A nodular buccal mass
5
A nodular buccal mass Hiroyuki Yamada, DDS, PhD, a Kenji Mishima, DDS, PhD, b Koji Kawaguchi, DDS, PhD, a Toshikatsu Horiuchi, DDS, c Kazutoshi Nakaoka, DDS, PhD, c Mitsuyoshi Iino, DDS, PhD, d Ichiro Saito, DDS, PhD, e and Yoshiki Hamada, DDS, PhD, f Yokohama and Tokyo, Japan TSURUMI UNIVERSITY SCHOOL OF DENTAL MEDICINE, YAMAGATA UNIVERSITY, AND UNIVERSITY OF TOKYO HOSPITAL (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:140-144) CASE PRESENTATION A 22-year-old man was referred to the Department of Oral and Maxillofacial Surgery, Tsurumi University Dental Hos- pital, for diagnosis and treatment of a left buccal nodule (Fig. 1), which he reported having for approximately 1 month. As the nodule grew in size, pain increased during mouth opening. The patient had not experienced any fever; there was no history of traumatic injury, and his medical and family his- tories were unremarkable. Physical examination revealed a rubbery immobile mass measuring 30 mm in diameter in the left buccal region. Overlying skin and oral mucosa were normal. No bruits or pulsations were present over the mass, and salivary secretion of the left parotid gland was not dis- turbed. There was neither neuroparalysis nor cervical lymph- adenopathy. Panoramic radiography showed that the dentition was in good condition. Computerized tomography (CT) images were obtained im- mediately after intravenous administration of contrast mate- rial, revealing a regularly shaped mass measuring 30 20 mm within the left masseter muscle. The mass was slightly and homogeneously enhanced. No bone destruction of the left mandibular ramus was noted (Fig. 2). T1-Weighted magnetic resonance imaging (MRI) revealed an isointense signal, confirming its location in the left mas- seter muscle (Fig. 3, A). The T2-weighted images revealed a homogeneous increase in signal intensity within the mass (Fig. 3, B). DIFFERENTIAL DIAGNOSIS Differential diagnosis of a buccal mass with rela- tively rapid growth includes various cysts, hemato- mas, an intramasseteric abscess, masseteric hypertro- phy, salivary gland neoplasms, and other benign and malignant tumors. Cystic lesions (e.g. dermoid cysts or salivary duct cysts) were clearly excluded by the CT findings, because fluid in the cysts would not have demon- strated enhancement by the contrast material. The absence of any history of trauma excluded hema- toma. Additionally, an intramasseteric abscess was unlikely, because there was no redness of the skin or oral mucosa over the mass and the patient had been without fever. Masseteric hypertrophy is a benign condition char- acterized by an enlargement of the bilateral masseter muscle which can appear as a homogeneous enlarge- ment on MRI. 1 In the present case however, MRI demonstrated a mass lesion. A salivary gland neoplasm was a possibility, because the lesion was in close proximity to both the parotid gland and the minor salivary glands of the buccal mucosa. Additionally, T1-weighted MRI showed an isointense mass located within the masseter muscle, and the T2-weighted image showed an increase in a Lecturer, Department of Oral and Maxillofacial Surgery, Tsurumi University School of Dental Medicine. b Associate Professor, Department of Pathology, Tsurumi University School of Dental Medicine. c Instructor, Department of Oral and Maxillofacial Surgery, Tsurumi University School of Dental Medicine. d Professor, Department of Dentistry, Oral and Maxillofacial Surgery, Plastic and Reconstructive Surgery, Faculty of Medicine, Yamagata University. e Professor, Department of Pathology, Tsurumi University School of Dental Medicine. f Professor, Department of Oral and Maxillofacial Surgery, Tsurumi University School of Dental Medicine. Received for publication Aug 1, 2009; returned for revision Apr 1, 2010; accepted for publication Apr 6, 2010. 1079-2104/$ - see front matter © 2010 Mosby, Inc. All rights reserved. doi:10.1016/j.tripleo.2010.04.013 140 Vol. 110 No. 2 August 2010 CLINICOPATHOLOGIC CONFERENCE Editor: Paul C. Edwards
