Anafilaksis (PIT 2008)
48
ANAPHYLAXIS: ANAPHYLAXIS: DIAGNOSIS, TREATMENT DIAGNOSIS, TREATMENT AND PREVENTION AND PREVENTION Heru Sundaru Heru Sundaru Drug Allergy and Anaphylaxis Clinic Division of Allergy – Clinical immunology Department of Internal medicine FKUI!SC" #a$arta
-
Upload
luthfita-rahmawati -
Category
Documents
-
view
225 -
download
0
Transcript of Anafilaksis (PIT 2008)
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 1/48
ANAPHYLAXIS:ANAPHYLAXIS:
DIAGNOSIS, TREATMENTDIAGNOSIS, TREATMENT
AND PREVENTIONAND PREVENTION
Heru SundaruHeru Sundaru
Drug Allergy and Anaphylaxis ClinicDivision of Allergy – Clinical immunology
Department of Internal medicine FKUI!SC"
#a$arta

7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 2/48
D%FI&I'I(& (F A&A)H*+A,ISD%FI&I'I(& (F A&A)H*+A,IS
Anaphylaxis is a severe- acute- life.threateningAnaphylaxis is a severe- acute- life.threateninggenerali/ed or systemic hypersensitivity reaction0generali/ed or systemic hypersensitivity reaction0
It is commonly- 1ut not al2ays- mediated 1y an allergicIt is commonly- 1ut not al2ays- mediated 1y an allergicmechanism- usually 1y Ig%0mechanism- usually 1y Ig%0
Allergic 3immunologic4 non.Ig%.mediated anaphylaxisAllergic 3immunologic4 non.Ig%.mediated anaphylaxisalso occurs0also occurs0
&on.allergic anaphylactic reactions- formerly called&on.allergic anaphylactic reactions- formerly called
anaphylactoid or pseudo.allergic reactions- may alsoanaphylactoid or pseudo.allergic reactions- may alsooccur0occur0
#ohansson S5( et al #ACI 6778-99:; <:6.=#ohansson S5( et al #ACI 6778-99:; <:6.=
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 3/48
Why we should kow!Why we should kow!
Anaphylaxis can be fatalAnaphylaxis can be fatal
Unpredictable and suddenlyUnpredictable and suddenly
Can happen anywhereCan happen anywhere
Its prevalence increasedIts prevalence increasedMedico legal ?Medico legal ?
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 4/48
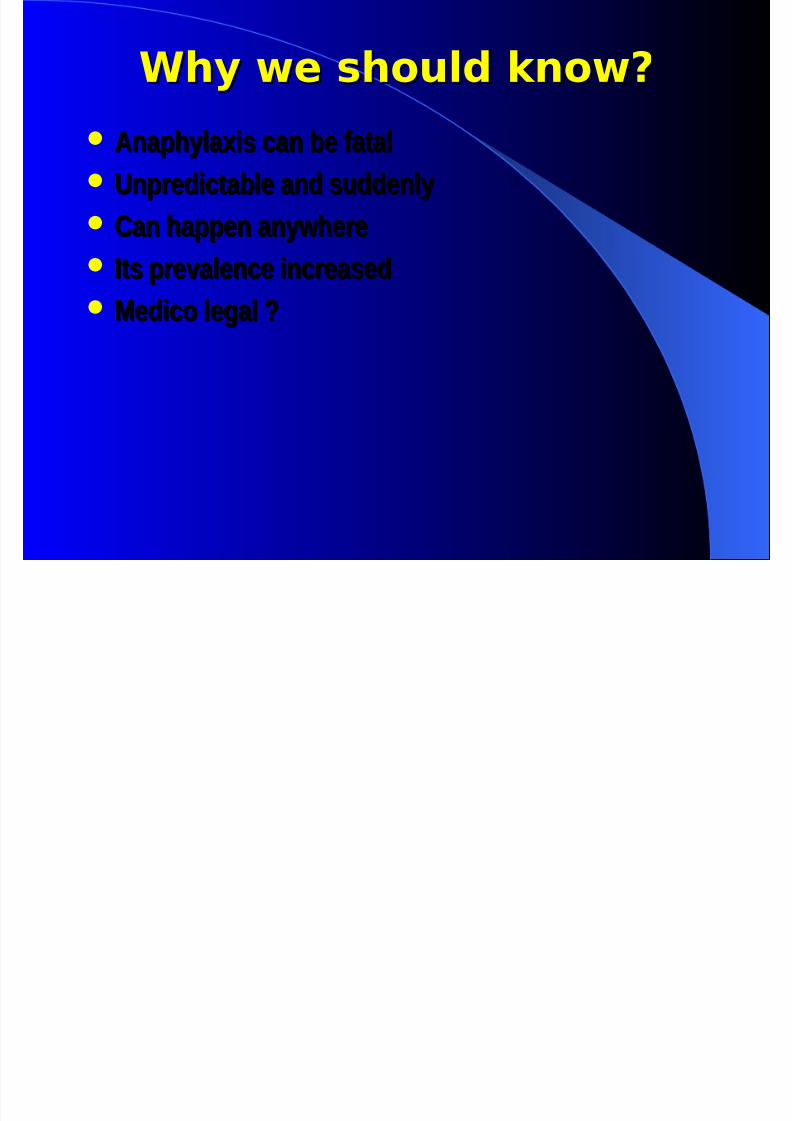
&um1er of hospital discharges 2ith the primary diagnosis of
anaphylaxis per 977 777 episodes of hospital discharge and cause
of anaphylaxis

7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 5/48
E"#de$#olo%y :E"#de$#olo%y :
)revalence of anaphylaxis
1. 1 : !"" attendees at #$ in U% &'tewart ( #wan)
1**+,
. Anaphylaxis hospital discharge -.+1"".""" &1**1 /
, 1".1"".""" &1**0 -, &'hei2 ( Alves) """,
!. 1!.!" ad3ission for anaphylaxis 1**" """
&4upta) et al. ""!,0. 10 death attributed to anaphylaxis in U% 1** /
""1 &5u3phrey) ""0,
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 6/48
A&"hyl&'#s: "o"ul&(#o s(udy # )A&"hyl&'#s: "o"ul&(#o s(udy # )
ye&*sye&*s Incidence &annual,: 1 per 1"".""" person / year
1!! residents who experienced 1-0 anaphylactic episode :
11+ residents 1 episode 11+ residents 1 episode
1! resident episode 1! resident episode
0 residents ! episode 0 residents ! episode -!6 atopy
+76 allergen identified: food) 3edication and insect sting
-6 allergy consultation 86 hospitali9ation
1 patient died
Yocum, et al. JACI 1999;104:452-6
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 7/48
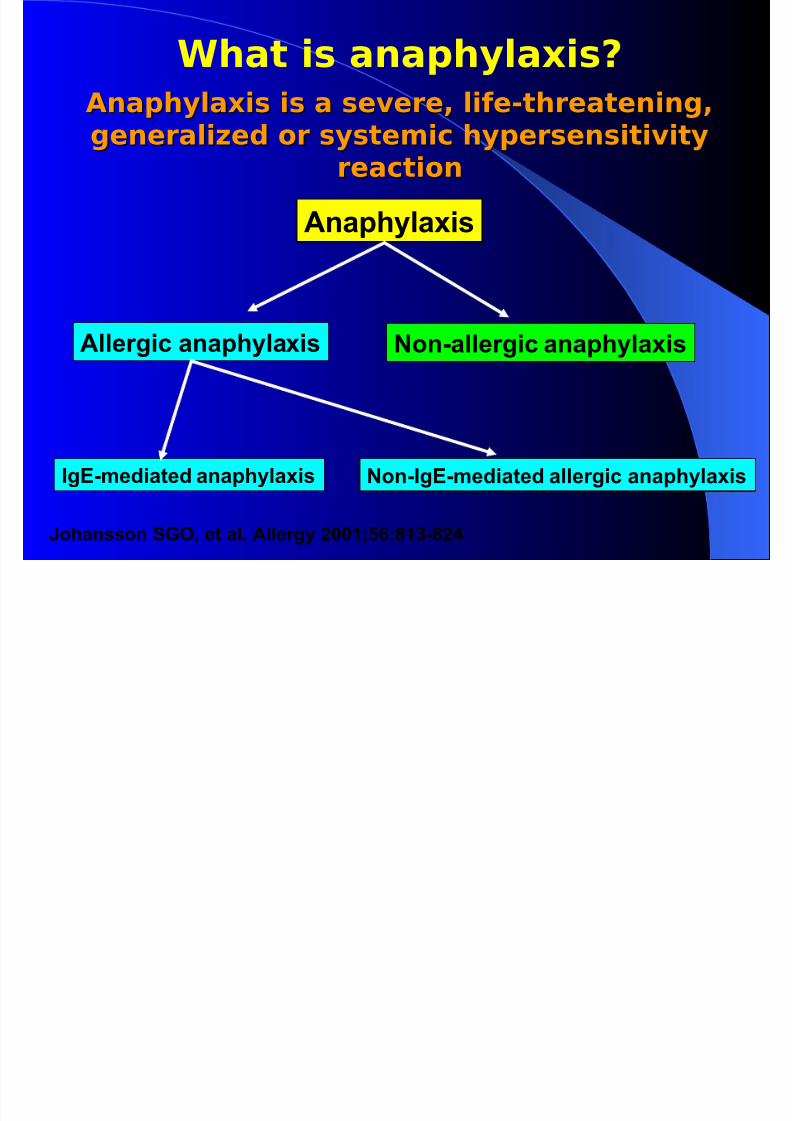
A&"hyl&'#s #s & se+e*e, l#e-(h*e&(e#%,A&"hyl&'#s #s & se+e*e, l#e-(h*e&(e#%,
%ee*&l#.ed o* sys(e$#/ hy"e*ses#(#+#(y%ee*&l#.ed o* sys(e$#/ hy"e*ses#(#+#(y*e&/(#o*e&/(#o
Anaphylaxis
Allergic anaphylaxis &on.allergic anaphylaxis
Ig%.mediated anaphylaxis &on.Ig%.mediated allergic anaphylaxis
#ohansson S5(- et al0 Allergy 6779>?=;<9:.<68
Wh&( #s &&"hyl&'#s!
