ANCA specificities to
sev eral dif fer ent tar get an ti gens, including PR3,
MPO and elastase (152,153,157-160).
Di ag no sis of cu ta ne ous man i fes ta tions
of We ge ner¢s granulomatosis (WG)
and mi cro scopic po ly angiitis (MPA)
WG and MPA are the pro to type sys temic dis -
eases as so ci ated with ANCA. Cu ta ne ous le sions
may oc cur in up to one-half of pa tients with WG (Ta -
ble 5) (161-163). In gen eral, cu ta ne ous le sions are
more likely in pa tients who have mul ti ple or gan sys -
tem in volve ment. Cu ta ne ous le sions may also be
the first man i fes ta tion of WG and may not be
vasculitic. Pa tients may de velop cu ta ne ous le sions
be fore the on set of up per air way or pul mo nary or re -
nal symp toms, mak ing the di ag no sis of WG very dif -
fi cult for der ma tol o gist. Some pa tients may de velop
more than one type of cu ta ne ous le sions, which
may change over time or with treat ment. In or der to
best uti lize lab o ra tory test ing for ANCA, it is es sen -
tial to rec og nize the cu ta ne ous pat terns of WG and
MPA, and, more im por tant, to rec og nize those dis -
or ders that can sim u late cu ta ne ous le sions seen in
WG (Ta ble 6). Spe cific le sions are de fined as be ing
di rectly re lated to WG and not as the re sults of in -
fec tion, drug sen si tiv ity or other de fin able causes
other than WG. The most com mon spe cific man i -
fes ta tion of cu ta ne ous WG are pal pa ble purpura
and ul cer ation with the histopathologic cor re la tion
of leukocytoclastic vasculitis (LCV), most of ten
with out granuloma for ma tion, and with a histo -
ACTA DERMATOVENEROLOGICA CROATICA 299
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313
Ta ble 5. Char ac ter is tic in volve ment of Wegener’sgranulomatosis by or gan/system
Organ/system %
Upper airway 90-95
Pulmonary 54-85
Pulmonary hemorrhage 5-15
Glomerulonephritis 51-80
Gastrointestinal >5
Ocular 35-52
Nervous system 20-50
Cardiac 8-16
Cutaneous lesions 15-50

patho logic cor re late of acute and/or granulomatous
in flam ma tion, re spec tively. Many other di ag nos tic
en ti ties with cu ta ne ous man i fes ta tions are to be
con sid ered on the dif fer en tial di ag no sis of WG (Ta -
ble 6). Di ag nos tic al go rithm for cu ta ne ous WG in -
cludes care ful clin i cal ex am i na tion and clin i cal
patho logic cor re la tion to con firm the di ag no sis (Ta -
ble 7). Test ing of ANCA may play a sig nif i cant role in
the eval u a tion of pa tients sus pected to have sys -
temic vasculitis or an other ill ness with pre sen ta tion
sim i lar to WG. Only a pos i tive C-ANCA (IIF) with a
pos i tive PR3-ANCA (ELISA) re sult, and a pos i tive
P-ANCA (IIF) with a pos i tive MPO-ANCA (ELISA)
re sult are sen si tive and spe cific for WG and MPA.
Re peat ANCA test ing is war ranted to fol low the
course of the dis ease in pa tients who have proven
WG or MPA as ANCA lev els cor re late loosely with
dis ease ac tiv ity and re lapses in the ab sence of
ANCA are rare. A pa tient with LCV and other cu ta -
ne ous find ings sug ges tive of WG with a pos i tive
C-ANCA/PR3-ANCA or P-ANCA/MPO-ANCA test
result should be followed carefully for subsequent
development of systemic disease manifestations
even if there is no sign of internal organ involvement
at the time of initial presentation.
DE VEL OP MENT OF ANCA AND THEIR
ROLE IN THE PATHOGENESIS OF
VASCULITIS
In ter ac tion of ANCA with their tar getan ti gens
PR3-ANCA are able to in hibit en zy matic ac tiv ity
of na tive and re com bi nant PR3 by bind ing near the
cat a lytic do main (164). Anti-PR3 an ti bod ies pre vent
the in ac ti va tion of PR3 by its nat u ral in hib i tor alfa-1
antitrypsin (a1-AT) (165). The in hib i tory ac tiv ity dif -
fers be tween sera and is not di rectly re lated to the
amount of spe cific an ti body. In a lon gi tu di nal study it
has been shown that dis ease ac tiv ity in pa tients
with WG cor re lates with the amount of in hib i tory ac -
tiv ity of the se rum rather than with the ti ter of
PR3-ANCA (166). Like wise, MPO-ANCA may in ter -
fere with bind ing of MPO to its nat u ral in hib i tor ceru -
loplasmin (167). This suggets that es cape of the en -
zyme from its inactivation may contribute to the in -
flam ma tory process.
The phenotypic ex pres sion of a1-AT is highly
poly mor phic: se verely, me dium and non-de fi cient
pro teinase in hib i tor phe no types can be dis tin -
guished (168,169). The prev a lence of ANCA of di -
verse spec i fic ity was re mark able among a pop u la -
tion with the se verely de fi cient phe no type (170).
These data sug gest that de fi cient a1-AT ac tiv ity is
involved in the induction of ANCA.
In ter ac tion of ANCA with en do the lialcells
As men tioned above, the an ti gens rec og nized
by MPO-ANCA and PR3-ANCA are con stit u ents of
gran ules from myeloid cells and are thought to be
spe cific for cells of the monomyeloid lin eage. Re -
300 ACTA DERMATOVENEROLOGICA CROATICA
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313
Ta ble 6. Di ag nos tic en ti ties with cu ta ne ous man i -fes ta tions to be con sid ered on dif fer en tial di ag no -sis of cu ta ne ous Wegener’s granulomatosis
Leukocytoclastic or granulomatous vasculitis
Pyoderma gangrenosum
Neutrophilic dermatoses
Infection (bacterial, fungal, mycobacterial)
Infestation (e.g., amebiasis)
Malignancy (lymphoma, lymphomatpoid granulomatosis, leukemia cutis)
Cutaneous Crohn’s disease
Drug reactions (including hydralazine and minocycline)
Panniculitis (alpha-1 antitrypsin deficiency, erythema nodosum)
Connective tissue syndromes (inclusive of SLE)
Acneiform lesions
Rheumatoid nodules/papules
Granuloma annulare
Calciphylaxis
Ta ble 7. Di ag nos tic al go rithm in dif fer en tial di ag no -sis of cu ta ne ous Wegener’s granulomatosis
Characteristic clinical findings (purpura, ulcerations, nodules, etc.)
Biopsy for routine microscopy and special stains for microorganisms
Biopsy for tissue culture*
Serologic tests including ANCA (IIF and ELISA)
Longitudinal follow up of ANCA
*Recommended in the majority of cases if histopathology or clinicalfindings may also be compatible with infectious cause.ANCA-antineutrophil cytoplasmic antibodies; IIF-indirectimmunofluorescence; ELISA-target antigen-specific solid-phaseassay

cent stud ies have dem on strated, how ever, that
PR3 can be ex pressed in other cell types as well, in
par tic u lar in re nal car ci noma cells (171) and hu man
en do the lial cells (172). These cells, primed by
cytokines (TNF-a, IL-1, IFN-g), ex press PR3 in their
cy to plasm and cell sur face mak ing PR3 avail able
for in ter ac tion with ANCA. Oth ers have not been
able to show en do the lial PR3 ex pres sion (173).
MPO and PR3 are cationic pro teins and as such
may bind to an ionic struc tures such as the glo mer u -
lar base ment mem brane (GBM) and the sur face of
en do the lial cells. It has, in deed, been shown that
ANCA can bind to cul tured hu man en do the lial cells
in cu bated with MPO (174). Un der these con di tions,
anti-MPO can in duce com ple ment-de pend ent en -
do the lial cell lysis. In vi tro in cu ba tion of en do the lial
cells with PR3 in duces pro duc tion of IL-8, en do the -
lial cell apoptosis, and de tach ment and lysis of the
en do the lium (175-177). Al though these in vi tro
stud ies have dem on strated that ANCA can in ter act,
di rectly or in di rectly, with en do the lial cells, di rect
immunofluorescence stud ies from lesional tis sue
have failed to show sig nif i cant de po si tion of IgG
along the en do the lium or the glo mer u lar cap il lary
wall. Thus, the in vivo rel e vance of those in vitro
studies has yet to be established.
ANCA-me di ated neutrophil andmonocyte ac ti va tion
In vi tro ac ti va tion of neu tro phils by PR3- and
MPO-ANCA re quires prior prim ing of cells by low
doses of proinflammatory cytokines, such as
TNF-a, IL-1b or LPS. Prim ing is as so ci ated with
translocation of ANCA tar get an ti gens on the sur -
face of neu tro phils, which makes them ac ces si ble
for in ter ac tion with an ti bod ies (178-180). ANCA
(anti-PR3 or anti-MPO), bound to ap pro pri ately dis -
played tar get an ti gens, have been shown to en -
hance neutrophil ox i da tive burst and degranulation
(178,179,181,182). Re leased neutrolytic en zymes
may pro duce tis sue in jury by means that in clude in -
duc tion of en do the lial cell apoptosis, de tach ment
and cytolysis (176,177,183,184). In ad di tion, they
se crete in flam ma tory me di a tors such as TNF-a,
IL-1, IL-8 and leukotriene B4 (185,186). Upon ac ti -
va tion by ANCA, PMN ex press in creased lev els of
ad he sion mol e cules, in clud ing b2-integrins, that fa -
cil i tate bind ing to and transmigration through the
endothelial monolayer (187,188).
The pre cise mech a nism un der ly ing ANCA-in -
duced neutrophil ac ti va tion is un clear. It ap pears
that neutrophil ac ti va tion in volves both spe cific
bind ing of the an ti bod ies via F(ab¢)2-frag ments to
sur face ex pressed PR3 or MPO and in ter ac tion of
their Fc-frag ments with FcgR on neu tro phils, par tic -
u larly with FcgRIIa-re cep tor (189,190). Very re -
cently, it has been shown that li ga tion of FcgRIIa
and FcgRIIIb is nec es sary for ANCA-in duced
neutro phil ac ti va tion, but that sig nal ing cas cades by
ANCA were dif fer ent from the sig nal path ways used
by FcgR engagement only (191).
The ef fect of ANCA on monocytes has been
stud ied to a lesser ex tent. ANCA have been shown
to ac ti vate monocytes to the pro duc tion of re ac tive
ox y gen spe cies (192), IL-8, a po tent at trac tant for
PMN (193), and monocyte chemoattractant pro -
tein-1(MCP-1), even with out prior prim ing (194). In -
creased pro duc tion of MCP-1 at the site of in flam -
ma tion could play an im por tant role in the for ma tion
of granulomas by am pli fi ca tion of lo cal monocyte
re cruit ment. Monocytes from the pe riph eral blood
of pa tients with WG showed the pres ence of MPO
and PR3 on their cell sur face dur ing ac tive dis ease,
and monocytes do ex press the FcgRIIa receptor
and CD18 (195).
T-cell re ac tiv ity to ANCA-as so ci ated
an ti gens
The pres ence of cel lu lar in fil trates in in flam ma -
tory le sions, frenquently also in the form of granu -
lomas, in pa tients with WG and some other vascu -
litis, such as polyarteritis nodosa, Kawasaki and
Takayasu¢s dis ease, sug gests an im por tant role of
cell-me di ated im mu nity in the pathogenesis of
these dis eases (196-200). Immunopathologic stud -
ies have shown that the in flam ma tory in fil trate is
com posed mainly of ac ti vated T-lym pho cytes, the
ma jor ity of which are CD4+ and macrophages
(196,197,199,201-203). In agree ment with these
data, the lev els of sol u ble IL-2 re cep tor are el e vated
in WG pa tients and in crease prior to ma jor re -
lapses, pro vid ing in di rect ev i dence for a role of ac ti -
vated T-cells in sys temic vasculitis (204,205).
T-lym pho cytes iso lated from WG pa tients pro lif er -
ate in re sponse to a crude neutrophil ex tract con -
tain ing PR3 and MPO (206,207). WG pa tients re -
ACTA DERMATOVENEROLOGICA CROATICA 301
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313

sponded more fre quently and strongly to PR3 than
con trols (208,209). How ever, not all WG pa tients
re sponded to PR3, and T-cell pro lif er a tion was also
found in healthy con trols (209). In this study, strong
IL-10 pro duc tion elic ited by PR3 in vi tro may have
an im por tant func tion in vivo. Re cently, it has been
shown that B-lym pho cyte ac ti va tion is re lated to ac -
tive dis ease, whereas T-lym pho cyte ac ti va tion per -
sists dur ing re mis sion of the dis ease in pa tients with
WG, which points to an in trin si cally dis or dered im -
mu ne sys tem in this dis ease.