-
Upload
hiroyuki-yamada -
Category
Documents
-
view
231 -
download
17
Transcript of A nodular buccal mass

Vol. 110 No. 2 August 2010
CLINICOPATHOLOGIC CONFERENCE Editor: Paul C. Edwards
A nodular buccal massHiroyuki Yamada, DDS, PhD,a Kenji Mishima, DDS, PhD,b Koji Kawaguchi, DDS, PhD,a
Toshikatsu Horiuchi, DDS,c Kazutoshi Nakaoka, DDS, PhD,c Mitsuyoshi Iino, DDS, PhD,d
Ichiro Saito, DDS, PhD,e and Yoshiki Hamada, DDS, PhD,f Yokohama and Tokyo, JapanTSURUMI UNIVERSITY SCHOOL OF DENTAL MEDICINE, YAMAGATA UNIVERSITY, AND UNIVERSITYOF TOKYO HOSPITAL
(Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:140-144)CASE PRESENTATIONA 22-year-old man was referred to the Department of Oral
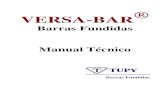
and Maxillofacial Surgery, Tsurumi University Dental Hos-pital, for diagnosis and treatment of a left buccal nodule (Fig.1), which he reported having for approximately 1 month. Asthe nodule grew in size, pain increased during mouth opening.The patient had not experienced any fever; there was nohistory of traumatic injury, and his medical and family his-tories were unremarkable. Physical examination revealed arubbery immobile mass measuring 30 mm in diameter in theleft buccal region. Overlying skin and oral mucosa werenormal. No bruits or pulsations were present over the mass,and salivary secretion of the left parotid gland was not dis-turbed. There was neither neuroparalysis nor cervical lymph-adenopathy. Panoramic radiography showed that the dentitionwas in good condition.
Computerized tomography (CT) images were obtained im-mediately after intravenous administration of contrast mate-rial, revealing a regularly shaped mass measuring 30 � 20
aLecturer, Department of Oral and Maxillofacial Surgery, TsurumiUniversity School of Dental Medicine.bAssociate Professor, Department of Pathology, Tsurumi UniversitySchool of Dental Medicine.cInstructor, Department of Oral and Maxillofacial Surgery, TsurumiUniversity School of Dental Medicine.dProfessor, Department of Dentistry, Oral and Maxillofacial Surgery,Plastic and Reconstructive Surgery, Faculty of Medicine, YamagataUniversity.eProfessor, Department of Pathology, Tsurumi University School ofDental Medicine.fProfessor, Department of Oral and Maxillofacial Surgery, TsurumiUniversity School of Dental Medicine.Received for publication Aug 1, 2009; returned for revision Apr 1,2010; accepted for publication Apr 6, 2010.1079-2104/$ - see front matter© 2010 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2010.04.013140
mm within the left masseter muscle. The mass was slightlyand homogeneously enhanced. No bone destruction of the leftmandibular ramus was noted (Fig. 2).
T1-Weighted magnetic resonance imaging (MRI) revealedan isointense signal, confirming its location in the left mas-seter muscle (Fig. 3, A). The T2-weighted images revealed ahomogeneous increase in signal intensity within the mass(Fig. 3, B).
DIFFERENTIAL DIAGNOSISDifferential diagnosis of a buccal mass with rela-
tively rapid growth includes various cysts, hemato-mas, an intramasseteric abscess, masseteric hypertro-phy, salivary gland neoplasms, and other benign andmalignant tumors.
Cystic lesions (e.g. dermoid cysts or salivary ductcysts) were clearly excluded by the CT findings,because fluid in the cysts would not have demon-strated enhancement by the contrast material. Theabsence of any history of trauma excluded hema-toma. Additionally, an intramasseteric abscess wasunlikely, because there was no redness of the skin ororal mucosa over the mass and the patient had beenwithout fever.
Masseteric hypertrophy is a benign condition char-acterized by an enlargement of the bilateral massetermuscle which can appear as a homogeneous enlarge-ment on MRI.1 In the present case however, MRIdemonstrated a mass lesion.