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 8/48
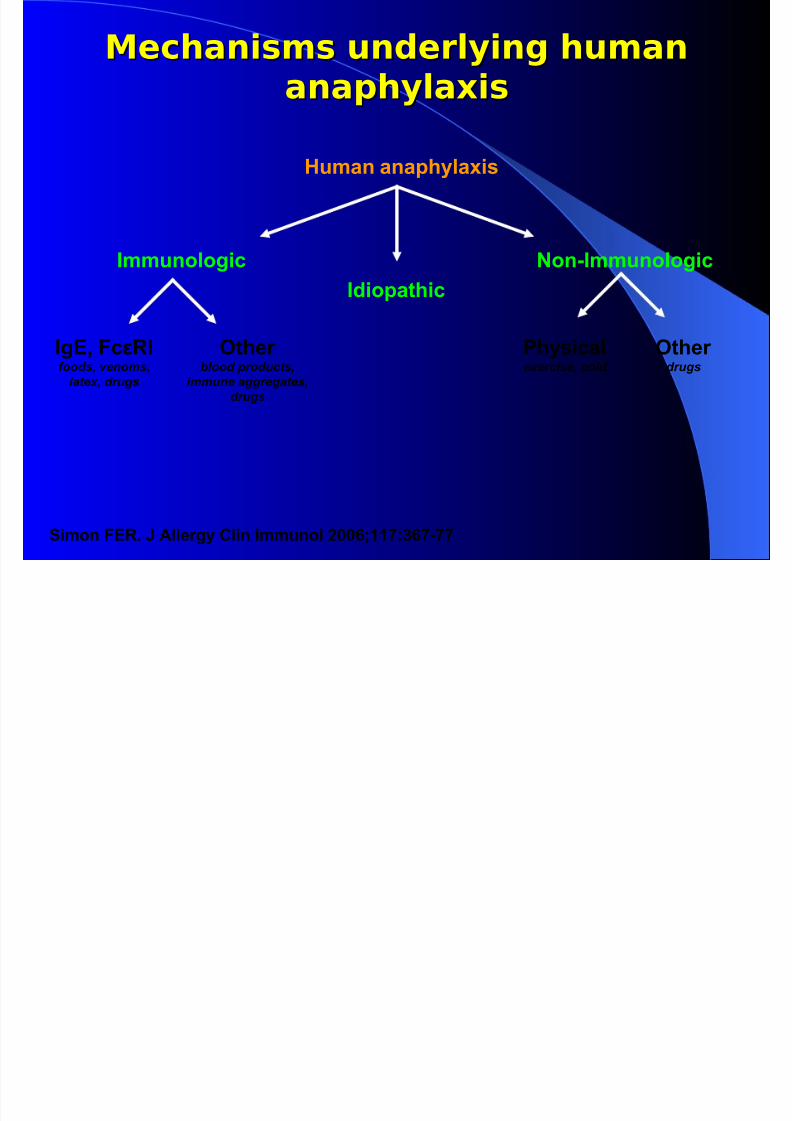
Me/h&#s$s ude*ly#% hu$&Me/h&#s$s ude*ly#% hu$&
&&"hyl&'#s&&"hyl&'#s
Human anaphylaxis
ImmunologicIdiopathic
&on.Immunologic
Ig%- Fc@!Ifoods, venoms,
latex, drugs
(ther blood products,
immune aggregates,
drugs
)hysicalexercise, cold
(ther drugs
Simon F%!0 # Allergy Clin Immunol 677=>99;:=.
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 9/48
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 10/48
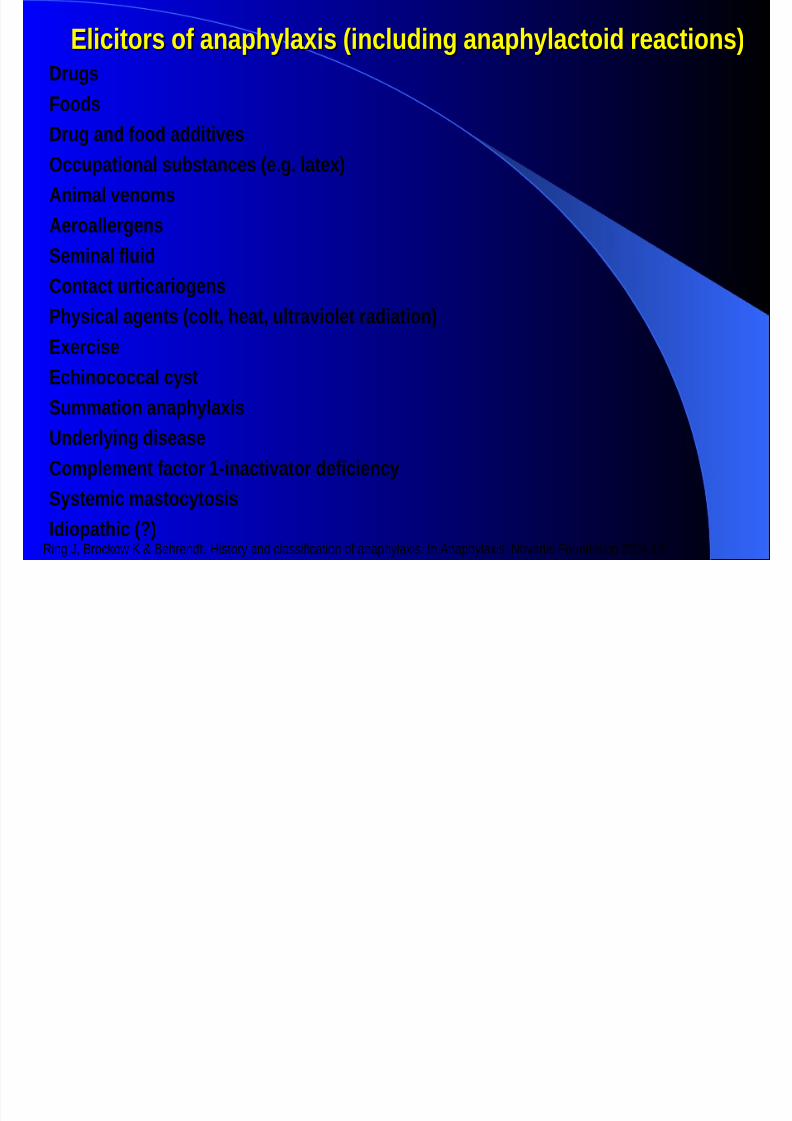
#licitors of anaphylaxis &including anaphylactoid reactions,#licitors of anaphylaxis &including anaphylactoid reactions,$rugs
oods
$rug and food additives;ccupational substances &e.g. latex,
Ani3al veno3s
Aeroallergens
'e3inal fluidContact urticariogens
5hysical agents &colt) heat) ultraviolet radiation,
#xercise
#chinococcal cyst
'u33ation anaphylaxis
Underlying disease
Co3ple3ent factor 1inactivator deficiency
'yste3ic 3astocytosis
Idiopathic &?,Ring J, Boc!o" # $ Be%en&t. 'i(to) an& cla((i*ication o* ana+%)lai(. In Ana+%)lai(. oati( /oun&ation 2004:12
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 11/48
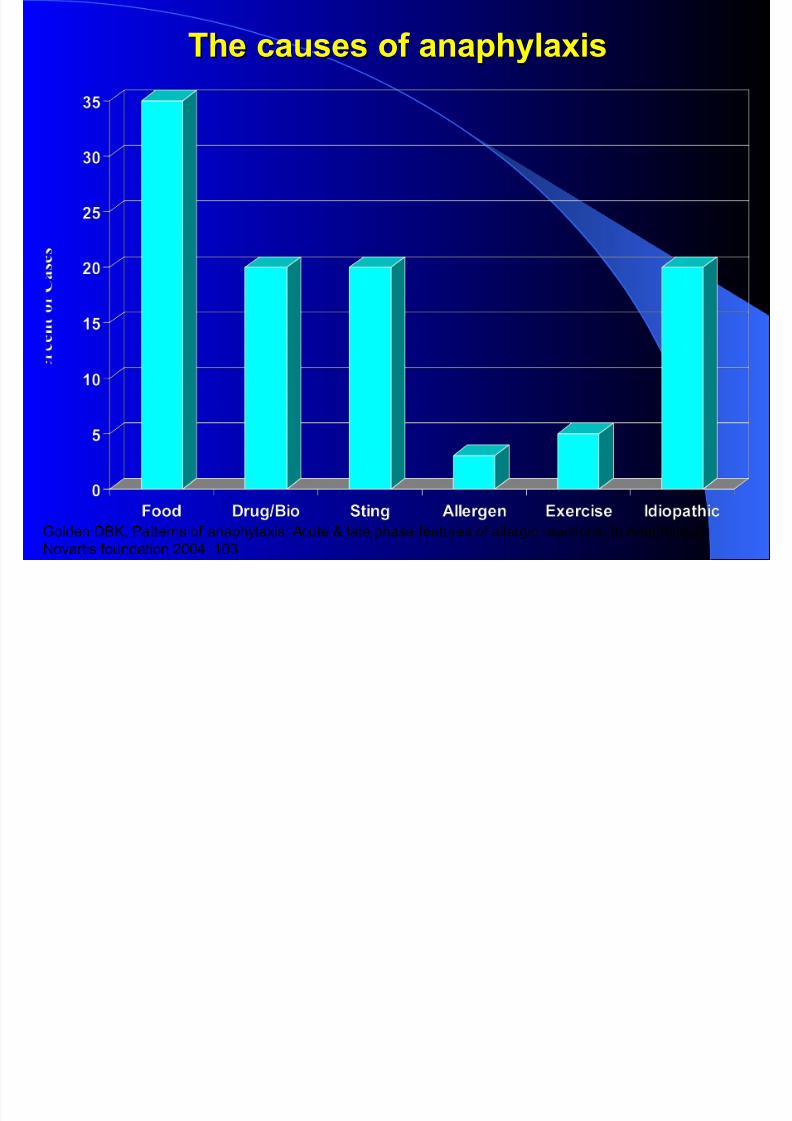
