Alterations in the Gastrointestinal System 26
14
UNIT Seven Alterations in the Gastrointestinal System CHAPTER 26 Structure and Function of the Gastrointestinal System Structure and Organization of the Gastrointestinal Tract Upper Gastrointestinal Tract Esophagus Stomach Middle Gastrointestinal Tract Lower Gastrointestinal Tract Gastrointestinal Wall Structure Innervation and Motility Innervation Enteric Nervous System Autonomic Nervous System Swallowing and Esophageal Motility Gastric Motility Small Intestinal Motility Colonic Motility Defecation Hormonal and Secretory Function Gastrointestinal Hormones Gastrointestinal Secretions Salivary Secretions Gastric Secretions Intestinal Secretions 459 Digestion and Absorption Carbohydrates Fats Proteins Anorexia, Nausea, and Vomiting Anorexia Nausea Vomiting S tructurally, the gastrointestinal tract is a long, hollow tube with its lumen inside the body and its wall acting as an interface between the internal and external environments. The wall does not normally allow harmful agents to enter the body, nor does it permit body fluids and other materials to es- cape. The process of digestion and absorption of nutrients re- quires an intact and healthy gastrointestinal tract epithelial lining that can resist the effects of its own digestive secretions. The process also involves movement of materials through the gastrointestinal tract at a rate that facilitates absorption, and it requires the presence of enzymes for the digestion and absorp- tion of nutrients. As a matter of semantics, the gastrointestinal tract also is re- ferred to as the digestive tract, the alimentary canal, and at times, the gut. The intestinal portion also may be called the bowel. For the purposes of this text, the salivary glands, the liver, and the pancreas, which produce secretions that aid in digestion, are considered accessory organs.
Transcript of Alterations in the Gastrointestinal System 26
UNITSevenAlterations in theGastrointestinal System
CHAPTER
26 Structure and Function ofthe Gastrointestinal System
Structure and Organization of the Gastrointestinal Tract
Upper Gastrointestinal TractEsophagusStomach
Middle Gastrointestinal TractLower Gastrointestinal TractGastrointestinal Wall Structure
Innervation and MotilityInnervation
Enteric Nervous SystemAutonomic Nervous System
Swallowing and Esophageal MotilityGastric MotilitySmall Intestinal MotilityColonic MotilityDefecation
Hormonal and Secretory FunctionGastrointestinal HormonesGastrointestinal Secretions
Salivary SecretionsGastric SecretionsIntestinal Secretions
459
Digestion and AbsorptionCarbohydratesFatsProteins
Anorexia, Nausea, and VomitingAnorexiaNauseaVomiting
Structurally, the gastrointestinal tract is a long, hollow tubewith its lumen inside the body and its wall acting as aninterface between the internal and external environments.
The wall does not normally allow harmful agents to enter thebody, nor does it permit body fluids and other materials to es-cape. The process of digestion and absorption of nutrients re-quires an intact and healthy gastrointestinal tract epitheliallining that can resist the effects of its own digestive secretions.The process also involves movement of materials through thegastrointestinal tract at a rate that facilitates absorption, and itrequires the presence of enzymes for the digestion and absorp-tion of nutrients.
As a matter of semantics, the gastrointestinal tract also is re-ferred to as the digestive tract, the alimentary canal, and at times,the gut. The intestinal portion also may be called the bowel. Forthe purposes of this text, the salivary glands, the liver, and thepancreas, which produce secretions that aid in digestion, areconsidered accessory organs.
460 Unit Seven: Alterations in the Gastrointestinal System
STRUCTURE AND ORGANIZATION OF THE GASTROINTESTINAL TRACT
In the digestive tract, food and other materials move slowlyalong its length as they are systematically broken down intoions and molecules that can be absorbed into the body. In thelarge intestine, unabsorbed nutrients and wastes are collectedfor later elimination. Although the gastrointestinal tract is lo-cated inside the body, it is a long, hollow tube, the lumen (i.e.,hollow center) of which is an extension of the external envi-ronment. Nutrients do not become part of the internal envi-ronment until they have passed through the intestinal wall andhave entered the blood or lymph channels.
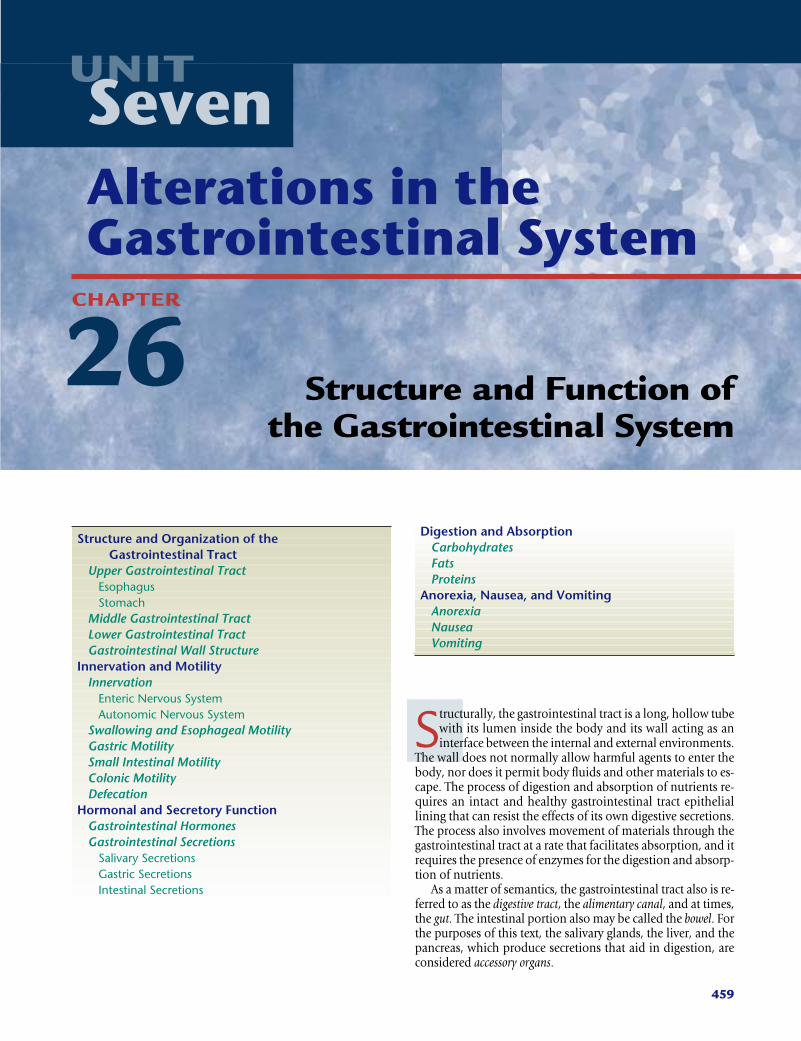
For simplicity and understanding, the digestive system canbe divided into four parts (Fig. 26-1). The upper part—themouth, esophagus, and stomach—acts as an intake source andreceptacle through which food passes and in which initial di-gestive processes take place. The middle portion consists of thesmall intestine—the duodenum, jejunum, and ileum. Most di-gestive and absorptive processes occur in the small intestine.The lower segment—the cecum, colon, and rectum—serves asa storage channel for the efficient elimination of waste. Thefourth part consists of the accessory organs—the salivaryglands, liver, and pancreas. These structures produce digestivesecretions that help dismantle foods and regulate the use andstorage of nutrients. The discussion in this chapter focuses on
the first three parts of the gastrointestinal tract. The liver andpancreas are discussed in Chapter 28.
Upper Gastrointestinal TractThe mouth forms the entryway into the gastrointestinal tractfor food; it contains the teeth, used in the mastication of food,and the tongue and other structures needed to direct food to-ward the pharyngeal structures and the esophagus.
EsophagusThe esophagus is a tube that connects the oropharynx withthe stomach. The esophagus begins at the lower end of thepharynx. It is a muscular, collapsible tube, approximately 25 cm (10 in) long, that lies behind the trachea. The muscu-lar walls of the upper third of the esophagus are skeletal-typestriated muscle; these muscle fibers are gradually replaced bysmooth muscle fibers until, at the lower third of the esopha-gus, the muscle layer is entirely smooth muscle.
The esophagus functions primarily as a conduit for passageof food from the pharynx to the stomach, and the structures ofits walls are designed for this purpose: the smooth muscle lay-ers provide the peristaltic movements needed to move foodalong its length, and the epithelial layer secretes mucus, whichprotects its surface and aids in lubricating food. There aresphincters at either end of the esophagus: an upper esophageal
■ FIGURE 26-1 ■ The digestive system.
Oral cavityTongue
Sublingual gland
Submandibulargland
Pharynx
Trachea
Liver (cut)
Gall bladderDuodenum
Commonbile duct
Pancreas
Ascendingcolon
Cecum
Vermiformappendix
IleumRectumAnus
Nasopharynx
Oropharynx
Hard palate
Soft palate
Parotid gland
Esophagus
StomachDiaphragm
Spleen
Transversecolon
Jejunum
Smallintestine
Descendingcolon
Sigmoid colon
sphincter and a lower esophageal sphincter. The upper eso-phageal, or pharyngoesophageal, sphincter consists of a circu-lar layer of striated muscle. The lower esophageal, or gastro-esophageal, sphincter is an area approximately 3 cm above thejunction with the stomach. The circular muscle in this areanormally remains tonically contracted, creating a zone of highpressure that serves to prevent reflux of gastric contents into theesophagus. During swallowing, there is “receptive relaxation”of the lower esophageal sphincter, which allows easy propul-sion of the esophageal contents into the stomach. The loweresophageal sphincter passes through an opening, or hiatus, inthe diaphragm as it joins with the stomach, which is located inthe abdomen. The portion of the diaphragm that surrounds thelower esophageal sphincter helps to maintain the zone of highpressure needed to prevent reflux of stomach contents into theesophagus.