The in vivo role of ANCA inex per i men tal mod els
Al though all of the afore men tioned mech a nisms
may be op er a tive in vivo in id io pathic vasculitis,
con clu sive ev i dence for the patho ge nic ity of ANCA
awaits a con vinc ing an i mal model of ANCA-in -
duced vasculitis. Sev eral an i mal mod els have now
emerged that may be rel e vant in this re spect (17).
Un for tu nately, hu man anti-PR3 an ti bod ies only re -
act with neu tro phils of ba boons and not with those
of lower spe cies. Also, im mu ni za tion of rats with hu -
man PR3 does not re sult in an ti bod ies re act ing with
rat neu tro phils. In ter est ingly, a re cent study has
shown that rats in jected with syngeneic rat
apoptotic neu tro phils de velop ANCA, but the spec i -
fic ity of these ANCA could not be es tab lished and
they did not seem to be PR3 or MPO (210). Re -
cently, PR3 has been de tected and cloned in mice
(211). Un for tu nately, monoclonal and polyclonal an -
ti bod ies to hu man PR3 do not re act with cloned
mouse PR3. Antihuman PR3 was in duced in mice
by idiotypic ma nip u la tion (212,213). The mice were
im mu nized with af fin ity-pu ri fied PR3-IgG from two
WG pa tients (212). Af ter two weeks, mice de vel -
oped anti-idiotypic (mouse anti-hu man anti-PR3
an ti bod ies, ab2) and, af ter four months, anti-anti-
idiotypic an ti bod ies re act ing with hu man PR3 (ab3).
In ad di tion, the sera de rived from these mice also
re acted with hu man MPO and en do the lial sur face
pro teins. Histopathologically, ster ile microabsces -
ses de vel oped in the lungs af ter eight months, and
mice died at 8-15 months af ter im mu ni za tion with
anti-PR3-IgG. The ab3 an ti bod ies were tested for
their neutrophil ac ti vat ing abil ity show ing that these
an ti bod ies were ca pa ble to in duce ad he sion of hu -
man neu tro phils to fibronectin and to ini ti ate a re spi -
ra tory burst (213). These stud ies dem on strate that
dysregulation of the idiotypic net work may lead to
the de vel op ment of patho genic autoantibodies.
Whether this the ory is rel e vant for the induction of
ANCA-associated vasculitis cannot, however, be
proven until pathogenic idiotypes on bacterial or
viral antigens are identified.
Sev eral an i mal mod els for anti-MPO-as so ci ated
vasculitis/glomerulonephritis have been de scribed.
Brown Nor way rats (the Th2-re sponder type), ex -
posed to mer cu ric cloride (HgCl2), de vel oped a
gen er al ized au to im mune dis ease, me di ated by
T-cell de pend ent polyclonal B-cell ac ti va tion (214).
The HgCl2-in duced au to im mune syn drome is char -
ac ter ized by lymphoproliferation, high IL-4 pro duc -
tion and hypergammaglobulinemia (215). In ad di -
tion, a mul ti tude of IgG autoantibodies ap peared in
these rats, in clud ing an ti bod ies to DNA, col la gen,
thy ro glob u lin and com po nents of the glo mer u lar
base ment mem brane (216,217). In ad di tion to the
above autoantibodies, HgCl2-treated rats de vel -
oped an ti bod ies to MPO (218). These rats also de -
vel oped wide spread tis sue in jury in clud ing necro -
tizing vasculitis in the submucosal ves sels of the
du o de num and ce cum (219). Sub se quent stud ies
have dem on strated an im por tant role for autore -
active CD4+ T cells which, upon trans fer into
healthy an i mals, can in duce the dis ease (220). On
the other hand, it was shown that CD4+OX22 high
T-cells were pro tec tive since de ple tion of these
cells ag gra vates the se ver ity of tis sue in jury, al -
though the autoantibody re sponse was not af fected
(221). Treat ment with cyclosporine dur ing the early
phase of the dis ease di min ished tis sue in jury and
de layed the rise in anti-MPO and anti-GBM auto -
anti bodies (222). In con trast, treat ment with cyclo -
sporine dur ing the late phase of the dis ease ex ac er -
bated tis sue in jury al though the de vel op ment of
anti-MPO and anti-GBM autoantibodies was com -
pletely suppressed. Taken together, these ob ser va -
tions suggest that HgCl2-induced vasculitis is pri -
mar ily T-cell dependent.
The MRL/lpr strain of mice spon ta ne ously de -
velop lymphoproliferation, proliferative glomerul o -
nephritis and sys temic necrotizing vasculitis of
small and me dium-sized ar ter ies and ar te ri oles,
that par tic u larly af fect the kid ney and gall blad der
(223,224). The spon ta ne ous de vel op ment of tis sue
in jury in these mice is im mu no log i cally char ac ter -
ized by ac cu mu la tion of T-cells with polyclonal
302 ACTA DERMATOVENEROLOGICA CROATICA
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313

B-cell stim u la tion re sult ing in the ap pear ance of
rheu ma toid fac tors and autoantibodies of di verse
spec i fic ity in clud ing autoantibodies against ds-
DNA, ss-DNA, his tones, smooth mus cle and ANCA
(225). How ever, monoclonal IgG an ti bod ies de rived
from these mice were found to be polyreactive,
recognizing MPO, LF and DNA (226).
SCG/KJ strain of mice, de rived from the F1 hy -
brid of BXSB and MRL/lpr mice, spon ta ne ously de -
velop rap idly pro gres sive glomerulonephritis and
necrotizing vasculitis (227). The sera from these
mice pro duce a perinuclear ANCA stain ing pat tern
on hu man and murine neu tro phils and re act with
murine neutrophil ex tract and hu man MPO by
ELISA (228,229). Trans fer of MPO spe cific hybrido -
mas de rived from SCG/KJ mice into the peri to neum
of nude mice in duced proteinuria, al though histolo -
gical ly no ev i dence for glomerulonephritis or vascu -
litis was found (228).
In duc tion of a se lec tive au to im mune re sponse to
MPO is a more di rect method of study ing the
pathophysiologic role of anti-MPO. Im mu ni za tion of
Brown Nor way rats with hu man MPO in com plete
Freund¢s adjuvant re sults in the de vel op ment of
anti-hu man MPO an ti bod ies cross-re act ing with rat
MPO and de layed-type hy per sen si tiv ity to hu man
MPO (230,231). The au to im mune re sponse alone
does not re sult in clin i cal le sions. How ever, af ter
uni lat eral per fu sion of the left kid ney with prod ucts
of ac ti vated neu tro phils con sist ing of proteolytic en -
zymes (HLE and PR3), MPO and its sub strate
H2O2, these MPO-im mu nized rats de velop necr o -
tizing cres cen tic glomerulonephritis with in ter sti tial
tubulonephritis and vasculitis. Sys temic in jec tion of
lysosomal en zymes, MPO and H2O2 in the jug u lar
vein of MPO-im mu nized rats also re sulted in small
ves sel vasculitis and gi ant cell for ma tion in the
lungs and guts but not in the kid neys (231). The lo -
cal iza tion of the in flam ma tory pro cess in the lungs
and guts sug gests that local factors, e.g., mu -
cosa-as so ci ated microbial elements, are involved.
The patho genic po ten tial of anti-MPO an ti bod -
ies in vivo has also been dem on strated in glo mer u -
lar base ment mem brane (anti-GBM) ne phri tis in
Brown Nor way rats pre vi ously im mu nized with hu -
man MPO (232). Im mu nized rats not only de vel -
oped an ti bod ies to hu man MPO but to rat MPO as
well. Fol low ing in jec tion of a subnephritogenic dose
of rab bit anti-rat GBM an ti bod ies, se vere glomeru -
lonephritis de vel oped char ac ter ized by hematuria,
proteinuria, fibrinoid ne cro sis of glo mer u lar cap il lar -
ies, ex ten sive fi brin ac cu mu la tion of monocy t -
es/mac ro phages and cres cent for ma tion. In con trol
im mu nized rats in jected with the anti-GBM an ti bod -
ies, only mild glomerulonephritis was found with out
ev i dence for cres cent for ma tion, sug gest ing that
the autologous anti-rat MPO antibodies are re s pon -
si ble for the exacerbation of the anti-GBM disease.
These stud ies suport the hy poth e sis that the
pres ence of ANCA it self is not suf fi cient to cause tis -
sue in jury. Ad di tional fac tors in duc ing a proinflam -
matory en vi ron ment are needed, which ini tially re -
sult in prim ing of neu tro phils and monocytes and
ac ti va tion of the en do the lium. Af ter that, ANCA ac ti -
vate primed neu tro phils/monocytes and form in situ
im mune com plexes with ANCA an ti gens re leased
from ac ti vated neu tro phils, thereby ex ac er bat ing
the in flam ma tory re sponse and fi nally leading to
vas culitis and tissue destruction.
IN TE GRA TIVE VIEW OF THE
PO TEN TIAL IM MUNE MECH A NISMS
IN THE PATHOGENESIS OF
ANCA-AS SO CI ATED VASCULITIS
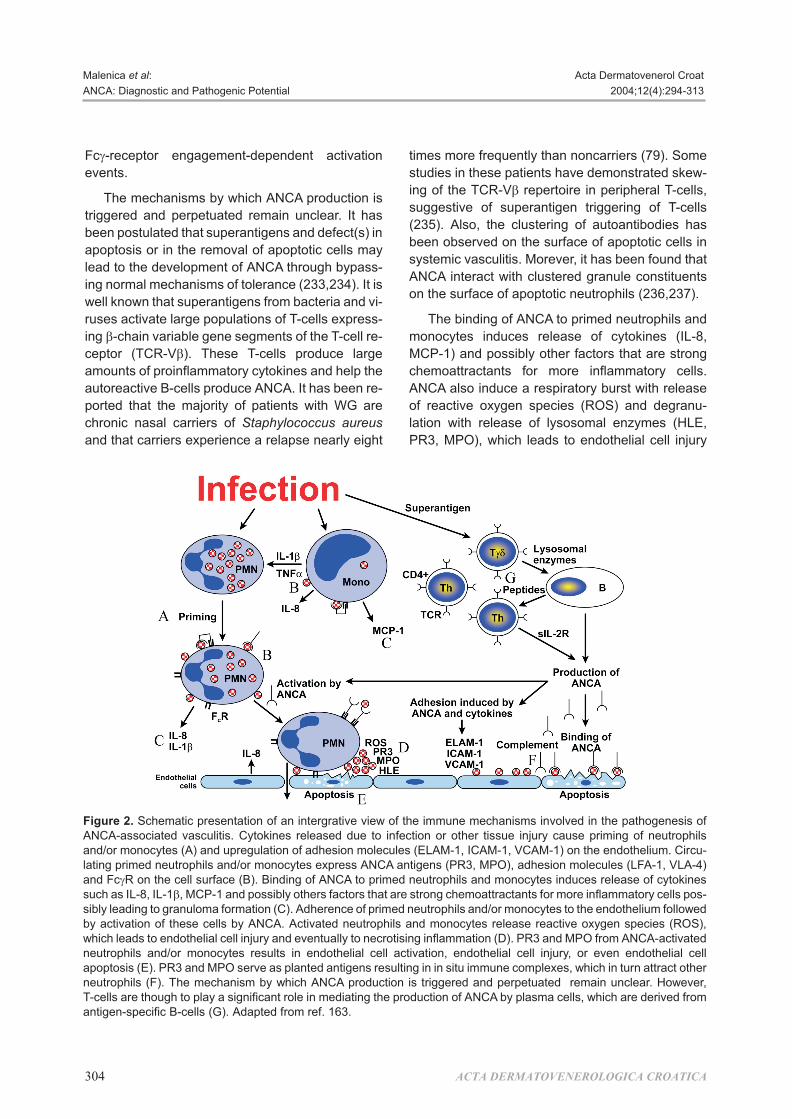
Sche matic pre sen ta tion of an in te gra tive view of
ANCA-me di ated vas cu lar tis sue dam age is shown
in Fig ure 2. The model is based on the four pre req -
ui sites for en do the lial cell dam age by ANCA: 1) the
pres ence of ANCA; 2) ex pres sion of tar get an ti gens
for ANCA on primed neu tro phils and monocytes; 3)
the ne ces sity of an in ter ac tion be tween primed neu -
tro phils and en do the lium by means of b2-integrins;
and 4) ac ti va tion of endothelial cells (7,8,16-20).
