An Introduction to Vestibular Rehabilitation - c.ymcdn.com · An Introduction to Vestibular...
61
An Introduction to Vestibular Rehabilitation Jennifer Fay, PT, DPT, NCS Neurologic Clinical Specialist Vestibular Rehabilitation Rusk Institute NYU Langone Medical Center
Transcript of An Introduction to Vestibular Rehabilitation - c.ymcdn.com · An Introduction to Vestibular...
An Introduction to Vestibular
Rehabilitation
Jennifer Fay, PT, DPT, NCS
Neurologic Clinical Specialist
Vestibular Rehabilitation
Rusk Institute
NYU Langone Medical Center
Objectives: •Describe Vestibular System Function, Anatomy
and physiology
•Identify evaluation components
•Identify common causes of dizziness
•Demonstrate Vestibular treatment and exercises
•BPPV testing and treatment.
•Considerations for Concussion
© Jennifer Fay, PT, DPT, NCS
Vestibular Anatomy
and Physiology
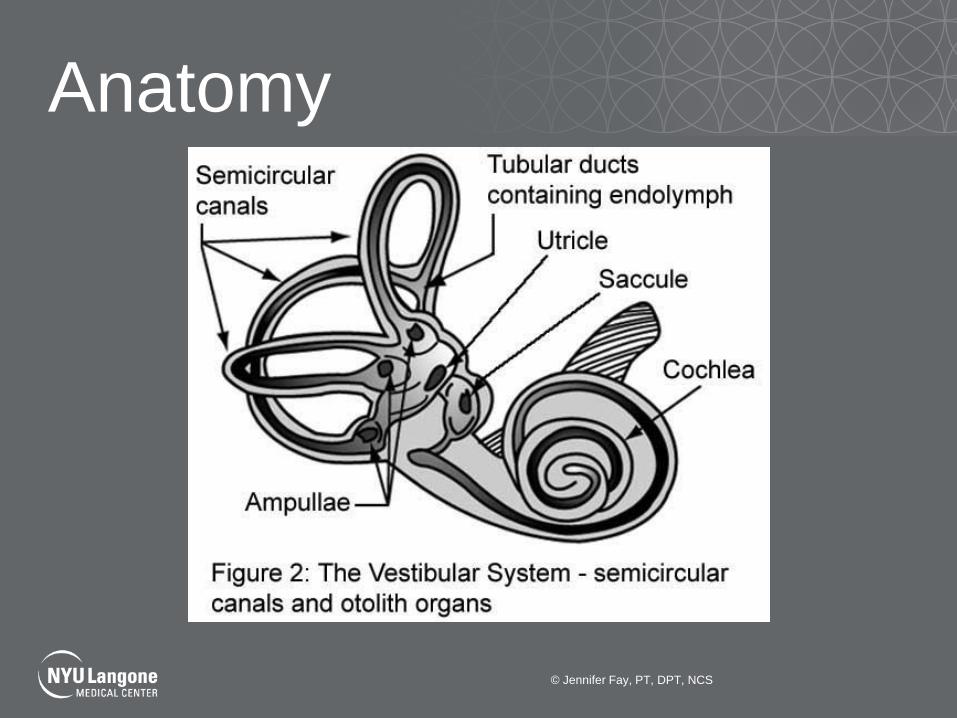
Anatomy
© Jennifer Fay, PT, DPT, NCS

Semicircular Canals
•Filled with endolymph with a density slightly greater
than water and moves freely within each canal in
response to the direction of head rotation.
(Schubert MC 2004)
•Act in pairs.
•Each semicircular canal is sensitive to motion in
the plane of that canal.
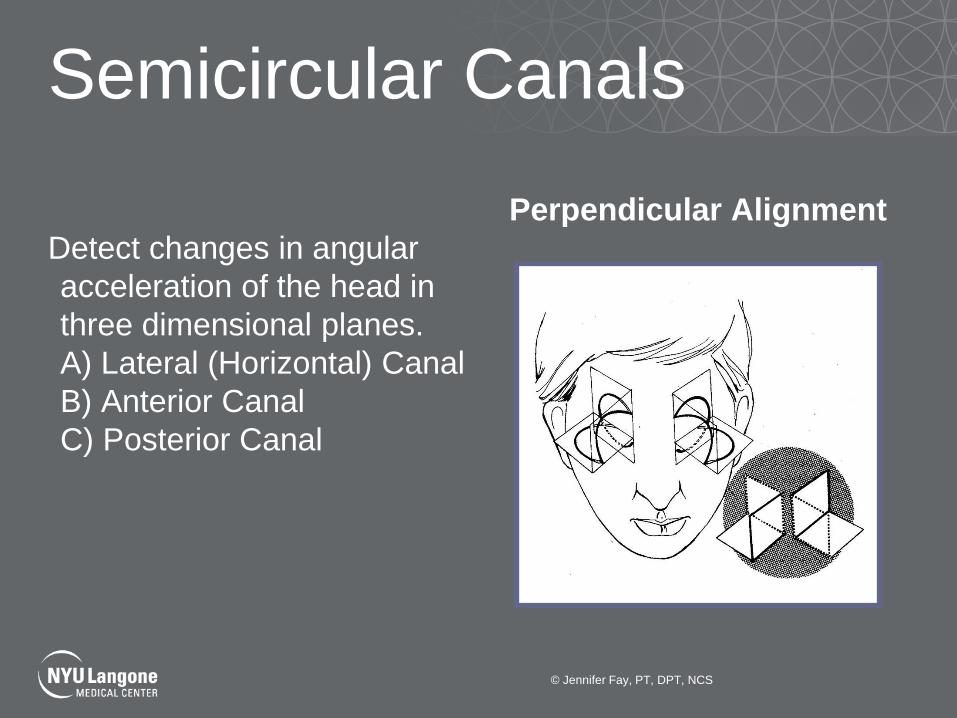
Semicircular Canals
Detect changes in angular
acceleration of the head in
three dimensional planes.
A) Lateral (Horizontal) Canal
B) Anterior Canal
C) Posterior Canal
Perpendicular Alignment
© Jennifer Fay, PT, DPT, NCS