'he causes of anaphylaxis'he causes of anaphylaxis
Golden DBK, Patterns of anaphylaxis: Acute & late phase features of allergic reactions. In Anaphylaxis.Noartis foundation !""#: $"%
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 12/48
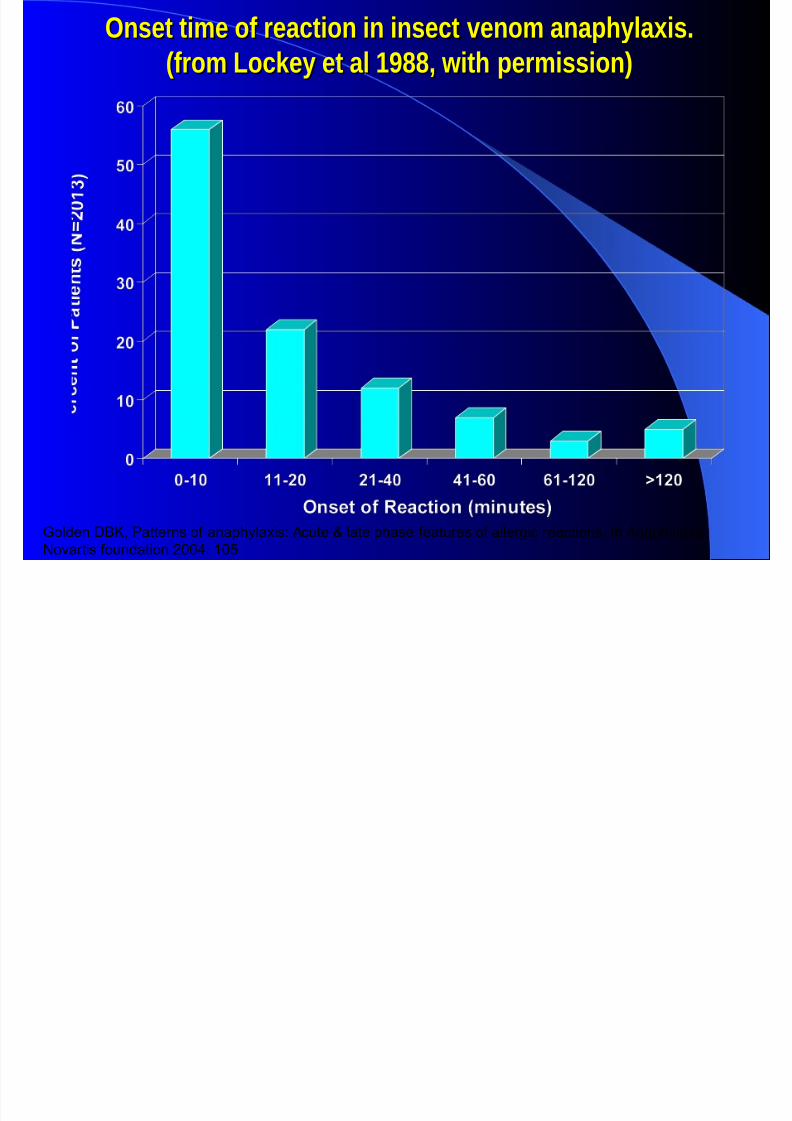
;nset ti3e of reaction in insect veno3 anaphylaxis.;nset ti3e of reaction in insect veno3 anaphylaxis.
&fro3 <oc2ey et al 1*77) with per3ission,&fro3 <oc2ey et al 1*77) with per3ission,
Golden DBK, Patterns of anaphylaxis: Acute & late phase features of allergic reactions. In Anaphylaxis.
Noartis foundation !""#: $"
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 13/48
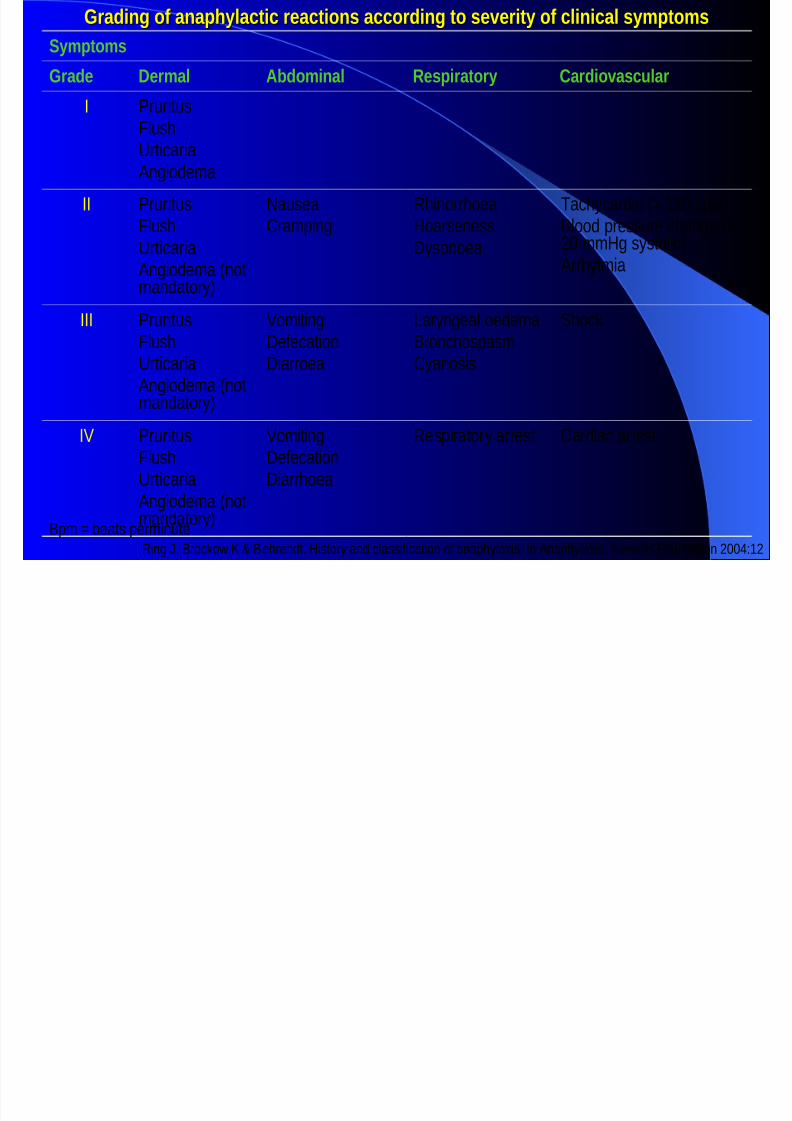
4rading of anaphylactic reactions according to severity of clinical sy3pto3s4rading of anaphylactic reactions according to severity of clinical sy3pto3s
'y3pto3s
4rade $er3al Abdo3inal =espiratory Cardiovascular
I uitu(
/lu(%ticaiaAngio&ema
II uitu(/lu(%ticaia
Angio&ema notman&ato)3
au(eaCam+ing
R%ino%oea'oa(ene(()(+noea
ac%)ca&ia 120 7+m3Bloo& +e((ue c%ange 20 mm'g ()(tolic3
A%)tmia
III uitu(/lu(%ticaia
Angio&ema notman&ato)3
8omitinge*ecationiaoea
a)ngeal oe&emaBonc%o(+a(mC)ano(i(
%oc!