In fec tion or other tis sue in jury in duces an in flam -
ma tory re sponse as so ci ated with cytokine re lease
(TNF-a, IL-1b) re sult ing in prim ing of neu tro phils
and/or monocytes. Prim ing of these cells prompts
ex pres sion of ANCA tar get an ti gens (PR3, MPO) on
their sur face. In this man ner the autoantigen be -
comes ac ces si ble to the cir cu lat ing ANCA. Primed
neu tro phils and monocytes also ex press Fcg-re -
cep tors on their sur face. Con se quently, ANCA can
bind to their sur face via their con stant re gion (Fc).
Si mul ta neous bind ing of cir cu lat ing an ti gen re -
leased from ac ti vated in flam ma tory cells may
cause crosslinking of Fcg-re cep tors initating the
ACTA DERMATOVENEROLOGICA CROATICA 303
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313
Fcg- re cep tor engagement-dependent activation
events.
The mech a nisms by which ANCA pro duc tion is
trig gered and per pet u ated re main un clear. It has
been pos tu lated that superantigens and de fect(s) in
apoptosis or in the re moval of apoptotic cells may
lead to the de vel op ment of ANCA through by pass -
ing nor mal mech a nisms of tol er ance (233,234). It is
well known that superantigens from bac te ria and vi -
ruses ac ti vate large pop u la tions of T-cells ex press -
ing b-chain vari able gene seg ments of the T-cell re -
cep tor (TCR-Vb). These T-cells pro duce large
amounts of proinflammatory cytokines and help the
autoreactive B-cells pro duce ANCA. It has been re -
ported that the ma jor ity of pa tients with WG are
chronic na sal car ri ers of Staph y lo coc cus aureus
and that car ri ers ex pe ri ence a re lapse nearly eight
times more fre quently than noncarriers (79). Some
stud ies in these pa tients have dem on strated skew -
ing of the TCR-Vb rep er toire in pe riph eral T-cells,
sug ges tive of superantigen trig ger ing of T-cells
(235). Also, the clus ter ing of autoantibodies has
been ob served on the sur face of apoptotic cells in
sys temic vasculitis. Morever, it has been found that
ANCA in ter act with clus tered granule constituents
on the surface of apoptotic neutrophils (236,237).
The bind ing of ANCA to primed neu tro phils and
monocytes in duces re lease of cytokines (IL-8,
MCP-1) and pos si bly other fac tors that are strong
chemoattractants for more in flam ma tory cells.
ANCA also in duce a re spi ra tory burst with re lease
of re ac tive ox y gen spe cies (ROS) and degranu -
lation with re lease of lysosomal en zymes (HLE,
PR3, MPO), which leads to en do the lial cell in jury
304 ACTA DERMATOVENEROLOGICA CROATICA
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313
Fig ure 2. Sche matic pre sen ta tion of an intergrative view of the im mune mech a nisms in volved in the pathogenesis ofANCA-as so ci ated vasculitis. Cytokines re leased due to in fec tion or other tis sue in jury cause prim ing of neu tro philsand/or monocytes (A) and upregulation of ad he sion mol e cules (ELAM-1, ICAM-1, VCAM-1) on the en do the lium. Cir cu -lat ing primed neu tro phils and/or monocytes ex press ANCA an ti gens (PR3, MPO), ad he sion mol e cules (LFA-1, VLA-4)and FcgR on the cell sur face (B). Bind ing of ANCA to primed neu tro phils and monocytes in duces re lease of cytokinessuch as IL-8, IL-1b, MCP-1 and pos si bly oth ers fac tors that are strong chemoattractants for more in flam ma tory cells pos -si bly lead ing to granuloma for ma tion (C). Ad her ence of primed neu tro phils and/or monocytes to the en do the lium fol lowed by ac ti va tion of these cells by ANCA. Ac ti vated neu tro phils and monocytes re lease re ac tive ox y gen spe cies (ROS),which leads to en do the lial cell in jury and even tu ally to necrotising in flam ma tion (D). PR3 and MPO from ANCA-ac ti vatedneu tro phils and/or monocytes re sults in en do the lial cell ac ti va tion, en do the lial cell in jury, or even en do the lial cellapoptosis (E). PR3 and MPO serve as planted an ti gens re sult ing in in situ im mune com plexes, which in turn at tract otherneu tro phils (F). The mech a nism by which ANCA pro duc tion is trig gered and per pet u ated re main un clear. How ever,T-cells are though to play a sig nif i cant role in me di at ing the pro duc tion of ANCA by plasma cells, which are de rived froman ti gen-spe cific B-cells (G). Adapted from ref. 163.
(apoptosis) and even tu ally to necrotizing in flam ma -
tion. Ex cept for cytokines, ANCA stim u la tion also
ac ti vates en do the lial cells re sult ing in in creased ad -
her ence of primed and ac ti vated neu tro phils to their
sur face. Con se quently, the re lease of cytotoxic
neutrophil con stit u ents can di rectly cause en do the -
lial cell dam age by di rect cytotoxicity, apoptosis and
com ple ment ac ti va tion by immune complex bound
on the endothelial cell surface.
This con cep tual scheme is con sis tent with clin i -
cal ob ser va tions and an i mal model data, which
clearly in di cate that ANCA alone do not nec es sar ily
lead to dis ease man i fes ta tions. Co factors that lead
to ac ti va tion of in flam ma tory and en do the lial cells
seem to be re quired to ac ti vate var i ous patho genic
mech a nisms leading to small vessel vasculitis.
CON CLU SION
The sig nif i cance of ANCA as di ag nos tic mark ers
for sys temic necrotizing vasculitis or id io pathic
necrotizing cres cen tic glomerulonephritis is well es -
tab lished. De tec tion of PR3-ANCA strongly sug -
gests a di ag no sis of Wegener¢s granulomatosis,
and changes in se rum lev els of these autoantibo -
dies seem to mir ror dis ease ac tiv ity. MPO-ANCA
are as so ci ated with var i ous forms of sys temic nec -
ro tizing vasculitis in clud ing id io pathic necrotizing
cres cen tic glomerulonephritis. The di ag nos tic sig -
nif i cance of ANCA against other tar get an ti gens is
not clear. Their use ful ness in mea sur ing dis ease
ac tiv ity is at pres ent not clear, al though some stud -
ies suggest that rises in anti-MPO levels precede
relapses.
Many ques tions re main con cern ing the patho -
physi o logic role of ANCA, al though both in vi tro and
in vivo ex per i men tal data strongly sup port a patho -
genic role for ANCA in vasculitis and glomerulo -
nephritis. How ever, ANCA alone are not suf fi cient
and other, prob a bly ex og e nous fac tors seem nec -
es sary for dis ease ac ti va tion and (re)ac ti va tion. Cir -
cum stan tial ev i dence from hu man (Staph y lo coc cus
aureus car riage) and ex per i men tal (e.g., the mer cu -
ric chlo ride model) stud ies sug gest that ex og e nous
fac tors, pos si bly of a microbial nature, are involved
in disease expression.
Ac knowl edge ments. We thank Mr. Zoran Tadiæ
from De part ment of An i mal Phys i ol ogy, School of
Nat u ral Sci ences and Math e mat ics, Uni ver sity of
Zagreb, for his il lus tra tion of the immunopathogenic
mech a nism of ANCA.
Abbrevations
AECA antiendothelial cell an ti body
ACPA anticytoplasmic an ti body
a1-AT a1-antitrypsin
AIH au to im mune hep a ti tis
ANA antinuclear an ti body
ANCA antineutrophil cy to plas mic an ti body
a/P-ANCA ‘atyp i cal’ perinuclear ANCA
C-ANCA cy to plas mic ANCA
P-ANCA perinuclear ANCA
BPI bac te ri cidal/per me abil ity-in creas ing pro tein
CD Crohn’s dis ease
CG cathepsin G
CTD con nec tive tis sue dis eases
CSS Churg-Strauss syn drome
ELAM en do the lial ad he sion mol e cule
ELISA en zyme-linked immunosorbent as say
FcgR Fc-gamma re cep tors
GBM glo mer u lar base ment mem brane
GS-ANA granulocyte-spe cific ANA
HLE hu man leu ko cyte elastase
HMG1 and 2 high mo til ity group of nonhistone chro mo -somal pro teins 1 and 2
H2O2 hy dro gen per ox ide
IB immunoblot
IBD in flam ma tory bowel dis ease
ICAM-1 intercellular ad he sion mol e cule-1
IIF in di rect immunofluorescence
IFN-g in ter feron-g
IL-1b interleukin-1b
IL-8 interleukin-8
iNCGN id io pathic necrotizing cres cen ticglomerulonephritis
LF lactoferrin
LCV leukocytoclastic vasculitis
LFA-1 lym pho cyte func tion an ti gen-1
LPS lipopolysaccharide
LZ lysozyme
MCP-1 monocyte chemoattractant pro tein-1
MPA mi cro scopic polyangiitis
MPO myeloperoxidase
MPO-ANCA myeloperoxidase - antineutrophic cytoplasma an ti body
PAN polyarteritis nodosa
PBC pri mary biliary cir rho sis
PM/DM polymyositis/dermatomyositis
PR3 proteinase-3
PR3-ANCA proteinase-3 antineutrophic cytoplasma an ti body
ACTA DERMATOVENEROLOGICA CROATICA 305
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313

PSC pri mary sclerosing cholangitis
RA rheu ma toid ar thri tis
RIA radioimmunoassay
ROS re ac tive ox y gen spe cies
SLE sys temic lupus erythematosus
SS Sjögren’s syn drome
SSc sys temic scle ro sis
TCR-Vb -cell re cep tor
TNF-a tu mor ne cro sis fac tor a
UC ul cer ative co li tis
VCAM-1 vas cu lar ad he sion mol e cule-1
VLA-4 very late an ti gen-4
WG Wegener’s granulomatosis
Ref er ences
1 Davies DJ, Moran JE, Niall JF, Ryan GB. Seg men talnecrotising glomerulonephritis with antineutrophilan ti body: pos si ble arborvirus ae ti ol ogy. BMJ 1982;318:1651-7.
2 Hall JB, Wadham BM, Wood CJ, Ash ton V, AdamWR. Vasculitis and glomerulonephritis: a sub groupwith an antineutrophil cy to plas mic an ti body. Aust NZ J Med 1984;14:277-8.
3 Van der Wouder FJ, Ras mus sen N, Lobatto S, Wiik A,Perman H, van Es LA, et al. Autoantibodies to neu tro -phils and monocytes: a new tool for di ag no sis and amarker of dis ease ac tiv ity in Wegener¢s granulo -matosis. Lan cet 1985;1:425-9.
4 Sav age COS, Winearls CG, Jones S, Mar shall PD, Lock -wood CM. Per spec tive study of radioimmuno assay foran ti bod ies against neutrophil cy to plasm in di ag no sis of sys temic vasculitis. Lan cet 1987;1:1389-93.
5 Falk RJ, Jennette JC. Anti-neutrophil cy to plas micautoantibodies with spec i fic ity for myeloperoxidasein pa tients with sys temic vasculitis and cres cen ticglomerulonephritis. N Engl J Med 1988;25:1651-7.
6 Hagen EC, Ballieux BE, Van Es LA, Daha MR, Van derWoude FJ. Antineutrophil cy to plas mic autoanti bo -dies: a re view of the an ti gens in volved, the as says andthe clin i cal and pos si ble pathogenetic con se quences.Blood 1993;81:1996-2002.
7 Kallenberg MGC, Brouwer E, Ween ing JJ, Co henTervaert WJ. Anti-neutrophil cy to plas mic an ti bod ies:cur rent di ag nos tic and pathophysiological po ten tial.Kid ney Int 1994;46:1-15.
8 Gross LW, Schmitt WH, Csernok E. ANCA and as so ci -ated dis eases: im mu no logic and pathogenetic as -pects. Clin Exp Immunol 1993;91:1-12.
9 Gross LW, Csernok E. Immunodiagnostic and patho -physiologic as pects of antineutrophil cy to plas mic an -ti bod ies in vasculitis. Curr Opin Rheumatol 1995;7:11-9.