Semicircular Canal
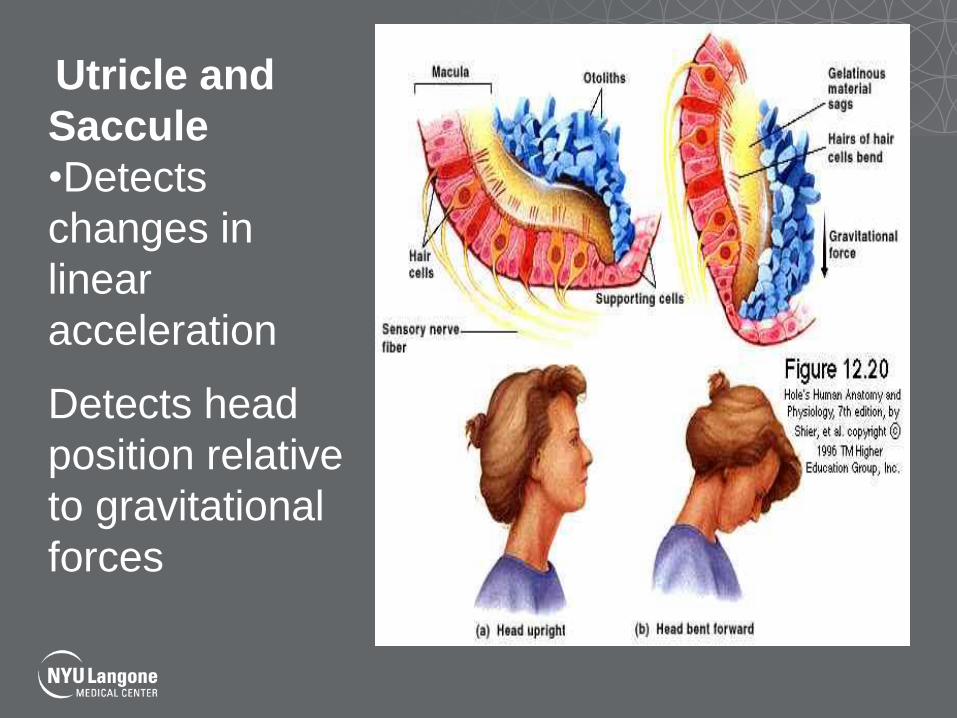
Utricle and
Saccule
•Detects
changes in
linear
acceleration
Detects head
position relative
to gravitational
forces
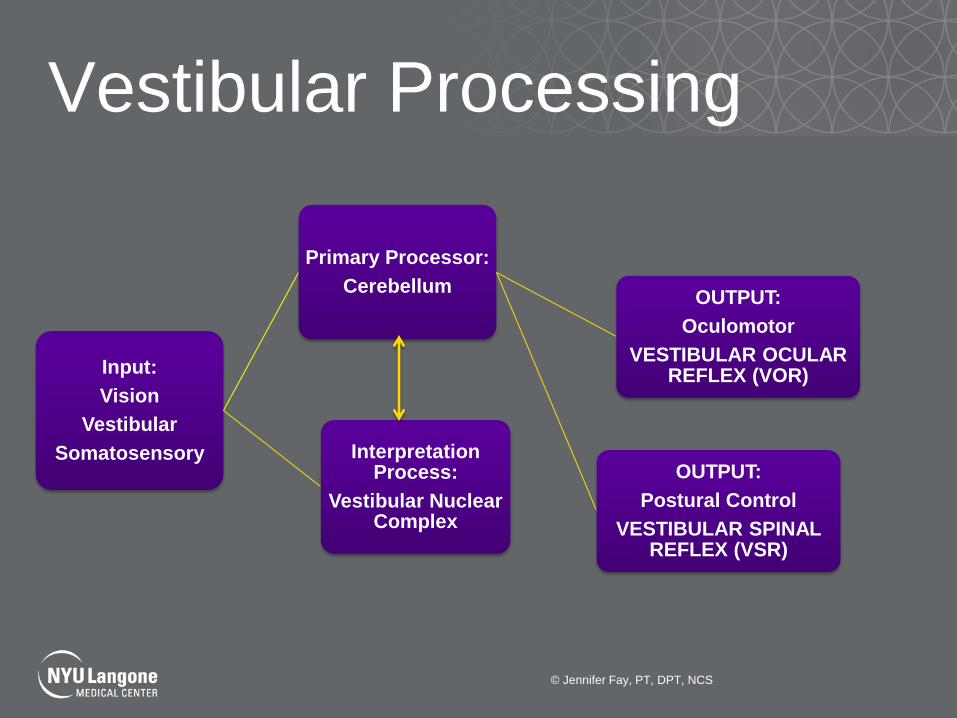
Vestibular Processing
Input:
Vision
Vestibular
Somatosensory
Primary Processor:
Cerebellum
OUTPUT:
Postural Control
VESTIBULAR SPINAL REFLEX (VSR)
OUTPUT:
Oculomotor
VESTIBULAR OCULAR REFLEX (VOR)
Interpretation Process:
Vestibular Nuclear Complex
© Jennifer Fay, PT, DPT, NCS