I8 uitu(/lu(%ticaiaAngio&ema not
man&ato)3
8omitinge*ecationia%oea
Re(+iato) ae(t Ca&iac ae(t
B+m 7eat( +eminuteRing J, Boc!o" # $ Be%en&t. 'i(to) an& cla((i*ication o* ana+%)lai(. In Ana+%)lai(. oati( /oun&ation 2004:12
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 14/48
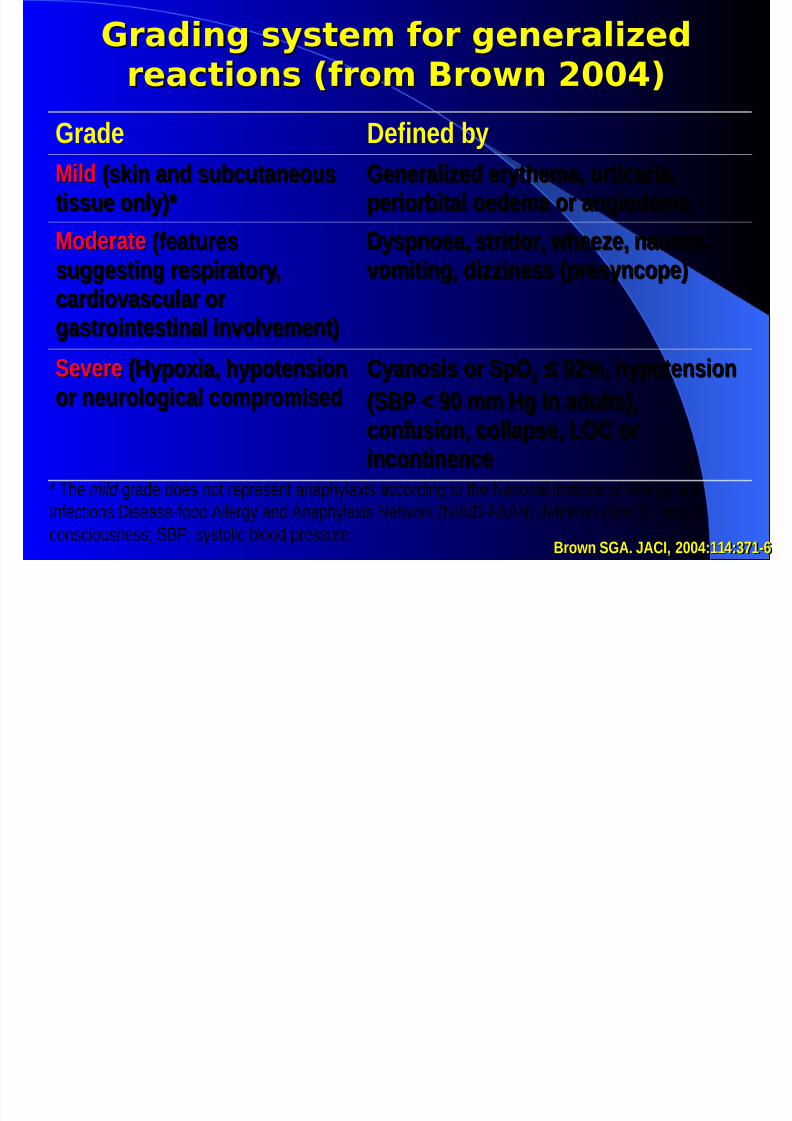
G*&d#% sys(e$ o* %ee*&l#.edG*&d#% sys(e$ o* %ee*&l#.ed
*e&/(#os 0*o$ 1*ow 23345*e&/(#os 0*o$ 1*ow 23345
4rade $efined byMildMild &s2in and subcutaneous&s2in and subcutaneous
tissue only,>tissue only,>4enerali9ed erythe3a) urticaria)4enerali9ed erythe3a) urticaria)
periorbital oede3a or angiode3a periorbital oede3a or angiode3a
ModerateModerate &features&features
suggesting respiratory)suggesting respiratory)cardiovascular orcardiovascular or
gastrointestinal involve3ent,gastrointestinal involve3ent,
$yspnoea) stridor) whee9e) nausea)$yspnoea) stridor) whee9e) nausea)
vo3iting) di99iness &presyncope,vo3iting) di99iness &presyncope,
'evere'evere &ypoxia) hypotension&ypoxia) hypotension
or neurological co3pro3isedor neurological co3pro3ised
Cyanosis or 'p;Cyanosis or 'p; @ *6) hypotension@ *6) hypotension
&'5 B *" 33 g in adults,)&'5 B *" 33 g in adults,)confusion) collapse) <;C orconfusion) collapse) <;C or
incontinenceincontinence< %e mild ga&e &oe( not e+e(ent ana+%)lai( acco&ing to t%e ational In(titute o* Alleg) an&
In*ection( i(ea(e-*oo& Alleg) an& Ana+%)lai( et"o! IAI-/AA3 &e*inition Bo 23, lo(( o*
con(ciou(ne((; B, ()(tolic 7loo& +e((ue.rown '4A. ACI) ""0:110:!81+rown '4A. ACI) ""0:110:!81+

7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 15/48
A&"hyl&'#s /& 6e &(&lA&"hyl&'#s /& 6e &(&l
e able to recogni9e the sy3pto3s
%now and avoid the triggers
ave an e3ergency action plan
Dreat it pro3ptly and appropriately
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 16/48
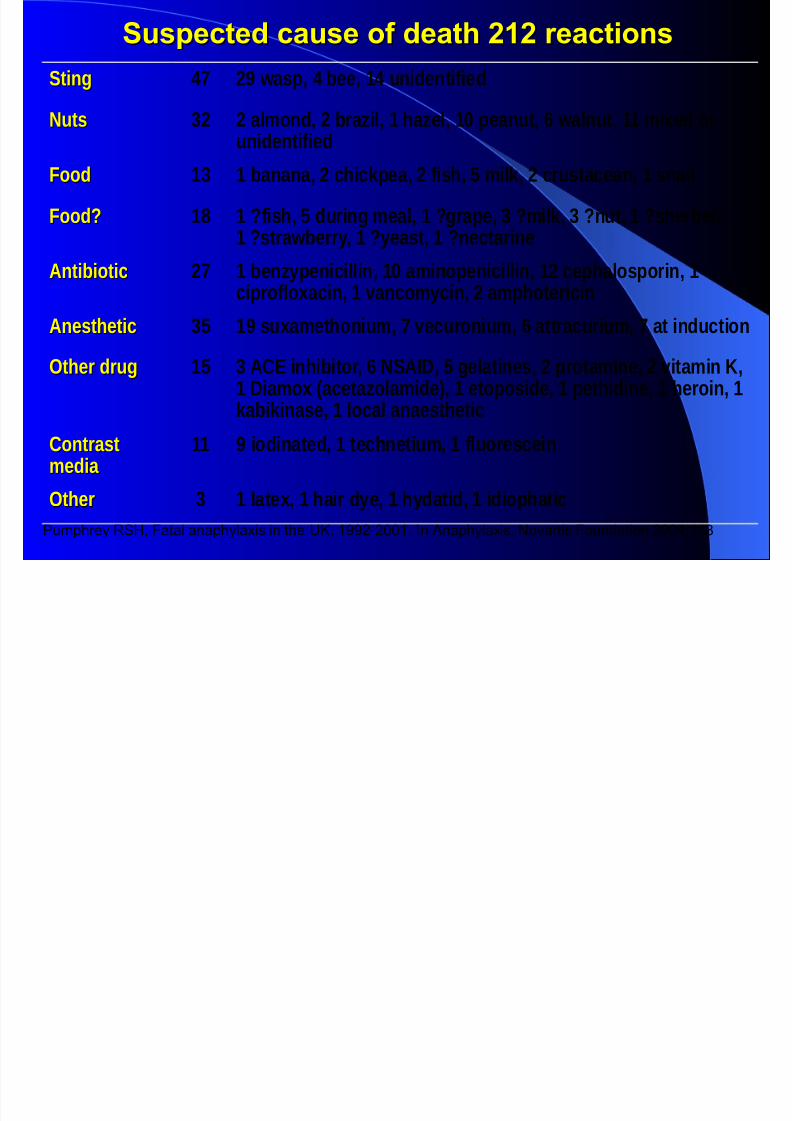
Suspected cause of death 696 reactionsSuspected cause of death 696 reactions
'ting'ting 08 * wasp) 0 bee) 10 unidentified
EutsEuts ! al3ond) bra9il) 1 ha9el) 1" peanut) + walnut) 11 3ixed orunidentified
oodood 1! 1 banana) chic2pea) fish) - 3il2) crustacean) 1 snail
ood?ood? 17 1 ?fish) - during 3eal) 1 ?grape) ! ?3il2) ! ?nut) 1 ?sherbet)1 ?strawberry) 1 ?yeast) 1 ?nectarine
AntibioticAntibiotic 8 1 ben9ypenicillin) 1" a3inopenicillin) 1 cephalosporin) 1ciprofloxacin) 1 vanco3ycin) a3photericin
