Anticorpi Monoclonali: i risultati delle sperimentazioni ... · Innate and Adaptive immunity in...
63
Anticorpi Monoclonali: i risultati delle sperimentazioni cliniche nel trattamento del Mieloma Multiplo Pellegrino Musto Direzione Scientifica IRCCS, Centro di Riferimento Oncologico della Basilicata Rionero in Vulture – Pz IRCCS CROB
Transcript of Anticorpi Monoclonali: i risultati delle sperimentazioni ... · Innate and Adaptive immunity in...

Anticorpi Monoclonali: i risultati delle sperimentazioni cliniche nel trattamento del Mieloma Multiplo
Pellegrino Musto
Direzione Scientifica
IRCCS, Centro di Riferimento Oncologico della Basilicata
Rionero in Vulture – Pz
IRCCS
CROB

• 1% of cancer
• 10% of hematological malignancies
• 2-4 cases/year/100.000
• Uncurable disease (?)
Multiple myeloma: a malignant proliferation of bone marrow plasma cells
abnormal production of a monoclonal immunoglobulin (M-protein)
Major clinical issues
• Osteolytic bone lesions
• Hypercalcemia
• Anemia
• Renal failure
• Heterogeneous clinical outcome (MGUS, SMM,
symptomatic myeloma, plasma cell leukemia)
• High molecular/genomic heterogeneity

Survival improvement
Myeloma Trialists’ Collaborative Group J Clin
Oncol. 1998;16:3832-42. Usmani SZ, et al. Leukemia. 2013;27:226–32.
Where we come from…
Median age 61 5-year OS with MP: 24%
OS
Years
0 1 2 3 4 6
0
100
40
60
80
20
5
Allocated cct (% ± SD)
Allocated MP (% ± SD)
24.4%
23.0%19.4%
18.0%
1.4% SD 1.4(log-rank)
2p>0.1; NS)
…where we are now
Median age 59 5-year OS with TT3: 73%
OS CR duration
Years
0 6 7 8 9
0
100
40
60
80
20
3 4 51 2
p<0.0001
TT3
TT2 + Thal
TT2 -Thal
TT1
Years
0 6 7 8 9
0
100
40
60
80
20
3 4 51 2
p<0.0001
TT3
TT2 + Thal
TT2 -Thal
TT1

Melfalane prednisone
Alte dosidi Melfalan
VAD
ABMT
Storia della terapia «real world» del mieloma multiplo
Alte dosi diDesametasone
HDT+ASCT
Talidomide
Bisfosfonati
Bortezomibin recidiva
Len-Dex in recidiva
Bortezomib + antraciclinaliposomiale in recidiva
VMP
MPT
VTD ASCT
Talidomide inmantenimento
1962
1983
1986
1996
1999
2003
2005
2008
2009
2011
2012
2014
1984
2013
BortezomibSCRd FDA
Dara FDA
PomaEMEA
2015
MPR-R
RD cont.MPR-RCarlfizomibKRdDara EMEAIxazomibFDA

Significant Advances in Multiple Myeloma Have Been Made in the Last Decade, but…
N=1038 patients with newly diagnosed MM between January 1, 2001 and
December 31, 2010
Patients were grouped into two time intervals based on year of diagnosis (2001–2005 and 2006 –2010) to compare OS rate
5
MM=multiple myeloma; OS=overall survival.
Kumar SK et al. Leukemia. November 15, 2013. doi:10.1038/leu.2013.313Kumar SK, et al. Leukemia. 2012;26:149-157.
The use of thalidomide, lenalidomide, and bortezomib as part of initial therapy has improved overall survival rates
1-year mortality: 8%, median OS NR
1-year mortality: 19%, median OS 3.8 yrs
Follow-up from diagnosis (years)
6543210
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
po
rtio
n s
urv
ivin
g Received novel agents
No novel agents
Poor survival in patients refractory to IMIDs and PIs

Innate and Adaptive immunity in cancer
Innate cells, including Natural Killer Cells, respond rapidly and are the body’s first line of defense against cancer2
Adaptive cells, including T cells and B cells, take longer to develop a tumor antigen-specific immune response2
NK T cell, Natural Killer T cell.1. Dranoff G. Nat Rev Cancer. 2004;4:11-22. 2. Borghaei H et al. Eur J Pharmacol. 2009;625:41-54.

7
Myeloma cells mediate profound immune dysfunctions in tumormicroenvironment leading, in particular, to NK cell suppression
MDSC
Agrawal et al., Exp Rev Clin Immunol 2008 Myeloid-derivedsuppressor cells
NK precursor
T reg
Killing of DC to preventNK cell priming
Immunosuppressivefactors such as IL-
10,TGFb and IDO Soluble
ligandssuch asMICA/B
Reduced NK differentiation
Myeloid-derivedimmunosuppressive factors(ROS, iNOS, O, IDO, TGFb…)

Anti-tumor immune response
Tumor growth
Tumor immunity: a dynamic interaction
Subclinical pre-diagnosis phase Clinical phase
ELIMINATIONof tumor cells
(partial or complete)
EQUILIBRIUMbetween
immune responseand tumor growth
ESCAPEof tumor cells
from immune control
Imm
un
ose
lect
ion
/ed
itin
g

Jelinek et al. Blood Reviews, 2015
Sondergeld et al. Clini Adv Hematol Oncol, 2015