Vision Somatosensory
Vestibular
BALANCE
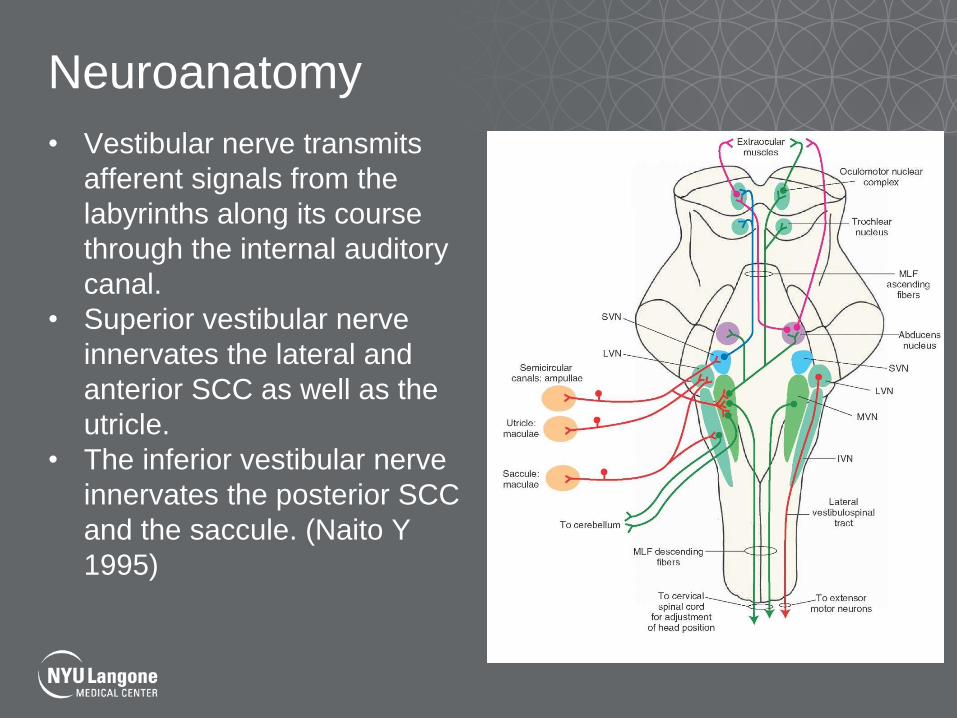
Neuroanatomy
• Vestibular nerve transmits
afferent signals from the
labyrinths along its course
through the internal auditory
canal.
• Superior vestibular nerve
innervates the lateral and
anterior SCC as well as the
utricle.
• The inferior vestibular nerve
innervates the posterior SCC
and the saccule. (Naito Y
1995)
Vestibular ocular reflex
© Jennifer Fay, PT, DPT, NCS

Vestibulo-occular reflex •As the head is rotated to the left,
the left vestibular nerve is
stimulated.
•The right vestibular nerve is
inhibited.
•This results in an excitation of
the right abducens nerve fibers
innervating the right lateral rectus
muscle and the left oculomotor
nerve fibers innervating the left
medial rectus muscle.

Vestibular spinal reflex
© Jennifer Fay, PT, DPT, NCS
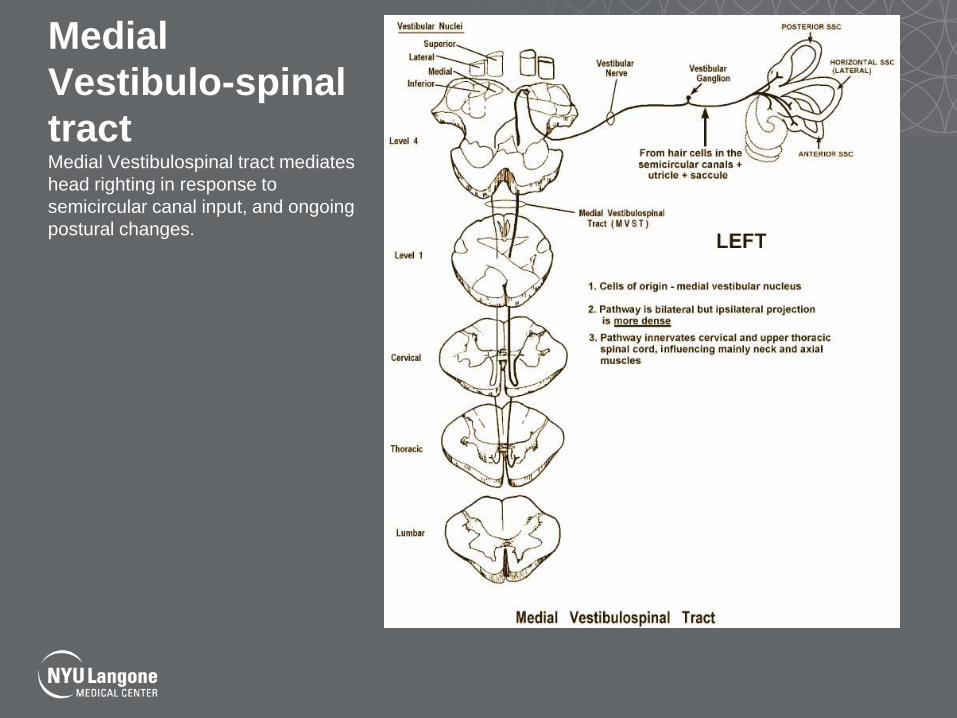
Medial
Vestibulo-spinal
tract Medial Vestibulospinal tract mediates
head righting in response to
semicircular canal input, and ongoing
postural changes.