10 Mayet JW, Helmreich-Becker I, Meyer zumBuschenfelde K-H. The pathophysiology of anti- neutrophil cy to plas mic an ti bod ies (ANCA) and theirclin i cal rel e vance. Crit Rev Oncol Hematol 1996;23:151-65.
11 Hoffman SG, Specks U. Antineutrophil cy to plas mican ti bod ies. Ar thri tis Rheum 1998;41:1521-37.
12 Schonermarck U, Lamprecht P, Csernok E, Gross LW.Prev a lence and spec trum of rheu matic dis eases as so -ci ated with proteinase 3-antineutrophil cy to plas mican ti bod ies (ANCA) and myeloperoxidase-ANCA.Rheumatology 2001;40:178-84.
13 Wiik A. Neutrophil-spe cific autoantibodies in chronic in flam ma tory bowel dis ease. Autoimmunity Rev2002;1:67-72.
14 Kallenberg CGM, Brouwer E, Mulder LHA, StegemanCA, Ween ing JJ, Co hen Tervaert WJ. ANCA – patho -physiology re vis ited. Clin Exp Immunol 1995;100:1-3.
15 Cid CM. New de vel op ments in the pathogenesis of sys -temic vasculitis. Curr Opin Rheumatol 1996;8:1-11.
16 Harper L, Sav age COS. Pathogenesis of ANCA-as so ci -ated sys temic vasculitis. J Pathol 2000;190:349-59.
17 Heeringa P, Brouwer E, Co hen Tervaert WJ, Ween ingJJ, Kallenberg CGM. An i mal mod els of anti-neutrophil cy to plas mic an ti body as so ci ated vasculitis. Kid ney Int 1998;53:253-63.
18 Hewins P, Co hen Tervaert JW, Sav age COS,Kallenberg CGM. Is Wegener¢s granulomatosis an au -to im mune dis ease? Curr Opin Rheumatol 2000;12:3-10.
19 Kallenberg CGM, Ravel A, Stegeman AC, Lim burgCP. New in sights into the pathogenesis of antineutro -phil cy to plas mic autoantibody-as so ci ated vasculitis.Autoimmun Rev 2002;1:65-6.
20 Reumaux D, Duthilleu P, Roos D. Pathogenesis of dis -eases with antineutrophil cy to plasm autoantibodies.Hu man Immunol 2004;65:1-12.
21 Wiik A. De lin ea tion of a stan dard pro ce dure for in di -rect immunofluorescence de tec tion of ANCA. AMPIS1989;97 (Suppl 6):12-3.
22 Hagen EC, Andrassy K, Csernok E, Daha MR, Gas kinG, Gross WL, et al. The value of in di rect immuno fluo -rescence and solid phase tech niques for ANCA de tec -tion. J Immunol Meth ods 1993;159:1-16.
23 Sun J, Fass DN, Hud son JA, Viss MA, Homburger HA,Specks U. Cap ture-ELISA based on re com bi nant pro -teinase 3 (PR3) is sen si tive for PR3-ANCA test ing andal lows de tec tion of PR3 and PR3-ANCA/PR3 im munecom plexes. J Immunol Meth ods 1998;221:111-23.
24 Hagen EC, Andrassy K, Csernok E, Daha MR, Gas kinG, Gross W, Hansen B, Heigl Z, Jayne D, KallenbergCGM, Lesavre P, Lock wood CM, Lüdemann J,Mascart-Lemone F, Mirapeix E, Pusey C, Ras mus senN, Sinico RA, Tzioufas A, Wieslander J, Wiik A, Vanden Woude FJ, EC/BCR Pro ject for ANCA as say stand -ardi sa tion. De vel op ment and a stand ardi sa tion ofsolid phase as says for the de tec tion of anti-neutrophilcy to plas mic an ti bod ies (ANCA. A re port on the sec -ond phase of an in ter na tional co op er a tive study onthe stand ardi sa tion of ANCA as says. J ImmunolMeth ods 1996;196:1-15.
25 Savige J, Gillis D, Benson E, Davies D, Esnault CJ,Paspaliaris B, Pollock W, Pusey Ch, Sav age OSC,Silvestrini R, van der Woude F, Wieslander J, Wiik A,for the In ter na tional Group for Con sen sus State menton Test ing and Re port ing of Antineutrophil Cy to plas -mic An ti bod ies (ANCA). Am J Clin Pathol 1999;111:507-13.
26 Savige AJ, Paspaliaris B, Silvestrini R, Davies D,Nikoloutsopoulos T, Sturgess A, et al. A re view ofimmunofluorescent pat terns as so ci ated with anti -neutrophil cy to plas mic an ti bod ies (ANCA) and their
306 ACTA DERMATOVENEROLOGICA CROATICA
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313

dif fer en ti a tion from other an ti bod ies. J Clin Pathol1998;51:568-75.
27 Co hen Tervaert JW, Goldschmeding R, Elema JD,Lim burg PC, van de Giessen M, Huitema MG, et al.As so ci a tion of autoantibodies to myeloperoxidasewith dif fer ent forms of vasculitis. Ar thri tis Rheum1990;33:1264-72.
28 Lee SS, Lawton MWJ, Chak W. Dis tinc tion be tweenantinuclear an ti body and P-ANCA. J Clin Pathol1991;44:962-3.
29 Jenne DE, Tschoop J, Lüdemann J, Utecht B, GrossWL. Wegener’s autoantigen de coded. Na ture 1990;346:520.
30 Lüdemann J, Csernok E, Ulmer M, Lemke H, UtechtB, Rautmann A. Anti-neutrophil cy to plasm an ti bod iesin Wegener¢s granulomatosis: immunodiagnosticvalue, monoclonal an ti bod ies and char ac ter iza tion ofthe tar get an ti gen. Neth J Med 1990;36:157-62.
31 Jennette JC, Hoidal JH, Falk RJ. Spec i fic ity of anti- neutrophil cy to plas mic an ti bod ies for proteinase 3.Blood 1990;75:2263-4.
32 Jennings U, Chang L, Savige JA. Anti-proteinase an ti -bod ies, their char ac ter iza tion and dis ease as so ci a -tions. Clin Exp Immunol 1994;95:251-6.
33 Specks U, Wiegert EM, Momburger HA. Hu man mastcells ex press ing re com bi nant proteinase 3 (PR3) assub strate for clin i cal test ing for anti-neutrophil cy to -plas mic an ti bod ies (ANCA). Clin Exp Immunol 1997;109:286-95.
34 Bini P, Gabay JE, Teitel A, Melchior M, Zhou J-L,Elkon KB. Antineutrophil cy to plas mic autoantibodiesin Wegener¢s granulomatosis rec og nize conformatio -nal epitopes on proteinase 3. J Immunol 1992;149:1409-15.
35 Segelmark M, Baslund B, Weislander J. Some pa tientswith antimyeloperoxidase an ti bod ies have a cANCApat tern. Clin Exp Immunol 1994;96:458-65.
36 Co hen Tervaert JW, Goldschmeding R, Elema JD,Lim burg PC, van der Giessen M, Huitema MG, et al.As so ci a tion of autoantibodies to myeloperoxidasewith dif fer ent forms of vasculitis. Ar thri tis Rheum1990;33:1264-72.
37 Nassberger L, Jonsson H, Sjoholm AG, Sturfelt G. Cir -cu lat ing antielastase in sys temic lupus erythematosus. Lan cet 1989;1:509.
38 Co hen Tervaert JW, Mulder L, Stegeman C, Elema J,Huitema M, The TH, Kallenberg CGM. Oc cur rence of autoantibodies to hu man leu co cyte elastase inWegener¢s granulomatosis and other in flam ma torydis or ders. Ann Rheum Dis 1993;52:115-20.
39 Halbwaches-Mecarelli L, Nusbaum P, Noel LH,Reumaux D, Erlinger S, Grünfeld JP, et al. Anti -neutrophil cy to plas mic an ti bod ies (ANCA) di rectedagainst cathepsin G in ul cer ative co li tis, Crohn¢s dis -ease and pri mary sclerosing cholangitis. Clin ExpImmunol 1992;90:79-84.
40 Mayet WJ, Hermann E, Finsterwalder J, Rieder H,Poralla T, Meyer zum Büschenfelde KH. An ti bod iesto cathepsin G in Crohn´s dis ease. Eur J Clin In vest1992;22:427-33.
41 Sobajima J, Ozaki S, Okazaki T, Osakada F, Sumita S,Mori K, et al. Anti-neutrophil cy to plas mic an ti bod ies(ANCA) in ul cer ative co li tis: anti-cathepsin G and anovel an ti body cor re late with a re frac tory type. ClinExp Immunol 1996;105:120-4.
42 Yahya TM, Ben e dict S, Shalabi A, Bayomi R.Anti-neutrophil cy to plas mic an ti body (ANCA) in ma -laria is di rected against cathepsin G. Clin ExpImmunol 1997;110:41-4.
43 Corremans IEM, Hagen EC, Daha MR, van der Woude FJ, van der Voort EAM, Kleijburg-Van Der Keur C, etal. Antilactoferrin an ti bod ies in pa tients with rheu ma -toid ar thri tis are as so ci ated with vasculitis. Ar thri tisRheum 1992;35:1466-75.
44 Lee SS, Lawton JWM, Chan CE. Antilactoferrin an ti -body in sys temic lupus erythematosus. Br J Rheumatol 1992;31:669-73.
45 Peen E, Almer S, Bodemar G, Ryden BO, Sjolin C,Tejle K, et al. Anti-lactoferrin an ti bod ies and othertypes of ANCA in ul cer ative co li tis, pri mary sclerosing cholangitis and Crohn¢s dis ease. Gut 1993;34:56-62.
46 Broekroelofs J, Mulder AHL, Nelis GF, WesterveldBD, Co hen Tervaert JW, Kallenberg CGM. Anti- neutrophil cy to plas mic an ti bod ies (ANCA) in serafrom pa tients with in flam ma tory bowel dis ease (IBD):re la tion to dis ease pat tern and dis ease ac tiv ity. DigDis Sci 1994;39:545-9.
47 Brimnes J, Niel sen OH, Wiik O, Heegaard NHH. Mo -lec u lar tar gets of autoantibodies to neu tro phils in pa -tients with ul cer ative co li tis. Dig Dis Sci 1999;44:415-23.
48 Zhao MH, Lock wood CM. Azurocidin is a novel an ti -gen for anti-neutrophil cy to plas mic autoantibodies(ANCA) in sys temic vasculitis. Clin Exp Immunol1996;103:397-402.
49 Moodie FDL, Leaker B, Cam bridge G, Totty NF, SegalAW. Al pha-enolase: a novel cytosolic autoantigen inANCA pos i tive vasculitis. Kid ney Int 1993;43:675-81.
50 Roozendaal C, Zhao MH, Horst G, Lock wood CM,Kleibeuker JH, Lim burg PC, et al. Catalase andalfa-enolase: two novel granulocyte an ti gens in in -flam ma tory bowel dis ease (IBD). Clin Exp Immunol1998;112:10-6.
51 Orth T, Kellner R, Diekmann O, Faust J, Meyer zumBuschenfelde KH, Mayet WJ. Iden ti fi ca tion and char -ac ter iza tion of autoantibodies against catalase and al -pha-enolase in pa tients with pri mary sclerosingcholangitis. Clin Exp Immunol 1998;112:507-15.
52 Dighiero G, Lymberi P, Monot C, Abauf N. Sera withhigh lev els of anti-smooth mus cle and anti-mi to chon -drial an ti bod ies fre quently bind to cytoskeleton pro -teins. Clin Exp Immunol 1990;82:52-66.
53 Kellner R, Orth T, Mayet WJ. Char ac ter iza tion of tar -get an ti gens from anti-neutrophil cy to plas mic an ti -bod ies in au to im mune hep a ti tis type 1. Elec tro pho re -sis 1997;18:507-10.
54 Orth T, Gerken G, Kellner R, Meyer zumBüschenfelde KH, Mayet WJ. Actin is a tar get an ti -gen of antineutrophil cy to plas mic an ti bod ies(ANCA) in au to im mune hep a ti tis type 1. J Hepatol1997;26:37-47.
55 Sobajima J, Ozaki S, Osakada F, Uesugi H, ShirakawaH, Yoshida M, et al. Novel autoantigens ofperinuclear antineutrophil cy to plas mic an ti bod ies(P-ANCA) in ul cer ative co li tis: novel nonhistone chro -mo somal pro teins, HMG1 and HMG2. Clin ExpImmunol 1997;107:135-40.