AnestheticAnesthetic !- 1* suxa3ethoniu3) 8 vecuroniu3) + attracuriu3) 8 at induction
;ther drug;ther drug 1- ! AC# inhibitor) + E'AI$) - gelatines) prota3ine) vita3in %)
1 $ia3ox &aceta9ola3ide,) 1 etoposide) 1 pethidine) 1 heroin) 12abi2inase) 1 local anaesthetic
ContrastContrast3edia 3edia
11 * iodinated) 1 technetiu3) 1 fluorescein
;ther;ther ! 1 latex) 1 hair dye) 1 hydatid) 1 idiophatic
Pu'phrey ()*, +atal anaphylaxis in the K, $--!!""$. In Anaphylaxis. Noartis +oundation !""#:$$/
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 17/48
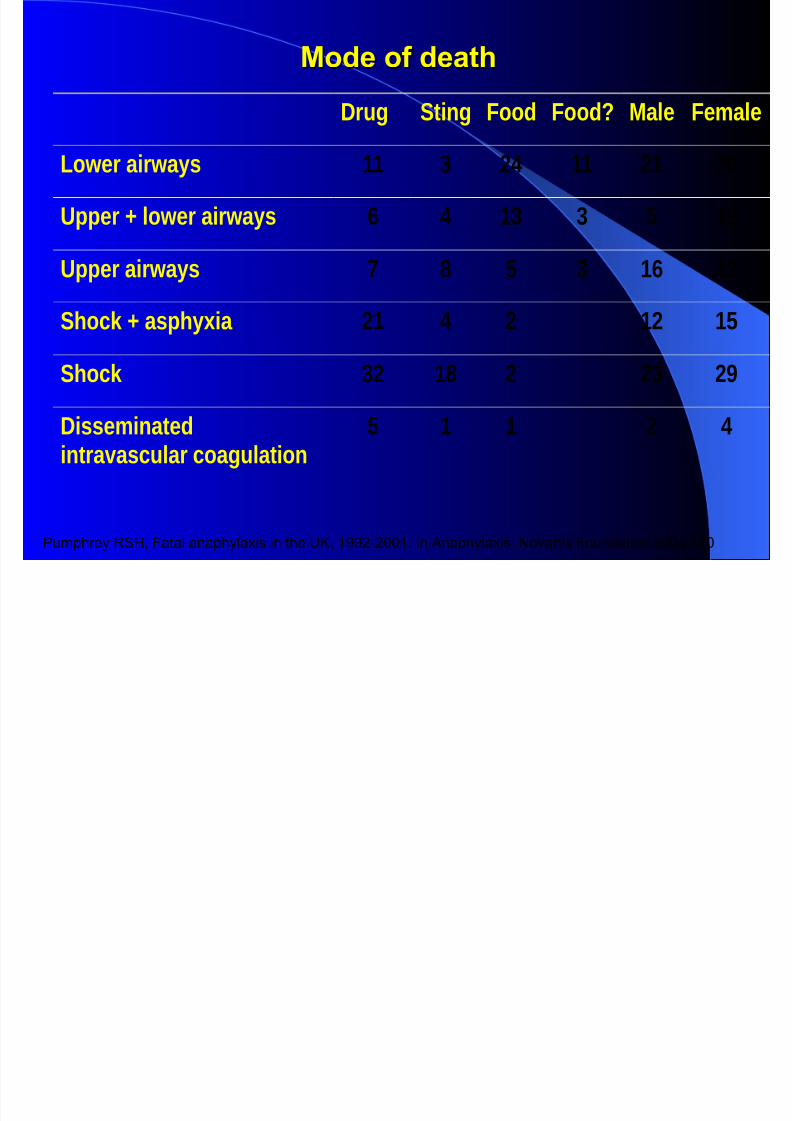
"ode of death"ode of death
$rug 'ting ood ood? Male e3ale
<ower airways 11 ! 0 11 1 +
Upper F lower airways + 0 1! ! - 1*
Upper airways 8 7 - ! 1+ 1
'hoc2 F asphyxia 1 0 1 1-
'hoc2 ! 17 ! *
$isse3inatedintravascular coagulation
- 1 1 0
Pu'phrey ()*, +atal anaphylaxis in the K, $--!!""$. In Anaphylaxis. Noartis +oundation !""#:$!"
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 18/48
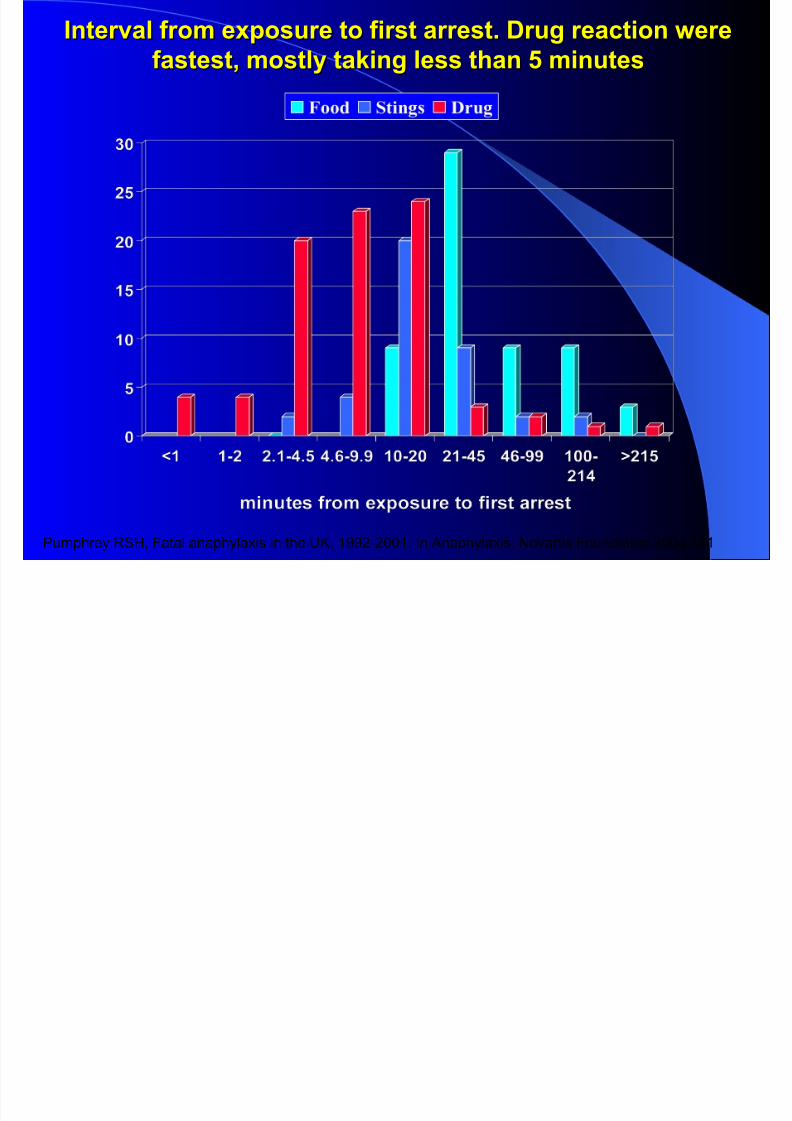
Interval from exposure to first arrest0 Drug reaction 2ereInterval from exposure to first arrest0 Drug reaction 2ere
fastest- mostly ta$ing less than ? minutesfastest- mostly ta$ing less than ? minutes
Pu'phrey ()*, +atal anaphylaxis in the K, $--!!""$. In Anaphylaxis. Noartis +oundation !""#:$!$

7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 19/48
7LINI7AL 8EAT9RES7LINI7AL 8EAT9RES

7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 20/48
A&"hyl&'#s sy$"(o$sA&"hyl&'#s sy$"(o$s
M;UD itching swelling of lips andor tongue
D=;AD itching) tightness) closure) hoarseness
'%IE itching) hives) redness) swelling 4UD vo3iting) diarrhea) cra3ps
<UE4 shortness of breath) cough) whee9e
#A=D wea2 pulse) di99iness) passing out
E#U=; headache) visual loss) loss of
consciousness) incontinence) confusion
8*eue/y o o//u**e/e o8*eue/y o o//u**e/e o
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 21/48
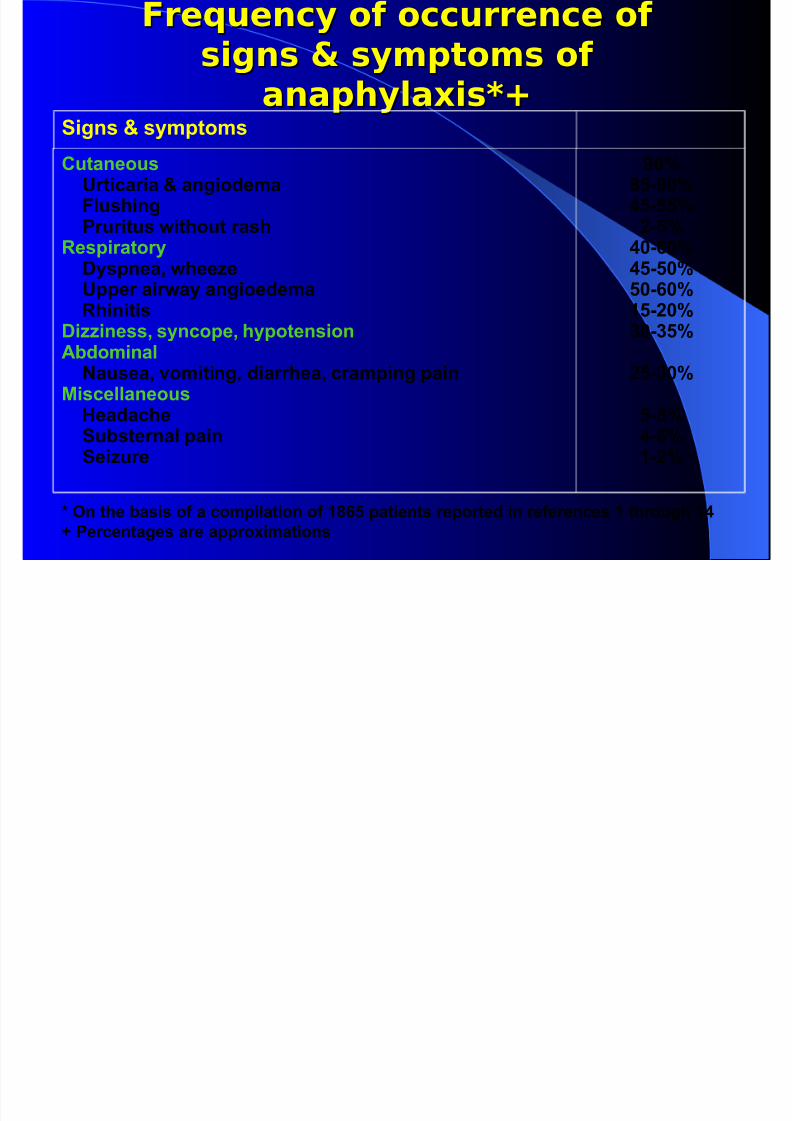
8*eue/y o o//u**e/e o8*eue/y o o//u**e/e os#%s ; sy$"(o$s os#%s ; sy$"(o$s o
&&"hyl&'#s<=&&"hyl&'#s<=
Signs B symptomsCutaneous Urticaria B angiodema Flushing )ruritus 2ithout rash!espiratory
Dyspnea- 2hee/e Upper air2ay angioedema !hinitisDi//iness- syncope- hypotensionA1dominal &ausea- vomiting- diarrhea- cramping pain
"iscellaneous Headache Su1sternal pain
Sei/ure
7<?.78?.??6.?