A salivary gland neoplasm was a possibility, becausethe lesion was in close proximity to both the parotidgland and the minor salivary glands of the buccalmucosa. Additionally, T1-weighted MRI showed anisointense mass located within the masseter muscle,
and the T2-weighted image showed an increase in
OOOOEVolume 110, Number 2 Yamada et al. 141
signal intensity within the mass. These findings areconsistent with both benign and low-grade malignantsalivary gland tumors,2,3 although diagnostically theyare not specific. A high-grade malignant salivary glandneoplasm was not considered likely because these arereported to show an irregularly shaped mass exhibitinglow signal intensity on T2-weighted images.2,4 Thefinding of slight enhancement of the buccal mass afterthe administration of contrast material on CT was com-patible with the radiographic presentation of a pleomor-phic adenoma.3,5
Hemangiomas in the masseter muscle are rela-tively rare, and approximately 90% of these lesionsdevelop before the age of 30 years.6 Examining aseries of oral and maxillofacial hemangiomas, Kaki-moto et al.7 reported that among 9 cases, on T1-weighted MRI the signal was isointense in 3 casesand hypointense in 5 cases, while T2-weighted im-ages revealed high intensity in 8 cases. However,Griffin et al.8 reported that, among 27 patients, 70%of intramuscular hemangiomas showed mildly hyper-intense signals on T1-weighted images, and 96% hada hyperintense signal on T2-weighted images.8 Inthis series, only 2 cases involved the head and neckregion. These contrasting findings demonstrate thatthe characteristic MRI findings of intramuscularhemangiomas in the oral and maxillofacial regionsare unclear, especially on T1-weighted images. In-terestingly, capillary hemangiomas exhibited strongcontrast enhancements on contrast-enhanced CT im-ages, whereas the cavernous types were not alwaysadequately enhanced by contrast material.9 Phlebo-liths were identified on CT images in approximately30% of cavernous hemangiomas.9 In the presentcase, although the findings of MRI and contrast-
Fig. 1. Photograph showing swelling of the left buccal region(arrowhead).
enhanced CT scans were consistent with cavernous
hemangiomas, phleboliths were not identified on theplain CT images.
Hodgkin’s lymphoma and non-Hodgkin’s lymphomafrequently involve the head and neck. Hodgkin’s lym-phoma arises in a single node or chain of nodes andspreads first to anatomically contiguous lymphoid tis-sues. Extranodal involvement is rare, with an incidenceof 4%-5%.10 In contrast, extranodal lesions occur in20%-34% of cases of non-Hodgkin’s lymphoma.11 Thedigestive tract is the site most frequently involved, andthe masticatory muscle is an uncommon site.11,12 OnMRI, intramuscular lesions of non-Hodgkin’s lym-phoma are homogeneously isointense or slightly hy-pointense relative to normal muscle on T1-weightedimages and are hyperintense relative to muscle on T2-weighted images.13,14 In addition, intramuscular lesionsof non-Hodgkin’s lymphoma mostly manifest as dif-fuse enlargement of the involved muscles.12-14 Thisobservation was not congruent with that of the presentcase, which showed a distinct mass in the left massetermuscle.
Rhabdomyomas are benign neoplasms of the skeletalmuscle that are the most frequently primary tumors ofthe heart in infants and children.15 Extracardiac rhab-domyomas, although very rare, show a striking predi-
Fig. 2. Contrast-enhanced computerized tomography revealsa regular-shaped mass measuring 30 � 20 mm within the leftmasseter muscle. The mass is slightly and homogeneouslyenhanced. No bone destruction is found on the left mandib-ular ramus.
lection for the head and neck regions.16

OOOOE142 Yamada et al. August 2010
Lastly, schwannoma and other soft tissue tumorsshould also be included in the differential diagnosis.
DIAGNOSIS AND MANAGEMENTBiopsy was performed via the oral mucosa under
local anesthesia. Yellow-colored solid tissue was ob-
Fig. 3. Magnetic resonance imaging. A, T1-Weighted axialimage, showing an isointense mass in the left masseter muscle(arrowheads). B, T2-Weighted axial image, showing a ho-mogeneously increased signal intensity within the mass.
tained. A fibrous capsule was not present (Fig. 4).
Examination of hematoxylin and eosin–stained sectionsrevealed proliferating aggregates of polygonal or ovalcells, forming alveolar structures. The individual cellu-lar aggregates were separated by a framework of fibro-vascular septa (Fig. 5, A). A single layer of neoplasticcells adhered to the fibrous septa with a central loss ofcellular cohesion. The tumor cells had ovoid nucleiwith scant amounts of indistinct cytoplasm (Fig. 5, B).