StomachThe stomach is a pouchlike structure that lies in the upper partof the abdomen and serves as a food storage reservoir duringthe early stages of digestion. Although the residual volume ofthe stomach is only approximately 50 mL, it can increase toalmost 1000 mL before the intraluminal pressure begins to rise.The esophagus opens into the stomach through an openingcalled the cardiac orifice, so named because of its proximity tothe heart. The part of the stomach that lies above and to the leftof the cardiac orifice is called the fundus, the central portion is
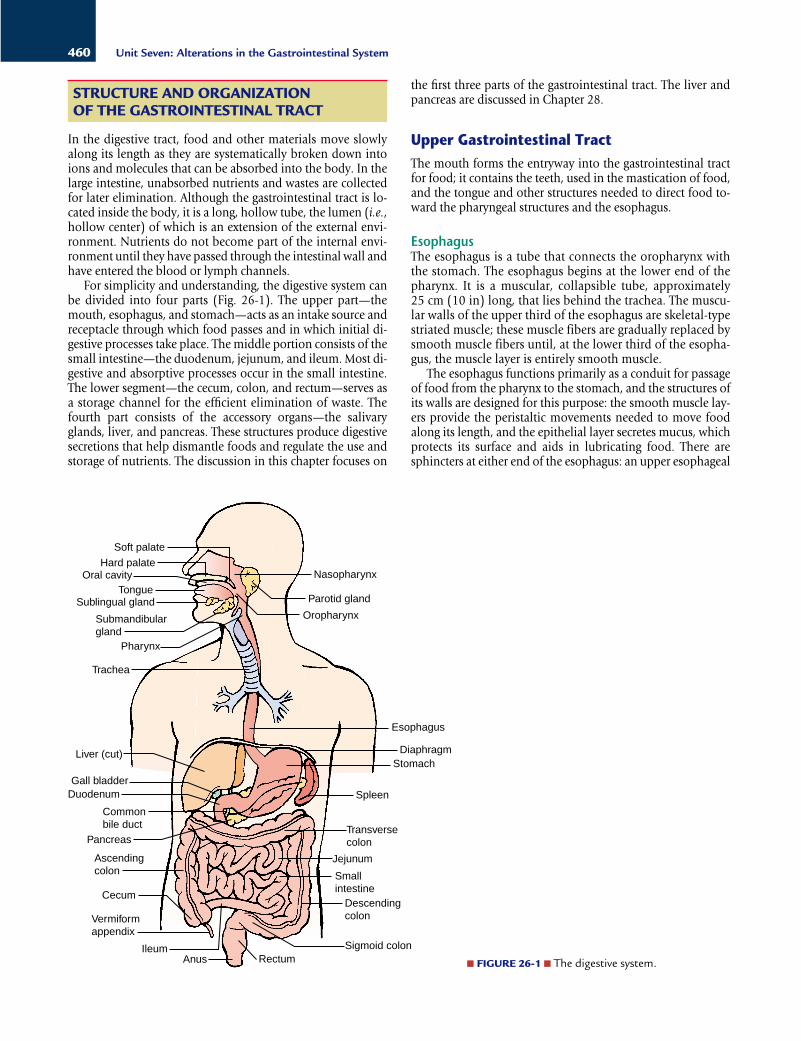
called the body, the orifice encircled by a ringlike muscle thatopens into the small intestine is called the pylorus, and theportion between the body and pylorus is called the antrum(Fig. 26-2). The presence of a true pyloric sphincter is a matterof controversy. Regardless of whether an actual sphincter exists,contractions of the smooth muscle in the pyloric area controlthe rate of gastric emptying.
Middle Gastrointestinal TractThe small intestine, which forms the middle portion of the di-gestive tract, consists of three subdivisions: the duodenum, thejejunum, and the ileum. The duodenum, which is approxi-mately 22 cm (10 in) long, connects the stomach to the jeju-num and contains the opening for the common bile duct andthe main pancreatic duct. Bile and pancreatic juices enter theintestine through these ducts. It is in the jejunum and ileum,which together are approximately 7 m (23 ft) long and must befolded onto themselves to fit into the abdominal cavity, thatfood is digested and absorbed.
Lower Gastrointestinal TractThe large intestine, which forms the lower gastrointestinal tract,is approximately 1.5 m (4.5 to 5 ft) long and 6 to 7 cm (2.4 to2.7 in) in diameter. It is divided into the cecum, colon, rectum,and anal canal. The cecum is a blind pouch that projects downat the junction of the ileum and the colon. The ileocecal valvelies at the upper border of the cecum and prevents the return offeces from the cecum into the small intestine. The appendixarises from the cecum approximately 2.5 cm (1 in) from theileocecal valve. The colon is further divided into ascending,transverse, descending, and sigmoid portions. The ascendingcolon extends from the cecum to the undersurface of the liver,where it turns abruptly to form the right colic (hepatic) flexure.The transverse colon crosses the upper half of the abdominalcavity from right to left and then curves sharply downwardbeneath the lower end of the spleen, forming the left colic
461Chapter 26: Structure and Function of the Gastrointestinal System
KEY CONCEPTS
STRUCTURE AND FUNCTION OF THE GASTROINTESTINAL TRACT
■ The gastrointestinal tract is a long, hollow tube thatextends from the mouth to the anus; food and fluidsthat enter the gastrointestinal tract do not becomepart of the internal environment until they havebeen broken down and absorbed into the blood or lymph channels.
■ The wall of the gastrointestinal tract is essentially afive-layered tube: an inner mucosal layer; a support-ing submucosal layer of connective tissue; a fourthand fifth layer of circular and longitudinal smoothmuscle that functions to propel its contents in aproximal-to-distal direction; and an outer, two-layered peritoneum that encloses and preventsfriction between the continuously moving segments of the intestine.
■ The nutrients contained in ingested foods and fluidsmust be broken down into molecules that can beabsorbed across the wall of the intestine. Gastricacids and pepsin from the stomach begin the diges-tive process: bile from the liver, digestive enzymesfrom the pancreas, and brush border enzymes breakcarbohydrates, fats, and proteins into molecules thatcan be absorbed from the intestine.
Fundus
Body
Pylorus
Duodenum
Esophagus
Antrum
■ FIGURE 26-2 ■ Structures of the stomach, showing the pace-maker area and the direction of chyme movement resulting fromperistaltic contractions.
(splenic) flexure. The descending colon extends from the colicflexure to the rectum. The rectum extends from the sigmoidcolon to the anus. The anal canal passes between the two me-dial borders of the levator ani muscles. Powerful sphinctermuscles guard against fecal incontinence.
Gastrointestinal Wall StructureThe digestive tract is essentially a five-layered tube (Fig. 26-3).The inner luminal layer, or mucosal layer, is so named becauseits cells produce mucus that lubricates and protects the innersurface of the alimentary canal. The epithelial cells in this layerhave a rapid turnover rate and are replaced every 4 to 5 days.Approximately 250 g of these cells are shed each day in thestool. Because of the regenerative capabilities of the mucosallayer, injury to this layer of tissue heals rapidly without leavingscar tissue. The submucosal layer consists of connective tissue.This layer contains blood vessels, nerves, and structures re-sponsible for secreting digestive enzymes. The third and fourthlayers, the circular and longitudinal muscle layers, facilitate move-ment of the contents of the gastrointestinal tract. The outerlayer, the peritoneum, is loosely attached to the outer wall of theintestine.
The peritoneum is the largest serous membrane in the body,having a surface area approximately equal to that of the skin.The peritoneum consists of two continuous layers—the parietaland the visceral peritoneum. The parietal peritoneum comes incontact with and is loosely attached to the abdominal wall,whereas the visceral peritoneum invests the viscera such as thestomach and intestines. A thin layer of serous fluid separatesthe parietal and visceral peritoneum, forming a potential spacecalled the peritoneal cavity. The serous fluid forms a moist andslippery surface that prevents friction between the continu-ously moving abdominal structures. In certain pathologicstates, the amount of fluid in the potential space of the peri-toneal cavity is increased, causing a condition called ascites.
