Acute Acalculous Cholecystitis
24
Acute acalculous cholecystitis Presented by Ri 郎正麟
-
Upload
triciazulueta -
Category
Documents
-
view
25 -
download
1
Transcript of Acute Acalculous Cholecystitis
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 1/24
Acute acalculous cholecystitis
Presented by Ri 郎正麟
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 2/24
Etiology• Etiology:
– Western: 10~15 % of acute cholecystitis
eMedicine journal, Jan 7 2002 vol 3,No.1
– China: 58/258--22.48% 湖北醫科大學研究 1998
– Japanese series: 0.64% after gastrectomy
– post-operation: fifth to seventh decade, female
dominant – trauma or burn: second to fourth decades, male
dominant Oxford textbook of Surgery
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 3/24
Predisposing factor
Most seen in ICU patients with severe illness• multiple trauma
• extensive burn
• major surgery
• sepsis
• TPN use
• opiates analgesia• anesthesia
• HIV infection The ICU Book 1998; p531-2
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 4/24
Pathophysiology-I
• depressed motility and starvation: trauma, burns,surgery, TPN, anesthesia, narcotics
– 2~14% after major trauma or burn J. Burn Care and Reha. 18(2):141-6, 1997 May-Apr
• decrease blood flow through cystic artery: CHF,arteriosclerosis, polyarteritis nodosa, SLE,
diabetes, shock
• obstruction of cystic duct by extrinsic
inflammation, lymphadenopathy, metastasis
• infection: Salmonella, cholera, ascaris, CMV
Kawasaki’s disease Am Sur. 1983 May, 49(5):175-7
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 5/24
Pathophysiology-II
• 57 p’ts AAC treated over a 9-years periods
– type I (trauma or critical illness, N=24): 45.8%
mortality, 66.7% acute ischemic cholecystitis, pre-op
Dx:50% – type II (s/s of acute cholecystitis N=20): 5% mortality,
50% acute on chronic cholecystitis, pre-op Dx: 90%
– type III (non-calculous gallbladder outflow obstruction,
N=13): 23.1% mortality, obstructive pathology, pre-opDx:15.4%
• AAC distinct clinical-pathological variant
of the disease S Afr J Surg 1999 Nov;37(4):99-104
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 6/24
Pathophysiology-III
• Impaired smooth muscle contractility-->the pathophysiology of acalculous cholecystitis
– in common bile duct ligation(CBDL) guinea pigs , electric stimulation
to activate intrinsic muscle
– H&E stained of muscle strips – a. progressive increase the inflammation and decrease the muscle
contractility to Ach
– b. nitric oxide synthase inhibitor increase
• CBDL affects the gallbladder contractility by two mechanism:
– 1. Decrease smooth muscle contractility
– 2. Decrease neurally mediated contractions--
• dysfunction of cholinergic excitory nerves
• upregulation of NO-mediated inhibition of smooth m. contractility
J Surg Res 2000 Feb;88(2):186-192
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 7/24
Pathophysiology-IV
• Acaculous cholecystitis induced by intra-
abdominal sepsis
– ligation and prick of the cecum in 25 animals
– varies degree of cholecystitis
– bile culture in 15 alive animals: 10 negative, 5
positive
– Streptococcus Fracalis and Streptococcus Sp.
• AAC in early stage induced by inflammatory process, and
infection of the bile represent a late event
Acta Biomed Ateneo Parmense 1996;67(1-2):61-7
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 8/24
Histopathology
• gall bladder edema of the serosa and
muscular layer, with patchy thrombosis of
arterioles and venules• area of necrosis develop and affect the
underlying mucosa
may due to factor VII activation lead to bloodvessel thrombosis in the seromuscular layer of the
gallbladderOxford textbook of Surgery