Lateral
Vestibulospinal
Tract Lateral vestibulospinal tract receives
majority of its input from otoliths and
the cerebellum.
Generates antigravity postural control,
or protective extension in the lower
extremities in response to head
position changes.
Nystagmus
•The vestibular system is a balanced system.
•Effects of activity from one vestibular organ are balanced by
effects from the other.
•A vestibular imbalance will cause overstimulation on one
side and slow tonic deviation of the eyes away from that
side.
•The tonic nature of the movement induced by the vestibular
system causes this slow movement followed by a rapid or
saccadic return to be repeated over and over.
•**Nystagmus will always beat to the side of increased
neural activity**
•Named relative to the fast phase relative to the patient.
Peripheral Causes of Dizziness
•Benign Paroxysmal Positional Vertigo
•Vestibular neuritis/labyrinthitis
•Meniere’s Disease
•Ototoxicity (chemotherapy/IV antibiotics)
•Acoustic Neuroma
Central Causes of Dizziness
•Concussion
•Cerebrovascular disorders
•Migraine
•Multiple sclerosis
•Epilepsy
•Craniocervical junction disorders
•Neoplastic: primary, metastatic or paraneoplastic
•Inherited ataxias
•Pyschogenic
•Neurodegenerative disorders: parkinsonism, normal
pressure hydrocephalus
Concussion
•43 working definitions of concussion. Only one is evidence
based.
43rd Working Definition of Concussion
Concussion is:
• A change in brain function following a force to the
head,which may be accompanied by temporary loss of
consciousness, but is identified in awake individuals,with
measures of neurologic and cognitive dysfunction.
© Jennifer Fay, PT, DPT, NCS
Risk Factors for More Complicated Recovery
•Age
•Younger athletes had more complicated recovery
•Migraine History and Symptoms
•Prior history of migraine or migraine symptoms
post concussion
•History of Learning Disability
•Repetitive Concussion
•Gender
•Females had longer recovery
Dizziness following Concussion
•Prevalence Reported to occur in 23% to 81% of cases in first days after injury (Alsalaheen et al 2010)
•55% of concussed athletes report dizziness as an early symptom (Lovell 2004) •32% of 141 patients with mild TBI report dizziness after 5 years.
Aural Symptoms
•Ringing, pressure, fullness or hearing changes
•Patients with mixed central and peripheral vestibular
dysfunction recover more slowly and incompletely. (Brown
2006)
•Could also have labyrinthine concussion.
•Warrants referral to Otology or Neuro-otology
Postural Control
•43% of athletes report
balance dysfunction
following sports related
concussion. (Lowell
2004)
•May resolve more
quickly than other
symptoms following
concussion. (Catena
2011)

Space and Motion Sensitivity
•Problems •Walking in supermarket or
crowded places?
•Heights?
•Wide open spaces?
•Clinical Assessments: •VOR Cancellation
•SOT (conditions 3,6)
•DHI Items 4 and 12
•Increased dizziness with
surround moving
Vestibular Evaluation
© Jennifer Fay, PT, DPT, NCS
Subjective History
•Specific Questions
•Aural Symptoms
•Hearing loss, fullness
•Positioning Symptoms
•BPPV
•Motion Sensitivity
•Head
•Visual
•Balance
•Headaches-migraines?
•Photophobia and phonophobia
•Nausea/vomiting
•History of Concussion or ever hit their head?
Characterizations of Symptoms
•Temporal course:
•paroxysmal lasting seconds, minutes, hours, days, weeks
•OR continuous with exacerbation lasting seconds minutes, hours,
days, weeks
•Type of dizziness: vertigo, imbalance, lightheadedness, falls,
disorientation
•Nausea & vomiting, headaches, any of the “Ds”=diplopia, dysphagia,
dysarthria, dysmetria, asymmetric muscle weakness
•Onset of symptoms-spontaneous OR head motion or visual motion
provoked
•Hearing-involvement in the auditory system e.g. tinnitus, aural fullness,
progressive or fluctuant hearing loss
Clinical Exam:
•Oculomotor exam in room light
•Ocular motility (ROM)
•Convergence
•Nystagmus
•Saccades
•Smooth Pursuit
•VOR
•Head Thrust Test
•Dynamic Visual Acuity
Clinical Exam
•Oculomotor exam with vision blocked (frenzels or infrared)
•Spontaneous and gaze evoked nystagmus
•Post head shaking nystagmus
•BPPV
•Dix-Hallpike
•Balance Exam:
•Romberg
•EO, EC, Foam EO, Foam EC
•Sharpened Romberg EO, EC
•Ambulation
•Ambulation with Head Rotation
•Dynamic Gait Index/Functional Gait Assessment
•BESS Test for concussion
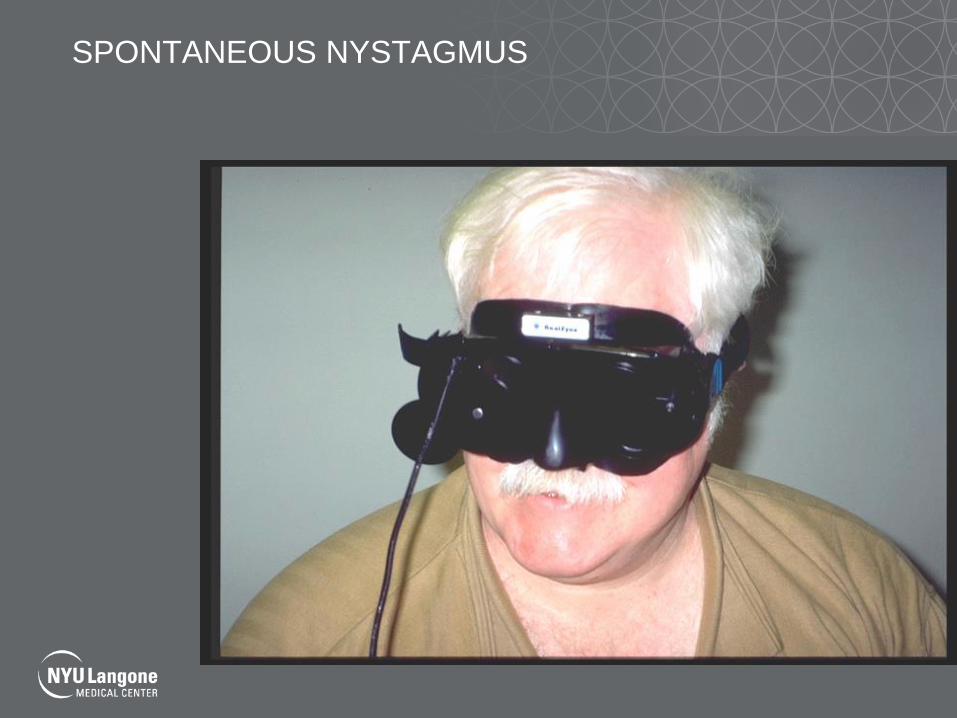
SPONTANEOUS NYSTAGMUS
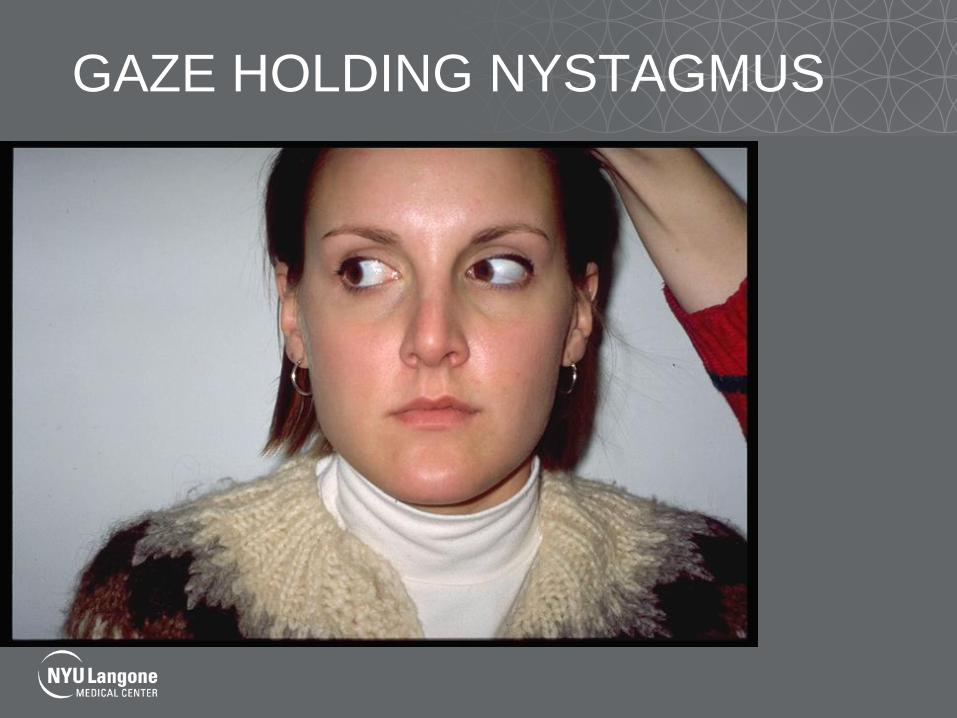
GAZE HOLDING NYSTAGMUS