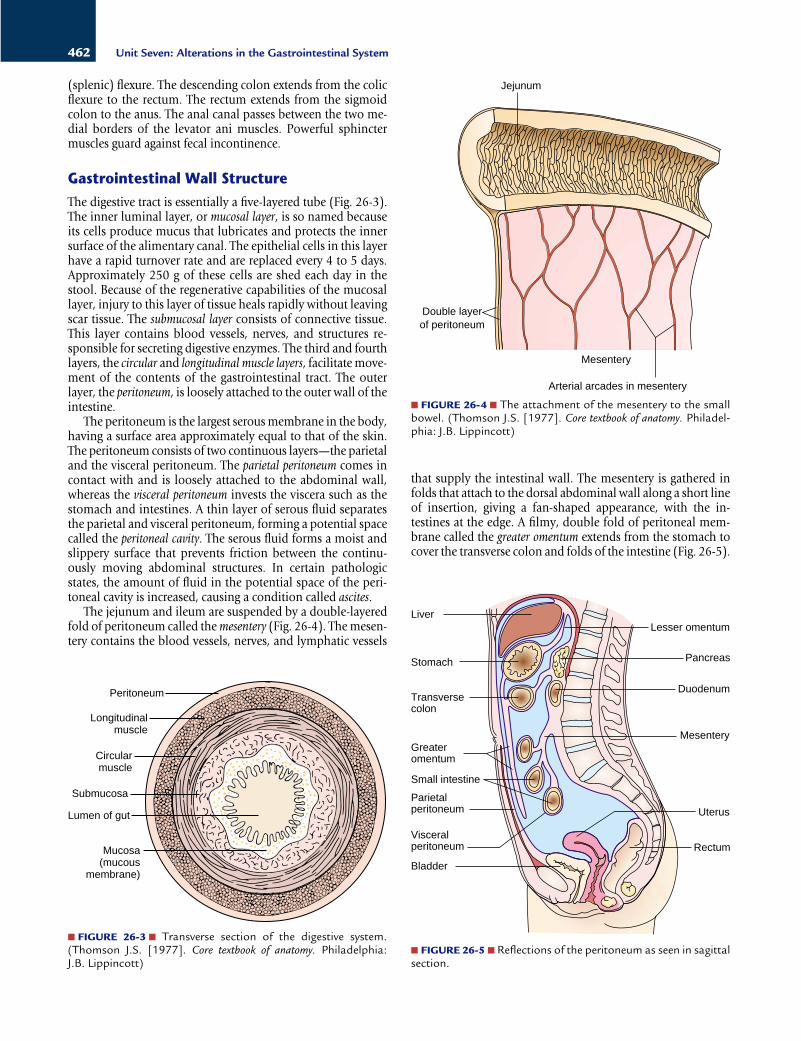
The jejunum and ileum are suspended by a double-layeredfold of peritoneum called the mesentery (Fig. 26-4). The mesen-tery contains the blood vessels, nerves, and lymphatic vessels
that supply the intestinal wall. The mesentery is gathered infolds that attach to the dorsal abdominal wall along a short lineof insertion, giving a fan-shaped appearance, with the in-testines at the edge. A filmy, double fold of peritoneal mem-brane called the greater omentum extends from the stomach tocover the transverse colon and folds of the intestine (Fig. 26-5).
462 Unit Seven: Alterations in the Gastrointestinal System
Peritoneum
Longitudinalmuscle
Circularmuscle
Submucosa
Lumen of gut
Mucosa(mucous
membrane)
■ FIGURE 26-3 ■ Transverse section of the digestive system.(Thomson J.S. [1977]. Core textbook of anatomy. Philadelphia:J.B. Lippincott)
Jejunum
Double layerof peritoneum
Mesentery
Arterial arcades in mesentery
■ FIGURE 26-4 ■ The attachment of the mesentery to the smallbowel. (Thomson J.S. [1977]. Core textbook of anatomy. Philadel-phia: J.B. Lippincott)
■ FIGURE 26-5 ■ Reflections of the peritoneum as seen in sagittalsection.
Liver
Stomach
Transversecolon
Greateromentum
Small intestine
Parietalperitoneum
Visceralperitoneum
Bladder
Lesser omentum
Pancreas
Duodenum
Mesentery
Uterus
Rectum

The greater omentum protects the intestines from cold. Italways contains some fat, which in obese persons can be a con-siderable amount. The omentum also controls the spread of in-fection from gastrointestinal contents. In the case of infection,the omentum adheres to the inflamed area so that the infectionis less likely to enter the peritoneal cavity. The lesser omentumextends between the transverse fissure of the liver and the lessercurvature of the stomach.
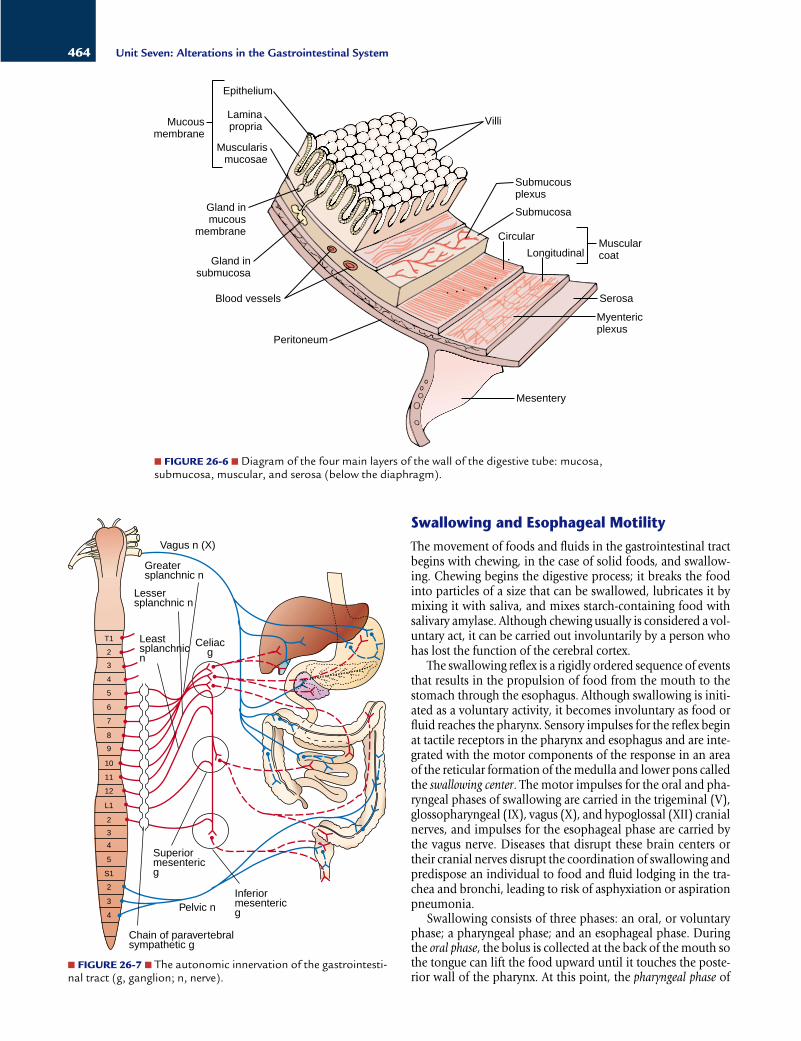
Enteric Nervous System The intramural neurons (i.e., those contained within the wallof the gastrointestinal tract) consist of two networks: themyenteric and submucosal plexuses. Both plexuses are aggre-gates of ganglionic cells that extend along the length of thegastrointestinal wall. The myenteric (Auerbach’s) plexus is lo-cated between the circular muscle and longitudinal musclelayers, and the submucosal (Meissner’s) plexus between themucosal layer and the circular muscle layers (Fig. 26-6). Theactivity of the neurons in the myenteric and submucosalplexuses is regulated by local influences, input from the ANS,and by interconnecting fibers that transmit informationbetween the two plexuses.
The myenteric plexus consists mainly of a linear chain ofinterconnecting neurons that extend the full length of the gas-trointestinal tract. Because it extends all the way down the in-testinal wall and because it lies between the two muscle layers,it is concerned mainly with motility along the length of the gut.The submucosal plexus, which lies between the mucosal andcircular muscle layers of the intestinal wall, is mainly con-cerned with controlling the function of each segment of the in-testinal tract. It integrates signals received from the mucosallayer into local control of motility, intestinal secretions, andabsorption of nutrients.
Intramural plexus neurons also communicate with receptorsin the mucosal and muscle layers. Mechanoreceptors monitorthe stretch and distention of the gastrointestinal tract wall, andchemoreceptors monitor the chemical composition (i.e., osmo-lality, pH, and digestive products of protein and fat metabo-lism) of its contents. These receptors can communicate directlywith ganglionic cells in the intramural plexuses or with visceralafferent fibers that influence ANS control of gastrointestinalfunction.
Autonomic Nervous SystemThe gastrointestinal tract is innervated by both the sympa-thetic and parasympathetic nervous systems. Parasympatheticinnervation to the stomach, small intestine, cecum, ascendingcolon, and transverse colon occurs by way of the vagus nerve(Fig. 26-7). The remainder of the colon is innervated by para-sympathetic fibers that exit the sacral segments of the spinalcord by way of the pelvic nerve. Preganglionic parasympa-thetic fibers can synapse with intramural plexus neurons, or they can act directly on intestinal smooth muscle. Mostparasympathetic fibers are excitatory. Numerous vagovagalreflexes influence motility and secretions of the digestivetract.
Sympathetic innervation of the gastrointestinal tract occursthrough the thoracic chain of sympathetic ganglia and theceliac, superior mesenteric, and inferior mesenteric ganglia.Sympathetic control of gastrointestinal function is largely me-diated by altering the activity of neurons in the intramuralplexuses. The sympathetic nervous system exerts several effectson gastrointestinal function. It controls mucus secretion by themucosal glands, reduces motility by inhibiting the activity ofintramural plexus neurons, enhances sphincter function, andincreases the vascular smooth muscle tone of the blood vesselsthat supply the gastrointestinal tract. The sympathetic fibersthat supply the lower esophageal, pyloric, and internal andexternal anal sphincters are largely excitatory, but their role incontrolling these sphincters is poorly understood.