10
Humanization of antibodies to overcome immunogenicity
‘ximab’
Chimeric mouse or rat Ig variable regions; human
constant regions (Rituximab)
’zumab’
Humanized chimeric mAb with only complementarity
determining regions being mouse origin (Bevacizumab,
Elotuzumab)
’umab’
Fully human(Daratumumab)
’momab’
Fully murine(Tositumomab)
Imai & Takaoka. Nature Reviews Cancer 2006; 6: 714-727
Immunogenicity
+ -

Targets for monoclonal antibody therapy in myeloma
Adapted from: Anderson KC. J Clin Oncol 2012;30:445-452
Cell surface targets
Signaling molecules
IL-6RANKLDKK1VEGFIGF-1SDF-1BAFF, APRIL

Cell Surface Targets
CS1 (SLAMF7) CD38
Vellette et al. Crit Rev Oncol/Hem. 2013 168-77; Malavasi et al., Physiol Rev. 2008;88(3):841-86.
SLAMF7: Signalling lymphocytic activation molecule F7.

Mechanisms of action
Van de Donk et al, Blood 2015 (submitted).
ADCC: antibody dependent cell-mediated cytotoxicity; ADCP: antibody depedent cell-mediated phagocytosis;
CDC; complement dependent cytotoxicity.

Monoclonal antibodies in MM
Target Antibody Mechanism of
action
Activity as
single
agent
Activity/under
evaluation in
combo
CS1
(SLAM
F7)
Elotuzumab
(Humanized IgG1k)
ADCC
Enhance NK
activity
Interference with
cell interaction
- + VD
+ Rd
CD38 Daratumumab
(Fully human IgG1k) ADCC
CDC
ADCP
Direct induction
of apopotosis
Modulation CD38
function
+ + V-based
+ Rd
+ Pd
Isatuximab
(SAR650984; chimeric
IgG1k)
+ + VCD
+ Rd
MOR202
(fully human IgG1l)
+
MM: multiple myeloma; ADCC: antibody depandent cell-mediated cytotoxicity; ADCP: antibody depedent cell-
mediated phagocytosis; CDC; complement dependent cytotoxicity; VD: bortezomib-dexamethasone; Rd:
lenalidomide;dexamethasone; Pd: pomalidomide-dexamethasone; VCD: bortezomib-cyclophosphamide-
dexamethasone; V: bortezomib

Mechanisms of action of Daratumumab
Jelinek et al. Blood Reviews, 2015

Phase 1/2 trial: Daratumumab single agent in
relapsed/refractory MM (GEN501)
Expansion cohort: Extended treatment for close to 2 years
Dose-escalation cohorts
Open label, weekly iv infusion, 8 weeks
Dose-escalation: 3+3 scheme*
0.005→0.05→0.1→0.5→1.0 →2.0→4.0→8.0→16.0 →24.0 mg/kg
Part 2: 72 pts
Open label, single arm, 8 and 16 mg/kg
8 weekly infusions followed by
8 biweekly infusions followed by up to
72 monthly infusions
Different combinations of premedications, predose infusions, infusion
volumes, and infusion rates (3 – 4 hours)
Part 1: 32 pts
* - start with pre-dose at 10% of full dose, max 10 mg
- 3 weeks’ delay after first full dose
- governed by independent data monitoring committee
Lokhorst et al. N Engl J Med 2015; 373:1207-1219

Daratumumab monotherapy (GEN501)
Part 2: Patients characteristics (72 Pts)
8 mg/kg (n=30) 16 mg/kg (n=42)
Median prior lines 4 4
Refractory to
Bortezomib
Lenalidomide
Bortezomib & lenalidomide
70%
87%
63%
71%
74%
64%
Overall, 79% were refractory to last line and 76% had received ASCT
Lokhorst et al. N Engl J Med 2015; 373:1207-1219

Re
sp
on
se
ra
te (
%)
40
8 mg/kg
(n=30)16 mg/kg
(n=42)
ORR=36%ORR=10%
PR n=3
(10%)
PR n=11
(26%)
VGPR n=2 (5%)
CR n=2 (5%)
30
20
10
0
Response increased to 56% in patients with ≤3 lines
Median time to first & best response: 0.9 & 1.8m
Lokhorst et al. N Engl J Med 2015; 373:1207-1219
Daratumumab monotherapy (GEN501): Part 2 efficacy
8 mg/kg:
Median 2.4 months
16 mg/kg:
Median 5.6 months
Duration of response: 6.9 m & not reached
OS @ 12 months: 77% in both groups
Response Rate Progression-free survival
Median follow-up:
16.9 months (8 mg/kg), 10.2 months (16 mg/kg)
PR: partial response; VGPR: very good PR; CR complete
response; ORR overall response rate; OS: overall survival

• Most AEs grade 1 or 2
– Most common (≥ 25% of pts): fatigue, allergic rhinitis, pyrexia
– Nasopharyngitis 24%, cough 21%
• Grade 3 or 4 AEs:
– 53% in 8 mg/kg group and 26% in 16 mg/kg group
– In ≥ 2 patients: pneumonia (5 pts), thrombocytopenia (4 pts),
neutropenia, leukopenia, anemia, hyperglycemia (2 each)
• Infusion-related reactions:
– 71% (all grade 1/2, except 1 grade 3)
– Mostly during first infusion (only 8% in more than one infusion)
– No discontinuation
Lokhorst et al. N Engl J Med 2015; 373:1207-1219
Daratumumab monotherapy (GEN501): Part 2 safety