Immunohistochemical staining was performed using anavidin-biotin method. Immunoreactivity for muscle-spe-cific actin (mouse anti–human muscle actin monoclonalantibody, clone HHF35; DakoCytomation, Glostrup, Den-mark; Fig. 5, C), MyoD1 (mouse anti-MyoD1 monoclo-nal antibody, clone 5.8A; DakoCytomation; Fig. 5, D),myogenin (mouse anti-myogenin monoclonal antibody,cloneF5D; DakoCytomation; Fig. 5, E) and vimentin(mouse antivimentin monoclonal antibody, clone V9; Da-koCytomation; data not shown) were positive in the tumorcells. Conversely, cytokeratin (mouse anti–human CKmonoclonal antibody, clone MNF116; DakoCytomation;data not shown) was negative in the tumor cells.
The final diagnosis was rhabdomyosarcoma, alveolartype.
Ten days after the biopsy, the mass was resectedunder general anesthesia. The surgical margin was pos-itive on the resected tumor specimen and was classifiedto group II according to the Intergroup Rhabdomyosar-coma Study (IRS) grouping system.17 Accordingly, thepatient received postoperative radiation to 45 Gy andchemotherapy consisting of 14 cycles of vincristine,actinomycin D, and cyclophosphamide (VAC).
DISCUSSIONRhabdomyosarcoma is a malignant neoplasm charac-
terized by skeletal muscle differentiation which is rela-
Fig. 4. A photograph showing a solid yellow mass at biopsyvia the oral mucosa.
tively uncommon in the head and neck of adults. The

n, orig400).
lear im
OOOOEVolume 110, Number 2 Yamada et al. 143
main histopathologic subtypes are classified as embryo-nal, alveolar, and pleomorphic types. Alveolar types ac-count for 20%-30% of all rhabdomyosarcomas and affect
Fig. 5. Photomicrographs of the excised lesion. A, Proliferaand eosin [HE] stain, original magnification �200). B, Polygoto fibrous septa with central loss of cellular cohesion (HE staifor muscle actin in the tumor cells (original magnification �(original magnification �400). E, Some tumor cells with nuc
young adults between 10 and 25 years of age.18 Prognosis
of alveolar types is poor compared with embryonaltypes.18,19
There are few reports describing the characteristic
gregates of cells exhibiting alveolar structures (hematoxylinls with ovoid nuclei. A single layer of neoplastic cells adheresinal magnification �400). C, Cytoplasmic immunoreactivityD, Nuclear immunoreactivety for MyoD1 in the tumor cellsmunoreactivity for myogenin (original magnification �400).
ting agnal cel
radiographic findings of rhabdomyosarcomas;20-23

OOOOE144 Yamada et al. August 2010
mostly consisting of a relatively small number of cases(9-17 patients) and including various histopathologictypes of rhabdomyosarcoma.
Treatment of rhabdomyosarcoma involves surgery,radiation, and chemotherapy. Histologic subtype,19 theprimary site of the tumor,24 and the clinical groupdefined by the IRS grouping system17 are the keyfactors in deciding on treatment modality. In thepresent case, although the primary site was favorable,24
the histologic subtype indicated a worse prognosis.18,19
Furthermore, the resection was incomplete. Therefore,postoperative radiation and intensive VAC chemother-apy were performed.
REFERENCES1. Fyfe EC, Kabala J, Guest PG. Magnetic resonance imaging in the
diagnosis of asymmetrical bilateral masseteric hypertrophy. Den-tomaxillofac Radiol 1999;28:52-4.
2. Som PM, Biller HF. High-grade malignancies of the parotidgland: identification with MR imaging. Radiology 1989;173:823-6.
3. Kakimoto N, Gamoh S, Tamaki J, Kishino M, Murakami S,Furukawa S. CT and MR images of pleomorphic adenoma inmajor and minor salivary glands. Eur J Radiol 2009;69:464-72.
4. Lee YY, Wong KT, King AD, Ahuja AT. Imaging of salivarygland tumours. Eur J Radiol 2008;66:419-36.
5. Lev MH, Khanduja K, Morris PP, Curtin HD. Parotid pleomor-phic adenomas: delayed CT enhancement. AJNR Am J Neuro-radiol 1998;19:1835-9.
6. Welsh D, Hengerer AS. The diagnosis and treatment of intra-muscular hemangiomas of the masseter muscle. Am J Otolaryn-gol 1980;1:186-90.
7. Kakimoto N, Tanimoto K, Nishiyama H, Murakami S, FurukawaS, Kreiborg S. CT and MR imaging features of oral and maxil-lofacial hemangioma and vascular malformation. Eur J Radiol2005;55:108-12.