463Chapter 26: Structure and Function of the Gastrointestinal System
In summary, the gastrointestinal tract is a long, hollowtube, the lumen of which is an extension of the external envi-ronment. The digestive tract can be divided into four parts:an upper part, consisting of the mouth, esophagus, andstomach; a middle part, consisting of the small intestine; alower part, consisting of the cecum, colon, and rectum; andthe accessory organs, consisting of the salivary glands, theliver, and the pancreas. Throughout its length, except for themouth, throat, and upper esophagus, the gastrointestinaltract is composed of five layers: an inner mucosal layer, a sub-mucosal layer, a layer of circular smooth muscle fibers, a layerof longitudinal smooth muscle fibers, and an outer serosallayer that forms the peritoneum and is continuous with themesentery.
INNERVATION AND MOTILITY
The motility of the gastrointestinal tract propels food prod-ucts and fluids along its length, from mouth to anus, in amanner that facilitates digestion and absorption. Except inthe pharynx and upper third of the esophagus, smooth mus-cle provides the contractile force for gastrointestinal motility(the actions of smooth muscle are discussed in Chapter 1).The rhythmic movements of the digestive tract are self-perpetuating, much like the activity of the heart, and are in-fluenced by local, humoral (i.e., blood-borne), and neural in-fluences. The ability to initiate impulses is a property of thesmooth muscle itself. Impulses are conducted from one mus-cle fiber to another.
The smooth muscle movements of the gastrointestinal tractare tonic and rhythmic. The tonic movements are continuousmovements that last for minutes or even hours. Tonic contrac-tions occur at sphincters. The rhythmic movements consist ofintermittent contractions that are responsible for mixing andmoving food along the digestive tract. Peristaltic movements arerhythmic propulsive movements that occur when the smoothmuscle layer constricts, forming a contractile band that forcesthe intraluminal contents forward. During peristalsis, the seg-ment that lies distal to, or ahead of, the contracted portion re-laxes, and the contents move forward with ease. Normal peri-stalsis always moves in the direction from the mouth towardthe anus.
InnervationGastrointestinal function is controlled by the enteric nervous sys-tem, which lies entirely within the wall of the gastrointestinaltract, and by the parasympathetic and sympathetic divisions ofthe autonomic nervous system (ANS).
Swallowing and Esophageal Motility
The movement of foods and fluids in the gastrointestinal tractbegins with chewing, in the case of solid foods, and swallow-ing. Chewing begins the digestive process; it breaks the foodinto particles of a size that can be swallowed, lubricates it bymixing it with saliva, and mixes starch-containing food withsalivary amylase. Although chewing usually is considered a vol-untary act, it can be carried out involuntarily by a person whohas lost the function of the cerebral cortex.
The swallowing reflex is a rigidly ordered sequence of eventsthat results in the propulsion of food from the mouth to thestomach through the esophagus. Although swallowing is initi-ated as a voluntary activity, it becomes involuntary as food orfluid reaches the pharynx. Sensory impulses for the reflex beginat tactile receptors in the pharynx and esophagus and are inte-grated with the motor components of the response in an areaof the reticular formation of the medulla and lower pons calledthe swallowing center. The motor impulses for the oral and pha-ryngeal phases of swallowing are carried in the trigeminal (V),glossopharyngeal (IX), vagus (X), and hypoglossal (XII) cranialnerves, and impulses for the esophageal phase are carried bythe vagus nerve. Diseases that disrupt these brain centers ortheir cranial nerves disrupt the coordination of swallowing andpredispose an individual to food and fluid lodging in the tra-chea and bronchi, leading to risk of asphyxiation or aspirationpneumonia.
Swallowing consists of three phases: an oral, or voluntaryphase; a pharyngeal phase; and an esophageal phase. Duringthe oral phase, the bolus is collected at the back of the mouth sothe tongue can lift the food upward until it touches the poste-rior wall of the pharynx. At this point, the pharyngeal phase of
464 Unit Seven: Alterations in the Gastrointestinal System
Mesentery
Myentericplexus
Serosa
MuscularcoatLongitudinal
Circular
Submucosa
Submucousplexus
Villi
Blood vessels
Gland insubmucosa
Gland inmucous
membrane
Mucousmembrane
Epithelium
Laminapropria
Muscularismucosae
Peritoneum
■ FIGURE 26-6 ■ Diagram of the four main layers of the wall of the digestive tube: mucosa, submucosa, muscular, and serosa (below the diaphragm).
■ FIGURE 26-7 ■ The autonomic innervation of the gastrointesti-nal tract (g, ganglion; n, nerve).
T1
3
2
4
5
6
7
8
9
10
11
12
L1
2
3
4
5
2
3
4
S1
Vagus n (X)
Greatersplanchnic n
Lessersplanchnic n
Leastsplanchnicn
Superiormesentericg
InferiormesentericgPelvic n
Chain of paravertebralsympathetic g
Celiacg

swallowing is initiated. The soft palate is pulled upward, thepalatopharyngeal folds are pulled together so that food doesnot enter the nasopharynx, the vocal cords are pulled together,and the epiglottis is moved so that it covers the larynx. Res-piration is inhibited, and the bolus is moved backward into theesophagus by constrictive movements of the pharynx. Althoughthe striated muscles of the pharynx are involved in the secondstage of swallowing, it is an involuntary stage.
The third phase of swallowing is the esophageal stage. As foodenters the esophagus and stretches its walls, local and centralnervous system reflexes that initiate peristalsis are triggered.There are two types of peristalsis: primary and secondary. Pri-mary peristalsis is controlled by the swallowing center in the brain stem and begins when food enters the esophagus.Secondary peristalsis is partially mediated by smooth musclefibers in the esophagus and occurs when primary peristalsis isinadequate to move food through the esophagus. Peristalsis be-gins at the site of distention and moves downward. Before theperistaltic wave reaches the stomach, the lower esophagealsphincter relaxes to allow the bolus of food to enter the stom-ach. The pressure in the lower esophageal sphincter normallyis greater than that in the stomach, an important factor in pre-venting the reflux of gastric contents.
Gastric MotilityThe stomach serves as a reservoir for ingested solids and liq-uids. Motility of the stomach results in the churning and grind-ing of solid foods and regulates the emptying of the gastric con-tents, or chyme, into the duodenum. Peristaltic mixing andchurning contractions begin in a pacemaker area in the middleof the stomach and move toward the antrum (see Fig. 26-2).They occur at a frequency of three to five contractions perminute, each with a duration of 2 to 20 seconds. As the peri-staltic wave approaches the antrum, it speeds up, and the en-tire terminal 5 to 10 cm of the antrum contracts, occluding thepyloric opening. Contraction of the antrum reverses the move-ment of the chyme, returning the larger particles to the body ofthe stomach for further churning and kneading. Because thepylorus is contracted during antral contraction, the gastric con-tents are emptied into the duodenum between contractions.
Although the pylorus does not contain a true anatomicsphincter, it does function as a physiologic sphincter to preventthe backflow of gastric contents and allow them to flow into theduodenum at a rate commensurate with the ability of the duo-denum to accept them. This is important because the regurgi-tation of bile salts and duodenal contents can damage the mu-cosal surface of the antrum and lead to gastric ulcers. Likewise,the duodenal mucosa can be damaged by the rapid influx ofhighly acid gastric contents.
Like other parts of the gastrointestinal tract, the stomach isrichly innervated by the enteric nervous system and its con-nections with the sympathetic and parasympathetic nervoussystems. Axons from the intramural plexuses innervate thesmooth muscles and glands of the stomach. Parasympatheticinnervation is provided by the vagus nerve and sympatheticinnervation by the celiac ganglia. The emptying of the stom-ach is regulated by hormonal and neural mechanisms. The hor-mones cholecystokinin and gastric inhibitory peptide, whichare thought to control gastric emptying, are released in responseto the pH and the osmolar and fatty acid composition of thechyme. Local and central circuitry are involved in the neural
control of gastric emptying. Afferent receptor fibers synapsewith the neurons in the intramural plexus or trigger intrinsic re-flexes by means of vagal or sympathetic pathways that partici-pate in extrinsic reflexes.
Disorders of gastric motility can occur when the rate is tooslow or too fast (see Chapter 27). A rate that is too slow leadsto gastric retention. It can be caused by obstruction or gastricatony. Gastric atony can occur as a complication of visceralneuropathies in diabetes mellitus. Surgical procedures that dis-rupt vagal activity also can result in gastric atony. Abnormallyfast emptying occurs in the dumping syndrome, which is a con-sequence of certain types of gastric operations. This condition ischaracterized by the rapid dumping of highly acidic and hyper-osmotic gastric secretions into the duodenum and jejunum.
Small Intestinal MotilityThe small intestine is the major site for the digestion and ab-sorption of food; its movements are mixing and propulsive.Regular peristaltic movements begin in the duodenum near theentry sites of the common duct and the main hepatic duct. Aseries of local pacemakers maintains the frequency of intes-tinal contraction. The peristaltic movements (approximately 12 per minute in the jejunum) become less frequent as theymove further from the pylorus, becoming approximately 9 perminute in the ileum.