Infusion-related reactions
• Possible signs and symptoms of acute infusion reactions
– Allergic reactions/hypersensitivity
– Skin reactions
– Systemic reactions
– Respiratory reactions
– Cardiovascular symptoms
• Administer pre-medication to reduce the risk of IRRs (approximately 1 hour prior to every
daratumumab infusion)
– intravenous corticosteroid
(methylprednisolone 100 mg or an equivalent long acting corticosteroid)
– oral antipyretic
(paracetamol at 650-1000 mg)
– oral or intravenous antihistamine
(diphenhydramide 25-50 mg or equivalent)
• Post-medication corticosteroids on 1st and 2nd day
after all infusions
• In case of occurrence of IRRs
– React early to mild signs of symptoms and immediately
stop the infusion
– Manage symptoms appropriately, consider e.g. antihistamines, corticosteroids
– Once symptoms have resolved, treatment may be resumed
at half the infusion rate
– In case of grade 4 IRRs permanently discontinue treatment

• Open-label, international, multicenter study
• Initially, pts randomized 1:1 to receive
DARA
– 8 mg/kg every 4 weeks or
– 16 mg/kg every week for 8 weeks, every
2 weeks for 16 weeks, then every 4 weeks
• 16 mg/kg DARA established as the
recommended dose for further study
• Results are reported for all patients treated
with 16 mg/kg DARA (n=106)
16 mg/kg
(n = 16)
8 mg/kg
(n = 18)
16 mg/kg
(n = 106)
Response
evaluated
Randomization
Additional 90
patients enrolled
at 16 mg/kg
Primary objective
• ORR in pts with ≥3 prior lines of therapy or disease refractory to PI and IMiD
Secondary objectives
• TTP, PFS, OS, DOR, TTR, clinical benefit rate, safety and tolerability
Lonial et al. ASCO 2015 (Abstract LBA8512); oral presentation
Phase 2 trial: Daratumumab in refractory MM
(MMY2002, Sirius trial)

Sirius Trial: Baseline patients characteristics
• Patients (n=106)
– ≥3 prior lines
– 80% prior ASCT
– 97% refractory to last line
– 95% refractory to proteasome inhibitor and IMiD
– 77% refractory to alkylating agents
– 66% refractory to 3 of 4 therapies (Bort, Len, Carf, and Pom)
– 63% refractory to pomalidomide
– 48% refractory to carfilzomib
• Treatment:
– Daratumumab monotherapy (16 mg/kg)
Lonial et al. ASCO 2015 (Abstract LBA8512); oral presentation

Sirius Trial: overall response rate
• ≥ VGPR 12%, ≥ MR 34%
• Median time to response: 1 month
• Median duration of response: 7.4
months
0
5
10
15
20
25
30
35
16 mg/kg
ORR = 29%
sCR: n=3 (3%)
VGPR: n=10 (9%)
PR: n=18 (17%)
Lonial et al. ASCO 2015 (Abstract LBA8512); oral presentation
33 33
30
21 20
30 29 28 2826
21
0
5
10
15
20
25
30
35
40
OR
R, %
Refractory to
All patients By patients subgroup

Sirius Trial: survival
Pooled analysis (GEN501/Sirius):
median follow-up:14.8 months, estimated median OS 19.9 months
96106 85 82 64 23 10 2 0Patients at
risk
80
100
60
40
20
00 42 6 8 16141210
Months from start of treatment
Pati
en
ts a
live (
%)
Median NE
(95% CI, 13.7–NE)Median 3.7 months
(95% CI, 2.8–4.6)
63106 38 32 17 5 4 1 0Patients at
risk
80
100
60
40
20
0
0 42 6 8 16141210
Months from start of treatment
Pa
tie
nts
pro
gre
ss
ion
-
fre
e a
nd
ali
ve
(%
)
Usmani et al Abs #29 Orlando, ASH 2015; Lonial et al. ASCO 2015 (Abstract LBA8512)
Progression-free survival Overall survival

Sirius Trial: Safety
• Serious AEs: 30%
• Grade 3/4: 23% (anemia &
thrombocytopenia: more frequently in non-
responders)
• No discontinuations due to DARA-related
AEs
• No febrile neutropenia reported
• Infusion-related reactions (IRR)
– 42.5% (mainly grade 1/2 & during first
infusion (Only 7% at >1 infusion)
– 4.7% grade 3 ( No grade 4)
• The most common IRRs
included nasal congestion
(12%), throat irritation (7%),
cough, dyspnea, chills, and
vomiting (6% each)
• No patients discontinued
treatment due to IRRs
Lonial et al. ASCO 2015 (Abstract LBA8512); oral presentation
0
5
10
15
20
25
30
35
40
45
Overall 1st infusion 2nd infusion 3rd or laterinfusion
Incid
en
ce
of IR
R, %

Daratumumab plus Len-Dex in Relapsed/Refractory myeloma

Overall Best Response
• Mean duration of follow-up: 12.9 months (Part 1, range: 4.0-22.1) and 5.6 months (Part 2, range: 2.7-7.0)
• Median time to response: 1 month for 16 mg/kg in Part 2
• Median time to CR in Part 2 was 4.9 months
• As has been observed with other mAbs, DARA may interfere with IFE
– Interference assay to be validated
CR 31% CR 6.7%
VGPR 46%
PR 23%
VGPR 43%
PR 37%
CR 6.7%
CR 8.0%CR
11.8%
VGPR 43.3%
VGPR 52%
VGPR 52.9%
100
86.7
50.0
60.064.7
Treatment
Perc
enta
ge (
%)
0
20
40
60
80
100
Part 1 Part 2
Overall best response
Treatment
0
20
40
60
≥2 cycles
(N = 30)
≥4 cycles
(N = 25)
≥6 cycles
(N = 7)
Perc
enta
ge (
%)
VGPR or better response bycycles of treatment (Part 2)
PR VGPR CR
27
Plesner T, et al. Oral presentation: 56th American Society of Hematology (ASH) Annual Meeting and Exposition; December 6-9, 2014; San Francisco, CA, USA.
.