87.=7
8?.?7?7.=79?.67:7.:?
6?.:7
?.<8.=9.6
E (n the 1asis of a compilation of 9<=? patients reported in references 9 through 98
)ercentages are approximations
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 22/48
DIAGNOSISDIAGNOSIS
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 23/48
DIA5&(SIS (F A&A)H*+A,ISDIA5&(SIS (F A&A)H*+A,IS
Clinical diagnosis 1ased on clinical presentation andexposure history
Flushing and tachycardia are invaria1ly present- other
cutaneous symptoms 3hives- itch4 may 1e a1sent
Anaphylaxis may 1e difficult to diagnose- especially 2hen
patients present 2ith 1radycardia 3instead of tachycardia-
2hich is usual4
Gery rarely- patients present only 2ith profound hypotension0
'he exposure to some inciting event is one $ey to the
diagnosis in this rare circumstance
0ie1er'an P0 et al. 2 Allergy 3lin I''unol !""4$$:)#/%!%

7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 24/48
DIA5&(SIS (F A&A)H*+A,ISDIA5&(SIS (F A&A)H*+A,IS3contd43contd4
Careful history to identify possi1le causesCareful history to identify possi1le causes
Can 1e confirmed 1y an elevated serum tryptase levelCan 1e confirmed 1y an elevated serum tryptase level
.. specific for mast cell degranulationspecific for mast cell degranulation
.. remains elevated for up to = hoursremains elevated for up to = hours
.. may not 1e elevated- especially inmay not 1e elevated- especially in food allergyfood allergy
!efer to allergist for specific testing!efer to allergist for specific testing
h l # # h# hl l#k l hA h l # # h# hl l#k l h
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 25/48
A&"hyl&'#s #s h#%hly l#kely whe &yA&"hyl&'#s #s h#%hly l#kely whe &y
oe o (he ollow#% > /*#(e*#& &*eoe o (he ollow#% > /*#(e*#& &*e
ul?lledul?lled @@
1. Acute onset of an illness &3inutes to several hours, withinvolve3ent of the s2in) 3ucosal tissue) or both &eg)generali9ed hives) pruritus or flushing) swollen lips
tongueuvula, AE$ AD <#A'D ;E# ; D# ;<<;GIE4
a. =espiratory co3pro3ise &eg) dyspnea) whee9ebronchospas3)stridor) reduce 5#) hypoxe3ia
b. =educed 5 or associated sy3pto3s of endorgan dysfunction&eg) hypotonia Hcollapse) syncope) incontinence,
am+(on ', et al. JACI 2006;11=:>91-2
A&"hyl&'#s #s h#%hly l#kely whe &yA&"hyl&'#s #s h#%hly l#kely whe &y

7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 26/48
A&"hyl&'#s #s h#%hly l#kely whe &yA&"hyl&'#s #s h#%hly l#kely whe &y
oe o (he ollow#% > /*#(e*#& &*eoe o (he ollow#% > /*#(e*#& &*e
ul?lledul?lled 22
. Dwo or 3ore of the following that occur rapidly afterexposure to a likely allergen for that patient &3inutes toseveral hours,:
a. Involve3ent of the s2in3ucosal tissue &eg) generali9ed hives)
itcflush) swollen lipstongueuvula,
b. =espiratory co3pro3ise &eg) dyspnea) whee9ebronchospas3)stridor) reduced 5#) hypoxe3ia
c. =educed 5 or associated sy3pto3s of endorgan dysfunction
&eg) hypotonia Hcollapse) syncope) incontinence,d. 5ersistent gastrointestinal sy3pto3s &eg) cra3py abdo3inal
pain) vo3iting,
A h l # # h# hl l#k l hA h l # # h# hl l#k l h
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 27/48
A&"hyl&'#s #s h#%hly l#kely whe &yA&"hyl&'#s #s h#%hly l#kely whe &y
oe o (he ollow#% > /*#(e*#& &*eoe o (he ollow#% > /*#(e*#& &*e
ul?lledul?lled >>
!. =educed 5 after exposure to known allergen for that patient &3inutes several hours,
a. Infants and children: lowsystolic 5 &age specific, or greater
than !"6 decrease in systolic 5>b. Adults: systolic 5 of less than *" 33 g or greater than !"6
decrease fro3 that personJs baseline
?/, ea! e+iato) *lo"; B, 7loo& +e((ue
< o" ()(tolic 7loo& +e((ue *o c%il&en i( &e*ine& a( le(( t%an =0 mm 'g *om 1 mont% to 1 )ea, le((
t%an =0 mm '@ 2 age3 *om 1 to 10 )ea(, an& le(( t%an 90 mm 'g *om 11 to 1= )ea(.