The peristaltic contractions produce segmentation wavesand propulsive movements of the small intestine. With seg-mentation waves, slow contractions of circular muscle occludethe lumen and drive the contents forward and backward. Mostof the contractions that produce segmentation waves are localevents involving only 1 to 4 cm at a time. They function mainlyto mix the chyme with the digestive enzymes from the pancreasand to ensure adequate exposure of all parts of the chyme tothe mucosal surface of the intestine, where absorption takesplace. The frequency of segmenting activity increases after ameal, presumably stimulated by receptors in the stomach andintestine.
Propulsive movements occur with synchronized activity ina section 10 to 20 cm long. They are accomplished by contrac-tion of the proximal portion of the intestine with the sequen-tial relaxation of its distal, or anal, portion. After material hasbeen propelled to the ileocecal junction by peristaltic move-ment, stretching of the distal ileum produces a local reflex thatrelaxes the sphincter and allows fluid to squirt into the cecum.
Motility disturbances of the small bowel are common, andauscultation of the abdomen can be used to assess bowel activity. Inflammatory changes increase motility. In many in-stances, it is not certain whether changes in motility occur be-cause of inflammation or occur secondary to toxins and un-absorbed materials. Delayed passage of materials in the smallintestine also can be a problem. Transient interruption of in-testinal motility often occurs after gastrointestinal surgery. In-tubation with suction often is required to remove the accumu-lating intestinal contents and gases until activity is resumed.
Colonic MotilityThe storage function of the colon dictates that movements inthis section of the gut are different from those in the small in-testine. Movements in the colon are of two types. First are thesegmental mixing movements, called haustrations, so named
465Chapter 26: Structure and Function of the Gastrointestinal System

because they occur within sacculations called haustra. Thesemovements produce a local digging-type action, which ensuresthat all portions of the fecal mass are exposed to the intestinalsurface. Second are the propulsive mass movements, in whicha large segment of the colon (≥20 cm) contracts as a unit, mov-ing the fecal contents forward as a unit. Mass movements lastapproximately 30 seconds, followed by a 2- to 3-minute periodof relaxation, after which another contraction occurs. A seriesof mass movements lasts only for 10 to 30 minutes and mayoccur only several times a day. Defecation normally is initiatedby the mass movements.
DefecationDefecation is controlled by the action of two sphincters, theinternal and external anal sphincters. The internal sphincter isa several-centimeters long circular thickening of smooth mus-cle that lies inside the anus. The external sphincter, which iscomposed of striated voluntary muscle, surrounds the internalsphincter. Defecation is controlled by defecation reflexes. Oneof these reflexes is the intrinsic myenteric reflex mediated bythe local enteric nervous system. It is initiated by distention ofthe rectal wall, with initiation of reflex peristaltic waves thatspread through the descending colon, sigmoid colon, and rec-tum. A second defecation reflex, the parasympathetic reflex, isintegrated at the level of the sacral cord. When the nerve end-ings in the rectum are stimulated, signals are transmitted firstto the sacral cord and then reflexly back to the descendingcolon, sigmoid colon, rectum, and anus by way of the pelvicnerves (Fig. 26-7). These impulses greatly increase peristalticmovements as well as relax the internal sphincter.
To prevent involuntary defecation from occurring, the ex-ternal anal sphincter, which is supplied by nerve fibers in thepudendal nerve, is under the conscious control of the cortex. Asafferent impulses arrive at the sacral cord, signaling the pres-ence of a distended rectum, messages are transmitted to the cor-tex. If defecation is inappropriate, the cortex initiates impulsesthat constrict the external sphincter and inhibit efferentparasympathetic activity. Normally, the afferent impulses inthis reflex loop fatigue easily, and the urge to defecate soonceases. At a more convenient time, contraction of the abdomi-nal muscles compresses the contents in the large bowel, reini-tiating afferent impulses to the cord.
HORMONAL AND SECRETORY FUNCTION
Each day, approximately 7000 mL of fluid is secreted into the gastrointestinal tract (Table 26-1). Approximately 50 to 200 mL of this fluid leaves the body in the stool; the remain-der is reabsorbed in the small and large intestines. Thesesecretions are mainly water and have sodium and potas-sium concentrations similar to those of extracellular fluid.Because water and electrolytes for digestive tract secretions arederived from the extracellular fluid compartment, excessivesecretion or impaired absorption can lead to extracellularfluid deficit.
The secretory activity of the gut is influenced by local, hu-moral, and neural influences. Neural control of gastrointestinalsecretory activity is mediated through the ANS. Secretory activ-ity, like motility, is increased with parasympathetic stimulationand inhibited with sympathetic activity. Many of the local in-fluences, including pH, osmolality, and chyme, consistently actas stimuli for neural and humoral mechanisms.
Gastrointestinal HormonesThe gastrointestinal tract is the largest endocrine organ in thebody. It produces hormones that pass from the portal circula-tion into the general circulation and then back to the digestivetract, where they exert their actions. Among the hormones pro-duced by the gastrointestinal tract are gastrin, secretin, andcholecystokinin. These hormones influence motility and thesecretion of electrolytes, enzymes, and other hormones. Thegastrointestinal tract hormones and their functions are sum-marized in Table 26-2.
The primary function of gastrin is the stimulation of gastricacid secretion. Gastrin also has a trophic, or growth-producing,effect on the mucosa of the small intestine, colon, and oxyntic(acid-secreting) gland area of the stomach. Removal of the tis-sue that produces gastrin results in atrophy of these structures.This atrophy can be reversed by the administration of exoge-nous gastrin.
Secretin is secreted by S cells in the mucosa of the duo-denum and jejunum in an inactive form called prosecretin.When an acid chyme with a pH of less than 4.5 to 5.0 entersthe intestine, secretin is activated and absorbed into the blood.Secretin causes the pancreas to secrete large quantities of fluidwith a high bicarbonate concentration and low chloride con-centration.
466 Unit Seven: Alterations in the Gastrointestinal System
In summary, motility of the gastrointestinal tract propelsfood products and fluids along its length from mouth to anus.Although the activity of gastrointestinal smooth muscle is self-propagating and can continue without input from the ner-vous system, its rate and strength of contractions are regu-lated by a network of intramural neurons that receive inputfrom the ANS and local receptors that monitor wall stretchand the chemical composition of luminal contents. Parasym-pathetic innervation occurs by means of the vagus nerve andnerve fibers from sacral segments of the spinal cord; it in-creases gastrointestinal motility. Sympathetic activity occursby way of thoracolumbar output from the spinal cord, itsparavertebral ganglia, and celiac, superior mesenteric, andinferior mesenteric ganglia. Sympathetic stimulation enhancessphincter function and reduces motility by inhibiting theactivity of intramural plexus neurons.
Secretions of the Gastrointestinal Tract
TABLE 26-1
Salivary 1200Gastric 2000Pancreatic 1200Biliary 700Intestinal 2000
Total 7100
Secretions Amount Daily (mL)

The primary function of cholecystokinin is stimulation ofpancreatic enzyme secretion. It potentiates the action of se-cretin, increasing the pancreatic bicarbonate response to lowcirculating levels of secretin. In addition to its effects on thepancreas, cholecystokinin also stimulates biliary secretion offluid and bicarbonate and it regulates gallbladder contractionand gastric emptying.
Two other hormones that contribute to gastrointestinalfunction are gastric inhibitory peptide and motilin. Gastricinhibitory peptide, which is released from the intestinal mucosain response to increased concentration of glucose and fats, in-hibits gastric acid secretion, gastric motility, and gastric emp-tying. Motilin, which stimulates intestinal motility and con-tributes to the control of the interdigestive actions of theintestinal neurons, is released from the upper small intestine.
Gastrointestinal SecretionsSalivary SecretionsSaliva is secreted by the salivary glands. The salivary glandsconsist of the parotid, submaxillary, sublingual, and buccalglands. Saliva has three functions. The first is protection andlubrication. Saliva is rich in mucus, which protects the oralmucosa and coats the food as it passes through the mouth,pharynx, and esophagus. The sublingual and buccal glandsproduce only mucus-type secretions. The second function ofsaliva is its protective antimicrobial action. The saliva cleansthe mouth and contains the enzyme lysozyme, which has anantibacterial action. Third, saliva contains ptyalin and amy-lase, which initiate the digestion of dietary starches. Secretionsfrom the salivary glands are primarily regulated by the ANS.Parasympathetic stimulation increases flow, and sympatheticstimulation decreases flow. The dry mouth that accompaniesanxiety attests to the effects of sympathetic activity on salivarysecretions.
Mumps, or parotitis, is an infection of the parotid glands.Although most of us associate mumps with the contagiousviral form of the disease, inflammation of the parotid glandscan occur in the seriously ill person who does not receive ad-equate oral hygiene and who is unable to take fluids orally.Potassium iodide increases the secretory activity of the salivaryglands, including the parotid glands. In a small percentage ofpersons, parotid swelling may occur in the course of treatmentwith this drug.