Serious Adverse Events
• 15 SAEs reported:
– Part 1: 7 (all assessed as
unrelated to DARA)
– Part 2: 8 (4 DARA-related)
• DARA related SAEs:
– Pneumonia, neutropenia,
diarrhea
(1 patient each [16 mg/kg])
– Laryngeal edema
(1 patient [16 mg/kg])
Plesner et al. ASH 2014 (Abstract 84); oral presentation
Daratumumab plus Len-Dex in RRMM: safety
≤8 mg/kg
Part 1
(n = 10)
16 mg/kg
Part 1
(n = 3)
16 mg/kg
Part 2
Current infusion
program (n = 21)
16 mg/kg
Part 2
Accelerated infusion
program (n = 11)
Perc
ent (%
)
0
20
40
60
Infusion-related reactions
20.020.0
33.3
38.1
4.8
63.6
First infusion Subsequent infusion
Infusion related Reactions
• 19/45 patients reported IRRs
• Majority grade 1 and 2
• Most (86%) during first infusion
• 18/19 patients with IRRs
recovered and continued
subsequent infusion
• Accelerated infusion was
tolerable but associated with
higher incidence of grade 1/2
Aes
•

MMY1001 (NCT01998971): Phase I Study of Daratumumab + Backbone Treatments
• VD: bortezomib (1.3 mg/m2 twice weekly x 4 cycles, then once weekly x 14 cycles)/dexamethasone (20 mg)a
– Newly diagnosed; n = 6
• VMP: bortezomib (1.3 mg/m2 twice weekly x 1 cycle, then once weekly x 8 cycles)/melphalan (9 mg/m2)/prednisone (60 mg/m2)b
– Newly diagnosed transplant ineligible; n = 12
• VTD: bortezomib (1.3 mg/m2 twice weekly x 4 cycles, then once weekly x 14 cycles )/thalidomide (100 mg daily x 21 days)/ dexamethasone (20 mg)a
– Newly diagnosed; n = 12
• PD: pomalidomide (4 mg once daily)/dexamethasone (40 mg)c
– Relapsed/refractory,≥2 lines of therapy including 2 consecutive cycles of lenalidomide and bortezomib; n 100
aDaratumumab once weekly x 2 cycles, then once every 3 weeks x 16 cycles or until transplantation.bDaratumumab once weekly x 1 cycle, then every 3 weeks x 8 cycles.cDaratumumab once weekly x 2 cycles, then once every 2 weeks x 4 cycles, then once every 4 weeks x 7 cycles or until disease progression; dexamethasone 20 mg if age >75 y.
ClinicalTrials.gov Identifier: NCT01998971. Available at: http://www.clinicaltrials.gov/ct2/show/NCT01998971?term=NCT01998971&rank=1. Accessed February 23, 2015.
29

Daratumumab + backbone treatments (MMY1001)
Response rate

MMY1001: Best Response (PR or Better) and Duration of Follow-up
Time from first dosing date (weeks)
VD + DARA VTD + DARA VMP + DARA POM-D + DARA
100003
100001
100004
100011
100005
100008
100014
100015
100017
100016
100019
100021
100022
100026
100024
100027
100028
100012
100023
100029
100018
100018
100018
100013
100009
0 3 6 9 12 16 18 21 24 27 30 33
PR
PR
PR
PR
PR
sCR
PR
PR
VGPR
VGPR
PR
PR
PR
PR
PR
PR
PR
PR
PR
VGPR
VGPR
VGPR
VGPR
PR
PR
PR
PR
PR
X
VGPR
Moreau P, et al. Oral presentation: 56th American Society of Hematology (ASH) Annual Meeting and Exposition; December 6-9, 2014; San Francisco, CA, USA.
31

• Most common AEs were hematologic; not likely related
to Dara
• Grade ≥3 AEs occurred in 22 (45%)
– Most common: neutropenia (25%), thrombocytopenia
(10%), anemia (8%), and pneumonia (6%)
• Apart from IRRs, the addition of DARA did not result in
additional toxicity
• IRRs occurred in 24 (49%) patients overall
– Generally grade 1 or 2 (3 grade 3 and no grade 4)
– Most occurred within the first day of the first cycle
Mateos et al. EHA 2015 (Abstract P275); poster presentation
Daratumumab Safety (MMY1001)

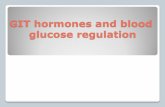
Blood compatibility testing for patients
receiving anti-CD38 mAbs
• CD38 is weakly expressed on human red blood cells (RBCs)
• Daratumumab does not interfere with the major antigens of
ABO/RhD typing, but with the minor ones
• Daratumumab binds to CD38 on RBCs false positive results
in the panreactive Indirect Antiglobulin Test (indirect Coombs
test)
Chapuy et al. Transfusion. 2015;55(6 Pt 2):1545-54
Oostendorp et al. Transfusion. 2015;55(6 Pt 2):1555-62
Hannon JL, et al. Transfusion. 2015;55(6 Pt 2):1555-62
Daratumumab binds
to CD38 on RBCs2
CD38
Daratumum
ab