RAPID HEAD THRUST
DYNAMIC VISUAL ACUITY

Balance Testing
© Jennifer Fay, PT, DPT, NCS

POSTUROGRAPHY
• Sensory Organization Test
Functional Gait Assessment
•Modification of the Dynamic Gait Index developed to improve reliability
and decrease the ceiling effect.
•Added gait with narrow base of support, ambulating backwards, and gait
with eyes closed.
© Jennifer Fay, PT, DPT, NCS

Ambulation with Head Turns
© Jennifer Fay, PT, DPT, NCS

TREATMENT
Principles of Treatment
•Habituation
•Adaptation –retinal slip
•Substitution
Habituation
•Asymmetry in labyrinth function results in “sensory
mismatch”.
•Repeated exposure to a provocative stimulus will
result in a reduction in the pathological response to
that treatment.
Adaptation
•Refers to long term changes that occur in response
of the vestibular system to input.
•In acute injury the gain of the VOR is reduced (eye
movement velocity is less than head movement
velocity).
•Resulting in retinal slip (blurred vision)
•Retinal slip causes an error signal resulting in a
change in the gain of the VOR.
Substitution
•Compensation for lack of vestibular function
through use of visual and somatosensory systems.
© Jennifer Fay, PT, DPT, NCS
Gaze Stability/VOR
•Have the patient focus on one letter and turn their
head as fast as they can while keeping letter in
focus and still.
•Progression:
•Duration
•Velocity
•Position
•Target distance
•Background
•Frequency

Vestibular-Ocular Reflex (VOR)
© Jennifer Fay, PT, DPT, NCS
Sensory Organization and Postural Control
•Static and Dynamic
Balance training: •Decreasing base of
support
•Perturbing visual and
somatosensory cues
•Head rotation
•Changing direction
•Stair climbing
•Dual task •Cognitive
•Manual
© Jennifer Fay, PT, DPT, NCS
100, 97, 94, 91
Recovery Depends On
•Central verses Peripheral
•Unilateral verses Bilateral
•Age
•Time from onset
•Comorbidities
•Use of medications (meclizine, antivert)
Vestibular Treatment
•Systematic monitoring throughout session of
symptoms
•Incorporate ocular motor training when needed
and/or make referrals
•Proceed at a slower rate with central injuries than
with peripheral injuries (“less is more”)
LAB
• Practice VOR
• Practice Sharpened Romberg with Eyes Closed
© Jennifer Fay, PT, DPT, NCS

Benign Paroxysmal
Positional Vertigo (BPPV)