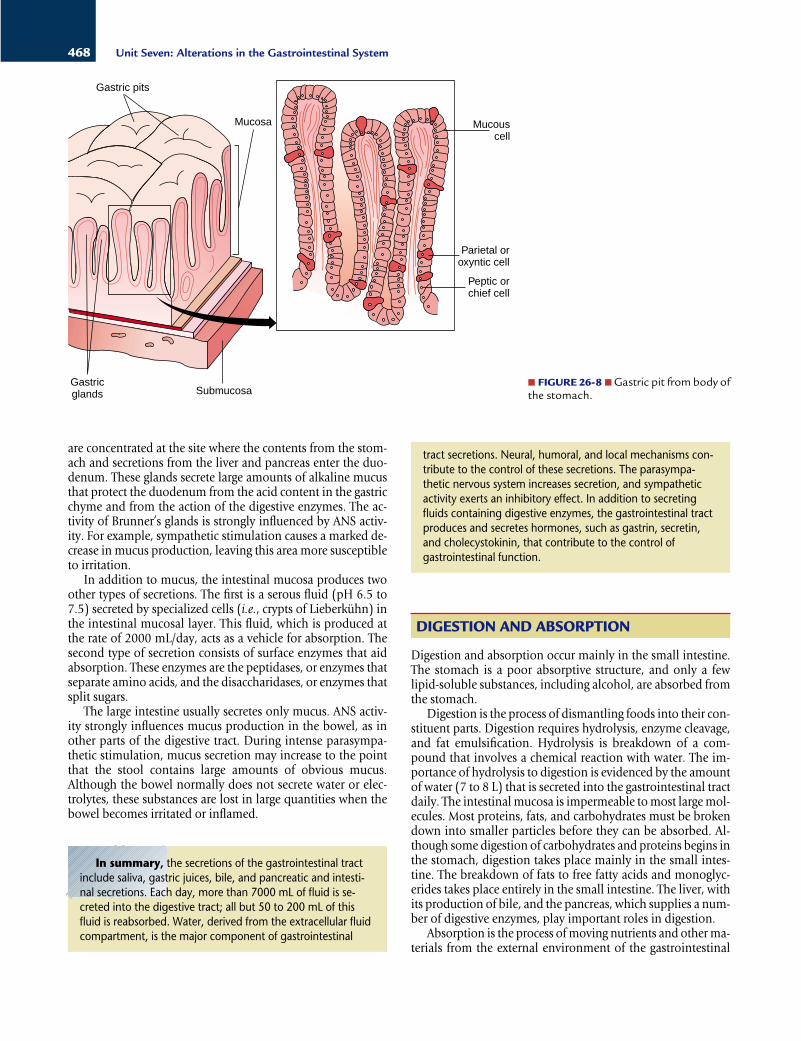
Gastric SecretionsIn addition to mucus-secreting cells that line the entire sur-face of the stomach, the stomach mucosa has two types ofglands: oxyntic (or gastric) glands and pyloric glands. Theoxyntic glands are located in the proximal 80% (body and fun-dus) of the stomach. They secrete hydrochloric acid, pep-sinogen, intrinsic factor, and mucus. The pyloric glands are lo-cated in the distal 20%, or antrum, of the stomach. Thepyloric glands secrete mainly mucus, some pepsinogen, andthe hormone gastrin.
The oxyntic gland area of the stomach is composed ofglands and pits (Fig. 26-8). The surface area and gastric pits are lined with mucus-producing epithelial cells. The bases ofthe gastric pits contain the parietal (or oxyntic) cells, which se-crete hydrochloric acid and intrinsic factor, and the chief (pep-tic) cells, which secrete large quantities of pepsinogen. Thereare approximately 1 billion parietal cells in the stomach; to-gether they produce and secrete approximately 20 mEq of hydrochloric acid in several hundred milliliters of gastric juiceeach hour. Gastric intrinsic factor, which is produced by theparietal cells, is necessary for the absorption of vitamin B12.The pepsinogen that is secreted by the chief cells is rapidly con-verted to pepsin when exposed to the low pH of the gastricjuices.
One of the important characteristics of the gastric mucosa isresistance to the highly acid secretions that it produces. Whenthe gastric mucosa is damaged by aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), ethyl alcohol, or bile salts, thisresistance is disrupted, and hydrogen ions move into the mu-cosal cells. As the hydrogen ions accumulate in the mucosalcells, intracellular pH decreases, enzymatic reactions becomeimpaired, and cellular structures are disrupted. The result is lo-cal ischemia and tissue necrosis. The mucosal surface is furtherprotected by prostaglandins.
Parasympathetic stimulation (through the vagus nerve) andgastrin increase gastric secretions. Histamine increases gastricacid secretions. Gastric acid secretion and its relation to pepticulcer are discussed in Chapter 27.
Intestinal SecretionsThe small intestine secretes digestive juices and receives secre-tions from the liver and pancreas (see Chapter 28). An exten-sive array of mucus-producing glands, called Brunner’s glands,
467Chapter 26: Structure and Function of the Gastrointestinal System
Major Gastrointestinal Hormones and Their ActionsTABLE 26-2
Cholecystokinin
Gastrin
Secretin
Duodenum, jejunum
Antrum of the stomach,duodenum
Duodenum
Hormone Site of Secretion Stimulus for Secretion Action
Products of protein digestion and longchain fatty acids
Vagal stimulation; epinephrine; neutralamino acids; calcium-containing fluidssuch as milk; and alcohol. Secretion isinhibited by acid contents in the an-trum of the stomach (below pH 2.5)
Acid pH or chyme entering duodenum(below pH 3.0)
Stimulates contraction of the gallbladder; stimulates secretion of pancreatic enzymes;slows gastric emptying
Stimulates secretion of gastric acid and pep-sinogen; increases gastric blood flow; stimu-lates gastric smooth muscle contraction; stimulates growth of gastric, small intestine,and colon mucosa
Stimulates secretion of bicarbonate-containingsolution by pancreas and liver
are concentrated at the site where the contents from the stom-ach and secretions from the liver and pancreas enter the duo-denum. These glands secrete large amounts of alkaline mucusthat protect the duodenum from the acid content in the gastricchyme and from the action of the digestive enzymes. The ac-tivity of Brunner’s glands is strongly influenced by ANS activ-ity. For example, sympathetic stimulation causes a marked de-crease in mucus production, leaving this area more susceptibleto irritation.
In addition to mucus, the intestinal mucosa produces twoother types of secretions. The first is a serous fluid (pH 6.5 to7.5) secreted by specialized cells (i.e., crypts of Lieberkühn) inthe intestinal mucosal layer. This fluid, which is produced atthe rate of 2000 mL/day, acts as a vehicle for absorption. Thesecond type of secretion consists of surface enzymes that aidabsorption. These enzymes are the peptidases, or enzymes thatseparate amino acids, and the disaccharidases, or enzymes thatsplit sugars.
The large intestine usually secretes only mucus. ANS activ-ity strongly influences mucus production in the bowel, as inother parts of the digestive tract. During intense parasympa-thetic stimulation, mucus secretion may increase to the pointthat the stool contains large amounts of obvious mucus.Although the bowel normally does not secrete water or elec-trolytes, these substances are lost in large quantities when thebowel becomes irritated or inflamed.
DIGESTION AND ABSORPTION
Digestion and absorption occur mainly in the small intestine.The stomach is a poor absorptive structure, and only a fewlipid-soluble substances, including alcohol, are absorbed fromthe stomach.
Digestion is the process of dismantling foods into their con-stituent parts. Digestion requires hydrolysis, enzyme cleavage,and fat emulsification. Hydrolysis is breakdown of a com-pound that involves a chemical reaction with water. The im-portance of hydrolysis to digestion is evidenced by the amountof water (7 to 8 L) that is secreted into the gastrointestinal tractdaily. The intestinal mucosa is impermeable to most large mol-ecules. Most proteins, fats, and carbohydrates must be brokendown into smaller particles before they can be absorbed. Al-though some digestion of carbohydrates and proteins begins inthe stomach, digestion takes place mainly in the small intes-tine. The breakdown of fats to free fatty acids and monoglyc-erides takes place entirely in the small intestine. The liver, withits production of bile, and the pancreas, which supplies a num-ber of digestive enzymes, play important roles in digestion.
Absorption is the process of moving nutrients and other ma-terials from the external environment of the gastrointestinal
468 Unit Seven: Alterations in the Gastrointestinal System
Peptic orchief cell
Gastricglands
Mucouscell
Gastric pits
Mucosa
Submucosa
Parietal oroxyntic cell
■ FIGURE 26-8 ■ Gastric pit from body ofthe stomach.
In summary, the secretions of the gastrointestinal tractinclude saliva, gastric juices, bile, and pancreatic and intesti-nal secretions. Each day, more than 7000 mL of fluid is se-creted into the digestive tract; all but 50 to 200 mL of thisfluid is reabsorbed. Water, derived from the extracellular fluidcompartment, is the major component of gastrointestinal
tract secretions. Neural, humoral, and local mechanisms con-tribute to the control of these secretions. The parasympa-thetic nervous system increases secretion, and sympatheticactivity exerts an inhibitory effect. In addition to secreting fluids containing digestive enzymes, the gastrointestinal tractproduces and secretes hormones, such as gastrin, secretin,and cholecystokinin, that contribute to the control ofgastrointestinal function.

tract into the internal environment. Absorption is accomplishedby active transport and diffusion. The absorptive function ofthe large intestine focuses mainly on water reabsorption. Anumber of substances require a specific carrier or transport sys-tem. For example, vitamin B12 is not absorbed in the absence ofintrinsic factor, which is secreted by the parietal cells of thestomach. Transport of amino acids and glucose occurs mainlyin the presence of sodium. Water is absorbed passively alongan osmotic gradient.