Daratumumab Development In all MM Settings
Ph 1 Ph 2 Ph 3KEY:
Ph 2 Study MMY2002DARA in ≥3
prior lines or double
refractory MM; single agent, 2-part study
Ph 3 Study MMY3007
DARA + VMP vs VMP in noASCT
Ph 3 StudyMMY3006
DARA + Vel/Thal/dex vs Vel/Thal/dex in
ASCT
Ph 1/2 Study 501FIH, single agent, dose escalation,
safety, PK
Ph 1/2 Study 503Rev/dexcombo
Ph 1b Multi-arm MMY1001 combo
Ph 2 Study SMM2001
Randomizedsingle agent
Ph 3 StudyMMY3004
Vel/dex/DARA vsVel/dex in pts1 prior therapy
Smoldering
Myeloma
Newly Diagnosed
Transplant & Nontransplant
Maintenance
Relapsed
1+ Prior Line
Relapsed-Refractory
Double Refractory
3+ Prior Lines
Ph 3 Study MMY3003
DARA + Rev/dexvs Rev/dex
1 prior therapy
Ph 3 StudyMMY3008
DARA + Rd vs R/d NoASCT
34

Elotuzumab: A Monoclonal Antibody Targeting SLAMF7
Elotuzumab Humanized, IgG1 mab specific for human SLAMF7
― No cross-reactivity with non-human homologues or other SLAM family members
Binds to a membrane-proximal motif of SLAMF7― Critical for mediating killing of target cells (in vitro)
SLAMF7 = Signalling Lymphocyte Activation Molecule Family 7;ITSM = Intracellular Tyrosine Switch MotifEAT-2 = Ewing's Sarcoma associated transcript 2
C2
V
Y261
Y281
CO
OH
NH
2
TM
Elotuzumab
mediates “inhibitory” signal
mediates “activating” signal EAT-2/CD45 dependent
mechanism (NK cells)
mediates self-adhesion
ITSM
SLAMF7
Expression highest on Plasma Cells
Varied expression across hematopoietic cells (NK, NK-T, DC, B, TCD8+, PC)
Not express on non-hematopoietic cells
SLAMF7 K/O Phenotype: compromised NK function
Veillette and Guo, Critical Reviews Oncol Hematol, 2013. Cruz-Munoz et al, Nature Immunology, 2009.

Differential SLAMF7 Signalling: Elotuzumab Activates NK Cells but not Myeloma Cells
Guo et al (Mol Cell Bio), 2015: Phosphorylation of SLAMF7 is mediated by Src kinases. Inhibitory mechanism (in EAT2-
/CD45+ cells) is mediated by SHIP-1. MM cells are deficient for EAT-2 and CD45, therefore SLAMF7 does not mediate activating or inhibitory effects in these cells.EAT-2 = Ewing's Sarcoma associated transcript 2; SLAMF7 = Signalling Lymphocyte Activation Molecule Family 7.
Myeloma CellsNK Cells
EAT-2+ EAT-2-
Activation No effect

Mechanisms of action of Elotuzumab
Liu et al. Blood Lymphat Cancer, 2014
The primary mechanism of action of elotuzumab against myeloma cells isNK cell-mediated ADCC. Elotuzumab can also interfere with the adhesionof myeloma cells to BMSC, or can induce NK cell activation directly throughbinding CS1 expressed on NK cells.

Dose-limiting toxicities were assessed during cycle 1
1701 A Phase I Multicenter, Open-Label, Dose Escalation Study of Elotuzumab Monotherapy in Subjects With advanced MM
Zonder JA et al. Blood. 2012;120(3):552-559

1701 Elotuzumab Monotherapy :Tolerability
• MTD was not reached up to the highest dose level of 20 mg/kg
• Key SAEs were first dose infusion reactions (IR)
– Gr 3 allergic reaction, Gr 2 rigors, fever, chest pressure, bradycardia
– No dose correlation seen for infusion reactions
– No serious infusion reactions following IV corticosteroid premedication
• No neutropenia or thrombocytopenia
• Transient reduction in lymphocytes seen within hours following first dose
AEs were generally mild to moderate in severity, and AEs attributed to study medication were primarily infusion-related
Zonder JA et al. Blood. 2012

1701 Elotuzumab Monotherapy : Pharmacodinamics
Saturation of CS1 by elotuzumab on bone marrow target cells increased as the dose of elotuzumab
increased. At dose of 10 mg/kg and 20 mg/kg elotuzumab, CS1 receptors on bone marrow-derived myeloma cells were consistently saturated. Lower dose groups
exhibited more variation in the level of target cell saturation achieved.