56 Uesugi H, Ozaki S, Sobajima J, Osakada F, ShirakawaH, Yoshida M, et al. Prev a lence and char ac ter iza tionof novel pANCA an ti bod ies to the high mo bil itygroup nonhistone chro mo somal pro teins HMG1 and
ACTA DERMATOVENEROLOGICA CROATICA 307
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313
HMG2 in sys temic rheu matic dis eases. J Rheumatol1998;25:703-9.
57 Sobajima J, Ozaki S, Uesugi H, Osakada F, ShirakawaH, Yoshida M, et al. Prev a lence and char ac ter iza tionof perinuclear anti-neutrophil cy to plas mic an ti bod ies(p-ANCA) di rected against HMG1 and HMG2 in ul -cer ative co li tis (UC). Clin Exp Immunol 1998;111:402-7.
58 Zhao MH, Jones SJ, Lock wood CM. Bac te ri cidal/per -me abil ity in creas ing (BPI) pro tein is an im por tant an ti -gen for antineutrophil cy to plas mic autoantibodies(ANCA) in vasculitis. Clin Exp Immunol 1996;99:49-56.
59 Stoffel MP, Csernok E, Herzberg C, Johnston T, CarrolSF, Gross WL. Anti-neutrophil cy to plas mic an ti bod ies (ANCA) di rected against bac te ri cidal/per me abil ity in -creas ing pro tein (BPI): a new seromarker for in flam -ma tory bowel dis eases and as so ci ated dis or ders. ClinExp Immunol 1996;104:54-9.
60 Yang JJ, Tuttle R, Falk RJ, Jennette JC. Fre quency ofanti-bac te ri cidal/per me abil ity-in creas ing pro tein (BPI) and anti-azurocidin in pa tients with re nal dis ease.Clin Exp Immunol 1996;105:125-31.
61 Schultz H, Csernok E, Johnston TW, Lock wood CM,Gross WL. Use of na tive and re com bi nant bac te ri -cidal/per me abil ity-in creas ing pro tein (BPI) as an ti gens for de tec tion of BPI-ANCA. J Immunol Meth ods1997;205:127-33.
62 Eggena M, Cohavy O, Parseghian MH, Hamkalo BA,Clem ens D, Ta SR, et al. Iden ti fi ca tion of histone H1as a cog nate an ti gen of the ul cer ative co li tis-as so ci -ated marker an ti body pANCA. J Autoimmun 2000;14:83-97.
63 Nolle B, Specks U, Lüdemann J, Ronrbach MS,Deremee RA, Gross WL. Anticytoplasmic an ti bod ies:their immunodiagnostic value in Wegener¢s granulo -matosis. Ann In tern Med 1989;111:28-40.
64 Hagen CE, Daha MR, Hermans J, Andrassy K, Csernok E, Gas kin G, et al. Di ag nos tic value of stan dard izedas says for anti-neutrophil cy to plas mic an ti bod ies inid io pathic sys temic vasculitis. EC/BCR pro ject forANCA stan dard iza tion. Kid ney Int 1998;53:743-53.
65 Malenica B, Božièeviæ M, Batiniæ D, Marušiæ M,Juretiæ A, Sentiæ M, et al. The sig nif i cance of de tec tion of anti-neutrophil cy to plas mic an ti bod ies (ANCA). Pe -riod Biol 1996; 98:505-10.
66 Westman WAK, Selga D, Bygren P, Segelmark M,Baslund B, Wiik A, et al. Clin i cal eval u a tion of a cap -ture ELISA for de tec tion of proteinase-3 antineutrophil cy to plas mic an ti body. Tech ni cal note. Kid ney Int1998;53:1230-6.
67 Venning MC, Quinn A, Broomhead V, Bird AG. An ti -bod ies di rected against neu tro phils (c-ANCA andp-ANCA) are of dinstict di ag nos tic value in sys temicvasculitis. Q J Med 1990;77:1287-96.
68 Savige JA, Gallicchio M, Georgiu T, Davies DJ. Di -verse tar get an ti gens rec og nized by cir cu lat ing an ti -bod ies in antineutrophil cy to plasm an ti body-as so ci -ated re nal vasculitides. Clin Exp Immunol 1990;82:238-43.
69 Co hen Tervaert JW, Mulder AHL, Stegemann CA,Elema JD, Huitema MG, The TH, et al. The oc cur -rence of autoantibodies to hu man leu ko cyte elastasein Wegener¢s granulomatosis and other in flam ma torydis or ders. Ann Rheum Dis 1993;552:115-20.
70 Rao JK, Weinberger M, Oddone EZ, Allen NB,Laudsman P, Feussner, JR. The role of antineutrophilcy to plas mic an ti body (cANCA) test ing in the di ag no -sis of Wegener¢s granulomatosis. Ann In tern Med1995;123:925-32.
71 Co hen Tervaert JW, Van der Woude FJ, Fauci AS,Ambrus JL, Velosa J, Keane WF, et al. As so ci a tion be -tween ac tive Wegener¢s granulomatosis and anticyto -plasmic an ti bod ies. Arch In tern Med 1989;149:2461-5.
72 Jayne DRW, Gas kin G, Pusey CD, Lock wood CM.ANCA and pre dict ing re lapse in sys temic vasculitis. Q J Med 1995; 88:127-33.
73 Egner W, Cha pel HM. Ti tra tion of an ti bod ies againstneutrophil cy to plas mic an ti gens is use ful in mon i tor -ing dis ease ac tiv ity in sys temic vasculitides. Clin ExpImmunol 1990;82:244-9.
74 Rus sell AK, Fass ND, Specks U. Antineutrophil cy to -plas mic an ti bod ies re act ing with the pro form ofproteinase 3 and dis ease ac tiv ity in pa tients withWegener`s granulomatosis and mi cro scopicpolyangiitis. Ar thri tis Rheum 2001;44:463-8.
75 Kerr GS, Fleischer THA, Hallahan CW, Leavitt RY,Fauci AS, Hoffman GS. Lim ited prog nos tic value ofchanges in antineutrophil cy to plas mic an ti body ti terin pa tients with Wegener¢s granulomatosis. Ar thri tisRheum 1993;36:365-71.
76 Co hen Tervaert JW, Huitema MG, Hene RJ, SluiterWJ, The TH, Van der Hem GK, et al. Pre ven tion of re -lapses in Wegener¢s granulomatosis by treat mentbased on antineutrophil cy to plas mic an ti body ti tre.Lan cet 1990;336:709:11.
77 Han KW, Choi KH, Roth MR, McCloskey TR, Niles LJ.Se rial ANCA titers: use ful tool for pre ven tion of re -lapses in ANCA-as so ci ated vasculitis. Kid ney Int2003;63:1079-85.
78 Gas kin G, Sav age COS, Jones RS, Rees AJ, Lock woodCM, Pusey CD. Anti-neutrophil cy to plas mic an ti bod -ies and dis ease ac tiv ity dur ing long-term fol low-up of70 pa tients with sys temic vasculitis. Nephrol DialTrans plant 1991;6:689-94.
79 Stegeman CA, Co hen Terveart JW, Man son WL,Kallenberg CGM. Chronic na sal car riage of Staph y lo -coc cus aureus in Wegener¢s granulomatosis: iden ti fi -ca tion of a sub group more prone to re lapses. Ann In -tern Med 1994;120:12-7.
80 Boomsma MM, Stegeman CA, van der Leij MJ, OostW, Hermans J, Kallenberg CGM, et al. Pre dic tion ofre lapses in Wegener`s granulomatosis by measur -rement of antineutrophil cy to plas mic an ti body lev els.A pro spec tive study. Ar thri tis Rheum 2000;43:2025-33.
81 Gi rard T, Mahr A, Noel L-H, Cordier J-F, Lesavre P,An dre M-H, et al. Are antineutrophil cy to plas mic an ti -bod ies a marker pre dic tive of re lapse in Wegener`sgranulomatosis? A pro spec tive study. Rheumatology2001;40:147-51.
82 Jennette JC, Falk RJ, Andrassy K, Ba con BA, Churg J,Gross WL, et al. No men cla ture of sys temicvasculitides: the pro posal of an In ter na tional Con sen -sus Con fer ence. Ar thri tis Rheum 1994;37:187-92.
83 Guillevin L, Visser H, Noel LH, Pourrat J, Ver nier I,Gayaraud M, et al. Antineutrophil cy to plasm an ti bod -ies in sys temic polyarteritis nodosa with and with outhep a ti tis B vi rus in fec tion and Churg-Strauss syn -drome – 62 pa tients. J Rheumatol 1993;20:1345-9.
308 ACTA DERMATOVENEROLOGICA CROATICA
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313

84 Haushild S, Csernok E, Schmitt WH, Gross WL.Antineutrophil cy to plas mic an ti bod ies in sys temicpolyarteritis nodosa with and with out hep a ti tis B vi rus in fec tion and Churg-Strauss syn drome. J Rheumatol1994;21:1173-4.
85 Pettersen E, Heigl Z. Anti-neutrophil cy to plas mic an ti -body (c-ANCA and p-ANCA) titers in re la tion to dis -ease ac tiv ity in pa tients with necrotizing vasculitis. Alon gi tu di nal study. Clin Nephrol 1992;37:219-28.
86 Zhao MH, Jones SJ, Lock wood CM. Bac te ri cidal/per -me abil ity-in creas ing pro tein (BPI) is an im por tant an ti -gen for anti-neutrophil cy to plasm autoantibodies(ANCA) in vasculitis. Clin Exp Immunol 1996;99:49-56.
87 Co hen Tervaert JW, Goldschmeding R, Elema JD, vander Giessen M, Huitema MG, van der Hem GK, et al.Autoantibodies against myeloid lysosomal en zymesin cres cen tic glomerulonephritis. Kid ney Int 1990;37:789-806.
88 Co hen Tervaert JW, Goldschmeding R, Von DemBorne AEGKR, Kallenberg CGM. Anti-myeloperoxi -dase an ti bod ies in the Churg-Strauss syn drome. Tho -rax 1991;46:70-1.
89 Co hen Tervaert JW, Kallenberg CGM. Anti-myelo -pero xidase an ti bod ies in Churg-Strauss syn drome. JNeurol 1993;240:449-52.
90 Guillevin L, Co hen P, Gayraud M, Lhote F, JarrousseB, Casassus P. Churg Strauss syn drome: clin i cal studyand long-term fol low-up of 96 pa tients. Med i cine(Bal ti more) 1999;78:26-37.
91 Van der Wall Bake AWL, Lobatto S, Jonges L, DahaMR, Van Es LA. IgA an ti bod ies di rected against cy to -plas mic an ti gens of polymorphonuclear leu ko cytes in pa tients with Henoch-Schönlein purpura. Adv ExpMed Biol 1987;216:1593-8.
92 Saulsbury FT, Kirkpatrick PR, Bolton WK. IgAantineutrophil cy to plas mic an ti body in Henoch- Schönlein purpura. Am J Nephrol 1991;11:295-300.
93 Ronda N, Esnault VLM, Layward L, Allen VSA,Feehally J, Lock wood CM. Antineutrophil cy to plasman ti bod ies (ANCA) of IgA isotype in adultHenoch-Schönlein purpura. Clin Exp Immunol1994;95:49-55.
94 Robson WL, Leung AK, Wood man RC. The ab senceof antineutrophil cy to plas mic an ti bod ies in pa tientswith Henoch-Schönlein purpura. Pediatr Nephrol1994;8:295-8.
95 Guzman J, Fung M, Petty RE. Di ag nos tic value ofantineutrophil cy to plas mic and anti-en do the lial cellan ti bod ies in early Kawasaki dis ease. J Pediatr 1994;124:917-20.
96 Nash MC, Shah V, Reader JA, Dillon MJ.Anti-neutrophil cy to plas mic an ti bod ies and anti-en -do the lial cell an ti bod ies are not in creased inKawasaki dis ease. Br J Rheumatol 1995;34:882-7.
97 Baranger TA, Audrain MA, Castagne A, Bar rier JH,Esnault VL. Ab sence of antineutrophil cy to plas mic an -ti bod ies in gi ant cell arteritis. J Rheumatol 1994;21:871-3.
98 Eichorn J, Sima D, Thiele B, Lindschau C, Turowski A,Schmidt H, et al. Anti-en do the lial cell an ti bod ies inTakayasu arteritis. Cir cu la tion 1996;94:2396-401.