BPPV
•Most common vestibular disorder in adults (Bhattacharyya,
Baugh et al. 2008)
•Most common cause of vertigo resulting from head trauma
(Fife and Giza 2013)
•“BPPV should always be considered in patients with head trauma
with complaints of positional vertigo.” (Fife and Giza 2013)
•Recurrence rates similar to idiopathic BPPV
Liu 2012:
•May take more maneuvers to achieve success
•More likely to be bilateral occurring in 25% vs 2% in idiopathic
•35% of patients with post-traumatic bppv were cured after one
maneuver vs. 85% in idiopathic bppv.
Benign Paroxysmal Positioning Vertigo (BPPV)
•Classic symptom:
•Brief (typically <1minute) episodes of vertigo
associated with changes in head position relative
to gravity
•Lying down-rising from horizontal orientation
•Rolling over in bed
•Bending over
•Looking up
© 2003 Canadian Medical Association; Association medicale canadienne. Published by Canadian Medical Association.
2
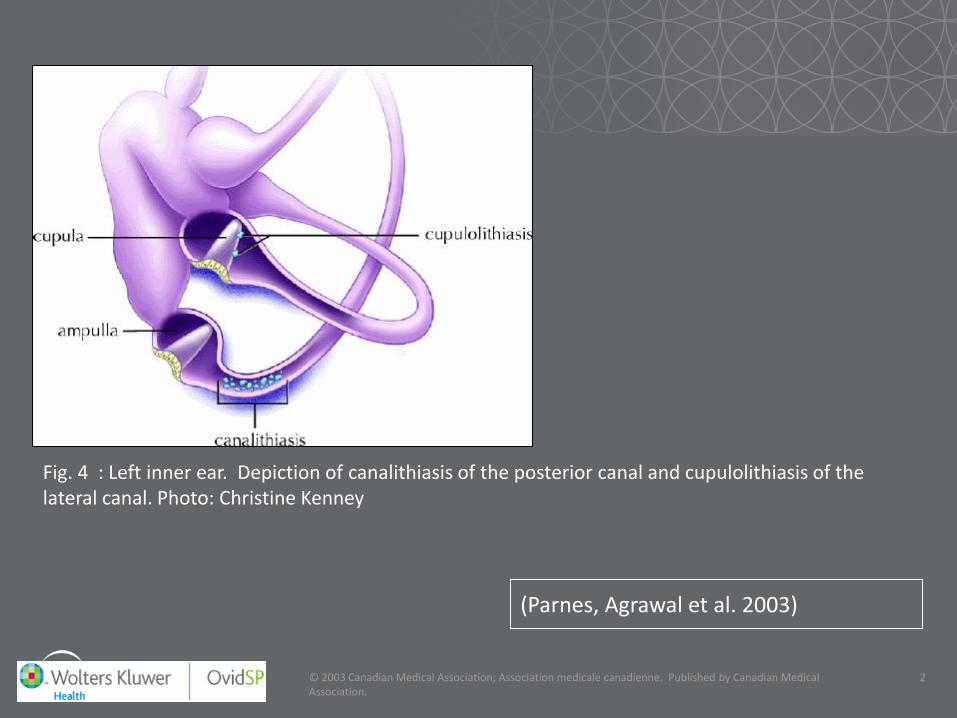
(Parnes, Agrawal et al. 2003)
Fig. 4 : Left inner ear. Depiction of canalithiasis of the posterior canal and cupulolithiasis of the lateral canal. Photo: Christine Kenney
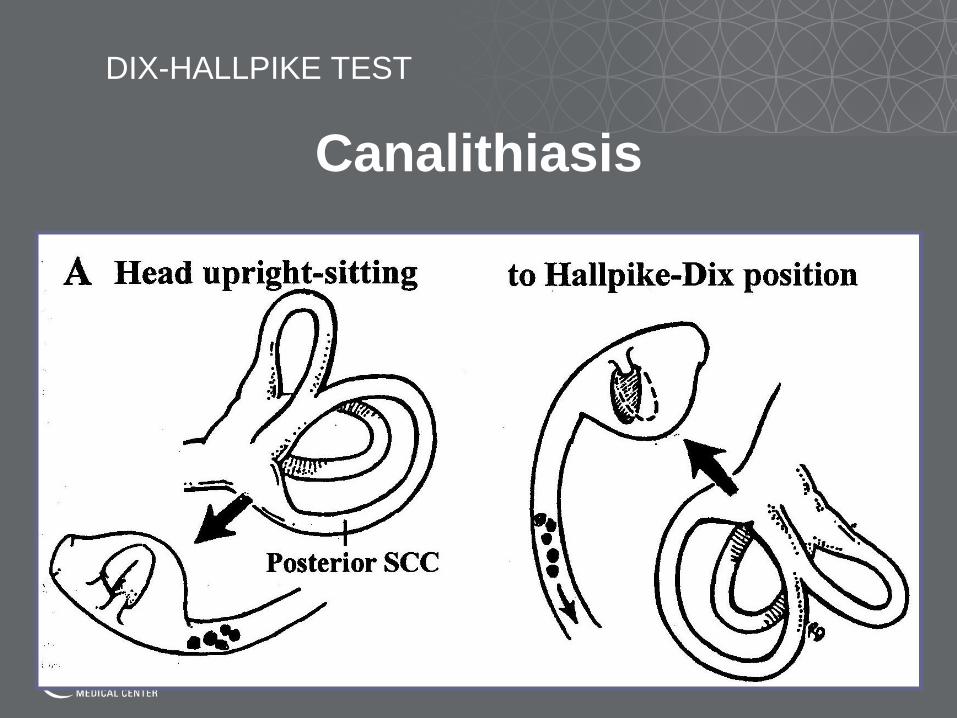
DIX-HALLPIKE TEST
Canalithiasis
Dix-Hallpike Test
•45 degrees cervical rotation
•Sit to supine with 20 degrees cervical extension
•Look for nystagmus and symptoms of vertigo
•Latency
•Direction
•Duration
•Fatigues
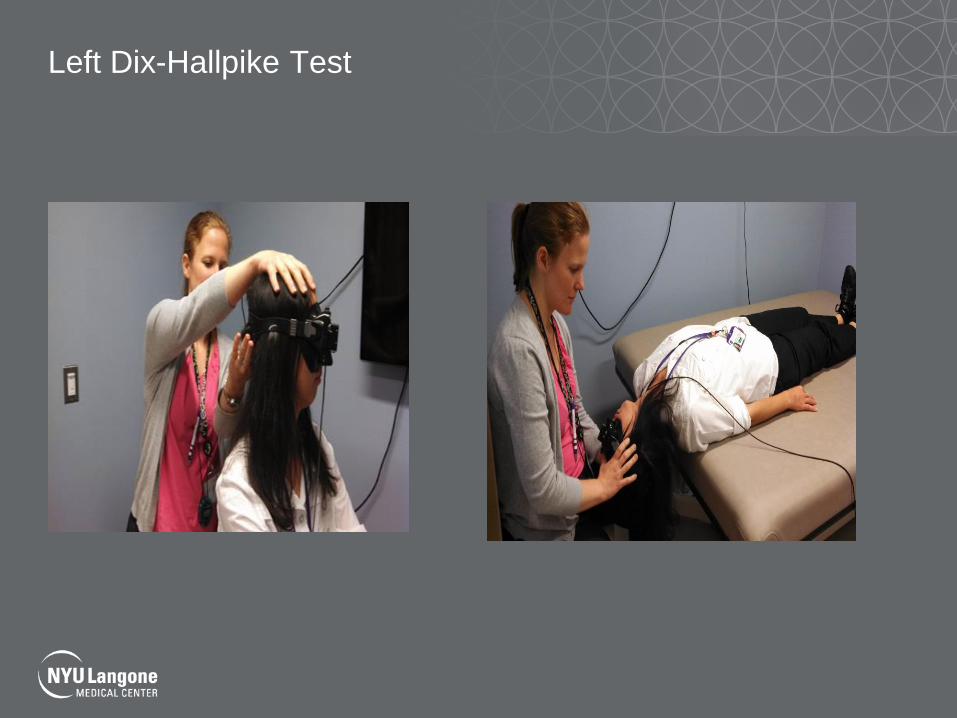
Left Dix-Hallpike Test
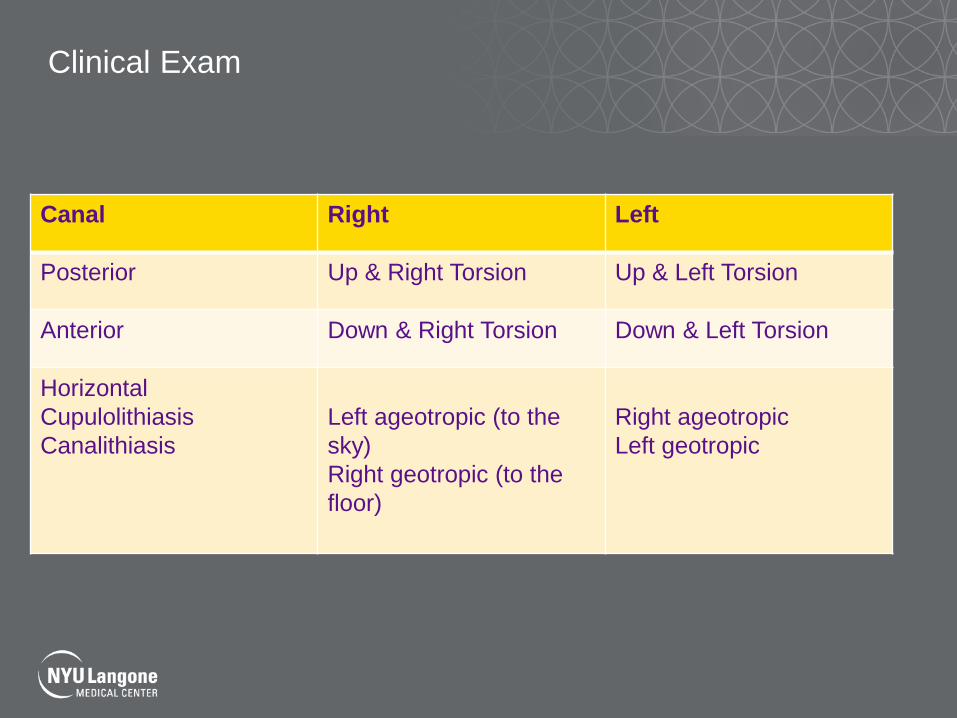
Clinical Exam
Canal Right Left
Posterior Up & Right Torsion Up & Left Torsion
Anterior Down & Right Torsion Down & Left Torsion
Horizontal
Cupulolithiasis
Canalithiasis
Left ageotropic (to the
sky)
Right geotropic (to the
floor)
Right ageotropic
Left geotropic
Left Posterior Canalithiasis Nystagmus
© Jennifer Fay, PT, DPT, NCS