1701 Elotuzumab Monotherapy: Efficacy
Zonder JA et al. Blood. 2012

Elotuzumab Synergizes With BortezomibTo Enhance Myeloma Cell Death
42
Van Rhee et al (Molecular Cancer Therapeutics), 2009.
Induces myeloma cell injury and lowers threshold for NK cell-mediated killing of myeloma cells by elotuzumab
Direct NK Cell activation
NK CellMyeloma Cell
Elotuzumab
SLAMF7
ADCC
CD16a +
Enhances expression of activating ligands and reduces inhibitory ligands on MM cells

Elotuzumab Synergizes with Lenalidomideto Enhance Myeloma Cell Death
Balasa et al (Cancer Imm and Immunotherapeutics), 2015.
LenalidomideInduces myeloma cell injury and lowers threshold for NK cell-mediated killing of myeloma cells by elotuzumab
Direct NK Cell activation
NK Cell
Elotuzumab
SLAMF7
ADCC
CD16a +
LenalidomideEnhances adaptive and innate immune system including production of IL2 to increase NK cell activity
Myeloma Cell

Phase 1 and 2 Elotuzumab Trials (Relapsed/refractory)
Trial Phase Treatment Sample Size Efficacy (%)Median
PFS
1701 1 Elotuzumab monotherapy 35 SD=26.5 —
1702 1 Elotuzumab + bortezomib 28 ORR=48 9.46 mo
1703 1Elotuzumab + lenalidomide/
dexamethasone28 ORR=82 33 months
1703 2Elotuzumab + lenalidomide/
dexamethasone73 ORR=84 29 months
009 2Elotuzumab + bortezomib/
dexamethasone152 ORR=65 9.7 months
These results compare favorably with ORR (27-38%/60%–61%) and median TTP (6-7/11.1-11.3 months) observed in four phase II/III clinical studies of bortezomib/dexamethasone or lelenalidomide/dexamethasone, respectively with similar patient populations

1702 Phase 1 trial Elotuzumab in combination with Bortezomib in the treatment of RRMM: Pharmacodinamics
Pharmacodynamic studies of MM cells isolated from patient bone marrow biopsies demonstrated that these threshold concentrations were associated with high saturation (80% and 95%, respectively) of available CS1 binding sites at doses of 10 mg/kg and 20 mg/kg, similar to that seen in murine models and in a clinical study of elotuzumab monotherapy.
Jakubowiak AJ et al. J Clin Oncol. 2012

1703 A Phase Ib/II, Multicenter, Open-Label, Dose-Escalation Study of Elotuzumab in Combination With Lenalidomide and Dexamethasone in Subjects With Relapsed MM: PK and PD
• PK and PD studies demonstrated that elotuzumab doses of 10 and 20 mg/kg achieved serum levels of antibody predicted to achieve optimal antitumor activity based on preclinical xenograftmodels and resulted in similar levels of CS1 receptor saturation on malignant bone marrow plasma cells.
• At these drug levels, 80% of CS1 sites on bone marrow MM cells were fully saturated .
Lonial S et al. J Clin Oncol. 2012

CA204-009: A randomized, open-label, phase 2 study of bortezomib and
dexamethasone with or without elotuzumab in patients with
relapsed/refractory myeloma (RRMM)
EloBd to progression
Bd to progression
E
N
R
O
L
L
M
E
N
T
N = 77
N = 75
PFS: primary endpoint
FOLLOW UP
• Cycles 1-8: 21 day cycles
• Cycle 9 onwards: 28 day cycles
• Cross over not permitted
Sample Size/Power:
N = 152. 80% power to detect a HR of 0.69 with 103 progression events
2-sided 0.30 significance level specified to test for difference in PFS between arms (p≤0.3 was considered significant)
– Investigational arm (EloBd): elotuzumab 10 mg/kg IV + bortezomib 1.3 mg/m2 IV* + (dexamethasone 20 mg po, or 8 mg IV and 8 mg po)
– Control arm (Bd): bortezomib 1.3 mg/m2 IV + dexamethasone 20 mg po
Accrual from Nov 2011
Interim analysis: June 2014
*Bortezomib to be administered SC following regulatory approval Jakubowiak A et al. EHA 2015 abs 103
Key inclusion
criteria
• RRMM
• 1–3 prior
therapies
• ECOG PS ≤2
• Prior
proteasome
inhibitor (PI)
treatment
permitted if not
refractory to PI

CA204-009: Baseline Demographics and Characteristics
Characteristic EBd (n=77) Bd (n=75) Total (N=152)
Age, mean (range) 65.4 (25–82) 65.1 (30–85) 65.3 (25–85)
≥65 years 43 (56) 42 (56) 85 (56)
≥75 years 15 (20) 14 (19) 29 (19)
Male, n (%) 42 (55) 37 (49) 79 (52)
Prior lines of therapy, n (%)
1 55 (71) 51 (68) 106 (70)
2 or 3 22 (29) 24 (32) 46 (30)
Months since diagnosis, median (range) 45 (9–296) 44 (8–285) 45 (8–296)
Prior proteasome inhibitor use, n (%)
Yes 38 (49) 37 (49) 75 (49)
Jakubowiak A et al. EHA 2015 abs 103
Characteristic EBd (n=77) Bd (n=75) Total (N=152)
ISS staging, n (%)
I 26 (34) 19 (25) 45 (30)
II 23 (30) 20 (27) 43 (28)
III 11 (14) 16 (21) 27 (18)
Not reported 17 (22) 20 (27) 37 (24)
Status disease at randomization, n (%)
Refractory 24 (16) 14 (9) 38 (25)
Relapsed 47(31) 57 (38) 104 (69)
Not reported 6 (4) 3 (2) 9 (6)

CA204-009: Overall Response Rate
0
20
40
60
Re
spo
nse
ra
te (
%)
EBd Bd
Overall
response rate
(PR or better)
Complete
response
(sCR + CR)*
VGPR≥ VGPR
(sCR + CR +
VGPR)
*Complete response rates in the EBd group may be underestimated due to interference from
therapeutic antibody in immunofixation and serum protein electrophoresis assay
There was no difference between the 2 treatment arms for stable disease (14 patients each) and
progressive disease (4 patients each)
65
63
4
2327
4
3034
Jakubowiak A et al. EHA 2015 abs 103