99 Savige JA, Gallicchio MC, Stock man A, CunninghamTJ, Rowley MJ, Georgiou T. Anti-neutrophil cy to -
plasm an ti bod ies in rheu ma toid ar thri tis. Clin ExpImmunol 1991;86:92-8.
100 Mulder AH, Horst G, Van Leeuwen MA, Lim burg PC,Kallenberg CGM. Antineutrophil cy to plas mic an ti bod -ies in rheu ma toid ar thri tis: char ac ter iza tion and clin i cal cor re la tions. Ar thri tis Rheum 1993;36:1054-60.
101 Rother E, Schochat T, Pe ter HH. Antineutrophil cy to -plas mic an ti bod ies (ANCA) in rheu ma toid ar thri tis: apro spec tive study. Rheumatol Int 1996;15:231-7.
102 Mustila A, Korpela M, Mustonen J, Helin H, HuhtalaH, Soppi E, Pasrenack A, Miettinen A. Perinuclearantineutrophil cy to plas mic an ti body in rheu ma toidar thri tis: a marker of se vere dis ease with as so ci atednephropathy. Ar thri tis Rheum 1997;40:710-7.
103 Cam bridge G, Wil liams M, Leaker B, Corbett M,Smith CR. Anti-myeloperoxidase an ti bod ies in pa -tients with rheu ma toid ar thri tis: prev a lence, clin i calcor re lates and IgG sub class. Ann Rheum Dis 1994;53: 24-9.
104 Braun MG, Csernok E, Schmitt WH, Gross WL. In ci -dence, tar get an ti gens and clin i cal im pli ca tions ofantineutrophil cy to plas mic an ti bod ies in rheu ma toidar thri tis. J Rheumatol 1996;23:826-30.
105 Nassberger L, Sjoholm AG, Jonsson H, Strufelt G,Akessen A. Autoantibodies against neutrophil cy to -plasm com po nents in sys temic lupus erythematosusand in hydralazine-in duced lupus. Clin Exp Immunol1990;81:380-3.
106 Schnabel A, Csernok E, Isenberg DA, Mrowka C,Gross WL. Antineutrophil cy to plas mic an ti bod ies insys temic lupus erythematosus. Prev a lence, specifici -ties and clin i cal sig nif i cance. Ar thri tis Rheum 1995;38:633-7.
107 Galeazzi M, Morozzi G, Sebastiani GD, Bellisai F,Marcolongo R, Cervera R, et al. Anti-neutrophil cy to -plas mic an ti body in 566 Eu ro pean pa tients with sys -temic lupus erythematosus: prev a lence, clin i cal as so -ci a tions and cor re la tion with other autoantibodies.Eu ro pean Con certed Ac tion on the Immunogeneticsof SLE. Clin Exp Rheumatol 1998;16:541-6.
108 Mer kel PA, Polisson RP, Chang Y, Skates SJ, Niles JL.Prev a lence of antineutrophil cy to plas mic an ti bod iesin a large in cep tion co hort of pa tients with con nec tive tis sue dis ease. Ann In tern Med 1997;126:866-73.
109 Mulder L, Van Rossum M, Horst G, Lim burg P,deGraeff-Meeder ER, Kuis W, et al. Antineutrophil cy -to plas mic an ti bod ies in ju ve nile chronic ar thri tis. JRheumatol 1997;24:568-75.
110 Helsboot J, Virgo S, McGuigan L, Sturgess A.Antineutrophil cy to plas mic an ti bod ies in in flam ma -tory ar thri tis – po ten tial for misdiagnosis. Br JRheumatol 1995;34:820-4.
111 Locht H, Peen E, Skogh T. Antineutrophil cy to plas mic an ti bod ies in re ac tive ar thri tis. J Rheumatol 1995;25:2304-6.
112 Papo T, Piette JC, Du LTH, Godeau P, Meyeer O,Kahn MF, et al. Antineutrophil cy to plas mic an ti bod ies in polychondritis. Ann Rheum Dis 1993;52:384-5.
113 Handrock K, Gross WL. Re laps ing polychondritis as asec ond ary phe nom e non of pri mary sys temicvasculitis. Ann Rheum Dis 1993;52:895-6.
114 Akimoto S, Ishikawa O, Tamura T, Miyachi Y.Antineutrophil cy to plas mic autoantibodies in pa tients with sys temic scle ro sis. Br J Dermatol 1996;134:407-10.
ACTA DERMATOVENEROLOGICA CROATICA 309
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313

115 Locke IC, Worrall JG, Leaker B, Black CM, Cam bridge G. Autoantibodies to myeloperoxidase in sys temicscle ro sis. J Rheumatol 1997;24:86-9.
116 Sen D, Isenberg AD. Antineutrophil cy to plas micautoantibodies in sys temic lupus erythematosus.Lupus 2003;12:651-8.
117 Saxon A, Shanahan F, Land ers C, Ganz R, Targan S. Adis tinct sub set of antineutrophil cy to plas mic an ti bod -ies is as so ci ated with in flam ma tory bowel dis ease. JAl lergy Clin Immunol 1990;86:202-10.
118 Rump JA, Scholmerich J, Gross V, Roth M, Helfes -rieder R, Rautman A, et al. A new type of peri nuclearanti-neutrophil cy to plas mic an ti body (p-ANCA) in ac -tive ul cer ative but not in Crohn¢s dis ease. Immuno -biology 1991;181:406-13.
119 Mulder AHL, Broekroelfors J, Horst G, Lim burg PC,Nelis GF, Kallenberg CGM. Anti-neutrophil cy to plas -mic an ti bod ies (ANCA) in in flam ma tory bowel dis -ease: char ac ter iza tion and clin i cal cor re lates. Clin Exp Immunol 1994;95:490-7.
120 Smetana-Škurla M, Krstuloviæ A, Ostojiæ R, KrznariæŽ, Rudolf M, Vuceliæ B, et al. Antineutrophil cy to plas -mic an ti bod ies (ANCA) in in flam ma tory bowel dis -ease (IBD): prev a lence and di ag nos tic role. Pe riodBiol 1998;100:489-94.
121 Duerr RH, Targan SR, Land ers CJ, LaRusso NF,Lindsay KL, Wiesner RH, et al. Neutrophil cy to plas -mic an ti bod ies: a link be tween pri mary sclerosingcholangitis and ul cer ative co li tis. Gastroenterology1991;100:1385-91.
122 Targan SR, Land ers C, Vidrich A, Czaja AJ. High-ti terantineutrophil cy to plas mic an ti bod ies in type-1 au to im -mune hep a ti tis. Gastroenterology 1995;108:1159-66.
123 Hertervig E, Wieslander J, Johansson C, Wiik A,Nilsson A. Anti-neutrophil cy to plas mic an ti bod ies inchronic in flam ma tory bowel dis ease: prev a lence anddi ag nos tic role. Scand J Gastroenterol 1995;30:693-8.
124 Free man H, Roeck B, Devine D, Carter C. Pro spec tive eval u a tion of neutrophil cy to plas mic autoantibodiesin 500 con sec u tive pa tients with in flam ma tory boweldis ease. Can J Gastroenterol 1997;11:203-7.
125 Krstuloviæ A, Krznariæ Ž, Rudolf M, Ostojiæ R, VuceliæB, Malenica B. Prev a lence of antineutrophil cy to plas -mic an ti bod ies (ANCA) in au to im mune hep a ti tis.Farm Vestn 1998;49:425-31.
126 Walmsley RS, Zhao RH, Ham il ton MI, Brownlee A,Chap man P, Pounder RE, et al. Antineutrophil cy to -plas mic autoantibodies against bac te ri cidal/per me -abil ity-in creas ing pro tein in in flam ma tory bowel dis -ease. Gut 1997;40:105-9.
127 Malenica B, Kozmar A, Ostojiæ R, Krznariæ Ž, VuceliæB. Antineutrophil cy to plas mic an ti bod ies (ANCA) inin flam ma tory bowel dis eases: char ac ter iza tion of an ti -genic specificities (Ab stract). J Autoimmunity 1999;(Suppl):81.
128 Kozmar A, Vuceliæ B, Ostojiæ R, Krznariæ Ž, MalenicaB. Antineutrophil cy to plas mic an ti bod ies (ANCA) inpa tients with au to im mune hep a ti tis (Ab stract). JAutoimmun 1999; (Suppl):79.
129 Abad E, Tural C, Mirapeix E, Cuxart A. Re la tion shipbe tween ANCA and clin i cal ac tiv ity in in flam ma torybowel dis ease: vari a tion in prev a lence of ANCA andev i dence of het er o ge ne ity. J Autoimmun 1997;10:175-80.
130 Vasiliauskas EA, Plevy SC, Land ers CJ, Binder SW,Fer gu son DM, Yang H, et al. Perinuclear antineutro -phil cy to plas mic an ti bod ies in pa tients with Crohn¢sdis ease de fine a clin i cal sub group. Gastro enterology1996;110:1810-9.
131 Sandborn WJ, Land ers CJ, Tremaine WJ, Targan SR.As so ci a tion of antineutrophil cy to plas mic an ti bod ieswith re sis tance to treat ment of left-sided ul cer ative co -li tis: re sults of a pi lot study. Mayo Clin Proc 1996;71:431-6.
132 Aitola P, Miettinen A, Mattila A, Matikainen M, SoppiE. Ef fect of proctocolectomy on se rum antineutrophilcy to plas mic an ti bod ies in pa tients with chronic ul cer -ative co li tis. J Clin Pathol 1995;48:645-7.
133 Sandborn WJ, Land ers CJ, Tremaine WJ, Targan SR.Antineutrophil cy to plas mic an ti body cor re lates withchronic pouchitis af ter ileal pouch-anal anas to mo sis.Am J Gastroenterol 1995;90:740-7.
134 Gur H, Shen G, Sutjita M, Terrberry J, Alosachie I,Barka N, et al. Autoantibody pro file in pri marysclerosing cholangitis. Pathobiology 1995;63:76-82.
135 Zauli D, Ghetti S, Grassi A, Descovich C, Cassani F,Ballardini G, et al. Anti-neutrophil cy to plas mic an ti -bod ies in type 1 and 2 au to im mune hep a ti tis. Hepa -tology 1997;25:1105-7.
136 Malenica B, Krstuloviæ A, Ostojiæ R, Vuceliæ B, Batiniæ D. Prev a lence of antineutrophil cy to plas mic an ti body (ANCA) in pa tients with au to im mune hep a ti tis (Ab -stract). Immunol Lett 1997;36:480.
137 Klassen RJL, Goldschmeding R, Dolman KM, VlekkeABJ, Weigl HM, Eeftinck Schattenkerk JKM, et al.Anti-neutrophil cy to plas mic autoantibodies in pa -tients with symp tom atic HIV in fec tion. Clin ExpImmunol 1992;87:24-30.
138 Savige JA, Chang L, Horn S, Crowe SM. Anti-nu clear,anti-neutrophil cy to plas mic and anti-glo mer u lar base -ment mem brane an ti bod ies in HIV-in fected in di vid u -als. Autoimmunity 1994;18:205-11.
139 Efthiniou J, Spickett G, Lane D, Thomp son A. Anti- neutrophil cy to plas mic an ti bod ies, cys tic fi bro sis andin fec tion. Lan cet 1991;337:1037-8.
140 Dav en port A, Lock RJ, Walling ton TB. Clin i cal rel e -vance of test ing for antineutrophil cy to plasm an ti bod -ies (ANCA) with a stan dard in di rect immuno fluores -cence ANCA test in pa tients with up per or lower re -spi ra tory tract symp toms. Tho rax 1994;49:213-7.
141 Galperin C, Shoenfeld Y, Gilburd B, Esterre P, MeroniPL, Del Papa N, et al. Anti-neutrophil cy to plas mic an -ti bod ies in pa tients with chromomycosis. Clin ExpRheumatol 1996;14:479-83.
142 Wenisch C, Wenisch H, Bankl H-C, Exner M,Graninger W, Looareesuwan S, et al. De tec tion ofanti-neutrophil cy to plas mic an ti bod ies af ter acutePlasmodium falciparum ma laria. Clin Diagn LabImmunol 1996;3:132-4.
143 Pudifin DJ, Duursma J, Gathiram V, Jack son TFHG. In -va sive amoebiasis is as so ci ated with the de vel op mentof anti-neutrophil cy to plas mic an ti body. Clin ExpImmunol 1994;97:48-51.
144 Cho CD, Asuncion A, Tatum AH. False-pos i tiveantineutrophil cy to plas mic an ti body in aspergillosiswith oxalosis. Arch Pathol Lab Med 1995;119:558-61.