The distinguishing characteristic of the small intestine is itslarge surface area, which in the adult is estimated to be ap-proximately 250 m2. Anatomic features that contribute to thisenlarged surface area are the circular folds that extend into thelumen of the intestine and the villi, which are finger-like pro-jections of mucous membrane, numbering as many as 25,000,that line the entire small intestine (Fig. 26-9). Each villus isequipped with an arrangement of blood vessels for the ab-sorption of fluid and dissolved material into the portal bloodand a central lacteal for absorption into the lymph (Fig. 26-10).Fats rely largely on the lymphatics for absorption.
Each villus is covered with cells called enterocytes that con-tribute to the absorptive and digestive functions of the smallbowel, and goblet cells that provide mucus. The crypts ofLieberkühn are glandular structures that open into the spacesbetween the villi. The enterocytes have a life span of approxi-mately 4 to 5 days; their replacement cells differentiate fromprogenitor cells located in the area of the crypts. The maturingenterocytes migrate up the villus and eventually are extrudedfrom the tip.
The enterocytes secrete enzymes that aid in the digestion ofcarbohydrates and proteins. These enzymes are called brushborder enzymes because they adhere to the border of the villusstructures. In this way they have access to the carbohydratesand protein molecules as they come in contact with the ab-sorptive surface of the intestine. This mechanism of secretionplaces the enzymes where they are needed and eliminates theneed to produce enough enzymes to mix with the entire con-tents that fill the lumen of the small bowel. The digested mol-
ecules diffuse through the membrane or are actively trans-ported across the mucosal surface to enter the blood or, in thecase of fatty acids, the lacteal. These molecules are then trans-ported through the portal vein or lymphatics into the systemiccirculation.
CarbohydratesCarbohydrates must be broken down into monosaccharides, orsingle sugars, before they can be absorbed from the small in-testine. The average daily intake of carbohydrate in theAmerican diet is approximately 350 to 400 g. Starch makes upapproximately 50% of this total, sucrose (i.e., table sugar) ap-proximately 30%, lactose (i.e., milk sugar) approximately 6%,and maltose approximately 1.5%.
Digestion of starch begins in the mouth with the action ofamylase. Pancreatic secretions also contain an amylase. Amy-lase breaks down starch into several disaccharides, includingmaltose, isomaltose, and α-dextrins. The brush border en-zymes convert the disaccharides into monosaccharides that canbe absorbed (Table 26-3). Sucrose yields glucose and fructose,lactose is converted to glucose and galactose, and maltose isconverted to two glucose molecules. When the disaccharidesare not broken down to monosaccharides, they cannot be ab-sorbed but remain as osmotically active particles in the con-tents of the digestive system, causing diarrhea. Persons who aredeficient in lactase, the enzyme that breaks down lactose, ex-perience diarrhea when they drink milk or eat dairy products.
Fructose is transported across the intestinal mucosa by fa-cilitated diffusion, which does not require energy expenditure.In this case, fructose moves along a concentration gradient.Glucose and galactose are transported by way of a sodium-dependent carrier system that uses adenosine triphosphate andthe Na+/K+-ATPase pump as an energy source (Fig. 26-11).
469Chapter 26: Structure and Function of the Gastrointestinal System
Circularmuscle Longitudinal
muscle Lymphnode
Serosa
Submucosa
Mucosalmuscle
Villus
Crypt ofLieberkuhn
..
■ FIGURE 26-9 ■ The mucous membrane of the small intestine.Note the numerous villi on a circular fold.
■ FIGURE 26-10 ■ A single villus from the small intestine.
Enterocyte being extrudedfrom a villus
Enterocyte
Vein
Artery
Lacteal
Crypt ofLieberkühn
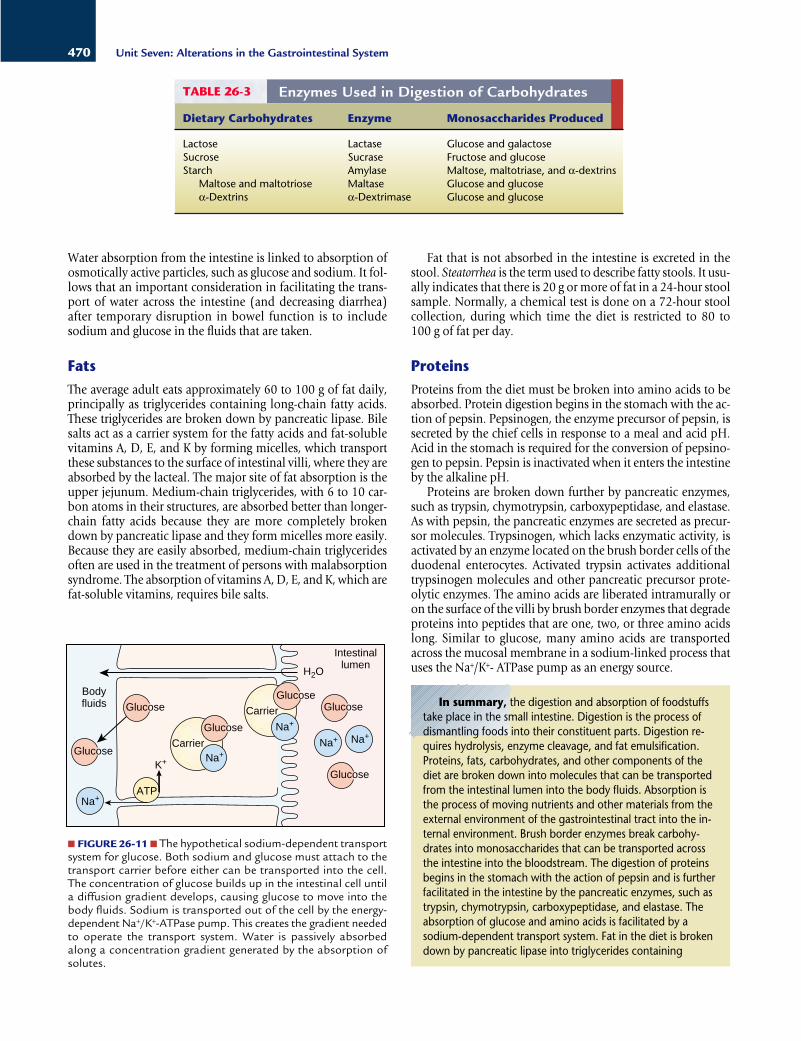
Water absorption from the intestine is linked to absorption ofosmotically active particles, such as glucose and sodium. It fol-lows that an important consideration in facilitating the trans-port of water across the intestine (and decreasing diarrhea)after temporary disruption in bowel function is to includesodium and glucose in the fluids that are taken.
FatsThe average adult eats approximately 60 to 100 g of fat daily,principally as triglycerides containing long-chain fatty acids.These triglycerides are broken down by pancreatic lipase. Bilesalts act as a carrier system for the fatty acids and fat-solublevitamins A, D, E, and K by forming micelles, which transportthese substances to the surface of intestinal villi, where they areabsorbed by the lacteal. The major site of fat absorption is theupper jejunum. Medium-chain triglycerides, with 6 to 10 car-bon atoms in their structures, are absorbed better than longer-chain fatty acids because they are more completely brokendown by pancreatic lipase and they form micelles more easily.Because they are easily absorbed, medium-chain triglyceridesoften are used in the treatment of persons with malabsorptionsyndrome. The absorption of vitamins A, D, E, and K, which arefat-soluble vitamins, requires bile salts.
Fat that is not absorbed in the intestine is excreted in thestool. Steatorrhea is the term used to describe fatty stools. It usu-ally indicates that there is 20 g or more of fat in a 24-hour stoolsample. Normally, a chemical test is done on a 72-hour stoolcollection, during which time the diet is restricted to 80 to 100 g of fat per day.
ProteinsProteins from the diet must be broken into amino acids to beabsorbed. Protein digestion begins in the stomach with the ac-tion of pepsin. Pepsinogen, the enzyme precursor of pepsin, issecreted by the chief cells in response to a meal and acid pH.Acid in the stomach is required for the conversion of pepsino-gen to pepsin. Pepsin is inactivated when it enters the intestineby the alkaline pH.
Proteins are broken down further by pancreatic enzymes,such as trypsin, chymotrypsin, carboxypeptidase, and elastase.As with pepsin, the pancreatic enzymes are secreted as precur-sor molecules. Trypsinogen, which lacks enzymatic activity, isactivated by an enzyme located on the brush border cells of theduodenal enterocytes. Activated trypsin activates additionaltrypsinogen molecules and other pancreatic precursor prote-olytic enzymes. The amino acids are liberated intramurally oron the surface of the villi by brush border enzymes that degradeproteins into peptides that are one, two, or three amino acidslong. Similar to glucose, many amino acids are transportedacross the mucosal membrane in a sodium-linked process thatuses the Na+/K+- ATPase pump as an energy source.