Progression-Free Survival
EBd Bd
HR 0.72 (70% CI 0.49–1.06; 95% CI 0.59–0.88);
stratified log-rank p=0.09
Median PFS
(95% CI)
9.7 mo
(7.4–12.2)
6.9 mo
(5.1–10.2)
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
PFS (months)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
77 69 58 47 41 32 26 22 14 11 5 3 2 1 0
75 61 50 37 32 25 21 14 11 9 5 3 1 0 0
EBd
Bd
Number of patients at risk
39%
33%
1-year PFS
EBd (events: 52/77)
Bd (events: 59/75)Pro
bab
ility p
ro
gressio
n free
EBd-treated patients had a 28% reduction in the risk of disease progression or death
Overall Survival
Early OS data show an observed improvement in favor of EBd
0 2 4 6 8 10 12 14 20 22 24 26 28
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
16 18 30
OS (months)
85%
74%
1-year OS
HR 0.61 (70% CI 0.43–0.85)
77 76 74 71 69 67 61 61 26 20 7 3 150 38 0
75 67 62 59 57 54 51 48 22 15 6 1 036 30 0
EBd
Bd
Number of patients at riskP
ro
bab
ilit
y o
f su
rviv
al
EBd
(events: 17/77)
Bd
(events: 23/75)
• 40 deaths observed at the time of analysis (17 EBd, 23 Bd), mainly due to
disease progression
Progression-free survival Overall survival
Jakubowiak A et al. EHA 2015 abs 103
CA204-009: A randomized, open-label, phase 2 study of bortezomib and
dexamethasone with or without elotuzumab in patients with RRMM
28% reduction in the risk of
disease progression 39% reduction in the risk of death

Events, n (%)EBd (n=75) Bd (n=75)
Any grade Grade 3–4 Any grade Grade 3–4
All adverse events 75 (100) 51 (68) 72 (96) 45 (60)
Infections and infestations 49 (65) 13 (17) 40 (53) 10 (13)
Diarrhea 32 (43) 6 (8) 25 (33) 3 (4)
Constipation 29 (39) 1 (1) 22 (29) 0
Cough 29 (39) 1 (1) 17 (23) 0
Anemia 28 (37) 5 (7) 21 (28) 5 (7)
Peripheral neuropathy 26 (35) 6 (8) 25 (33) 7 (9)
Pyrexia 25 (33) 0 20 (27) 3 (4)
Peripheral edema 22 (29) 3 (4) 18 (24) 0
Insomnia 22 (29) 0 14 (19) 1 (1)
Asthenia 20 (27) 3 (4) 21 (28) 2 (3)
Fatigue 20 (27) 3 (4) 19 (25) 1 (1)
Paresthesia 20 (27) 0 14 (19) 4 (5)
Nausea 19 (25) 1 (1) 16 (21) 1 (1)
Thrombocytopenia 12 (16) 7 (9) 20 (27) 13 (17)
Jakubowiak A et al. EHA 2015 abs 103
No additional adverse events versus Bd
CA204-009: A randomized, open-label, phase 2 study of bortezomib and
dexamethasone with or without elotuzumab in patients with RRMM
Safety

Infusion Reactions
• No Grade 3–5 infusion reactions (7% grade 1-2)
• No infusion reactions at maximum planned infusion rate of 5 mL/min
• 27 patients received elotuzumab infusion within 1 hour
• No patient discontinued because of an infusion reaction
• Infusion reactions were low and manageable
Events, n (%)EBd (n=75)
Grade 1–2 Grade 3–5
Infusion reaction 5 (7) 0
Pyrexia 2 (3) 0
Bone pain 1 (1) 0
Chills 1 (1) 0
Flushing 1 (1) 0
Nausea 1 (1) 0
Peripheral sensory neuropathy 1 (1) 0
Jakubowiak A et al. EHA 2015 abs 103

ELOQUENT-2: Elotuzumab-Rd vs Rd• Open-label, international, randomized, multicenter, phase 3 trial
(168 global sites)
Key inclusion criteria
RRMM
1–3 prior lines of therapy
Prior Len exposure permitted in 10% of study population (patients not refractory to Len)
Elo plus Len/Dex (E-Ld) schedule (n=321)
Elo (10 mg/kg IV): Cycle 1 and 2: weekly; Cycles 3+: every other week
Len (25 mg PO): Days 1–21Dex: weekly equivalent, 40 mg
Len/Dex (Ld) schedule (n=325)
Len (25 mg PO): Days 1–21;
Dex: 40 mg PO Days 1, 8, 15, 22
Repeat every 28 days
Assessment
Tumor response: every 4 weeks until progressive disease
Survival: every 12 weeks after disease progression
Endpoints:
– Co-primary: PFS and ORR
– Other: overall survival (data not yet mature), duration of response,
quality of life, safety
All patients received premedication to mitigate infusion reactions prior to
elotuzumab administration
Elotuzumab IV infusion administered ~ 2–3 hours
Lonial S et al N Engl J Med, 2015