145 Dav en port A. “False pos i tive” perinuclear and cy to -plas mic antineutrophil cy to plas mic an ti body re sults
310 ACTA DERMATOVENEROLOGICA CROATICA
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313

lead ing to misdiagnosis of Wegener¢s granulomatosisand/or mi cro scopic polyarteritis. Clin Nephrol 1992;37:124-30.
146 Zhao MH, Jayne DR, Ardiles LG, Culley F, HodsonME, Lock wood CM. Autoantibodies against bac te ri -cidal/per me abil ity-in creas ing pro tein in pa tients withcys tic fi bro sis. Q J Med 1996;89:259-65.
147 Al bert LJ, Inman RD. Mo lec u lar mim icry and auto -immunity. N Engl J Med 1999;341:2068-74.
148 Croft J, Fatenejad S. Self an ti gens and epitope spread -ing in sys temic autoimmunity. Ar thri tis Rheum 1997;40:1274-82.
149 Vanderlugt CJ, Miller SD. Epitope spread ing. CurrOpin Immunol 1996;8:831-6.
150 Nassberger L, Sjoholm AG, Jonsson H, Sturfelt G,Akesson A. Autoantibodies against neutrophil cy to -plasm com po nents in sys temic lupus erythematosusand in hydralazine-in duced lupus. Clin Exp Immunol1990;81:380-3.
151 Jones BF, Ma jor GAC. Cres cen tic glomerulonephritisin a pa tient tak ing penicillamine as so ci ated withantineutrophil cy to plas mic an ti body. Clin Nephrol1992;38:293.
152 Dolman KM, Gans ROB, Vervaat TJ, Zevenbergen G,Maingay D, Nikkels RE, et al. Vasculitis and anti -neutrophil cy to plas mic autoantibodies as so ci ated withpropylthiouracil ther apy. Lan cet 1993;342:651-2.
153 Vogt BA, Kim Y, Jennette JC, Falk RJ, Burke BA,Sinaiko A. Antineutrophil cy to plas mic autoantibody- pos i tive cres cen tic glomerulonephritis as a com pli ca -tion of treat ment with propylthiouracil in chil dren. JPediatr 1994;124:986-8.
154 Kawachi Y, Nukaga H, Hoshino M, Iwata M, OtsukaF. ANCA-as so ci ated vasculitis and lupus-like syn -drome caused by methimazole. Clin Exp Dermatol1995;20:345-7.
155 Short AK, Lock wood CM. An ti gen spec i fic ity inhydralazine as so ci ated ANCA pos i tive sys temicvasculitis. Q J Med 1995;88:775-83.
156 Eklayam O, Yaron M, Caspi D. Minocycline in ducedar thri tis as so ci ated with fe ver, livedo reticularis andpANCA. Ann Rheum Dis 1996;55:766-71.
157 Tanemoto M, Miyakawa H, Hanai J, Yago M, KitaokaM, Uchida S. Myeloperoxidase-antineutrophil cy to -plas mic an ti body-pos i tive cres cen tic glomerulo nep -hri tis com pli cat ing the course of Graves¢ dis ease: re -port of three adult cases. Am J Kid ney Dis 1995;26:774-80.
158 D¢Cruz D, Chesser AMS, Lightowler C, Comer M,Hurst MJ, Baker LRI, et al. Antineutrophil cy to plas mican ti body-pos i tive cres cen tic glomerulonephritis as so -ci ated with anti-thy roid drug treat ment. Br JRheumatol 1995;34:1090-1.
159 Kitahara T, Hiromura K, Maezawa A, Ono K,Narabara N, Yano S, et al. Case of propylthiouracil-in -duced vasculitis as so ci ated with anti-neutrophil cy to -plas mic an ti body (ANCA): re view of lit er a ture. ClinNephrol 1997;47:336-40.
160 Choi HK, Mer kel PA, Walker AM, Niles JL. Drug as so -ci ated antineutrophil cy to plas mic an ti body/pos i tivevasculitis, prev a lence among pa tients with high titersof antimyeloperoxidase an ti bod ies. Ar thri tis Rheum2000;43:405-13.
161 Walsh JS, Gross DJ. Wegener¢s granulomatosis in volv -ing the skin. Cutis 1999;64:183-6.
162 Gib son EL. Cu ta ne ous vasculitis up date. DermatolClin 2001;19:603-15.
163 Gib son EL, Specks U, Homburger H. Clin i cal util ity of ANCA tests for the der ma tol o gist. Int J Dermatol2003;42:859-69.
164 Daouk R, Palsson R, Arnaout AM. In hi bi tion ofproteinase 3 by ANCA and its cor re la tion with dis ease ac tiv ity in Wegener’s granulomatosis. Kid ney Int1995;47:1528-36.
165 Van de Wiel, BA, Dollman KM, van der Meer- Gerritsen CH, Nack CE, von dem Borne AEGK,Goldschmeding R. In ter fer ence of Wegener’s granu -lomatosis autoantibodies with neutrophil proteinase 3 ac tiv ity. Clin Exp Med 1992;90:409-14.
166 Dolman KM, Stegeman CA, Van de Wiel BA, HackCE, Von dem Borne AEGK, Kallenberg CGM,Goldschmeding R. Rel e vance of clas sic anti-neutro -phil cy to plas mic autoantibody (c-ANCA)-me di ated in -hi bi tion of proteinase 3-alfa 1-antitrypsin complexa -tion to dis ease ac tiv ity in Wegener¢s granulomatosis.Clin Exp Immunol 1993;93:405-10.
167 Grif fin SV, Chap man PT, Lianos EA, Lock wood CM.The in hi bi tion of myeloperoxidase by ceruloplasmincan be re versed by anti-myeloperoxidase an ti bod ies.Kid ney Int 1999;55:917-25.
168 Elzouki A-N, Segelmark M, Weislander J, Erikson S.Strong link be tween the al pha-1-antitrypsin PiZ al leleand Wegener¢s granulomatosis. J In tern Med 1994;236:543-8.
169 Esnault LV, Andrian AM, Sesbone R. Al pha-1-anti -trypsin phenotyping in ANCA-as so ci ated diaseases:one of sev eral ar gu ments for pro te ase/antiprotease im -bal ance in sys temic vasculitis. Exp Clin Immunogenet1997;14:206-13.
170 Grif fith M, Lovegrove J, Gas kin G, Witehouse D,Pusey C. C-ANCA anti-neutrophil cy to plas mic an ti -body positivity in vasculitis pa tients is as so ci ated withthe Y al lele of al pha-1-antitrypsin, and p-antineu -trophil cy to plas mic an ti body positivity with the S al -lele. Nephrol Dial Trans plant 1996;11:438-43.
171 Mayet WJ, Hermann E, Csernok E, Knuth A, Poralla T,Gross WL, et al. A hu man re nal can cer cell line as anew an ti gen source for the de tec tion of an ti bod ies tocy to plas mic and nu clear an ti gens in sera of pa tientswith Wegener¢s granulomatosis. J Immunol Meth ods1991;143:57-64.
172 Mayet WJ, Csernok E, Szymkowiak C, Gross WL,Meyer zum Buschenfelde KM. Hu man en do the lialcells ex press proteinase 3, the tar get an ti gen of anti- cy to plas mic an ti bod ies in Wegener¢s granulomatosis.Blood 1993;82:1221-9.
173 Brandt M de, Meyer O, Dacosta L, Elbim C, PasquierC. Anti-proteinase 3 (PR3) an ti bod ies (cANCA) rec og -nize var i ous tar gets on the hu man um bil i cal en do the -lial cell (HUVEC) mem brane. Clin Exp Immunol1999;115:362-8.
174 Ballieux BE, Zondervan KT, Kievit P, Hagen EC, Es LA, van der Woude FJ, et al. Bind ing of proteinase 3 andmyeloperoxidase to en do the lial cells in duceANCA-me di ated en do the lial dam age through ADCC.Clin Exp Immunol 1994;97:52-60.
175 Berger SP, Seelen MA, Hiemstra PS, Gerritsma JSJ,Heemskerk E, van der Woude, et al. Proteinase 3, thema jor autoantigen of Wegener¢s granulomatosis, en -hances IL-8 pro duc tion by en do the lial cells in vi tro. JAm Soc Nephrol 1996,7:694-701.
ACTA DERMATOVENEROLOGICA CROATICA 311
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313

176 Ballieux BEPB, Hiemstra PS, Klar-Mohamad N, Hagen EC, van Es LA, van der Woude FJ, et al. De tach mentand cytolysis of hu man en do the lial cells by proteinase 3. Eur J Immunol 1994;24:3211-5.
177 Yang JJ, Kettritiz R, Falk RJ, Jennette JC, Gaido ML.Apoptosis of en do the lial cells in duced by theneutrophil serine pro teas es, proteinase 3 and elastase. Am J Pathol 1996;149:1617-26.
178 Csernok E, Ernst M, Schmitt W, Bainton DF, GrossWL. Ac ti vated neu tro phils ex press proteinase 3 ontheir plasma mem brane in vi tro and in vivo. Clin ExpImmunol 1994;95:244-50.
179 Gilligan H, Brady B, Brady H, Hebert MJ, Slayter HS,Xu Y, et al. Antineutrophil cy to plas mic auto anti bo -dies in ter act with pri mary gran ule con stit u ents on thesur face of apoptotic neu tro phils in the ab sence ofneutrophil prim ing. J Exp Med 1996;184:2231-41.
180 Reumaux D, DeBoer M, Meijer AB, Duthilleul P,Roos D. Ex pres sion of myeloperoxidase (MPO) byneu tro phils is nec es sary for their ac ti va tion by anti- neutrophil cy to plasm autoantibodies (ANCA) againstMPO. J Leukoc Biol 2003;73:841-6.
181 Falk RJ, Terrell RS, Charles LA, Jennette JC. Anti- neu -trophil cy to plas mic autoantibodies in duce neu tro -phils to degranulate and pro duce ox y gen rad i cals invi tro. Proc Natl Acad Sci USA 1990;87:4115-9.
182 Brouwer E, Huitema MG, Mulder AHL, Heeringa P,Van Goor H, Co hen Tervaert JW, et al. Neutrophil ac -ti va tion in vi tro and in vivo in Wegener¢s granulo -matosis. Kid ney Int 1994;45:1121-31.
183 Evert BH, Jennette JC, Falk RJ. Anti-myeloperoxidasean ti bod ies stim u late neu tro phils to dam age hu manen do the lial cells. Kid ney Int 1992;41:375-83.
184 Sav age COS, Pottinger BE, Gas kin G, Pusey CD,Pearson JD. Autonatibodies de vel op ing to myelope -ro xidase and proteinase 3 in sys temic vasculitis stim u -late neutrophil cytotoxicity to wards cul tured en do the -lial cells. Am J Pathol 1992;141:335-42.
185 Griminger F, Hattr K, Papavassilis C, Temmesfeld B,Csernok E, Gross WL. Neutrophil ac ti va tion by anti- pro te inase 3 an ti bod ies in Wegener’s granulomatosis: role of arachidonic acid and leukotriene B4 gen er a -tion. J Exp Med 1996;184:1567-72.
186 Brooks CJ, King WJ, Radford DJ, Adu D, McGrath M,Sav age COS. IL-1 beta pro duc tion by hu man polymorphonuclear leu ko cytes stim u lated by anti-neutro -phil cy to plas mic autoantibodies – rel e vance to sys -temic vasculitis. Clin Exp Immunol 1996;106:273-9.
187 Keogan MT, Rifkin I, Ronda N, Lock wood CM, Brown DL. Antineutrophil cy to plasm an ti bod ies in creaseneutrophil ad he sion to cul tured hu man en do the lium.Adv Exp Med Biol 1993;336:115-9.
188 Jonhnson PA, Al ex an der HD, Mc Millan SA, MaxwellAP. Upregulation of the granu lo cytes ad he sion mol e -cule Mac-1 by autoantibodies in au to im munevasculitis. Clin Exp Immunol 1997,107:513-9.
189 Mulder AHL, Heeringa P, Brouwer E, Lim burg PC,Kallenberg CGM. Ac ti va tion of granu lo cytes byanti-neutrophil cy to plas mic an ti bod ies (ANCA): a FcgamaRII-de pend ent pro cess. Clin Exp Immunol1994;98:270-8.
190 Porges AJ, Redecha PB, Kimberly WT, Csernok E,Gross WL, Kimberly RP. Anti-neutrophil cy to plas mican ti bod ies en gage and ac ti vate hu man neu tro phils via FcgamaRIIa. J Immunol 1994;153:1271-80.