470 Unit Seven: Alterations in the Gastrointestinal System
Enzymes Used in Digestion of CarbohydratesTABLE 26-3
Lactose Lactase Glucose and galactoseSucrose Sucrase Fructose and glucoseStarch Amylase Maltose, maltotriase, and α-dextrins
Maltose and maltotriose Maltase Glucose and glucoseα-Dextrins α-Dextrimase Glucose and glucose
Dietary Carbohydrates Enzyme Monosaccharides Produced
Intestinallumen
Na+Na+
Na+
Na+
Na+
Glucose
Glucose
Carrier
Carrier
Bodyfluids
ATP
H2O
K+
Glucose
Glucose
Glucose
Glucose
■ FIGURE 26-11 ■ The hypothetical sodium-dependent transportsystem for glucose. Both sodium and glucose must attach to thetransport carrier before either can be transported into the cell.The concentration of glucose builds up in the intestinal cell untila diffusion gradient develops, causing glucose to move into thebody fluids. Sodium is transported out of the cell by the energy-dependent Na+/K+-ATPase pump. This creates the gradient neededto operate the transport system. Water is passively absorbedalong a concentration gradient generated by the absorption ofsolutes.
In summary, the digestion and absorption of foodstuffstake place in the small intestine. Digestion is the process ofdismantling foods into their constituent parts. Digestion re-quires hydrolysis, enzyme cleavage, and fat emulsification.Proteins, fats, carbohydrates, and other components of thediet are broken down into molecules that can be transportedfrom the intestinal lumen into the body fluids. Absorption isthe process of moving nutrients and other materials from theexternal environment of the gastrointestinal tract into the in-ternal environment. Brush border enzymes break carbohy-drates into monosaccharides that can be transported acrossthe intestine into the bloodstream. The digestion of proteinsbegins in the stomach with the action of pepsin and is furtherfacilitated in the intestine by the pancreatic enzymes, such astrypsin, chymotrypsin, carboxypeptidase, and elastase. Theabsorption of glucose and amino acids is facilitated by asodium-dependent transport system. Fat in the diet is brokendown by pancreatic lipase into triglycerides containing

medulla near the sensory nuclei of the vagus. The chemore-ceptor trigger zone is located in a small area on the floor of thefourth ventricle, where it is exposed to both blood and cere-brospinal fluid. It is thought to mediate the emetic effects ofblood-borne drugs and toxins.
The act of vomiting consists of taking a deep breath, closingthe airways, and producing a strong, forceful contraction of thediaphragm and abdominal muscles along with relaxation ofthe gastroesophageal sphincter. Respiration ceases during theact of vomiting. Vomiting may be accompanied by dizziness,light-headedness, decrease in blood pressure, and bradycardia.
The vomiting center receives input from the gastrointestinaltract and other organs; from the cerebral cortex; from thevestibular apparatus, which is responsible for motion sickness;and from the chemoreceptor trigger zone, which is activated bymany drugs and endogenous and exogenous toxins. Hypoxiaexerts a direct effect on the vomiting center, producing nauseaand vomiting. This direct effect probably accounts for the vom-iting that occurs during periods of decreased cardiac output,shock, environmental hypoxia, and brain ischemia caused byincreased intracranial pressure. Inflammation of any of theintra-abdominal organs, including the liver, gallbladder, or uri-nary tract, can cause vomiting because of the stimulation of thevisceral afferent pathways that communicate with the vomitingcenter. Distention or irritation of the gastrointestinal tract alsocauses vomiting through the stimulation of visceral afferentneurons.
Several neurotransmitters and receptor subtypes are impli-cated as neuromediators in nausea and vomiting. Dopamine,serotonin, and opioid receptors are found in the gastro-intestinal tract and in the vomiting and chemoreceptor triggerzone. Dopamine antagonists, such as prochlorperazine, de-press vomiting caused by stimulation of the chemoreceptortrigger zone. Serotonin is believed to be involved in the nauseaand emesis associated with cancer chemotherapy and radiationtherapy. Serotonin antagonists (e.g., granisetron and ondan-setron) are effective in treating the nausea and vomiting asso-ciated with these stimuli. Motion sickness appears to be acentral nervous system (CNS) response to vestibular stimuli.Norepinephrine and acetylcholine receptors are located in thevestibular center. The acetylcholine receptors are thought tomediate the impulses responsible for exciting the vomiting cen-ter; norepinephrine receptors may have a stabilizing influencethat resists motion sickness. Many of the motion sickness drugs(e.g., dimenhydrinate) have a strong CNS anticholinergic effectand act on the receptors in the vomiting center and areas re-lated to the vestibular system.
471Chapter 26: Structure and Function of the Gastrointestinal System
ANOREXIA, NAUSEA, AND VOMITING
Anorexia, nausea, and vomiting are physiologic responses thatare common to many gastrointestinal disorders. These re-sponses are protective to the extent that they signal the presenceof disease and, in the case of vomiting, remove noxious agentsfrom the gastrointestinal tract. They also can contribute to im-paired intake or loss of fluids and nutrients.
AnorexiaAnorexia represents a loss of appetite. Several factors influenceappetite. One is hunger, which is stimulated by contractions ofthe empty stomach. Appetite or the desire for food intake is reg-ulated by the hypothalamus and other associated centers in thebrain (see Chapter 29). Smell plays an important role, as evi-denced by the fact that appetite can be stimulated or sup-pressed by the smell of food. Loss of appetite is associated withemotional factors, such as fear, depression, frustration, andanxiety. Many drugs and disease states cause anorexia. For ex-ample, in uremia the accumulation of nitrogenous wastes inthe blood contributes to the development of anorexia. Anore-xia often is a forerunner of nausea, and most conditions thatcause nausea and vomiting also produce anorexia.
NauseaNausea is an ill-defined and unpleasant subjective sensation. Itis the conscious sensation resulting from stimulation of themedullary vomiting center that often precedes or accompaniesvomiting. Nausea usually is preceded by anorexia, and stimulisuch as foods and drugs that cause anorexia in small doses usu-ally produce nausea when given in larger doses. A commoncause of nausea is distention of the duodenum or upper smallintestinal tract. Nausea frequently is accompanied by auto-nomic nervous system manifestations such as watery salivationand vasoconstriction with pallor, sweating, and tachycardia.Nausea may function as an early warning signal of a pathology.
VomitingVomiting, or emesis, is the sudden and forceful oral expulsionof the contents of the stomach. It usually is preceded by nau-sea. The contents that are vomited are called vomitus. Vomit-ing, as a basic physiologic protective mechanism, limits thepossibility of damage from ingested noxious agents by empty-ing the contents of the stomach and portions of the small in-testine. Nausea and vomiting may represent a total-body re-sponse to drug therapy, including overdosage, cumulativeeffects, toxicity, and side effects.
Vomiting involves two functionally distinct medullary cen-ters: the vomiting center and the chemoreceptor trigger zone.The act of vomiting is integrated by the vomiting center, whichis located in the dorsal portion of the reticular formation of the
In summary, the signs and symptoms of many gastro-intestinal tract disorders are manifested by anorexia, nausea,and vomiting. Anorexia, or loss of appetite, may occur aloneor may accompany nausea and vomiting. Nausea, which is anill-defined, unpleasant sensation, signals the stimulation of themedullary vomiting center. It often precedes vomiting andfrequently is accompanied by autonomic responses, such assalivation and vasoconstriction with pallor, sweating, andtachycardia. The act of vomiting, which is integrated by thevomiting center, involves the forceful oral expulsion of thegastric contents. It is a basic physiologic mechanism that ridsthe gastrointestinal tract of noxious agents.
medium- and long-chain fatty acids. Bile salts form micellesthat transport these substances to the surface of intestinal villi,where they are absorbed.

Visit the Connection site at connection.lww.com/go/porthfor links to chapter-related resources on the Internet.
BIBLIOGRAPHYBerne R.M., Levy M.N. (1997). Principles of physiology (3rd ed., pp. 354–
400). St. Louis: C.V. Mosby.Ganong W.F. (1999). Review of medical physiology (19th ed., 459–491).
Stanford: Appleton & Lange.Gershon M.D. (1999). The enteric nervous system: A second brain.
Hospital Practice 34 (7), 31–52.Guyton A.C., Hall J.E. (2000). Textbook of medical physiology (10th ed.,
pp. 718–770). Philadelphia: W.B. Saunders.Johnson L.R. (2001). Gastrointestinal physiology (6th ed.). St. Louis: C.V.
Mosby.
472 Unit Seven: Alterations in the Gastrointestinal System
REVIEW QUESTIONS■ Describe the physiologic function of the digestive system interms of transport of food, digestion, absorption of nutrients,and storage of waste products.
■ Approximately 7000 mL of fluid is secreted into the gastro-intestinal tract, with only about 200 mL being eliminated in thestool. Explain the source, composition, function, and removalof this fluid from the gastrointestinal tract.
■ Describe the site of gastric acid and pepsin production andsecretion in the stomach.
■ Describe the function of the gastric mucosal barrier.
■ Relate the characteristics of the small intestine to its absorp-tive function and explain the function of intestinal brush borderenzymes in the digestion and absorption of carbohydrates, fats,and proteins.
■ Explain the relationship between the enteric nervous systemand the autonomic nervous system in the regulation of gastro-intestinal function.
■ Describe the innervation of the reflexive and voluntarycomponents of defecation.













![Motilidade gastrointestinal [Modo de Compatibilidade] · MOTILIDADE GASTROINTESTINAL Objetivo: Estudar os mecanismos fisiológicos responsáveis pela motilidade gastrointestinal Roteiro:](https://static.fdocument.pub/doc/165x107/5ba2c53109d3f208588c90c2/motilidade-gastrointestinal-modo-de-compatibilidade-motilidade-gastrointestinal.jpg)