Characteristic E-Ld (n=321) Ld (n=325)
Age (years), median (range) 67 (37–88) 66(38–91)
≥65 years 187 (58) 183 (56)
Region, %
Europe 61 60
North America 21 21
Rest of the world 18 19
International Staging System disease stage, n (%)
I 44 43
II 32 32
III 21 21
Not reported 4 14
Cytogenetics (FISH)del(17p)
Yes 32 32
No 66 67
Not reported 2 1
t(4;14)
Yes 9 10
No 89 89
Not reported 2 1
1q21
Yes 46 50
No 53 49
Not reported 2 1
Baseline Demographics and
Disease Characteristics
FISH = fluorescence in situ hybridization

Baseline Demographics and
Disease Characteristics
Characteristic E-Ld (n=321) Ld (n=325)
Prior regimens, median (range) 2 (1–4) 2 (1–4)
Prior therapies, %
Bortezomib 68 71
Melphalan* 69 61
Thalidomide 48 48
Lenalidomide† 5 7
Response to most recent line of therapy, %‡
Refractory 35 35
Bortezomib refractory 22 21
Thalidomide refractory 9 11
Relapsed 65 65
Prior stem cell transplantation, % 52 57
*Oral or intravenous. †Prior lenalidomide was permitted if best response was ≥partial response and patients were not refractory to prior lenalidomide
treatment; patients could not receive more than 9 cycles of lenalidomide and had at least 9 months between the last dose of lenalidomide and
progression. ‡One patient in the elotuzumab group had an unknown response to the most recent line of therapy

Co-primary Endpoint: Overall Response Rate
*Defined as partial response or better. †Complete response rates in the E-Ld group may be underestimated due to interference from
therapeutic antibody in immunofixation and serum protein electrophoresis assay
0
20
40
60
80
100
Resp
on
se r
ate
(%
)
E-Ld Ld
p=0.0002
79
66
Overall
response
rate*
Complete
response
(sCR + CR)†
Very good
partial
response
Combined
response
(sCR + CR +
VGPR)
Partial
response
47
21
2833
28
38
46

Progression-free survival
Lonial S et al N Engl J Med, 2015: 1-11
ELOQUENT-2: Elotuzumab-Rd vs Rd
Median 19.4 vs 14.9 months
E-Ld−treated patients had a 30% reduction in the risk of disease progression or death;
treatment difference at 1 and 2 years was 11% and 14%, respectively

Progression Free Survival by Tumor Response

• No Grade 4–5 infusion reactions
• 33 patients (10%) infusion reaction , 29/33 grade 1-2
• 2 (1%) discontinued because of an infusion reaction
ELOQUENT-2: Elotuzumab-Rd vs Rd
Safety
Lonial S et al N Engl J Med, 2015: 1-11

Elotuzumab Clinical Development Program
Dex, dexamethasone; liri, lirilumab; ure, urelumab.1. Clinicaltrials.gov. NCT00425347. 2. Clinicaltrials.gov. NCT00726869. 3. Clinicaltrials.gov. NCT01241292. 4. Clinicaltrials.gov. NCT01393964. 5. Clinicaltrials.gov. NCT02252263. 6. Clinicaltrials.gov. NCT00742560. 7. Clinicaltrials.gov. NCT01478048. 8. Clinicaltrials.gov. NCT01632150. 9. Clinicaltrials.gov. NCT01441973. 10. Clinicaltrials.gov. NCT02159365. 11. Clinicaltrials.gov. NCT01239797. 12. Clinicaltrials.gov. NCT01335399.
Phase I Phase IIPhase III
Lenalidomide/dex ±elotuzumab
CA204-004 (N=646)11
Relapsed
CA204-006 (N=750)12
Newly diagnosed
1701 (N=35)1
Relapsedelotuzumab monotherapy
CA204-009 (N=150)7
Relapsedelotuzumab ± bortezomib/dex
1702 (N=28)2
Relapsedelotuzumab + bortezomib
CA204-005 (N=20)3
Relapsedelotuzumab + lenalidomide/dex
CA204-007 (N=26)4
Normal renal function/Renallyimpaired
elotuzumab + lenalidomide/dex
CA204-010 (N=40)8
Relapsedelotuzumab + thalidomide/dex
CA204-011 (N=40)9
Smolderingelotuzumab monotherapy
17036
(N=102)Relapsed
elotuzumab + lenalidomide/dex
CA223-028 (N=136)5
Relapsedelotuzumab + lirielotuzumab + ure
CA204-112 (N=76)10
Newly Diagnosed/Relapsedelotuzumab +
lenalidomide/dex

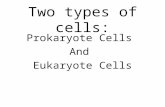
Analyses of Real World Data on Overall Survival in Multiple Myeloma
Patients with at Least 3 Prior Lines of Therapy Including a PI and an
IMiD, or Double Refractory to a PI and an IMiD
Usmani et al Abs #4498 Orlando, ASH 2015
.
237 days
154 days

Chemotherapy
Immunotherapy
All causes mortality
• Median OS is considered less suitable for survival curves that are skewed to the right since it does not differentiate the proportion of patients alive or dead after 50% of the patients have died
• Median OS provides a measure of when 50% of patients will die, it does not provide a true reflection of the survival time that may be expected from the patients who are alive after the median OS is reached

V
High-dosechemotherapy
ThalidomideBortezomib
Multiple Myeloma - incurable disease?
COMBOMPT VMPVTDRd
Maintenance/Consolidation
New combo with Nextgeneration PI/IMIDsMoAbContinuoustherapy
Future treatment paradigmsstart from nowaday’s evidence
Median survival > 7 yrs
CR: 50-70%