5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 9/24
Clinical presentation-I:
• Symptoms: – fever (70~95%)
– RUQ pain with tenderness (60~100%)
– nausea and vomiting (35~65%)
– abdominal pain (60~90%) The ICU Book 1998; p531-2
• Physical exam: vary with the severity – right hypochondrial tenderness
– muscle guarding, rigidity, rebound tenderness
– some degree of fever
– tachycardia
– Murphy’s sign: variable eMedicine J.Jan 7 2002, Vol 3 No.1

5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 10/24
Clinical presentation-II:
• Laboratory finding:
– ALT/AST: mildly raised
– alkaline phosphate: mildly elevated
– bilirubin: variable, may rise to 85 mol/l
– CBC/DC: elevated due to acute inflammation
eMedicine J.Jan 7 2002, Vol 3 No.1

5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 11/24
Images studies-I• Ultrasound: the most useful diagnosis tool
– gallbladder wall thickness>4 mm with an
increase in its volume (vesicular hydrop)
– sonographic Murphy’s sign
– biliary sludge in a tender thickened gallbladder
but fail to demostrate stones
– intramural gas, pericholecystic fluid or
sloughed mucosa – no intrahepatic or extrahepatic ducts dilatation
– color doppler scan to r/o ischemia condition
eMedicine J.Jan 7 2002, Vol 3 No.1
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 12/24
Images studies-II• Evaluate sonographic abnormalities of gallbladder
other than acalculous cholecystitis
– 55 p’t in ICU, US/every 2 weeks, calculi exclude (11/55)
– sonographic features of acalculous cholecystitis:
• a. gallbladder wall thickening d. pericholecystic fluid• b. gallbladder distension e. gallbladder sludge
• c. intramural gallbladder lucencies f. Murphy’s sign
– correlated with clinical and laboratory finding
– echo result: 30/44 (84%): at least one; 25/44 (57%):2~3; 6/44 (14%): 4~5
• gallbladder abnormalities are frequently seen on
US in ICU patient Am L Roentgenol 2000 Apr;174(4):973-7
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 13/24
Images studies-III• morphine cholescintigraphy :
– highly sensitive (95%) but poor specific (38%)
• CT scan:
– periportal inflammation and gall bladder walledema
– r/o other differential diagnosis
• PES and ERCP: – r/o other differential diagnosis
eMedicine J.Jan 7 2002, Vol 3 No.1
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 14/24
Images studies-IV
• Cholescintigraphy to the early diagnosis of acuteacalculous cholecystitis in ICU patients
• 32 p’t (78% with TPN)--suspected AAC
• underwent Tc-99m mebrofenin cholescitigraphy, morphine
sulphate administered if GB was not viualised after1 hr(16p’t)
• final Dx: clinical improvement, another etiology for symptom
presented or histopathology following cholecystectomy
• finding:
– I: non-visualization of gallbladder during the first 60’
– II: persistent non-visualization 30’ following morphine administration
– III: non-visualization of the small bowel for at least 90’
• 79% sensitivity and 100% specificity using the criteria “I and
II or III” Eur J Nucl Med 1999 Oct;26(10):1317-25
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 15/24
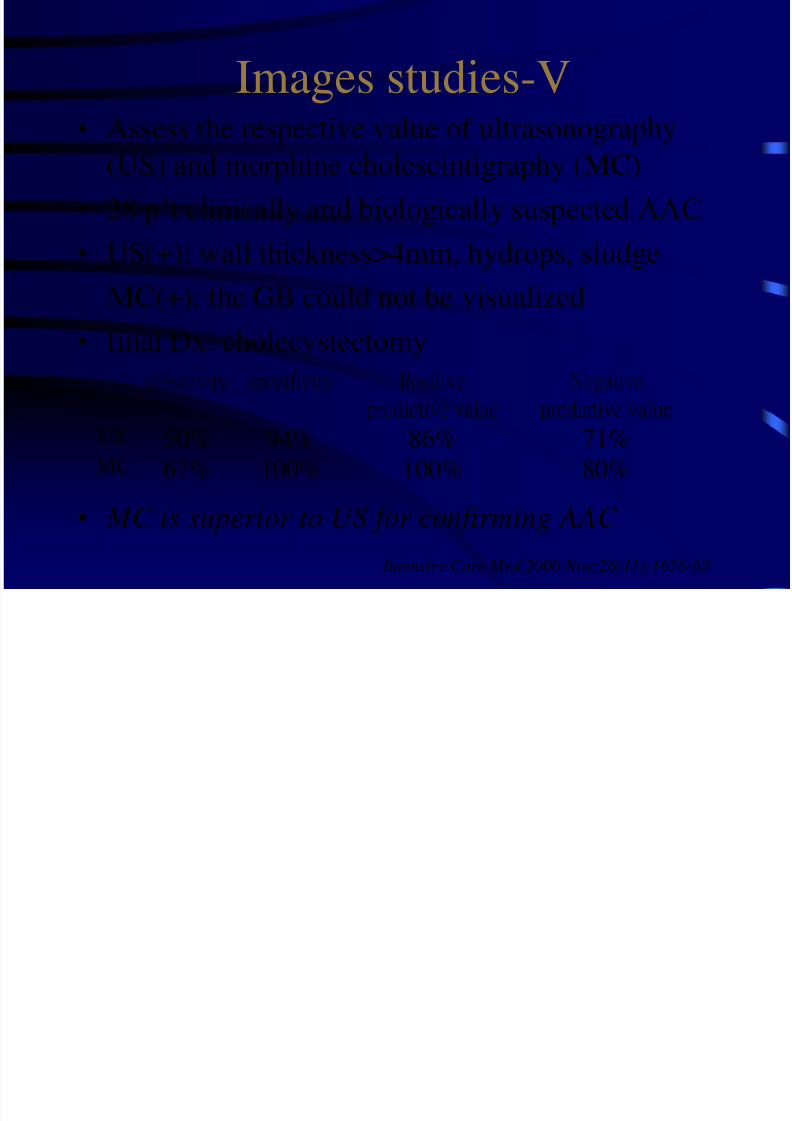
Images studies-V
• Assess the respective value of ultrasonography(US) and morphine cholescintigraphy (MC)
• 28 p’t clinically and biologically suspected AAC
• US(+): wall thickness>4mm, hydrops, sludge
MC(+): the GB could not be visualized
• final Dx: cholecystectomy
• MC is superior to US for confirming AAC
Intensive Care Med 2000 Nov;26(11):1658-63
sensitivity specificity Positive
predictive value
Negative
predictive valueUS 50% 94% 86% 71%
MC 67% 100% 100% 80%