7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 28/48
DIFF%!%&'IA+ DIA5&(SIS (FDIFF%!%&'IA+ DIA5&(SIS (F
A&A)H*+A,ISA&A)H*+A,IS 5asoagal reactions
+lushing
6astocytosis
3arcinoid syndro'e
*yperentilation syndro'e
Glo1us hystericus
*ereditary angioede'a
7ther types of shoc8, eg. cardiogenic, septic )co'1roid poisoning
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 29/48
TREATMENTTREATMENT
E ( E$e*%e/y $&&%e$e( o
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 30/48
E$e*%e/y $&&%e$e( oE$e*%e/y $&&%e$e( o
&&"hyl&'#s&&"hyl&'#s
1. to+ a&mini(tation o* +eci+itant, a((e(( eaction (eeit) an& teatacco&ingl):
Call for assistance
Adrenaline I.3 &lateral thigh, "."1 3g2g up to ".- 3g
i.v access<ie flatelevate legs if tolerated
igh flow oxygen) airwayventilation support if needed
I K5;D#E'IL# A<';:Additional wide bore I.v access &I.e 104 or 1+4 in adults, for nor3al
saline infusion
i.v nor3al saline bolus " 3<2g over 1 3in under pressure
Bo"n, @A. ?meg De& Au(tala(ia. 2006;1E:155-16=
E ( h l #E ( h l #

7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 31/48
. If there is inadeuate response) an i33ediate life threat) or deterioration:
And consider also:• ypotension
o =epeat nor3al saline boluses 10-20 mF!g a( nee&e&, u+ to 50mF!g total oe t%e *i(t
>0 mino i.v atropine 0.02 mgF!g i* (eee 7a&)ca&ia minimum &o(e 0.1 mg3
o i. vasopressors to oecome a(o&ilation a(o+e((in 10-40 unit( in a&ult(, ometaaminol 2-10 mg in a&ult(3<. or anaphylactic cardiac arrest, a+i& e(calation to
high dose adrenaline >-53 mg ee) 2-> min3 mig%t 7e e**ectieo I. glucagonphosphodiesterase inhibitorsballon pu3p i* β-7loc!e& o %eat *ailue:
@lucagon &o(e in a&ult(: loa& "it% 1-5 mg oe 5 min, *ollo"e& 7) 5-15 µgFmin<• ronchospas3
o Continuou( salbuta3ol ne7uliGe( o continuou( actuation( o* metee& &o(e in%ale intoentilation cicuit i* intu7ate&3
o i.v. hydrocortisone 5 mgF!g 6 %oul) *ollo"e& 7) oal prednisone 1 mgF!g ma. 50 mg3
*o 4 &a)(• Upper airway obstruction
o e7uliGe& a&enaline 5 mg in H m, I.e. 5 m o* 1:1000 ma) +oi&e (ome elie*o e+ae *o (ugical
tat an I. adrenalin infusion a( +e %o(+ital gui&eline(F+otocolR
Re+eat i.m a&enalin ee) >-5 min a( nee&e&
E$e*%e/y $&&%e$e( o &&"hyl&'#sE$e*%e/y $&&%e$e( o &&"hyl&'#s
Bo"n, @A. ?meg De& Au(tala(ia. 2006;1E:155-16=
E$e*%e/y $&&%e$e( o &&"hyl&'#sE$e*%e/y $&&%e$e( o &&"hyl&'#s
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 32/48
> (1serve for an adeuate period and arrange appropriate follo2 up;(1serve for an adeuate period and arrange appropriate follo2 up;i0 (1serve for a minimum of 8 h after the resolution of all sy'pto's
and signs
• 9a8e 1lood for seru' 'ast cell tryptase on arrial, $ h after arrialand prior to discharge.• Ad'it longer oernight; those <ith seere reactions, a history of
lifethreatening reactions or poorly controlled• Asth'a, and those <ho present late in the eening
ii0 (utpatient follo2 up 1y a specialist allergist is reco''ended for allthose <ith 'oderateseere reactions, and <ith 'ild reactions tofood if the patient also has asth'a
Prior to discharge allergen avoidance measures including "edicAlert;. =nsure that an alert is placed in hospital >practicerecords>co'puter syste', and ensure that your referralletter>su''ary contains a detailed record of reaction features &ti'ing, possi1le precipitants and ti'es of exposure
iii0 Arrange for an %pi)en- demonstrate correct use 2ith an %pi)en'rainer and provide a <ritten action plan http:>><<<.allergy.org.au;
if there is a significant ris8 of reexposure and outpatient follo< up<ill 1e delayed
E$e*%e/y $&&%e$e( o &&"hyl&'#sE$e*%e/y $&&%e$e( o &&"hyl&'#s
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 33/48
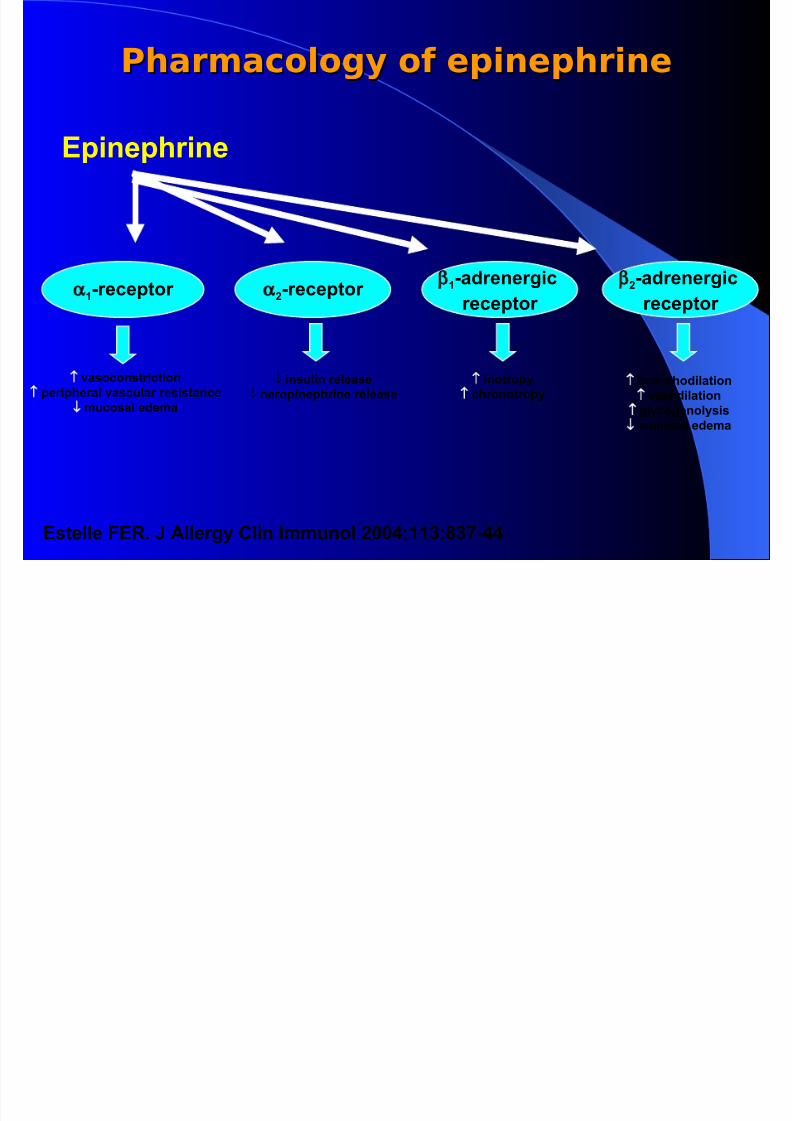
Ph&*$&/olo%y o e"#e"h*#ePh&*$&/olo%y o e"#e"h*#e
%pinephrine
9.receptor 6.receptor 9.adrenergic
receptor
6.adrenergic
receptor
↑
vasoconstriction
↑
peripheral vascular resistance↓
mucosal edema
↓ insulin release
↓ neropinephrine release
↑ inotropy
↑
chronotropy
↑ 1ronchodilation
↑
vasodilation↑ glycogenolysis
↓ mucosal edema
%stelle F%!0 # Allergy Clin Immunol 6778>99:;<:.88
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 34/48
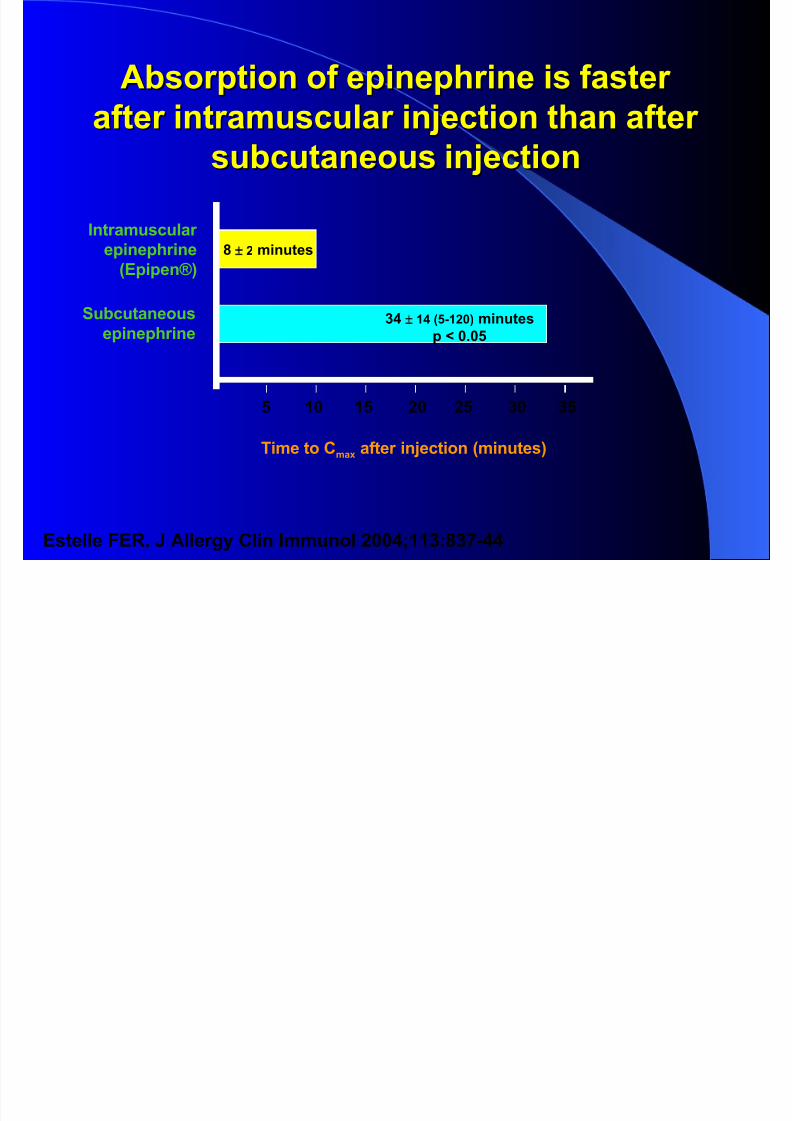
A1sorption of epinephrine is fasterA1sorption of epinephrine is faster
after intramuscular inJection than afterafter intramuscular inJection than after
su1cutaneous inJectionsu1cutaneous inJection
%stelle F%!0 # Allergy Clin Immunol 6778>99:;<:.88
:8±
98 3?.9674 minutes
p 707?