Treatment
•Epley or Canal repositioning Maneuver
•Each position is held for 30 sec-2 min
•Designed to treat canalithiasis
•Semont Maneuver
•Designed to treat cupulolithiasis
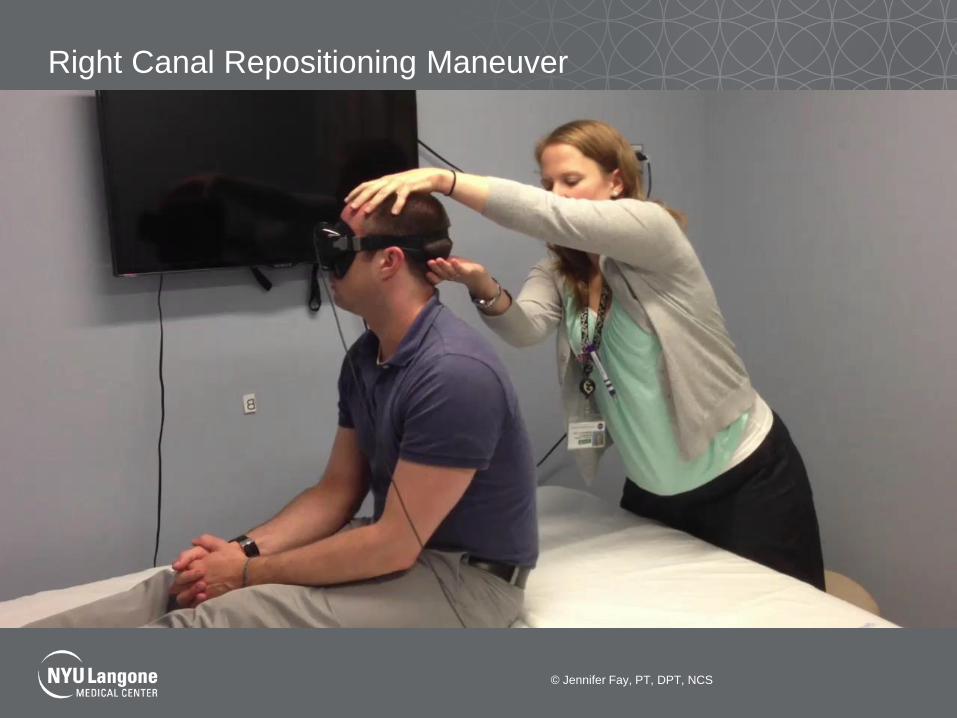
Right Canal Repositioning Maneuver
© Jennifer Fay, PT, DPT, NCS
References:
• Bhattacharyya, N., R. F. Baugh, L. Orvidas, D. Barrs, L. J. Bronston, S. Cass, A. A. Chalian, A. L. Desmond, J. M. Earll, T. D. Fife, D. C. Fuller, J. O. Judge, N. R. Mann, R. M. Rosenfeld, L. T. Schuring, R. W. Steiner, S. L. Whitney, J. Haidari, O.-H. American Academy of and F. Neck Surgery (2008). "Clinical practice guideline: benign paroxysmal positional vertigo." Otolaryngol Head Neck Surg 139(5 Suppl 4): S47-81.
• Froehling, D. A., M. D. Silverstein, D. N. Mohr, C. W. Beatty, K. P. Offord and D. J. Ballard (1991). "Benign positional vertigo: incidence and prognosis in a population-based study in Olmsted County, Minnesota." Mayo Clin Proc 66(6): 596-601.
• Froehling DA, S. M., Mohr DN, Beatty CW (1994). "Does this dizzy patient have a serious form of vertigo?" JAMA: Journal of the American Medical Association 271(5): 385-388.
• Goldberg JM, F. C. (1971). "Physiology of peripheral neurons innervating semicircular canals of the squirrel monkey, I: resting discharge and response to constant angular accelerations. ." Journal of Neurophysiology 34: 141-153.
• Herdman SJ, H. C., Delaune W (2011). "Variables Associated with Outcome in Patients with Unilateral Vestibular Hypofunction." Neurorehabilitation and Neural Repair 26(2): 151-162.
• Krebs D.E., G. K. M., Riley P.O, Parker S.W. (1993). "Double-blind, placebo-controlled trial of rehabilitation for bilateral vestibular hypofunction-Preliminary report. ." Otolaryngology-Head and Neck Surgery 109: 735-741.
• Lysakowski A, M. L., Fernandez C, Goldberg JM. (1995). "Physiological identification of morphologically distinct afferent classes innervating the cristae ampullares of the squirrel monkey. ." Journal of Neurophysiology 73: 1270-1281.
• M, N. (1988). "Vestibular Habituation Training: Specificity of Adequate Exercise." Archives Otolaryngology Head Neck Surgery 114: 883-886.
• Naito Y, N. A., Lee WS, et al. (1995). "Projections of the individual vestibular end-organs in the brain stem of the squirrel monkey. ." Hearing Research 87: 141-155.
• Schubert MC, M. L. (2004). "Vestibulo-ocular Physiology Underlying Vestibular Hypofunction." Physical Therapy 84(4): 373-385. • TC, H. (2011). "Neurophysiology of vestibular rehabilitation " NeuroRehabilitation 29: 127-141. • Whitney SL, S. P. (2011). "Principles of vestibular physical therapy rehabilitation " NeuroRehabilitation 29: 157-166. • Fife, T. D. and C. Giza (2013). "Posttraumatic vertigo and dizziness." Semin Neurol 33(3): 238-243. • Valovich McLeod, T. C. and T. D. Hale (2015). "Vestibular and balance issues following sport-related concussion." Brain Inj 29(2):
175-184. • Gurley, J. M., B. D. Hujsak and J. L. Kelly (2013). "Vestibular rehabilitation following mild traumatic brain injury."
NeuroRehabilitation 32(3): 519-528. • Lei-Rivera, L., J. Sutera, J. A. Galatioto, B. D. Hujsak and J. M. Gurley (2013). "Special tools for the assessment of balance and
dizziness in individuals with mild traumatic brain injury." NeuroRehabilitation 32(3): 463-472.