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 16/24
Differential diagnosis
• Bile duct stricture
• biliary colic
• biliary disease
• biliary obstruction
• choledocholithiasis
• cholelithiasis• duodenal ulcer
• gallbladder cancer
• Gastric ulcer
• gastritis
• viral hepatitis
• irritable bowel
syndrome
• acute/chronicpancreatitis
eMedicine J.Jan 7 2002, Vol 3 No.1
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 17/24
Clinical events-I• AAC in p’ts with severe trauma
– 28 p’ts with contusion severe trauma
– US every 5~7 days for early detection
– 7 p’ts developed sono change starting 9th days – 4 proved histologically, 3 underwent
cholecystectomy; the other died due to hypovolemia
• US easily detect the GB morphological change• no morbidity or mortality due to
cholecystectomy Rev Gastroenterol Mex 1996 Oct-Dec;61(4):348-55
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 18/24
Clinical events-II
• AAC after aortic reconstruction
– 7/996 p’t during 1987~1997, retrospectively
– 6 p’ts had prolonged intraoperative hypotension
and increase blood transfusion
– s/s: developed fever, leukocytosis. LFT
elevation in a mean of 32 days after operation
– 5 p’ts underwent cholecystectomy, 2 p’ts hadplacement of cholecystostomy tubes
– gangrene or perforation was evident
– overall mortality: 71% J Am Coll Surg 1997 Mar;184(3):245-8

5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 19/24
Clinical events-III
• AAC in patients with surgical acute renal
failure
– 11/143 p’ts with surgical acute renal failure
– Dx: clinical, US, lab finding
– received Abx at the time of diagnosis
– 5 p’ts treated conservatively, 6 p’ts underwent
cholecystectomy
– mortality rate: 45.5%, no significant different
from ARF without AAC
Acta Med Croatica 2000;54(1):15-20
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 20/24
Clinical events-IV
• GB abnormalities in MICU: ultrasound study
– 30 p’ts estimate US in the first 2 days, 2 exclude
due to previous cholecystectomy – 61%(17/28) considering acute acalculous
cholecystitis
– 3 major finding under US: 25% sludge, 22% wallthickening, 11% hydrops
– none of these p’ts needed a surgical procedure
Intensive Care Med 1996 Apr;22(4):356-8
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 21/24
Clinical events-V
• AAC in China
– 58/258 in acute cholecystitis
– Dx: 1.symptoms, 2. Signs, 3.Lab, 4. Image
– M:F:1.07:1; <60 y/o: 70.69%; less systemic disease
– no shock, no heart failure, no mortality
– all medical treatment
– etiology: 13/58: gastropathy; 5/58: HTN or angina;3/58: GB polyp; 1/58: ascaris; 1/58:GB ca; 7/58:Hx
of op; 3/58: pancreatic disease 湖北醫科大學研究 1998
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 22/24
Clinical events-VI
• AAC: incidence, risk factor, diagnosis, and outcome
• 53 m/o, 27 cases(M:17, F:10)
• 14(52%) in critical ill p’ts, 17(63%) from non-biliary tract
operation, 0.19% in SICU p’ts • image: MC (90% sensitivity), CT (67%), US(29%)
• AAC associate complication: gangrene(63%),
perforation(15%), abscess(4%)
• total mortality: 41%
To improve outcome, a high index of suspision with early
radiologic evaluation and multiple studies is necessary. Am Surg 1998 May;64(5):471-5
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 23/24
Treatment
• medical treatment: no effective?
• initially antibiotic given: vancomycin
+imipenem• Immediate cholecystectomy: larparoscopic
or laparotomy
• percutaneous cholecystosotomy withexternal biliary drainage
eMedicine J.Jan 7 2002, Vol 3 No.1
5/16/2018 Acute Acalculous Cholecystitis - slidepdf.com
http://slidepdf.com/reader/full/acute-acalculous-cholecystitis-55ab55e2341fc 24/24
Thanks for your attention!!