? 97 9? 67 6? :7 :?
<± 6 minutes
'ime to Cmax after inJection 3minutes4
Intramuscular
epinephrine
3%pipenL4
Su1cutaneous
epinephrine
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 35/48
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 36/48
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 37/48
PREVENTIONPREVENTION
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 38/48
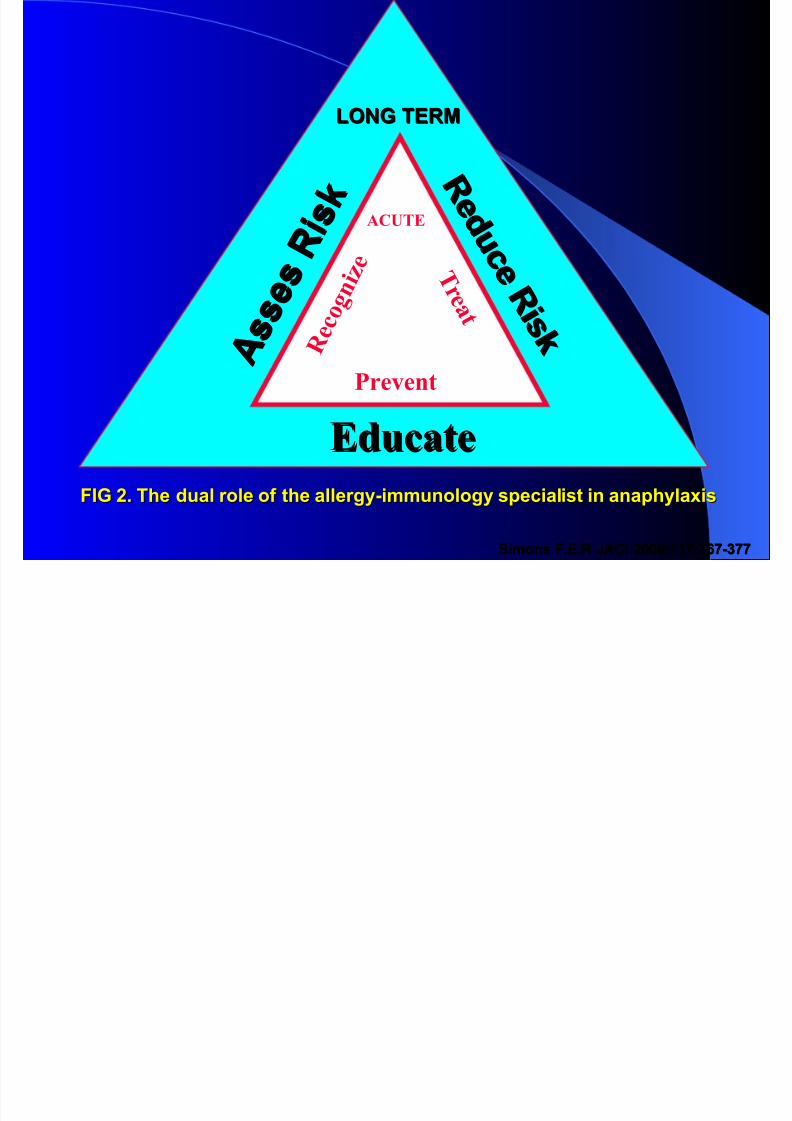
+(&5 '%!"+(&5 '%!"
A s s e s ! i s $
A s s e s
! i s $
! e d u
c e ! i s $
! e d u
c e ! i s $
EducateEducate
R e c o g n i z e
ACUTE
T r e a t
Prevent
FI5 60 'he dual role of the allergy.immunology specialist in anaphylaxisFI5 60 'he dual role of the allergy.immunology specialist in anaphylaxis
Simons F0%0! #ACI 677=>99;:=.:Simons F0%0! #ACI 677=>99;:=.:
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 39/48
Mhy is follo2 up is needed NMhy is follo2 up is needed N
Anaphylaxis can occur repeatedly
'he trigger need to 1e confirmed
+ong.term preventive strategies
need to 1e implemented
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 40/48
Edu/&(#o o &&"hyl&'#sEdu/&(#o o &&"hyl&'#s
Individuals and their fa3ilies
Caregivers
ealth case professional &doctors) nurses,
irst respondent
#3ergency 3edical services
Deachers coaches) child care providers
ood industries) restaurant) law 3a2ers
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 41/48
90 )rior History . Identification90 )rior History . Identification
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 42/48
60 "edical alert 1rachelet60 "edical alert 1rachelet99
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 43/48
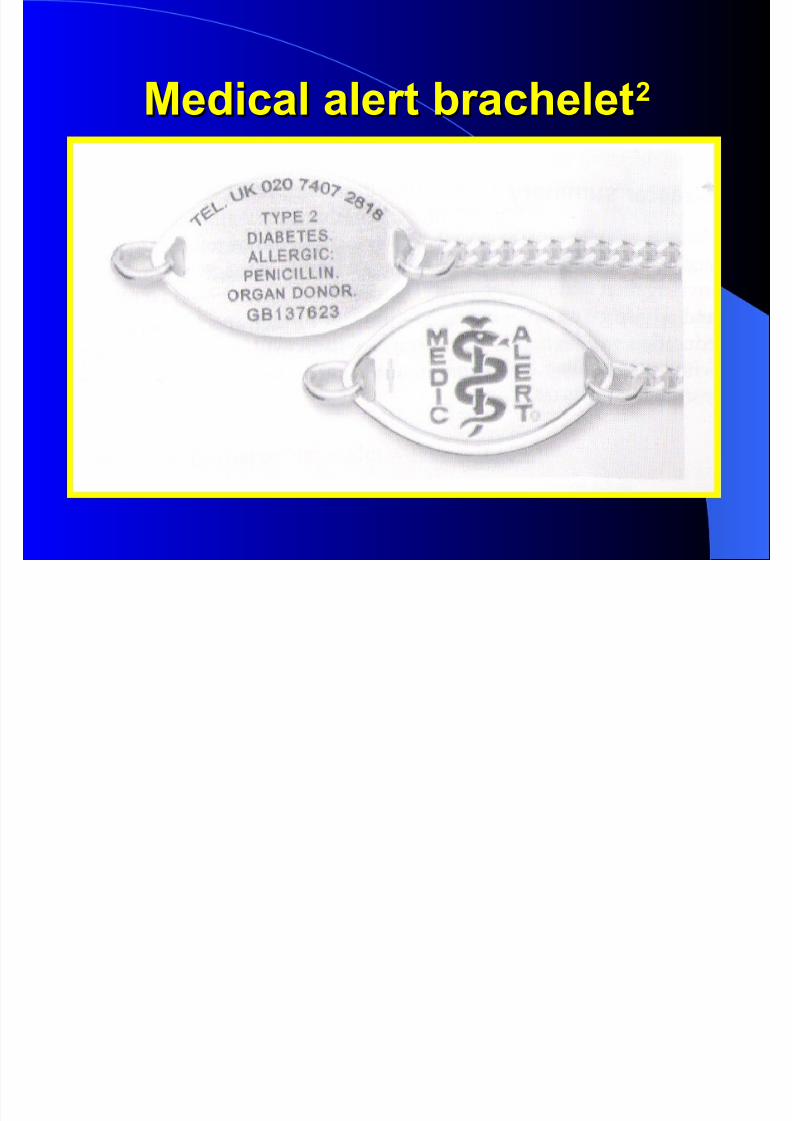
"edical alert 1rachelet"edical alert 1rachelet66
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 44/48
)revention)revention99
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 45/48
:0 %mergency Kit:0 %mergency Kit
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 46/48
)revention)revention66
)harmacologic prophylaxis ; !C"
Immunotherapy
Hidden allergens- cross reactivity Maiting :7 minutes after inJections
S l Ch f C dS l Ch f C d

7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 47/48
Sample Chef CardSample Chef Card'o the Chef;'o the Chef;
MA!&I&5O I am allergic to peanuts0 In order to avoid a life.threateningreaction- I must avoid the follo2ing ingredients;
Artificial nuts
Peer nuts
Cold pressed- expelled- or extruded peanut oil
5round nuts
"andelonas
"ixed nuts
"on$ey nuts
&ut pieces
)eanut
)eanut 1utter )eanut flour
)lease ensure any utensils B euipment used to prepare my meal- as
2ell as prep surfaces- are thoroughly cleaned prior to use0 'han$s for
your cooperation
"uno/0 Anaphylaxis 67780 Miley- Chichester0 )0 6=?.?
7/25/2019 Anafilaksis (PIT 2008)
http://slidepdf.com/reader/full/anafilaksis-pit-2008 48/48