8. Griffin N, Khan N, Thomas JM, Fisher C, Moskovic EC. Theradiological manifestations of intramuscular haemangiomas inadults: magnetic resonance imaging, computed tomography andultrasound appearances. Skeletal Radiol 2007;36:1051-9.
9. Aspestrand F, Kolbenstvedt A. Vascular mass lesions and hy-pervascular tumors in the head and neck. Characteristics at CT,MR imaging and angiography. Acta Radiol 1995;36:136-41.
10. Aiken AH, Glastonbury C. Imaging Hodgkin and non-Hodgkinlymphoma in the head and neck. Radiol Clin North Am2008;46:363-78.
11. Krol AD, le Cessie S, Snijder S, Kluin-Nelemans JC, Kluin PM,Noordijk EM. Primary extranodal non-Hodgkin’s lymphoma(NHL): the impact of alternative definitions tested in the Com-prehensive Cancer Centre West population-based NHL registry.
Ann Oncol 2003;14:131-9.12. Chong J, Som PM, Silvers AR, Dalton JF. Extranodal non-Hodgkin lymphoma involving the muscles of mastication. AJNRAm J Neuroradiol 1998;19:1849-51.
13. Lee VS, Martinez S, Coleman RE. Primary muscle lymphoma:clinical and imaging findings. Radiology 1997;203:237-44.
14. Surov A, Holzhausen HJ, Arnold D, Schmidt J, Spielmann RP,Behrmann C. Intramuscular manifestation of non-Hodgkin lym-phoma and myeloma: prevalence, clinical signs, and computedtomography features. Acta Radiol 2010;51:47-51.
15. Schoen FJ, Mitchell RN. The heart. In: Kumar V, Abbas AK,Fausto N, Aster JC. editors. Robbins and Cotran pathologic basisof disease. 8th ed. Philadelphia: Elsevier Saunders; 2009. p.583-4.
16. Neville BW, Damm DD, Allen CM, E. Bouquot J. Rhabdomy-oma. In: Oral and maxillofacial pathology. 3rd ed. St. Louis:Saunders Elsevier; 2008. p. 550-2.
17. Maurer HM, Beltangady M, Gehan EA, Crist W, Hammond D,Hays DM, et al. The Intergroup Rhabdomyosarcoma Study—I. Afinal report. Cancer 1988;61:209-20.
18. Neville BW, Damm DD, Allen CM, E. Bouquot J. Rhabdomyo-sarcoma. In: Oral and maxillofacial pathology. 3rd ed. St. Louis:Saunders Elsevier; 2008. p. 559-61.
19. Raney RB, Chintagumpala M, Anderson J, Pappo A, Qualman S,Wharam M, et al. Results of treatment of patients with superficialfacial rhabdomyosarcomas on protocols of the Intergroup Rhab-domyosarcoma Study Group (IRSG), 1984-1997. Pediatr BloodCancer 2008;50:958-64.
20. Lee JH, Lee MS, Lee BH, Choe DH, Do YS, Kim KH, et al.Rhabdomyosarcoma of the head and neck in adults: MR and CTfindings. AJNR Am J Neuroradiol 1996;17:1923-8.
21. Latack JT, Hutchinson RJ, Heyn RM. Imaging of rhabdomyo-sarcomas of the head and neck. AJNR Am J Neuroradiol1987;8:353-9.
22. Hagiwara A, Inoue Y, Nakayama T, Yamato K, Nemoto Y,Shakudo M, et al. The “botryoid sign”: a characteristic feature ofrhabdomyosarcomas in the head and neck. Neuroradiology2001;43:331-5.
23. Yousem DM, Lexa FJ, Bilaniuk LT, Zimmerman RI. Rhabdomy-osarcomas in the head and neck: MR imaging evaluation. Radi-ology 1990;177:683-6.
24. Rodeberg DA, Stoner JA, Hayes-Jordan A, Kao SC, Wolden SL,Qualman SJ, et al. Prognostic significance of tumor response atthe end of therapy in group III rhabdomyosarcoma: a report fromthe children’s oncology group. J Clin Oncol 2009;27:3705-11.
Reprint requests:
Dr. H. YamadaDepartment of Oral and Maxillofacial SurgeryTsurumi University School of Dental Medicine2-1-3 Tsurumi, Tsurumi-kuYokohama, 230-8501
[email protected]