191 Reumaux D, Vossebeld PJM, Roos D, Verhoeven AJ.Ef fect of tu mor ne cro sis fac tor-in duced integrin ac ti va -tion on Fc gamma re cep tor II-me di ated sig nal trans -duction: rel e vance for ac ti va tion of neu tro phils byanti-proteinase 3 or anti-myeloperoxidase an ti bod ies.Blood 1995;86:3189-95.
192 Weidner S, Neupart W, Goppelt-Struebe M, Ruprecht DH. Antineutrophil cy to plas mic an ti bod ies in ducehu man monocytes to pro duce ox y gen rad i cals in vi -tro. Ar thri tis Rheum 2001;44:1698-706.
193 Ralston DR, Marsh CB, Lowe MP, Wewers MD.Antineutrophil cy to plas mic an ti bod ies in duce mono -cyte IL-8 re lease. Role of sur face proteinase 3, al pha/1antitrypsin and Fc gamma re cep tors. J Clin In vest1997;100:1416-24.
194 Casselman B, Kilgore K, Miller B, War ren J. An ti bod -ies to neutrophil cy to plas mic an ti gens in duce mono -cyte chemoattractant pro tein-1 se cre tion from hu manmonocytes. J Lab Clin Med 1995;126:495-502.
195 Mul ler Kobold AC, Kallenberg CGM, Co hen TervaertJW. Monocyte ac ti va tion in pa tients with Wegener’sgranulomatosis. Ann Rheum Dis 1999;58:237-45.
196 Pall AA, Sav age COS. Mech a nisms of en do the lial cellin jury in vasculitis. Springer Sem i nar Immunopathol1994;16:23-37.
197 Ras mus sen N, Petersen J. Cel lu lar im mune re sponsesand pathogenesis in c-ANCA pos i tive vasculitides. JAutoimmun 1993;6:227-36.
198 Kallenberg CGM, Co hen Terveart JW, van derWoude FJ, Goldschmeding R, von dem BorneAEGKR, Ween ing JJ. Autoimmunity to lysosomal en -zymes: new clues to vasculitis and glomerulone -phritis? Immunol To day 1991;12:61-4.
199 Mathieson PW, Oliveira DBG. The role of cel lu lar im -mu nity in sys temic vasculitis. Clin Exp Immunol1995;100:183-5.
200 Ballieux BEPB, Van Der Burg SH, Hagen EC, Van DerWoude FJ, Melief CJM, Van Es LA, Daha MR. Cell-me -di ated autoimmunity in pa tients with Wegener´sgranulomatosis. Clin Exp Immunol 1995;100:186-93.
201 Giscombe R, Grunewald J, Nityanand S, Lefvert AK. Tcell (TCR) V gene us age in pa tients with sys temicnecrotizing vasculitis. Clin Exp Immunol 1995;101:213-9.
202 Cid MC, Grau JM, Casademont J, Cam po E, Coil- Vinent B, Lopez-Soto A, et al. Immuno histo chemicalchar ac ter iza tion of in flam ma tory cells and im mu no -logic ac ti va tion mark ers in mus cle and nerve bi opsyspec i mens from pa tients with sys temic poly arte ritisnodosa. Ar thri tis Rheum 1994;37:1055-61.
203 Seko JY, Minota S, Kiwasaki A, Shinkai Y, Maeda K,Yagita H, et al. Perforin-se cret ing killer cell in fil tra tion and ex pres sion of a 65-kD heat-shock pro tein in aor tic tis sue of pa tients with Takayasu¢s arteritis. Clin In vest1994;93:750-8.
204 Stegeman CA, Co hen Tervaert JW, Huitema MG,Kallenberg CGM. Se rum mark ers of T-cell ac ti va tionin re lapse of Wegener¢s granulomatosis. Clin ExpImmunol 1993;91:415-20.
205 Schmitt WH, Heesen C, Csernok E, Gross WL. El e -vated se rum level of sol u ble interleukin-2-re cep tor(sIL-2R) in Wegener¢s granulomatosis. Ar thri tis Rheum1992;35:108-12.
206 Petersen J, Ras mus sen N, Szpirt W, Hermann E,Mayet W. T lym pho cyte pro lif er a tion to neutrophil
312 ACTA DERMATOVENEROLOGICA CROATICA
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313
cy to plas mic an ti gen(s) in Wegener¢s granulomatosis.Am J Kid ney Dis 1991;18:205.
207 Brouwer E, Stegeman CA, Huitema MG, Lim burg PC,Kallenberg CGM. T-cell re ac tiv ity to proteinase 3 andmyeloperoxidase in pa tients with Wegener¢s granu -lomatosis. Clin Exp Immunol 1994;98:448-53.
208 Grif fith ME, Coulthart A, Pusey CD. T cell re sponsesto myeloperoxidase (MPO) and proteinase 3 (PR3) inpa tients with sysstemic vasculitis. Clin Exp Immunol1996;103:253-8.
209 Papa ER, Franssen CF, Lim burg PC, Huitema MG,Kallenberg CGM, Co hen Tervaert JW. In vi tro cyto -kine pro duc tion and pro lif er a tion of T cells from pa -tients with anti-proteinase 3 and antimyelo peroxi da -se- as so ci ated vasculitis in re sponse to proteinase 3and myeloperoxidase. Ar thri tis Rheum 2002;46:1894-904.
210 Patry YC, Trewick CD, Gregoire M, Audrian MA,Moreau AM, Mul ler JY, et al. Rats in jected with sy -ngeneic rat apoptotic neu tro phils de vel oped antineu -trophil cy to plas mic an ti bod ies. J Am Soc Nephrol2001;12:1764-8.
211 Aveskogh M, Lützelschwab C, Huang MR, Hellman L. Char ac ter iza tion of cDNA clones en cod ing mouseproteinase 3 (myeloblastin) and cathepsin G. Immu -no genetics 1997;46:181-91.
212 Tomer Y, Gilburd B, Blank M, Lider O, Hershkoviz R,Fishman P, et al. Char ac ter iza tion of bi o log i cally ac -tive antineutrophil cy to plas mic an ti bod ies in duced inmice. Ar thri tis Rheum 1995;38:1375-81.
213 Blank M, Tomer Y, Stein M, Kopoloviæ J, Wiik A,Meroni PL, et al. Im mu ni za tion with anti-neutrophilcy to plas mic an ti body (ANCA) in duces the pro duc tion of mouse ANCA and perivascular lym pho cyte in fil tra -tion. Clin Exp Immunol 1995;102:120-30.
214 Druet P, Pelletier L, Hirsch F, Rossert J, Pasquier R,Druet E, et al. Mer cury-in duced au to im mune glome -rulonephritis in an i mals. Contrib Nephrol 1988;61:120-30.
215 Hirsh F, Couderc J, Sapin C, Fournie G, Druet P.Polyclonal ef fect of HgCl2 in the rat, its pos si ble rolein ex per i men tal au to im mune dis ease. Eur J Immunol1982;12:620-5.
217 Aten J, Veninga A, Coers W, Sonnenberg A, Timpl R,Claessen N, et al. Autoantibodies to the laminin P1frag ment in HgCl2-in duced mem bra nous glomerulo -pathy. Am J Pathol 1995;146:1467-80.
218 Esnault VLM, Mathieson PW, Thiru S, Oliviera DB,Lock wood CM. Autoantibodies to myeloperoxidasein Brown Nor way rats treated with mer cu ric chlo ride.Lab In vest 1992;67:114-20.
219 Mathieson PW, Thiru S, Oliviera DBG. Mer cu ricchlo ride treated Brown Nor way rats de velop wide -spread tis sue in jury in clud ing necrotizing vasculitis.Lab In vest 1992;67:121-9.
220 Pelletrier L, Pasquier R, Rossert J, Vial MC, Mandet C,Druet P. Autoreactive T cells in mer cury-in ducedauto immunity. J Immunol 1988;140:750-4.
221 Mathieson PW, Thiru S, Oliviera DBG. Reg u la toryrole of 0X22+ T cells in mer cury-in ducedautoimmunity in the Brown Nor way rat. J Exp Med1993;177:114-20.
222 Qasim FJ, Mathieson PW, Thiru S, Oliviera DBG.Cyclosporin A ex ac er bates mer cu ric chlo ride-in -
duced vasculitis in the Brown Nor way rat. Lab In vest1995;72:183-91.
223 Hewicker M, Trautwein G. Se quen tial study ofvasculitis in MRL mice. Lab Anim 1987;21:335-41.
224 Moyer CF, Strandberg DJ, Reinish CL. Sys temic mo -no nuclear cell vasculitis in MRL/lpr mice: a histo -logical and immunocytochemical anal y sis. Am JPathol 1987;127:229-42.
225 Izui S, Eisenberg RA. Cir cu lat ing anti-DNA-rheu ma -toid fac tor com plex in MRL/1 mice. Clin ImmunolPathol 1980;15:536-51.
226 Harper JM, Lock wood CM, Cooke A. Anti-neutrophilcy to plasm an ti body in MRL-lpr/lpr mice. Clin ExpImmunol 1993;93 (Suppl 1):22.
227 Kinjoh K, Good RA, Nemoto K, Falk RJ, Jennette JC.SCG/Kj mice de velop cres cen tic glomerulonephritis(CGN), vasculitis and MPO-spe cific P-ANCA (Ab s -tract). Clin Exp Immunol 1995;101 (Suppl 1):53.
228 Kinjoh K, Good RA, Tay lor J, Nachman P, Falk RJ,Jennette JC. Hybridomas from SCG/j mice pro duceP-ANCA with spec i fic ity for myeloperoxidase (MPO)and in duce proteinuria in nude mice (Ab stract). ClinExp Immunol 1995;101 (Suppl 1):37.
229 Kobayashi K, Shibata T, Sugisaki S. Ag gra va tion of ratnephrotoxic se rum ne phri tis by anti-myeloperoxidase an ti bod ies. Kid ney Int 1995;47:454-63.
230 Brouwer E, Huitema MG, Klok PA, de Weerd H, Co -hen Tervaert JW, Ween ing JJ, et al. Anti-myelo -peroxidase as so ci ated proliferative glomerulonene -phritis: an an i mal model. J Exp Med 1993;177:905-14.
231 Heeringa P, Foucher P, Klok PA, Huitema MG, Co hen Tervaert JW, Ween ing JJ, et al. Sys temic in jec tion ofprod ucts of ac ti vated neu tro phils and H202 inmyeloperoxidase-im mu nized rats leads to necrotizing vasculitis in the lungs and gut. Am J Pathol1997;151:131-9.
232 Heeringa P, Brouwer E, Klok PA, Huitema MG, vanden Born J, Ween ing JJ, et al. Autoantibodies tomyelo peroxidase ag gra vate mild anti-glo mer u lar- ba -se ment-mem brane me di ated glo mer u lar in jury. Am JPathol 1996;149:1695-706.
233 Co hen Tervaert JW, Popa ER, Bos NA. The role ofsuperantigens in vasculitis. Curr Opin Rheumatol1999;11:24-31.
234 Utz PJ, An der son P. Posttranslational pro tein mod i fi -ca tions, apoptosis and the by pass of tol er ance toautoantigens. Ar thri tis Rheum 1998;41:1152-60.
235 Giscombe R, Grunewald J, Nityanand S, Lefvert AK. Tcell re cep tor (TCR) V gene us age in pa tients with sys -temic necrotizing vasculitis. Clin Exp Immunol 1995;101:213-9.
236 Moosig F, Csernok E, Kumanovics G, Gross WL.Opsonization of apoptotic neu tro phils by anti-neutro -phil cy to plas mic an ti bod ies (ANCA) leads to en -hanced up take by macrophages and in creased re lease of tu mour ne cro sis fac tor-al pha (TNF-al pha). Clin ExpImmunol 2000;122:499-503.
237 Gilligan HM, Bredy B, Brady HR, Hebert MJ, SlayterHS, Xu Y, et al. Antineutrophil cy to plas mic autoanti -bodies in ter act with pri mary gran ule con stit u ents onthe sur face of apoptotic neu tro phils in the ab sence ofneutrophil prim ing. J Exp Med 1996;184:2231-41.
ACTA DERMATOVENEROLOGICA CROATICA 313
Malenica et al: Acta Dermatovenerol Croat
ANCA: Di ag nos tic and Patho genic Po ten tial 2004;12(4):294-313